
Abstract
Conspiracy beliefs are associated with vaccination hesitancy, which is commonly interpreted as evidence that conspiracy theories contribute to a worldview that damages public health. An alternative, and often ignored, explanation for this relationship is that people may rationalize their existing vaccination hesitancy through conspiracy theories. In two panel studies conducted at multiple time points during the vaccination campaign of 2021, we tested the temporal relationships between COVID-19 conspiracy beliefs and vaccination intentions. Study 1 (three waves in a Dutch sample) provided evidence for temporal effects of conspiracy beliefs on vaccination hesitancy and of vaccination hesitancy on conspiracy beliefs. Study 2 (two waves in a U.S. sample), however, only supported an effect of vaccination hesitancy on conspiracy beliefs over time. Although these findings provide some support for the idea that conspiracy beliefs shape increased vaccination hesitancy, they more consistently support the alternative idea that vaccination hesitancy shapes increased conspiracy beliefs.
Keywords
During the first half of 2021, millions of people around the world were inoculated with one of the medically certified corona vaccines. Significant portions of the population were hesitant to take the vaccine, however, which had implications for policy (e.g., restrictions specifically for unvaccinated people), polarization, and health. Vaccination hesitancy is commonly associated with COVID-19 conspiracy theories, for instance, suggesting that the coronavirus is a hoax or that pharmaceutical companies are dishonest about the side effects of vaccines. Conspiracy theories are broadly defined as suspicions that a group of actors collude in secret to achieve malevolent goals (Bale, 2007; Douglas & Sutton, 2023; Van Prooijen & Van Vugt, 2018). Vaccination intentions are correlated with antivaccination conspiracy theories (Freeman et al., 2021), conceptually unrelated conspiracy theories (e.g., the assassination of John F. Kennedy; Hornsey et al., 2018), and a general predisposition toward conspiracy theories (e.g., political cynicism, Bang Petersen et al., 2021; conspiracy mentality, Winter et al., 2022). A conspiratorial mind-set hence is closely coupled with, and possibly even inherent to, vaccination hesitancy (Enders et al., 2022).
While most research examining the link between vaccination hesitancy and conspiracy beliefs was cross-sectional (e.g., Enders et al., 2022; Freeman et al., 2021; Hornsey et al., 2018, 2021), the 2021 vaccination campaign was a dynamic event that unfolded over the course of several months. Moreover, vaccination intentions and conspiracy beliefs are shaped by a myriad of factors and, therefore, are likely to change over time. For instance, vaccination intentions are influenced by political communications (Hornsey et al., 2020; Pink et al., 2021) and social media behavior (Rathje et al., 2022; Schlette et al., 2022). Conspiracy beliefs change over time during election campaigns (Golec de Zavala & Federico, 2018; Wang & Van Prooijen, 2023), and of particular relevance for the present purposes, show cross-lagged relationships across multiple time points with various health responses (e.g., physical distancing) during the course of the COVID-19 pandemic (Bierwiaczonek et al., 2020, 2022; Pummerer et al., 2022; Van Prooijen et al., 2022, 2023).
The present research sought to move beyond a cross-sectional approach by examining the link between vaccination intentions and COVID-19 conspiracy beliefs in two panel studies with multiple waves that were conducted during the first half of 2021. This approach enables a test of two contrasting, but not mutually exclusive, theoretical accounts of the relationship between vaccination hesitancy and conspiracy beliefs (see also Van Prooijen et al., 2022). The first account is the popular perspective that COVID-19 conspiracy beliefs contribute to a worldview assuming that medical authorities should not be trusted. As such, conspiracy beliefs may gradually shape vaccination hesitancy over time. The second account, however, is the alternative, and often ignored, possibility that conspiracy theories help people rationalize their existing beliefs and behaviors (e.g., Mercier, 2020; Van Prooijen, 2022). It hence may be the case that vaccination hesitancy increases people’s tendency to accept COVID-19 conspiracy theories over time. In the following sections, we illuminate both theoretical ideas in more detail and formulate our hypotheses.
Do Conspiracy Theories Predict Vaccination Hesitancy Over Time?
One key insight is that conspiracy theories are consequential: People’s beliefs drive their behaviors, and conspiracy beliefs therefore have implications for a range of pressing societal issues pertaining to not only health but also climate change, polarization, and voting behavior (Jolley et al., 2022; Van Prooijen & Douglas, 2018). This view for instance stipulates that by highlighting how the world is governed through secret and evil plots, conspiracy theories gradually erode the trust that people have in powerful authorities. People therefore may become increasingly reluctant to follow the health advice of these authorities, particularly for a relatively invasive medical procedure such as vaccination. Experimental findings are consistent with this view by showing that exposure to misinformation about vaccines (Loomba et al., 2021) and conspiracy theories (Jolley & Douglas, 2014) lower people’s vaccination intentions.
