
Abstract
Social relationships influence physical health, yet questions remain regarding the nature of this association. For instance, when it comes to predicting health-relevant processes in daily life, few studies have examined (a) the relative importance of both positive and negative relational experiences, and (b) variability in relational experiences (in addition to mean levels). To address these gaps, we conducted a daily study (N = 4,005; ~ 30,000 observations) examining relationships, stress, and physiology in daily life. Heart rate and blood pressure were assessed using an optic sensor and integrated with an app-based study. Results demonstrated that higher mean levels of positive and lower mean levels of negative relational experiences predicted lower stress, better coping, and better physiological functioning in daily life, such as lower systolic blood pressure reactivity. Greater variability in negative (but not positive) relational experiences predicted lower stress, better coping, and lower systolic blood pressure reactivity.
An extensive body of research demonstrates that close relationships are an important contributor to physical health (e.g., Holt-Lunstad et al., 2010; Robles et al., 2014). Despite this, a number of questions remain regarding the precise nature of the link between relationships and physical health. For example, prior research has only begun to elucidate how relationships contribute to health-relevant psychological and physiological processes in everyday life (Pietromonaco, & Collins, 2017; Slatcher, & Selcuk, 2017). Moreover, although theorists have stressed the importance of both positive and negative aspects of relationships in contributing to physical health, little research has simultaneously examined how each of these aspects of relationships uniquely contribute to health-relevant processes in everyday life, especially in the context of a high-powered study which can adequately simultaneously compare the two. Finally, recent research has demonstrated that variability in relationship functioning contributes to well-being outcomes (even accounting for average levels of relationship functioning; e.g., Eller et al., 2022; Girme et al., 2018; Overall, 2020); however, little work has considered how relational variability contributes to outcomes relevant to physical well-being. In this research, we address these limitations by examining the ways in which mean levels and variability in both positive and negative aspects of individuals’ relationships predict stress, coping, blood pressure (BP), BP reactivity, and heart rate (HR) reactivity in everyday life.
Close Relationships and Physical Health: Prior Research and Outstanding Questions
How do close relationships influence physical health? Theorists suggest that positive and negative aspects of relationships engender psychological and physiological changes, which can accumulate into long-term physical health consequences (e.g., Pietromonaco & Collins, 2017; Slatcher & Selcuk, 2017; Smith & Weihs, 2019). Some prior research has indeed documented that key facets of relationships contribute to proximal psychological and biological processes (e.g., stress, emotion regulation, and immunologic and cardiovascular functioning), thereby contributing more broadly to health, with much of this work focusing on either (a) negative aspects of relationships, like conflict (e.g., Powers et al., 2006; Smith et al., 2020), or (b) social support (Bowen et al., 2014; Uchino, 2004; Uchino et al., 2018).
Despite this prior research, two recent reviews have argued that the existing literature is lacking in a few notable ways (Pietromonaco & Collins, 2017; Slatcher & Selcuk, 2017). First, despite the theoretical importance of positive relational processes in contributing to physical health, little research has examined how positive aspects of relationships (e.g., responsiveness, intimacy, and closeness) are associated with proximal psychological (e.g., stress) and physiological processes (e.g., cardiovascular functioning) that contribute to broad physical health functioning. Moreover, among the few studies that do examine how positive aspects of relationships predict biological indicators of physical well-being (e.g., Saxbe et al., 2008), these positive relational processes are often not directly compared with the challenging relational experiences (e.g., relationship conflict) that have received more attention in past literature (see Slatcher et al., 2015 for an exception). In addition, much of the prior research has focused exclusively on intimate relationships and health; although they have been studied less frequently, other types of close relationships (e.g., friendships and family relationships) also have the potential to influence the psychological and biological processes that contribute to physical health (e.g., Lu et al., 2021). Our goal in this work was to examine the links between relationship experiences and the proximal psychological and physiological processes that impact physical health using a high-powered study, which would be able to detect even small but meaningful effects of both positive and negative relational experiences when they are directly compared.
