
Abstract
In three studies, with samples from different countries (the United States and Israel) and religions (Christians and Jews), we found that individual levels of fear of death significantly predicted lower willingness to register as organ donors (Studies 1 and 2). Moreover, after being asked about their organ donation status (i.e., whether they are registered as donors), fear of death significantly increased among unregistered people. This did not occur among registered people, who had already faced the decision to become donors in the past (Study 2). Finally, providing non-registered (non-religious) people with a defense strategy to manage their fear of death increased their willingness to sign an organ donation commitment, partially by increasing their feelings of hopefulness. The implications of these findings for increasing organ donation registration are discussed.
Introduction
The number of patients awaiting transplantation worldwide is exceeding the demand for available organs every year. 1 More than 100,000 people need a lifesaving transplant in the United States alone. This gap is puzzling considering that although Americans support organ donation (henceforth: OD) as a lifesaving treatment, only about half of them commit to donating organs after their death. 2 Because most transplants come from deceased donors, increasing the number of people who enroll in state donor registries has become increasingly important.
However, this goal is challenging because many people find choosing to donate organs after death aversive (e.g., Morgan et al., 2008) since it confronts them with the distressing thought of their death (e.g., Harel & Kogut, 2021; Reynolds-Tylus et al., 2021). Surprisingly, only a few studies have investigated the association between OD decisions and fear of death (e.g., Harel et al., 2017; Hirschberger et al., 2008; Jain & Ellithorpe, 2016; Reynolds-Tylus et al., 2021). Furthermore, this research has largely examined how different manipulations that increase (or decrease) death-related thoughts affected attitudes and decisions regarding OD. However, it has not addressed the association between individual differences in fear of personal death (henceforth: FPD) and OD decisions. Moreover, the interaction between such manipulations and individual differences in FPD is yet to be examined. Such examination is in line with recent studies on health communication highlighting the importance of the congruence between individuals’ characteristics and the way messages aiming to improve health-related decisions are framed (e.g., Betsch et al., 2016).
We aim to expand previous research on fear of death and OD decisions in several ways: First, we examine for the first time how individual differences in FPD shape the decision to commit to OD after death, and whether FPD levels significantly differ between registered donors and those who refused to register.
Second, we employ a longitudinal design and measure FPD before and after reminding people about their decision to register (or not) as donors. This can inform us about how FPD deters OD commitment.
Third, we explore whether eliciting a sense of immortality promotes unregistered people’s willingness to register as organ donors. This is a challenging goal considering that past research showed the difficulties of persuading people to register because of relatively stable beliefs (such as religious identities, e.g., Da Silva & Frontera, 2015, and other more specific beliefs, Harel et al., 2022). Here, we show that individual differences in FPD are related to people’s OD status (registered vs. unregistered) beyond religious identity and that eliciting a sense of immortality increases the willingness to register among non-religious people.
Fourth, since religiousness is one of the main obstacles to OD registration (e.g., Da Silva & Frontera, 2015), it is important to study the specific death fears held by religious and non-religious people, and how they may predict willingness to commit to OD in each population. This has both theoretical and practical implications that can further our understanding of the complex relations between FPD and OD registration and can help devise simple and cost-effective ways to increase registration.
Theoretical Background
The cognitive ability to understand that death is inevitable induces terror and anxiety (Solomon et al., 1991). Terror management theory (TMT) suggests several defense mechanisms that people use to tame death anxiety (Pyszczynski et al., 1999) such as suppressing death-related thoughts by shifting to the future or adopting beliefs and conceptions that create symbolic immortality (e.g., adhering to cultural worldviews that instill a sense of importance and value, Solomon et al., 1991).
According to TMT (e.g., Greenberg et al., 1997), acting prosocially helps suppress anxiety-provoking cognitions about death—insofar as helping others makes people feel more valuable, and the world more meaningful. Thus, when death thoughts are salient, people may act prosocially to protect themselves from the intimidating awareness of their personal mortality.