While longitudinal designs are not necessarily well-suited to prove causality (Ployhart & Ward, 2011), this theoretical framework does suggest a specific prediction about the temporal relationship between conspiracy beliefs and vaccination intentions: Endorsing COVID-19 conspiracy theories is associated with a decreased willingness to take vaccines over time (Hornsey et al., 2021). Various longitudinal studies have provided support for the temporal effects of conspiracy beliefs on other health behaviors. For instance, during the COVID-19 pandemic, conspiracy beliefs predicted decreased physical distancing over time, more strongly than the reversed temporal order (Bierwiaczonek et al., 2020; Van Prooijen et al., 2022). Assuming a similar process for vaccination hesitancy, we hypothesized that COVID-19 conspiracy beliefs would predict a decrease in vaccination intentions over time (Hypothesis 1).
Do Conspiracy Theories Rationalize Vaccination Hesitancy?
Although the idea that conspiracy theories shape vaccination hesitancy is a common assumption, it should be recognized that an important alternative explanation exists for the relationship between these variables: People may use conspiracy theories to rationalize their existing antivaccination sentiments. This idea is consistent with classic theories of cognitive dissonance (Festinger, 1957), as well as with insights that conspiracy beliefs often emerge through a motivated reasoning process (e.g., Enders & Smallpage, 2019; Miller et al., 2016). Relatedly, conspiracy theories can imbue counter-normative behavior—such as refusing to get vaccinated amid a pandemic—with a sense of legitimacy (Van Prooijen, 2022).
While research mostly found support for the idea that conspiracy theories shaped health behaviors such as decreased physical distancing over time (Bierwiaczonek et al., 2020; Van Prooijen et al., 2022), it is not a given that these findings generalize to vaccination intentions. Physical distancing is mostly socially restrictive, whereas vaccination is more likely considered fear-arousing and physically invasive. People hence may be quite uncomfortable with the prospect of being vaccinated—particularly in the context of the COVID-19 vaccines that were developed relatively quickly, raising widespread concerns about (long-term) side effects. Such initial hesitancy may motivate people to look for reasons not to get vaccinated, which they can find in COVID-19 conspiracy theories (suggesting, for instance, that the coronavirus is a hoax or created for nefarious purposes). Indeed, a preliminary network analysis found stronger support for an effect of vaccination hesitancy on conspiracy beliefs than vice versa (Bronstein et al., 2022). This line of reasoning suggests that low vaccination intentions predict an increase in COVID-19 conspiracy beliefs over time (Hypothesis 2).
The Current Research
Study 1 took place in the Netherlands and had three waves (February to July 2021) that all measured COVID-19 conspiracy beliefs and vaccination intentions, although our main analysis focused on the first two waves due to a low number of participants who still were not vaccinated at Wave 3. Study 2 took place in parallel in the United States and had two waves (March and April 2021). While the key purpose of the present project was to examine the temporal order of the links between COVID-19 conspiracy beliefs 1 and vaccination hesitancy (making it necessary to focus on vaccination intentions, as vaccination decisions are irreversible), the studies also tested whether conspiracy beliefs prospectively predicted the actual vaccination behavior. This further extends earlier research that examined vaccination intentions in cross-sectional designs.
Open Science Practices
Data and supplementary materials are openly accessible on the Open Science Framework, and Study 2 was preregistered before running the first wave. 2 The studies have formal approval from the ethics committee of our university.
Study 1
Method
Participants and Design
The study contained three waves throughout the Dutch COVID-19 vaccination campaign in the first half of 2021. Wave 1 took place from February 3 to 9, 2021, and had 4,558 participants (2,613 men, 1,583 women, 365 missing; Mage = 54.41, CI95% [53.93, 54.88]); Wave 2 took place from 22 April to 3 May 2021 and contained 3,031 of the participants that also completed Wave 1 (1,895 men, 1,136 women; Mage = 58.36, CI95% [57.83, 58.89]); Wave 3 took place from 29 June to 9 July 2021 and contained 2,685 of the participants that also completed Wave 1 (1,677 men, 1,008 women; Mage = 57.00, CI95% [56.43, 57.56]). A total of 2,358 participants completed all three waves (1,493 men, 865 women; Mage = 59.51, CI95% [58.92, 60.10]).
Procedure
The project was part of a larger data-collection effort in collaboration with Kieskompas (Election compass), a Dutch political research organization that coordinates large research panels. Kieskompas complies with EU privacy (General Data Protection Regulations) regulations, is closely monitored by the Dutch privacy authority, and adheres to the ethical norms of our university. The panels were acquired through voting advice applications before Dutch elections and were complemented with targeted survey studies. For each wave, participants were invited through email.