Relational Variability and Psychological and Physiological Concomitants
In addition to mean levels of relationship functioning, research in relationship science has demonstrated that when it comes to predicting key outcomes, it is important to consider variability in relationships (e.g., Arriaga et al., 2006; Campbell et al., 2010; Girme et al., 2018). For instance, researchers (e.g., Don et al., 2022; Girme et al., 2018) have drawn on the Relational Turbulence Model (Solomon & Knobloch, 2004) to suggest that greater relational variability, including variability in both positive and negative relational experiences (e.g., Don et al., 2022), may create uncertainty in the relationship, such as questions, doubts, or ambiguity about the state of the relationship. This uncertainty, in turn, theoretically contributes to greater irritations and negative emotions, thereby creating a turbulent experience for individuals in the relationship. Indeed, numerous studies have demonstrated that within-person variability (which tends to be operationalized as within-person standard deviations) in constructs such as relationship quality or attachment security tends to predicts key outcomes, even while accounting for mean levels of those same variables (Campbell et al., 2010; Eller et al., 2022; Girme et al., 2018). Generally speaking, people who report greater relational variability tend to experience maladaptive outcomes (e.g., Girme et al., 2018), although there may be some relationship behaviors or specific relationship contexts where this is not the case, and where variability may be beneficial (especially in negative relational contexts; e.g., Don et al., 2022; Overall, 2020). Consistent with this literature, relational variability may have implications for the everyday psychological and physiological responses that contribute to health (e.g., stress or BP reactivity), although little existing research has examined this possibility. A high-powered sample is particularly beneficial when studying variability because the goal is to try to detect the incremental influence of relational variability on key outcomes beyond mean levels of relational experiences.
Health-Relevant Psychological and Physiological Processes
To assess health-relevant psychological and physiological processes, we focused on self-reported and physiological outcomes: stress, coping, BP (mean levels and reactivity), and HR reactivity. Stress and coping are well-established contributors to physical well-being (Thoits, 2010) and tend to vary across the course of everyday experiences (e.g., Bolger et al., 1989). HR and BP (a) offer insight into processes that do not rely on self-reported responses and thus are less likely to be contaminated by social desirability responding, and (b) tend to vary across daily life (e.g., Uchino et al., 2006). In addition, BP and BP reactivity are related to cardiovascular disease and hypertension (e.g., Treiber et al., 2003; Vrijkotte et al., 2000), and are linked to psychological experiences (e.g., Carroll et al., 2012). While some prior research has linked relational experiences to BP and HR (e.g., Cribbet et al., 2020; Holt-Lunstad et al., 2007; Kamarck et al., 1990; Shankar et al., 2011), to our knowledge, no work has done so while simultaneously examining (a) positive and negative relational experiences, and (b) variability as well as mean levels of relational experiences in a high-powered daily study.
The Current Research
In this study, participants completed daily check-ins via their smartphone or smartwatch, which included assessments of their BP, HR, stress, coping, and (at selected check-ins) their positive and negative relational experiences, reflecting on their closest relationship. 1 We anticipated that greater mean levels of positive relational experiences and lower mean levels of negative relational experiences would be independently associated with lower stress, better coping, lower HR reactivity, and lower BP reactivity. We also expected that relational variability would be maladaptive, such that greater variability in both positive and negative relational experiences would predict greater stress, worse coping, greater BP (mean levels and reactivity), and greater HR reactivity.
The data and data analytic syntax for this study are available at the corresponding Open Science Framework (OSF) page for this study at the following address: https://osf.io/q4bth/?view_only=91bad24fc94547c8bd458b2dbdd19a2d. Materials for this article are also available at the OSF page for this study. This study was not preregistered.
Method
Participants and Procedure
We designed an ecological momentary assessment study to measure emotions, stress, and physiology via an app that could be downloaded to smartphones. Here, we present results from questions obtained once every 3 days, so from this point we use the term daily diary to emphasize the once-a-day nature of this data, as opposed to multiple momentary assessments. The app leveraged an optic sensor embedded in some Samsung phones and watches (e.g., Galaxy S9) that allowed for measurements of HR and BP (see Gordon & Mendes, 2021, for validation study). In brief, the validation article describes laboratory and field studies comparing BP and HR obtained from the optic sensor to estimates from Food and Drug Administration (FDA)-approved BP monitors (A&D UA-651BLE monitor). In laboratory studies, we observed overall correlations between the optic sensor and FDA-approved monitors of r = .78 and r = .82, for systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively, and r = .96 for HR. Critically, when comparing two FDA-approved BP monitors to each other in a small sample, we observed comparable but lower correlations than with the optic sensor, r = .75 and r = .72, for SBP and DBP, respectively, and r = .90 for HR. In field studies across 3,380 observations, we observed overall correlations of r = .70 and r = .76 for SBP and DBP, respectively, and r = .98 for HR. In contrast, two FDA-approved BP monitors showed similar correlations, r = .77 and r = .64, for SBP and DBP, respectively, and r = .90 for HR. In summary, the validity of the sensor was excellent for estimating HR and showed moderate-to-strong agreement with FDA-approved BP monitors when estimating SBP and DBP.