However, research suggests that mortality salience (henceforth, MS) increases prosocial behavior only in ways that are consistent with one’s cultural standards of helping, which uphold the moral principles of one’s cultural worldview. For instance, Jonas et al. (2002) found that MS enhances a bias toward charitable causes that support one’s own cultural affiliation (e.g., donating to an American vs. a foreign association). This aligns with the idea that MS encourages people to transcend the physical self through behaviors that support relevant worldviews or values (Arndt et al., 2002). Moreover, the helping situation often features competing norms and values (e.g., generosity and accumulation of wealth). In such cases, MS would encourage the norm(s) that is more salient in the situation (Jonas et al., 2013). In the case of signing an OD commitment, the prosocial value of saving lives competes with other possibly more salient beliefs elicited by the context. For religious people, it could be the belief that individuals should not intervene with God’s will by giving someone else’s organs to a dying person (Davis & Randhawa, 2006; Morgan et al., 2008), or the belief for the body to remain intact after death, so that it may be resurrected in the End of Days. This belief is not limited to religious people and may reflect the general discomfort or anxiety people may have about OD (e.g., Harel et al., 2022; Robinson et al., 2014). When considering an OD commitment, a decision that triggers death thoughts, people are likely to follow the above beliefs that are directly related to the context of OD (rather than adhering to the value of saving lives). Thus, although OD is a prosocial act, it may not be enhanced by MS.
Another reason why MS may not increase willingness to donate organs stems from the fact that the prosocial act (donating the organs) requires the death of the donor themselves. Accordingly, Hirschberger et al. (2008) found that, under MS, people donated more to charity, but not to charities that re-evoke the sense of self-mortality. Corroborating this idea, Harel and colleagues (2017) found that presenting OD cases in a way that makes thoughts of death salient (e.g., identifying the deceased donor) decreases people’s willingness to register as organ donors. Conversely, OD cases that heighten lifesaving thoughts (such as identifying the recipient who was saved by ODs) increase willingness to commit to OD. Although some studies found that MS increases information-seeking and positive attitudes toward OD, MS can distance people from prosocial acts that highlight their own death, as in the case of OD commitments.
Besides the thoughts of death that likely emerge when considering signing an OD commitment, individuals vary in the extent to which they generally fear death and in their chief death-related concern. Florian and Har-Even (1984) and Florian et al. (1984) constructed a tri-dimensional model of the FPD that addresses three aspects of meaning that people may attach to their own death. The intrapersonal dimension comprises concerns and worries related to the consequences of death for one’s own mind and body—such as worries about the decomposition of the body and the fear of failure to accomplish important life goals. The interpersonal dimension consists of concerns about the painful impact of death on one’s close relationships and family—such as the fear of being unable to provide for one’s family. Finally, the transpersonal dimension refers to concerns related to the hereafter—such as fear of punishment in the afterlife.
Based on this model, Florian and Kravetz (1983) constructed and validated a 31-item self-report questionnaire, known as the FPD Scale, which includes 6 subscales: Self Fulfillment (fear of losing opportunities for self-fulfillment), Social Identity (fear of losing social presence and identity), Family and Friends (fear about the consequences of one’s death to family and friends), Transcendental Consequences (concern about the uncertainty and ambiguity of the state of personal existence after death), Self-Annihilation (the fear of the state of physical and personal disintegration and annihilation), and Punishment in the Hereafter. While the research that we reviewed supports the idea of a general correlation between FPD and OD registration, it is possible that certain fears are more or less strongly associated with OD decisions. A closer investigation of these relations may provide a more fine-grained analysis of this issue.
In sum, while several studies examined the effect of incidental manipulations of death salience on OD decisions, our work is the first, to the best of our knowledge, to test the role of individual differences in FPD and its subscales in OD registration decisions. Moreover, our research is the first to directly compare registered and unregistered people’s FPD and to test how a reminder of their decision to sign an OD commitment (or not) affects their respective FPD. Finally, we test whether a manipulation that increases the sense of immortality among unregistered people can increase their willingness to register as organ donors.