Measures
In each wave, participants were asked dichotomously (no versus yes) whether they were already vaccinated with one of the medically approved COVID-19 vaccines. Participants who responded “no” were then asked whether they intended to get vaccinated against COVID-19 (1 = certainly not, 5 = certainly). As might be expected, vaccination intention and participant numbers were lowest at Wave 3 for this variable, when all Dutch adults who wanted to get vaccinated already had had the opportunity to do so (Wave 1: N = 4,477, M = 4.33, CI95% [4.29, 4.36]; Wave 2: N = 2,071, M = 4.22, CI95% [4.17, 4.28]; Wave 3: N = 394, M = 2.71, CI95% [2.54, 2.87]). Each wave also included a four-item measure of COVID-19 conspiracy beliefs (Azevedo et al., 2022; Van Prooijen et al., 2023), for example, “The coronavirus (COVID-19) is a hoax invented by interest groups for financial gains” (1 = strongly disagree, 5 = strongly agree) (Wave 1: M = 1.45, CI95% [1.43, 1.47], α = .91; Wave 2: M = 1.46, CI95% [1.44, 1.48], α = .93; Wave 3: M = 1.53, CI95% [1.51, 1.55], α = .91).
Results
Waves 1 and 2
Our main analyses focused on Waves 1 and 2, which we analyzed separately given the large loss of data associated with Wave 3. In hierarchical regression analyses, we included in Step 1 the control variables gender, age, education level (1 = University Master, 8 = No education; recoded), and self-reported political ideology (0 = left wing, 10 = right wing) as reported in Wave 1. The regression results are displayed in Table 1.
The Relationships Between COVID-19 Conspiracy Beliefs (CB) and Vaccination Intentions at Waves 1 and 2: Hierarchical Regression Results—Study 1
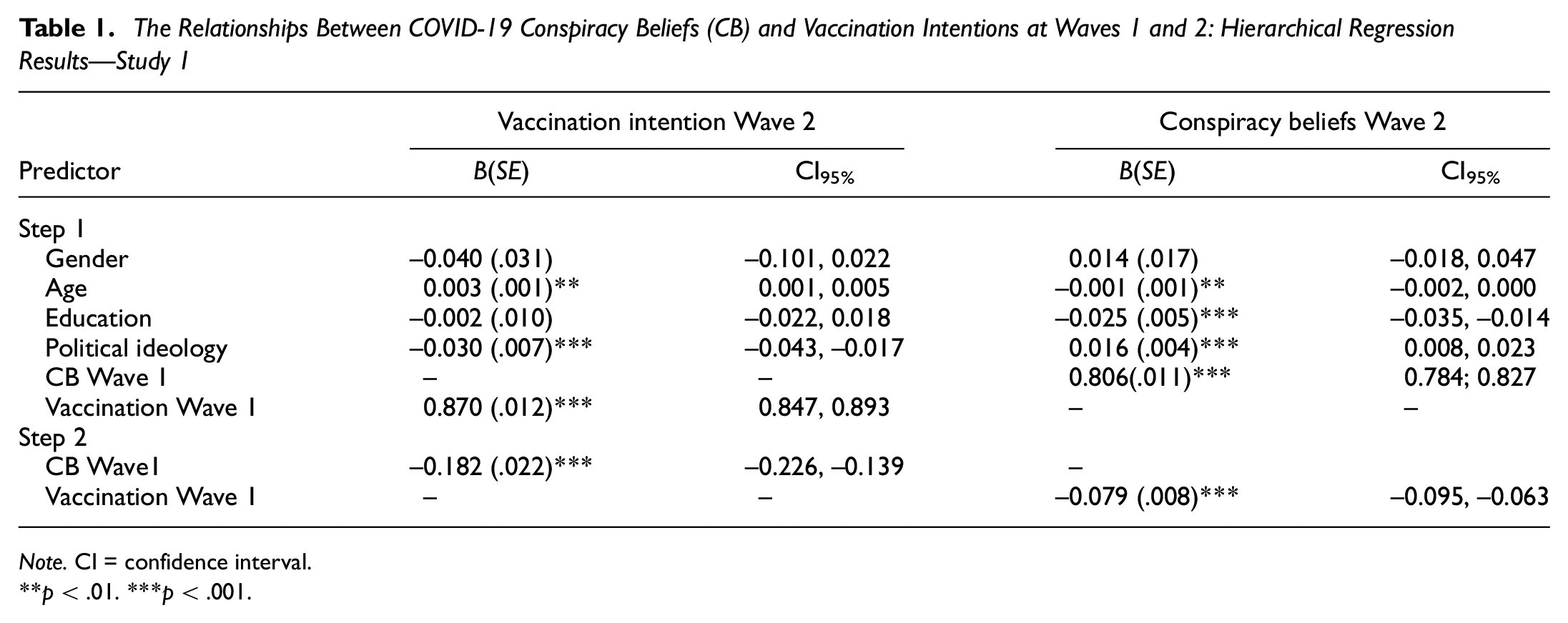
Note. CI = confidence interval.
p < .01. ***p < .001.