Participants were required to be at least 18 years old, and proficient in English. For the purpose of these analyses, participants included 4,005 people (see data cleaning strategy below for information on how we arrived at this final analytic sample). Participants were 48.12 years old on average (SD = 12.84). With respect to sex, 34.9% identified as female, 64.7% identified as male, 0.3% identified as another gender (e.g., transgender and genderfluid). With respect to race, 8.1% identified as Asian, 6.4% identified as Black or African American, 3.0% identified as Indian, 8.4% identified as Latino, 2.4% identified as Native American or Alaska native, 0.5% identified as Pacific Islander, 74.5% identified as White or European, and 1.5% declined to provide their race (participants were able to select more than one category, so the percentages do not add to 100%). The study was approved for global use and participants from across the world participated but the largest concentration of participants was from countries where we offered the app on the Google Playstore: the United States, 68.6%; the United Kingdom, 9.4%; Australia, 8.6%; Canada, 5.9%; India, 1.4%; Hong Kong, 0.7%; New Zealand, 0.05%; Singapore, 1.4%; and all other countries, 3.5%.
Once enrolled in the study, participants were sent notifications three times each day (7:00 am–10:00 am; 10:00 am–4:00 pm; and 8:00 pm–11:00 pm). During each check-in, participants first provided a sensor reading by placing their finger over the optic sensor for approximately 30 seconds. This provided information to estimate HR, SBP, and DBP. Following the sensor measurement, participants completed self-report items. At every check-in, participants received questions related to stress and coping. In addition, participants received a rotating series of additional questions that appeared during a check-in every third day, meaning that across the course of the 21-day study, participants would see each set of these additional questions up to seven times. The questions assessing participants’ relational experiences were presented during the evening check-in as part of these additional, rotating questions.
The study was designed to be 21 days long; however, participants were allowed to continue completing assessments beyond the 21-day study period if they wished to do so (and some participants did). To encourage participation, participants instantly received their BP and HR measurements. At the end of each week, they also received summary reports of their physiological responses and daily psychological experiences (e.g., stress and emotions). Data collection occurred from March 15, 2019, to December 31, 2021. The Human Research Protection Program of University of California, San Francisco approved this research.
Measures
Positive and Negative Relational Experiences
Every 3 days, participants were prompted to think about the person in their life with whom they were the closest, which could have been a spouse, friend, or family member. Positive relational experiences were assessed using four items (e.g., “To what extent did you feel satisfied with this person today?”). Negative relational experiences were assessed using three items (“e.g., Did you experience conflict with this person today?” (positive α = .94; negative α = .70; r = −.29, p < .001). 2
Physiologic Measures
At each check-in, SBP, DBP, and HR were assessed. At the start of the study, to best estimate BP, participants were encouraged to calibrate their BP value using a cuff. BP levels were only displayed to those who calibrated the sensor to an external device. Participants were able to recalibrate at any time during the study so we offset BP values by their calibration values to make sure they were equated within-person. When predicting overall BP, we only used calibrated values (81.8% of BP values were calibrated). Finally, to calculate within-person reactivity scores, we approximated baseline by identifying the check-in with the individual’s lowest HR value and subtracted the corresponding SBP, DBP, and HR from that check-in from all of their other daily check-in HR, SBP, and DBP scores (Gordon & Mendes, 2021).