This Research
We conducted three studies to explore the association between FPD and people’s willingness to register as organ donors. In Study, 1 we examined the relationship between individual differences in overall FPD (and in each of the six subscales) and the decision to sign an OD commitment (Yes/No) in a representative sample of the Jewish population in Israel. In Study 2, we measured and compared individual differences in FPD among American MTurkers (both registered and unregistered) before and after asking them about their willingness to register as organ donors. This allowed us to detect changes in FPD caused by considering an OD registration. Finally, in Study 3, we employed a manipulation that provides participants with a defense mechanism (i.e., increasing sense of immortality) and examined its effect on unregistered people’s willingness to commit to ODs.
Importantly, in our studies, we consider people’s religious identity. First, extensive research showed how religion is a major obstacle to ODs (Da Silva & Frontera, 2015). Second, religious people likely experience specific fears of death such as the fear of punishment in the hereafter (Florian & Kravetz, 1983). Finally, the manipulation to increase a sense of immortality that we use in Study 3 includes some evidence about a sort of existence after the physical death of the body (e.g., Dechesne et al., 2003; Schoenrade, 1989). This manipulation likely interacts with people’s religious identity, since most religious people believe in the afterlife (e.g., Bivens et al., 1995).
The study received approval from the Human Subjects Research Committee of the Ben-Gurion University of the Negev, Number 1913-1 (2019-2025). All participants signed a consent form before participation. All data collected in this research and studies’ procedures can be found online at https://osf.io/vs25r/?view_only=9c589cc90ee3454ca1a1505f325582cb
Study 1
Method
We recruited a representative sample of the Jewish population in Israel (excluding ultraorthodox people; N = 507; 50.6% female, Mage = 38.82, SDage = 13.28), via an online survey company. Participants first completed a short version (19 items) of the FPD scale (Florian et al., 1984; Florian & Kravetz, 1983). Next, they reported whether they were registered as organ donors. Finally, they completed demographic information including a self-definition of their religious identity (by choosing one of four options: not religious, traditional, religious, and ultraorthodox).
Results and Discussion
A total of 327 participants (64.4%) were not registered as organ donors (henceforth: refusers), while 181 people reported being registered donors (henceforth: signers). 3 We conducted a logistic regression analysis to test whether FPD (averaged across the 19 items, α = .92) predicted participants’ decision to register. The model was significant, χ2(1) = 15.61, Nagelkerke R 2 = .04, indicating that higher FPD significantly predicted lower willingness to register as an organ donor, b = −0.27, SE = 0.07, p < .001. In line with previous research, when added to the model, participants’ religious identity significantly predicted their decision, b = −0.85, SE = 0.12, p < .001, with higher scores corresponding to lower willingness to register. Importantly, FPD remained significant, b = −0.28, SE = 0.07, p < .001. Moreover, there was no significant interaction between religious identity and FPD in predicting registration decisions (p = .65). Finally, all FPD subscales significantly predicted the decision to register (ps < .05). However, only the Fear of a Punishment in the Hereafter significantly correlated with religious identity and thus seems to represent religious people’s unique FPD (see Table 1).