To test our first hypothesis, we included Wave 1 COVID-19 conspiracy beliefs as an independent variable in Step 2, with Wave 2 vaccination intentions as dependent variable while including Wave 1 vaccination intentions as an additional control variable in Step 1. This analysis contained 1,959 participants, yielding 95% power to detect a small effect size (f 2 = .007). Step 1 was significant (R 2 = .75), F(5, 1,953) = 1,190.55, p < .001, indicating that vaccination intentions at Wave 2 were stronger to the extent people were older and politically more left wing (see Table 1). Step 2 was also significant (ΔR 2 = .008), F(1, 1,952) = 66.37, p < .001. Supporting Hypothesis 1, higher COVID-19 conspiracy beliefs at Wave 1 predicted decreased vaccination intentions at Wave 2.
To test our second hypothesis, we included Wave 1 vaccination intentions as an independent variable in Step 2, with Wave 2 COVID-19 conspiracy beliefs as a dependent variable while including Wave 1 COVID-19 conspiracy beliefs as an additional control variable in Step 1. This analysis contained 3,011 participants, yielding even more statistical power than the previous analysis. 3 Step 1 was significant (R 2 = .68), F(5, 3,005) = 1,265.17, p < .001. As can be seen in Table 1, COVID-19 conspiracy beliefs at Wave 2 were stronger to the extent people were less educated, more right wing, and younger. Step 2 was also significant (ΔR 2 = .010), F(1, 3,004) = 94.08, p < .001. In line with Hypothesis 2, lower vaccination intention at Wave 1 predicted higher COVID-19 conspiracy beliefs at Wave 2.
Full Longitudinal Analysis
We then also analyzed the full three waves with a cross-lagged panel model (CLPM) and a random-intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015). These analyses were fully exploratory given that it was restricted to participants who (a) were not vaccinated yet in the summer of 2021 and (b) participated in all three waves (N = 324). To save degrees of freedom (considering the relatively low sample size for these complex statistical models), this analysis did not include control variables. The sample size meets the requirements for structural equation modeling of five to six participants per estimated parameter (Bentler & Chou, 1987). The analysis was run in the lavaan package of R (Rosseel, 2012), and model fit was determined using the common indicators Comparative Fit Index (CFI >.90), the Root Mean Square Error of Approximation (RMSEA <.08), and the Standardized Root Mean Squared Residual (SRMR <.08). Results are displayed in Figure 1.
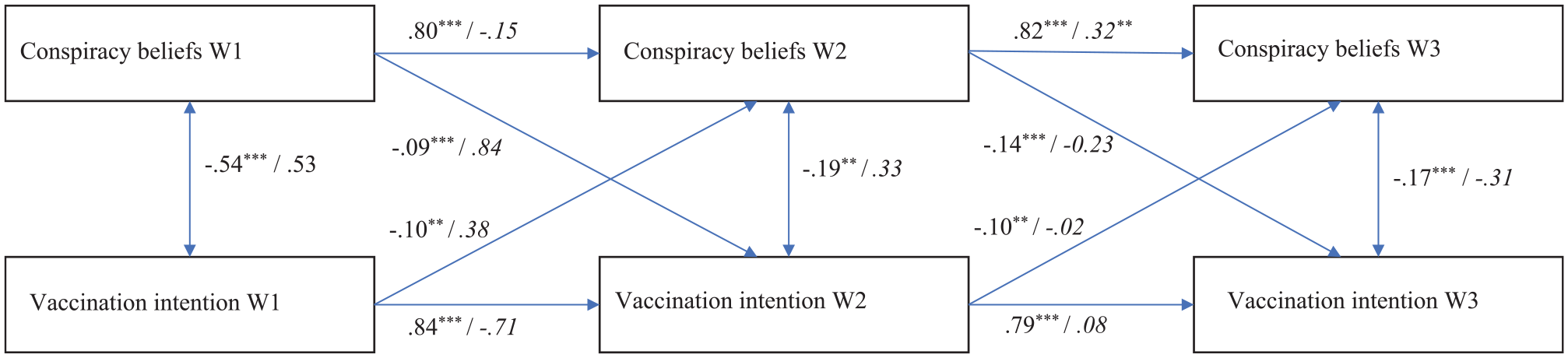
The Relationship Between Conspiracy Beliefs and Vaccination Intentions Over Time (Fully Standardized Solution)
The CLPM had a good fit according to two out of three indicators, the exception being the RMSEA (CFI = 0.96; RMSEA = 0.25, CI90% [0.21, 0.30]; SRMR = 0.027; χ2 [4, N = 324] = 87.88, p < .001). We regard the fit of the model acceptable, particularly in light of Monte Carlo simulations showing that the RMSEA often falsely indicates a poor fit when models have small degrees of freedom (Kenny et al., 2015). All the cross-lagged paths were significant and in the predicted direction, further supporting Hypotheses 1 and 2.