Stress and Coping
At every check-in, participants responded to items about stress and coping. Participants were first presented with a question that assessed whether or not they had experienced any majorly stressful events since the previous check-in (“Have you experienced any particularly stressful events since your last check-in”). If participants answered “no” to that question (which included 83.4% of the responses), they were presented with questions that assessed their general stress (“I feel stressed, anxious, overwhelmed”) and coping (“I feel in control, coping well, on top things”) in the current moment on a scale from 1 = not at all to 5 = extremely. Because some prior research and theory emphasize the importance of examining people’s stress in relation to their perceived ability to cope with the situation (rather than examining the two separately; e.g., Mendes et al., 2007), we also examined the ratio of stress to coping as an outcome. We created a stress-to-coping ratio by dividing participants’ stress scores by their coping scores. As such, greater scores indicated a greater ratio of perceived stress relative to one’s ability to cope. 3
Data Analytic Strategy and Cleaning
Our goal was to examine how mean levels and fluctuations in positive and negative relational experiences predicted participants’ stress, coping, SBP, DBP, SBP reactivity, DBP reactivity, and HR reactivity across the check-ins in which they reported those relational experiences. We calculated within-person means and standard deviations for positive and negative relational experiences for each individual included in the study. Although standard deviations can technically be calculated with only two values, to include a reasonable range of assessments for calculating relational variability, we required that all participants complete at least three relational check-ins to be included in final analyses. For the physiological outcomes, we eliminated extreme values for SBP (<80 and >210), DBP (<50 and >180), HR (<30 and >200), body mass index (BMI) (<15 and >60), and age (>90). We also removed any BP or HR values when individuals reported exercising within 30 min of the check-in.
The data were nested, such that daily check-ins were nested within individuals, and we, therefore, utilized multilevel modeling to test our hypotheses. In particular, we constructed two-level models in which check-ins were nested within participants. All of the predictors of interest were person-level variables, and so we examined a series of random intercept models for each outcome. We first started by testing a model that included only mean levels of positive and negative relational experiences as predictors. We then tested a model that included positive and negative relational variability as additional predictors. Finally, we tested a model that included interactions between mean levels and variability as predictors of each outcome to ascertain whether variability had the same effect at differing mean levels. In the models predicting the physiological outcomes, we also included age, BMI, and sex as covariates. For each analysis, we calculated effect sizes in the form of r values for each parameter using the t-to-r transformation used by Kashdan and Steger (2006): r= √(t2/t2+df).
Among participants who completed at least three relational check-ins, the average number of check-ins was 65.51 (SD = 117.20, Max = 2,804). Mean levels (r =−.002, p = .87) and variability (r =−.004, p = .78) in positive relational experiences were not associated with the number of check-ins participants completed. Participants who had higher levels of negative relational experiences tended to complete fewer check-ins, though the effect size was small (r = .05, p < .001), but variability in negative relational experiences was not associated with the number of check-ins participants completed (r = −.003, p = .81). As is the default for multilevel modeling, participants were incorporated into analyses even if they were missing data on an outcome variable at one or more check-ins.
Because of the high degree of variability in the number of check-ins participants completed, for the primary set of analyses presented in this article, we examined only the first 100 check-ins (or up to a maximum of 14 relational check-ins). To ensure results were largely the same regardless of the number of check-ins we included in the analyses, we also re-examined these same analyses using data in which we examined (a) only the first 63 check-ins (21 days of data, the length of the original study, or up to a maximum seven relational check-ins), and (b) all check-ins participants completed (see OSM Supplemental Tables 17–32 for results, which were largely the same). Because it was necessary to remove extreme values, and filter based on variables such as age, BMI, and exercise, the analyses for each outcome variable included a slightly different number of observations (e.g., stress and coping analyses n = 29,807; SBP reactivity n = 30,458).
In addition, after conducting our primary analyses, we also tested two sets of ancillary analyses. First, we examined whether the number of check-ins that participants completed moderated the results of our primary findings. Specifically, we included number of check-ins as a moderator of the association between both mean levels and variability in positive and negative relational experiences and each of the outcomes of interest. Second, we re-conducted our primary analyses while including a series of demographic covariates, including age, BMI, socioeconomic status, and race.
Results
Descriptive statistics and bivariate correlations are presented in Table 1. As expected, higher mean levels of positive relational experiences were correlated with lower negative relational experiences (r = −.29). In addition, the higher the average positive relationship experience, the less positive relational variability (r =−.44). In contrast, those who reported higher average negative relationship experiences reported greater negative relationship variability (r =.42).