Correlation Between Religious Identity and FPD Subscales (Upper Rows) and Logistic Regression Predicting Willingness to Register (Lower Rows)
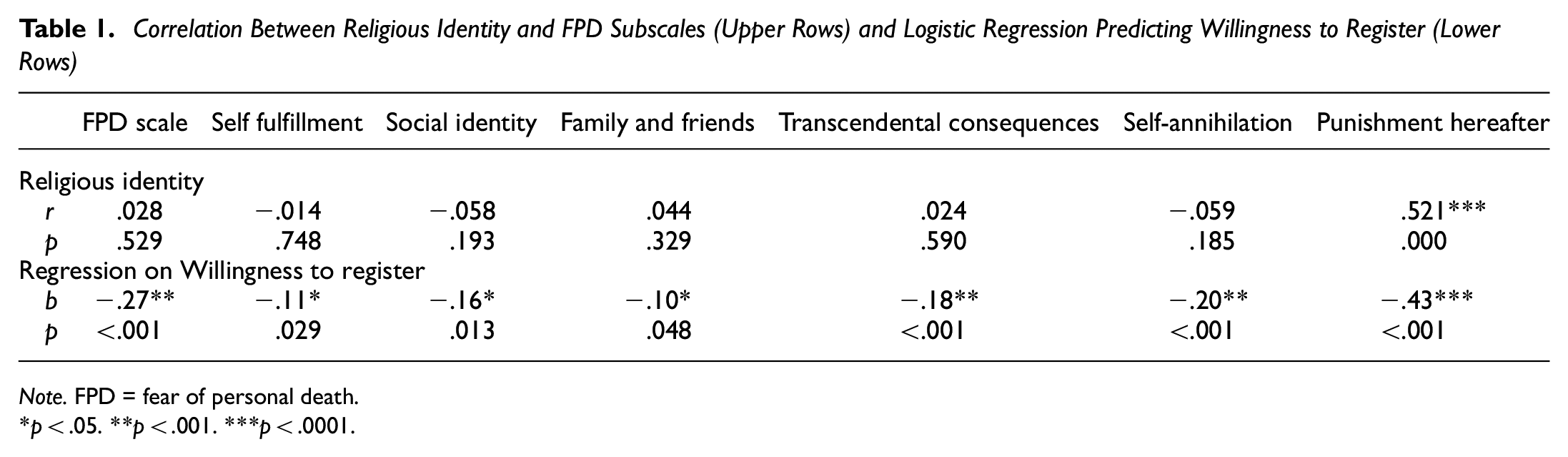
Note. FPD = fear of personal death.
p < .05. **p < .001. ***p < .0001.
We found that FPD and each of its subscales significantly predicted lower willingness to register as organ donors above and beyond religiousness. Finally, religiousness was only significantly correlated with the specific fear of Punishment in the Hereafter, and not with the other subscales of the FPD.
Study 1 showed that the more people fear death, the less likely they are to become organ donors. However, what remains unanswered is whether asking people to sign an OD commitment—which likely makes them think of death—increases FPD. Study 2 addresses this question by examining FPD levels before and after asking people about their willingness to register as organ donors. We hypothesized that considering signing an OD commitment would increase FPD among refusers but not among signers, whose overall FPD is lower (as found in Study 1). Because signers have already dealt with that decision in the past, it is unlikely that considering it once again would affect them. In addition, to increase external validity and generalizability, in Study 2, we sampled U.S. MTurk respondents.
Study 2
Methods
We recruited N = 803 (50% female, Mage = 34.7, SDage = 12.96) participants residing in the United States through MTurk with an approval rate ≥90% on past surveys in exchange for a $ 0.50 fee for each part of the survey. 4 At Time 1, participants first rated their religious identity on a 4-point scale (from secular to religious), followed by the Duke University Religion Index, which includes 5 items (e.g., “How often do you spend time in private religious activities?” “In my life, I experience the presence of the Divine”; α = .91). Next, they completed the long version (31 items) of the FPD scale (Florian & Har-Even, 1983; α = .95) followed by basic demographics. At Time 2, a follow-up survey sent a week later, participants first read that our laboratory is collaborating with the government website “OrganDonor.gov” to increase public commitment to ODs in the United States and promote enrollment in state donor registries. They were then asked whether they would like to sign an OD commitment. 5 Participants had three options to choose from. They could report that they are already registered as organ donors, choose to sign a commitment during the experiment, 6 or refuse to sign. After the decision, they completed the Duke University Religion Index and the FPD scale once again, as at Time 1.
Results and Discussion
A total of 452 participants (56%) reported being already registered donors, while 312 participants were unwilling to sign a commitment. 7 The remaining 39 participants were willing to sign the commitment during the experiment. Since we were interested in comparing signers to refusers, these 39 participants were removed from the analysis (including these participants revealed similar results. Specifically, levels of FPD of this small group were in between signers and refusers at both Time 1 and Time 2).