We then also analyzed the RI-CLPM, which controls for stable, trait-like variance that differs between participants by including random intercepts in the model. As such, the cross-lagged paths in the RI-CLPM reflect actual within-person change over time (Hamaker et al., 2015). The model had an excellent fit (CFI = 1.00; RMSEA = 0.006, CI90% [0.000, 0.147]; SRMR = 0.008; χ2 [1, N = 324] = 1.011, p = .315). The random intercepts of COVID-19 conspiracy beliefs and vaccination intentions were negatively associated (estimate = −0.963, SE = 0.108, z = −8.916, CI95% [−1.175, −0.752]). None of the cross-lagged paths were significant, however. This suggests that the observed effects for the CLPM reflect between-person differences in how the link between COVID-19 conspiracy beliefs and vaccination intentions developed over time among participants who were not vaccinated yet by the summer of 2021. Put differently, vaccination intentions were more likely to decrease over time among participants high on conspiracy beliefs than among those low on conspiracy beliefs; likewise, conspiracy theories were more likely to increase over time among participants with low vaccination intentions than among those with high vaccination intentions.
Vaccination Behavior
As a final analysis, we tested whether COVID-19 conspiracy beliefs at Wave 1 would predict whether participants were vaccinated at Wave 3. We conducted a logistic regression analysis in which the control variables were entered in Step 1 and COVID-19 conspiracy beliefs in Step 2, with vaccination behavior as a dependent variable (0 = no, 1 = yes). Step 1 was significant, χ2(4) = 266.39, p < .001 (Nagelkerke R 2 = .167). People were more likely to get vaccinated when they were older, B = 0.059, SE = .004, Wald = 221.67, p < .001; Exp(B) = 1.061, CI95% [1.053, 1.069], more highly educated, B = 0.127, SE = .041, Wald = 9.55, p = .002; Exp(B) = 1.136, CI95% [1.048, 1.231], and more left wing, B = −0.132, SE = .026, Wald = 25.05, p < .001; Exp(B) = 0.877, CI95% [0.832, 0.923]. The effect of gender was not significant (p = .906).
More importantly, Step 2 was significant, χ2(1) = 296.73, p < .001 (Nagelkerke R 2 = .336). Respondents holding stronger COVID-19 conspiracy beliefs in February 2021 were substantially less likely to be vaccinated by early July 2021, B = −1.318, SE = .083, Wald = 253.37, p < .001; Exp(B) = 0.268, CI95% [0.228, 0.315]. Extending earlier research showing a negative correlation between conspiracy beliefs and vaccination intentions in cross-sectional designs (e.g., Enders et al., 2022; Freeman et al., 2021; Hornsey et al., 2018), these findings indicate that COVID-19 conspiracy beliefs prospectively predicted actual vaccination behavior in subsequent months during the COVID-19 pandemic.
Discussion
The findings supported both hypotheses. This provides evidence not only for the common assumption that COVID-19 conspiracy theories shape vaccination hesitancy over time but also for the alternative perspective that vaccination hesitancy predicts increased belief in COVID-19 conspiracy theories over time.
A limitation of Study 1 was the high level of attrition. Once vaccinated, participants were not asked for their subsequent vaccination intentions anymore. This limitation was unavoidable given the circumstances and the relatively long time lag between waves: Many participants easily could have received both required COVID-19 vaccinations before the next measurement, and during the first half of 2021, it was not yet known that there would be a round of booster shots by the end of 2021. These participants therefore were likely to have low vaccination intentions despite having a favorable attitude toward vaccination (i.e., Once fully inoculated, people are unlikely to intend getting redundant additional shots). In Study 2, we addressed this issue through a smaller time lag between waves (i.e., 5 weeks). As such, most people who would get their first shot in between waves would still require a second shot at Wave 2.
Study 2
Method
Participants
Wave 1 took place on March 18, 2021. We recruited 602 U.S. participants (321 men, 270 women, 10 other, 1 preferred not to say; Mage = 32.08, CI95% [31.18, 32.98]) through Prolific. Wave 2 took place 5 weeks later (from April 22 to 29, 2022), and we reinvited 562 participants of the first wave (40 participants were already vaccinated against COVID-19 at Wave 1 and were therefore not reinvited). This yielded 429 participants who completed both waves (response rate 76%; 218 men, 199 women, 10 other, 2 preferred not to say; Mage = 32.89, CI95% [31.81, 33.96]). The sample provides 95% power to detect a small effect size (f 2 = .030).
Procedure
Participants were recruited to participate in a two-wave online study via Prolific. After giving their informed consent, participants provided basic demographics (e.g., gender, age, and education level). Participants rated their political orientation on two scales (1 = very left, 7 = very right; and 1 = very liberal, 7 = very conservative), which were strongly correlated (r = .92, p < .001) and therefore averaged into a single index of political orientation. Participants then responded to questions measuring their vaccination intentions and COVID-19 conspiracy beliefs, as part of a larger questionnaire.
Measures
COVID-19 conspiracy beliefs were measured with the same four items as Study 1 (Wave 1: M = 1.52, CI95% [1.45, 1.58], α = .89; Wave 2: M = 1.56, CI95% [1.48, 1.64], α = .90), and vaccination intention was measured with a single item (“Are you willing to get vaccinated with a medically approved COVID-19 vaccine?”; 1 = not at all, 5 = definitely). 4
Results
Confirmatory Analyses
As preregistered, we tested the hypotheses with hierarchical regression analyses. The control variables (gender, age, education, and political ideology) were included in Step 1. Regression results are displayed in Table 2.
The Relationships Between COVID-19 Conspiracy Beliefs (CB) and Vaccination Intentions at Waves 1 and 2: Hierarchical Regression Results—Study 2
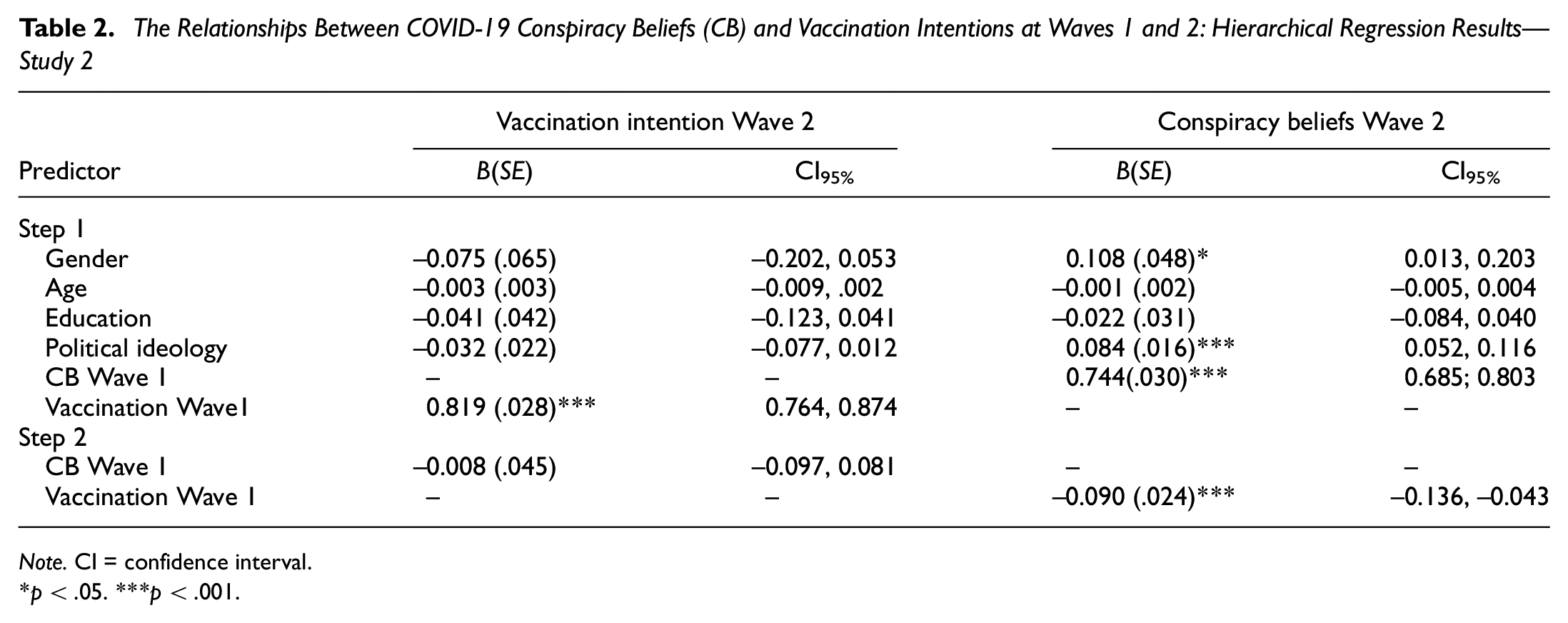
Note. CI = confidence interval.
p < .05. ***p < .001.