Fear of Personal Death
We conducted a mixed-model analysis of variance (ANOVA) on FPD (averaged across the 31 items), with Time as a within-subject variable and OD status (signers vs. refusers) as a between-subject variable. Results revealed a significant main effect of Time, F(1, 762) = 9.17, p = .003, ηp 2 = .012, such that, overall, participants reported higher FPD at Time 2 (M = 4.00, SD = 1.34) after being asked to sign the commitment, than at Time 1 (M = 3.90, SD = 1.29), when OD was not mentioned. As predicted, this main effect was qualified by a significant two-way interaction between Time and OD status, F(1, 762) = 5.59, p = .018, ηp 2 = .007. As illustrated in Figure 1, signers’ FPD level did not differ between Time 1 (M = 3.88, SD = 1.24) and Time 2 (M = 3.89, SD = 1.29), F(1, 762) = 0.27, p = .60, ηp 2 < .001. However, refusers reported greater FPD at Time 2 (M = 4.15, SD = 1.41), after being asked about their willingness to register as organ donors, than at Time 1 (M = 4.00, SD = 1.37), F(1, 762) = 12.29, p < .001, ηp 2 = .016. The interaction remained significant, F(1, 762) = 5.39, p = .022, ηp 2 = .007 even with religious identity and level of religiosity (Duke University Religion Index) as covariates. Finally, the FPD subscales that significantly replicated the interaction between Time and OD status were as follows: fear of losing one’s social identity, e.g., the fear of being forgotten by others, F(1, 762) = 4.42, p = .036, ηp 2 = .006, and self-annihilation, e.g., destruction of one’s personality and body, F(1, 762) = 9.16, p = .003, ηp 2 = .012. The results for the Transcendental Consequences scale (e.g., the fear of the unknown) approached significance, F(1, 762) = 2.98, p = .085, ηp 2 = .004.
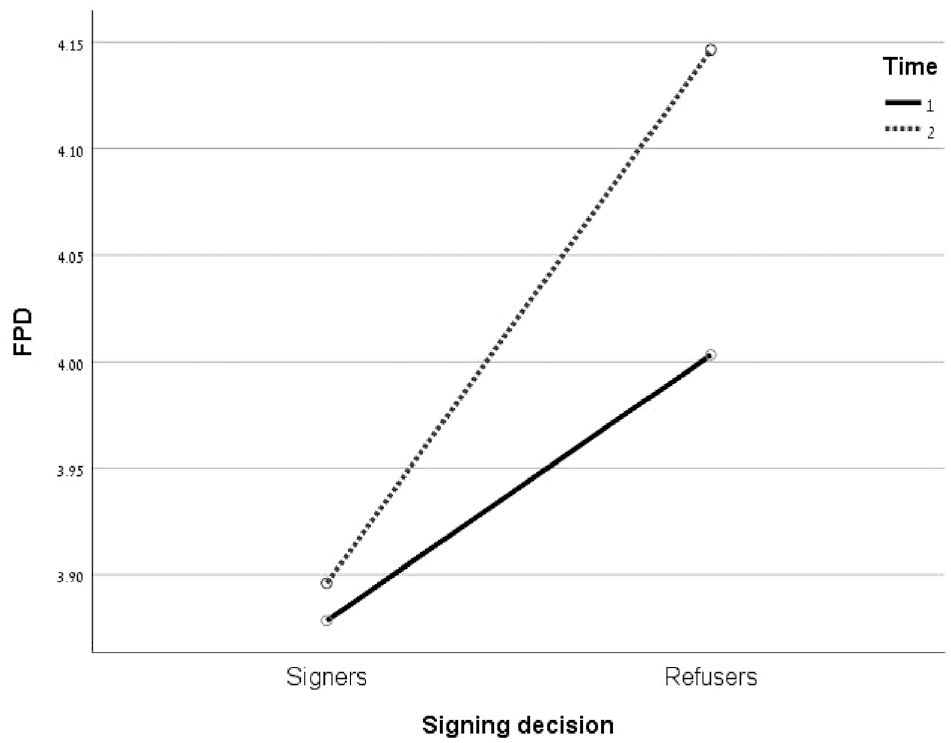
The Fear of Personal Death for Signers and Refusers at Time 1 and 2
Willingness to Register
Replicating the results of Study 1, a logistic regression analysis on willingness to register with FPD and level of religiosity (Duke University Religion Index) as predictors revealed significant results, χ2(2) = 19.97, Nagelkerke R 2 = .035, p < .001 at Time 1, and χ2(2) = 20.61, Nagelkerke R 2 = .04, p<.001 at Time 2. Specifically, FPD (b = −0.11, SE = 0.06, p = .055) and religiosity (b = −0.26, SE = 0.06, p < .001) predicted lower willingness to register at Time 1 and at Time 2 (b = −0.17, SE = 0.06, p = .003 for FPD and b = −0.23, SE = 0.06, p < .001 for religiosity).
In sum, these results corroborate the idea that FPD is related to lower willingness to register as organ donors. This fear becomes more intense after being asked to register, especially among refusers, possibly preventing them from registering.
In Study 3, we provided unregistered people with a defense strategy against FPD in a bid to increase their willingness to register as donors. We presented participants with a scenario taken from Dechesne and colleagues (2003) describing the possibility of a continued life after the physical death of the body to instill an idea of immortality (Dechesne et al., 2003). In their study, participants who read about afterlife were less affected by thoughts of death than those who did not read about it. Similarly, Schoenrade (1989) showed that individuals with stronger (vs. weaker) belief in afterlife reported more positive attitudes toward death after being reminded about it.
Study 3
Method
We recruited N = 178 non-donors 8 (42.7% female, Mage = 38.9, SDage = 12.38 years) residing in the United States through MTurk with an approval rate ≥95% in past surveys in exchange for $ 0.60. Participants were assigned to one of two conditions manipulated between-subjects. Those in the control condition (N = 90) read a short passage about animal navigation while those in the afterlife condition (N = 88) about near death experience and afterlife. The passage was taken almost verbatim from Dechesne and colleagues (2003) and included “convincing evidence for some form of life after death” (p. 724). The passages in both conditions had the same length.
Next, all participants read that our laboratory is collaborating with the government website “OrganDonor.gov,” to increase public commitment to OD in the United States and promote enrollment in state donor registries. As a manipulation check, we asked participants to report the extent to which they believe in an existence after the physical death of the body (1 = not at all; 7 = very much). Next, we asked them whether they would like to sign an OD commitment (Yes or No). Before completing the survey, we collected basic demographic information, asked participants whether they belonged to any particular religion or denomination (Yes/No), and to rate their self-definition of their religiosity on a 7-point scale (1 = not at all religious; 7 = very religious). We followed Dechesne et al. (2003) procedure, which examined emotions following the manipulation as a possible underlying mechanism. In an exploratory approach, we focused on three relevant negative emotions (anxious, vulnerable, and distressed), but also included hope, a positive emotion that may be evoked by the thought of an afterlife, and because previous research has shown its effect in enhancing willingness to commit to OD (Harel et al., 2017). Participants rated the extent to which they felt each of the four emotions when reading about OD, on a 7-point scale (1 = not at all; 7 = very much).
Results
Preliminary Results
An independent t-test revealed that participants who belonged to a particular religion (N = 111) rated their level of religiosity (M = 5.21, SD = 1.36) significantly higher than those with no particular religious affiliation (M = 2.85, SD = 2.05), F(1, 174) = 84.24, p < .0001, d = 1.36. The effect of condition was not significant, F(1, 174) = 0.41, p = .52, and neither was the interaction, F(1, 174) = 0.008, p = .93. They also reported greater beliefs in existence after death (M = 5.77, SD = 1.23) than those with no particular religion (M = 4.04, SD = 2.20), F(1, 174) = 46.66, p < .0001, d = 0.97. The effect of condition was not significant, F(1, 174) = 1.78, p = .18 and neither was the interaction, F(1, 174) = 1.20, p = .28.