To test Hypothesis 1, we included vaccination intention at Wave 1 as an additional control variable in Step 1 and entered COVID-19 conspiracy beliefs at Wave 1 in Step 2. The dependent variable was vaccination intention at Wave 2. Step 1 was significant (R 2 = .74), F(5, 413) = 239.86, p < .001, which was due to the autoregressive effects of vaccination intention at Wave 1; none of the control variables were significant (see Table 2). Step 2, in turn, was not significant (ΔR 2 = .000), F(1, 412) = 0.029, p = .865. Contrary to Hypothesis 1, COVID-19 conspiracy beliefs at Wave 1 did not predict vaccination intentions at Wave 2.
To test Hypothesis 2, we included COVID-19 conspiracy beliefs at Wave 1 as an additional control variable and entered vaccination intention at Wave 1 in Step 2. The dependent variable was conspiracy beliefs at Wave 2. Step 1 was significant, (R 2 = .69), F(5, 412) = 183.08, p < .001. Besides a strong autoregressive effect of COVID-19 conspiracy beliefs at Wave 1, we found significant effects of gender and right-wing political orientation (see Table 2). Step 2 was also significant (ΔR 2 = .010), F(1, 411) = 14.35, p < .001. Supporting Hypothesis 2, lower vaccination intentions at Wave 1 predicted higher COVID-19 conspiracy beliefs at Wave 2.
Vaccination Behavior
We then again conducted a logistic regression analysis, testing whether COVID-19 conspiracy beliefs at Wave 1 would predict whether participants were vaccinated at Wave 2 (0 = no, 1 = yes). The control variables were entered in Step 1, and conspiracy beliefs in Step 2. Step 1 was significant, χ2(4) = 27.22, p < .001 (Nagelkerke R 2 = .084). Only political ideology was significant, showing that vaccination behavior was more likely to the extent participants were more left wing, B = −0.318, SE = .069, Wald = 20.94, p < .001; Exp(B) = 0.728, CI95% [0.635, 0.834]. Step 2 also was significant, χ2(1) = 12.67, p < .001 (Nagelkerke R 2 = .122). Respondents who held stronger COVID-19 conspiracy beliefs at Wave 1 were less likely to be vaccinated by Wave 2, B = −0.517, SE = .154, Wald = 11.32, p < .001; Exp(B) = 0.596, CI95% [0.441, 0.806].
Exploratory Analysis
As the two studies provided inconsistent support for Hypothesis 1, we conducted an equivalence test for the null effect observed in Study 2 (Lakens et al., 2018). To do so, we took the standardized regression weight for testing Hypothesis 1 that we observed in Study 1 (i.e., the effect of conspiracy beliefs at Wave 1 on vaccination intentions at Wave 2, β = −.11) as the smallest effect size of interest. Then, we tested whether this value was in the 90% confidence interval for the standardized regression weight testing Hypothesis 1 in Study 2. Results revealed that the confidence interval did not include the smallest effect size of interest (β = −.005, CI90% [−.055, .045]), further indicating that Study 2 yielded no support for Hypothesis 1.
Discussion
Unlike Study 1, the Study 2 results only supported Hypothesis 2 and not Hypothesis 1. While it is commonly assumed that conspiracy beliefs shape vaccination hesitancy over time, only the alternative perspective—that vaccination hesitancy shapes conspiracy beliefs over time—was supported in both studies.
General Discussion
In two multi-wave panel studies, the present research sought to examine two competing (but not mutually exclusive) explanations for the relationship between conspiracy beliefs and vaccination hesitancy. The first is the popular view that conspiracy beliefs shape vaccination hesitancy over time; the second is the alternative, and often ignored, possibility that conspiracy beliefs help to rationalize people’s existing vaccination hesitancy. Study 1 supported both ideas, but Study 2 only supported the prediction that vaccination hesitancy predicts increased conspiracy thinking over time. Although these findings do not warrant a rejection of the idea that conspiracy beliefs shape increased vaccination hesitancy (see also Jolley & Douglas, 2014), they do indicate that the relationship between these two variables is for an important part due to vaccination hesitancy shaping increased conspiracy beliefs.