Willingness to Register
We computed a logistic regression analysis with willingness to register (coded as 0 = No, 1 = Yes) as the dependent variable and condition (control vs. afterlife), whether participants belonged to any particular religion (coded as 0 = No, 1 = Yes) and their interaction as predictors. The model was significant, χ2(2) = 9.08, Nagelkerke R 2 = .07, p = .028. Results showed no significant effect of condition χ2(1) = 2.47, p = 0.12, a significant effect of whether participants belonged to any particular religion, b = −1.49, SE = 0.67, p = .026, qualified by a significant interaction with condition, b = 1.76, SE = 0.81, p = .029. Among participants who belonged to a particular religion, no difference in willingness to register emerged between conditions (32.2% vs. 32.7% in the control and afterlife condition, respectively), p = .99. However, among participants who did not belong to any particular religion, those in the afterlife conditions were ~4 times more likely to sign (38.9%) than those in the control condition (9.7%), x(1) = 7.51, p = .01.
Moderated Mediation Analyses
For exploratory purposes, we conducted a series of moderated mediation analyses with condition (control vs. afterlife) as predictor, each of the four emotions as mediators, whether participants belonged to any religion as moderator, and willingness to register as the dependent variable (Model 7 with SPSS Macro, Hayes, 2017). Only feelings of hopefulness revealed significant results. 9 Specifically, we found a significant interaction between condition and whether participants belonged to any particular religion on hopefulness, b = −1.42, SE = 0.63, p = .03, showing that learning about afterlife increased hopefulness for those who did not belong to any religion, b = 1.18, SE = 0.50, p = .02, but not for those who did belong to any (p = .55). Importantly, the indirect effect of condition on willingness to register through feeling of hopefulness was significant for those who did not belong to any particular religion, b = 0.87, SE = 0.40, 95% confidence interval (CI) = [0.173, 1.768], but not for those who did belong, b = −0.17, SE = 0.32, 95% CI = [−0.893, 0.396]. This suggests that, for non-religious people, providing a defense strategy supporting the existence of afterlife increased feelings of hopefulness, which in turn increased willingness to register as organ donors. This strategy was not helpful for religious people who already showed a greater belief in afterlife regardless the manipulation.
General Discussion
We examined the association between FPD and people’s willingness to register as organ donors. In three studies, and with samples from different countries (the United States and Israel) and religions (Christians and Jews), we found that FPD significantly predicted lower willingness to register as organ donors (Studies 1 and 2). Moreover, not only did unregistered people report higher FPD than registered people, but their fear increased after being asked about their OD status. Importantly, we did not observe the same pattern among registered people who already decided to become donors in the past. However, unregistered people, who possibly avoided the decision in the past, became more afraid of death when asked about the same decision in the present.
Although several studies have shown that manipulations to increase the salience of death-related thoughts decreased people’s willingness to register as organ donors (e.g., Harel et al., 2017; Hirschberger et al., 2008; Reynolds-Tylus et al., 2021), to the best of our knowledge, our study is the first to examine the association between individual differences in FPD and OD registration. We suggest that besides the inhibitory effect of incidental manipulations to increase thoughts of death (e.g., focusing on the deceased donor, or writing about one’s own death), individual differences in FPD are also related to people’s reluctance to commit to ODs. Moreover, the results of Study 2 suggest that people with higher FPD may be more affected by such incidental manipulations (as reflected by their increase in FPD upon the request to register as organ donors). Thus, it is important to explore the combined effect of situational factors and individual’s level of FPD when studying OD decisions.
Our results also highlight significant differences in levels of FPD between people that are registered and those who refuse to register as organ donors (who reported higher levels of FPD), as well as between religious and non-religious people. Specifically, we found that religious people hold a unique fear of punishment in the hereafter, which may explain their reluctance to register as donors.
Finally, Study 3 demonstrated that providing non-religious unregistered people with a defense strategy to manage their FPD may encourage them to sign an OD commitment. We used a manipulation that previously instilled a sense of immortality (Dechesne et al., 2003) by providing participants with evidence about a continued life after the physical death of the body. This defense mechanism significantly increased non-religious, unregistered people’s willingness to register as organ donors. However, it was not effective for religious people, who already held a stronger belief in afterlife, regardless of the manipulation. Since the results of Study 1 suggest that religious people are particularly concerned about the fear of a punishment in the hereafter, future research may examine manipulations to provide religious people with defense strategies that are specific to this fear. This idea is consistent with the concept of culture-sensitive health communication (Betsch et al., 2016), which underscores the importance of the congruence between recipients’ cultural background and health messages when seeking to improve medical decision-making.
Finally, our exploratory moderated mediation revealed that, for non-religious people, the idea of a continued life after the physical death of the body increased hopefulness, which in turn increased willingness to register. Interestingly, the three negative emotions that we examined (anxiousness, vulnerability, and distress) did not explain this effect. The idea that focusing on positive hopeful messages enhances willingness to ODs has been found in previous research (Harel et al., 2017; Harel & Kogut, 2021), showing that OD presentations that focus on the recipient who was saved by ODs enhanced registration and willingness to donate the organs of a deceased relative (compared with a focus on the deceased donor). Thus, hopeful messages may tame non-registered people’s FPD, enhancing their willingness to support ODs. However, as noted earlier, our approach was exploratory and hopefulness was measured with a single item. Future research is needed to further examine this mechanism, as well as other possible explanations for the effect of the afterlife manipulation on willingness to register. Moreover, future research should use manipulations to increase other defense strategies to deal with FPD, such as enhancing people’s self-esteem or making their worldviews more salient (e.g., Pyszczynski et al., 1999), and examine their effect on willingness to register.
Another limitation is that participants self-reported whether they were donors, which might have led some to lie about it. However, we believe that most participants’ reports were honest. First, the percentages of registered donors in our studies closely match those in the respective populations (see footnotes 3, 7, and 8). Second, there is converging evidence that people are averse to lying (both to themselves and to others) and value morality (e.g., Abeler et al., 2019; Gneezy et al., 2018; Mazar et al., 2008). Third, in our studies, there was no financial incentive for lying. Finally, even if some participants lied about being a donor, the mere thought of actually signing a commitment is still likely to evoke fear and negative emotions similar to actually doing so.
Previous research suggests that the percentage of people who choose to become potential organ donors varies across countries—in line with the policy used to determine voluntary consent. Specifically, in countries with an “opt-out” policy (i.e., where anyone who has not expressly refused is considered a donor), consent rates are around 70%—while, in countries with an “opt-in” policy (where only those who have given explicit consent are donors), only 10% to 40% of the population voluntarily sign up as donors (Johnson & Goldstein, 2003). This discrepancy occurs, at least in part, because the action of registering as a potential organ donor is perceived as being significantly more substantial in the opt-in regime than in the opt-out one (Davidai et al., 2012). Our findings raise the possibility that in opt-in countries, deviation from the status quo—namely, deciding to register as an organ donor—may increase FPD. Anticipating the increase in such feelings or general discomfort (e.g., Morgan et al., 2008) may cause people to avoid the topic altogether. Moreover, previous research suggests that people feel particularly vulnerable when making a decision that deviates from the status quo (e.g., Risen & Gilovich, 2008). An interesting avenue for future research would be to compare FPD among registered and unregistered people in opt-out countries. For instance, it is possible that, in opt-out countries, asking registered donors about their OD status may raise FPD because it forces them to consider their OD status, something that they did not actively do in the past.
Besides the theoretical contribution to the understanding of the role played by FPD in OD decisions, our research may offer practical implications to increase support for OD by presenting the issue in a more positive, hopeful way. Despite the intuition that death-focused messages may attract attention and encourage action, our study suggests that messages that reduce fear of death and inspire hope may help increase support for ODs, potentially saving more lives.
Footnotes
Handling Editor: Malgorzata Kossowska
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Israel Science Foundation Grant 1426/20 and by the National Science Foundation (NSF) Grant 1559546.