An important question is why the temporal effects of conspiracy beliefs on vaccination hesitancy emerged in Study 1 but not in Study 2. While speculative, a plausible possibility is that the time lag between waves was smaller in Study 2 (5 weeks) than that in Study 1 (about 11 weeks between Waves 1 and 2). It may be the case that people’s vaccination intentions change more slowly over time than their conspiracy beliefs. Belief in conspiracy theories can adapt quickly to changing societal circumstances (Wang & Van Prooijen, 2023). But vaccination is a personal medical choice that many citizens consider to be unsettling. People therefore may choose to carefully weigh their options, rendering vaccination attitudes that are less likely to change within a short time frame. More research is required to test this possibility.
The current research makes three novel contributions. First, while conspiracy beliefs certainly impact some of people’s health behaviors (e.g., Pummerer et al., 2022), the present findings underscore that some health behaviors may also shape people’s conspiracy beliefs (cf. Bierwiaczonek et al., 2022; Van Prooijen, 2022). This insight also has implications for interventions aimed at increasing vaccination uptake by reducing conspiracy beliefs. Second, the present findings suggest that different health behaviors may have a qualitatively different relationship with conspiracy beliefs. After all, the present findings indicate a different link between conspiracy beliefs and vaccination intentions over time than previous research has observed for other health behaviors such as physical distancing (Bierwiaczonek et al., 2020; Van Prooijen et al., 2022). Third, most previous studies have examined vaccination intentions in cross-sectional designs (Enders et al., 2022; Freeman et al., 2021; Hornsey et al., 2018). Both studies reported here show that COVID-19 conspiracy beliefs prospectively predicted a decreased likelihood of getting inoculated in the weeks that followed.
Limitations
The current studies also have several limitations. One issue was that the samples were limited in various ways. Notably, neither sample was nationally representative. Moreover, Study 1 had high levels of nonrandom attrition, as participants who were vaccinated were not asked for future vaccination intentions anymore. This could potentially have biased the estimates, particularly in later waves. Of importance, asking fully vaccinated participants for their future vaccination intentions also could have biased estimates (e.g., once fully inoculated, intentions to get an additional shot are likely to be low). Study 2 was designed to address this limitation through a smaller time lag in between waves, implying that most participants who were not vaccinated at Wave 1 still required a second shot at Wave 2. Still, the nonrandom attrition in Study 1 implies a limitation in the interpretation of these findings.
Furthermore, while suggestive, the findings presented here do not fully prove causality, as it is impossible to control for all possible confounding variables (Ployhart & Ward, 2011). Indeed, there were many complexities during the COVID-19 vaccination campaign that were difficult to capture, such as variation in policies (across time and between countries), news about side effects that were associated more strongly with some vaccines than with others, and so forth. We acknowledge that establishing a causal effect of vaccination hesitancy on conspiracy beliefs will be quite a challenge for future research, as it would require researchers to manipulate vaccination hesitancy experimentally.
Finally, the present findings do not provide solid evidence for the underlying process that we assume. While the temporal effects of vaccination intentions on conspiracy beliefs are consistent with a rationalization process (Van Prooijen et al., 2022), these effects do not provide insight into the exact reasoning processes that took place. How exactly do participants use conspiracy theories to justify not getting vaccinated? How does this unfold over time? Moreover, do people rationalize their vaccination hesitancy mostly toward themselves (i.e., self-justification), toward others (i.e., self-presentation), or both? These are open questions that suggest fruitful avenues for future research.
Concluding Remarks
Conspiracy beliefs are associated with vaccination hesitancy, which is often seen as a testimony to the dangerous effects of conspiracy theories. Indeed, intervention campaigns to increase public health often focus on reducing conspiracy beliefs (Loomba et al., 2021). These considerations ignore a realistic alternative possibility: When people are reluctant to get vaccinated, they subsequently may use conspiracy theories to rationalize these sentiments. While the present findings provided some support for the temporal effects of conspiracy theories on vaccination intentions, only the temporal effects of vaccination intentions on conspiracy beliefs were consistently observed in both studies. The relationship between vaccination hesitancy and conspiracy theories appears for an important part due to a rationalization process that unfolds over time.
Supplemental Material
sj-docx-1-spp-10.1177_19485506231181659 – Supplemental material for Do Conspiracy Theories Shape or Rationalize Vaccination Hesitancy Over Time?
Supplemental material, sj-docx-1-spp-10.1177_19485506231181659 for Do Conspiracy Theories Shape or Rationalize Vaccination Hesitancy Over Time? by Jan-Willem van Prooijen and Nienke Böhm in Social Psychological and Personality Science
Footnotes
Handling Editor: Christopher, Federico
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.