Descriptive Statistics and Bivariate Correlations for Primary Study Variables
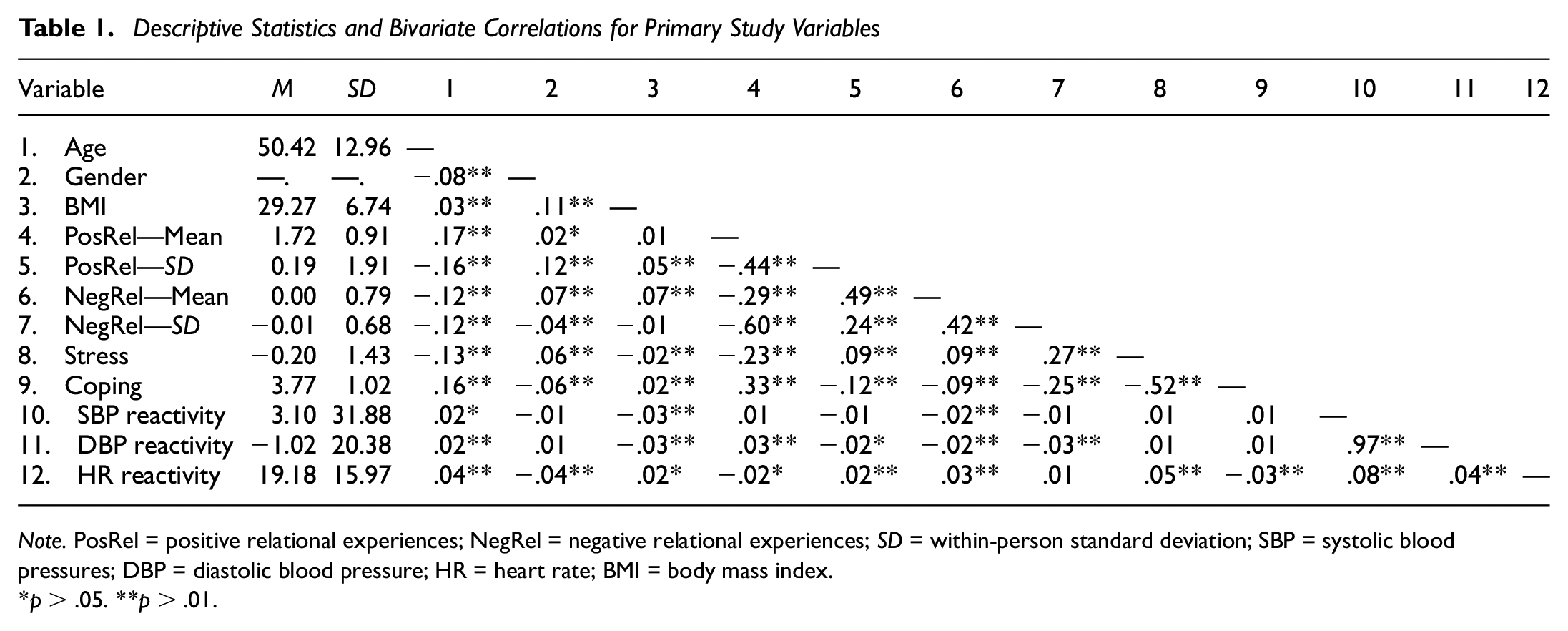
Note. PosRel = positive relational experiences; NegRel = negative relational experiences; SD = within-person standard deviation; SBP = systolic blood pressures; DBP = diastolic blood pressure; HR = heart rate; BMI = body mass index
p > .05. **p > .01.
We then examined our primary questions, and results of multilevel models examining how positive and negative relational experiences predict stress, coping, stress-to-coping ratios, BP, BP reactivity, and HR reactivity are presented in Tables 2 to 4, and in the OSM in Supplemental Tables 1 to 3. Greater mean levels of positive relational experiences were significantly associated with lower stress, better coping, a lower ratio of stress to coping, greater DBP reactivity, and lower overall SBP (but only in the first model tested, which did not include relational variability). Effect sizes for mean levels of positive relational experiences in predicting these outcomes ranged from small to moderate (r = .03–.30). With respect to main effects, greater variability in positive relational experiences only predicted a greater stress-to-coping ratio, but variability was not associated with stress, coping, or any of the physiological outcomes. The interaction between mean levels and variability in positive relational experiences was significant in predicting stress and overall SBP, and the size of this association was small. These interactions are presented in Figure 1. We probed simple slopes by examining the association between variability in positive relational experiences and (a) daily stress and (b) overall SBP at low (−1 SD) and high (+1 SD) mean levels of positive relational experiences. At high mean levels of positive relational experiences, greater variability in positive relational experiences was associated with greater daily stress (B = .04, 95% CI = [0.01, 0.08], p = .007, r = .05) and SBP (B = .83, 95% CI = [0.02, 1.66], p = .04, r = .03). By contrast, at low mean levels of positive relational experiences, the association between variability in positive relational experiences and both stress (B = −.01, 95% CI = [−0.03, 0.02], p = .65, r = .03) and SBP (B =−.18, 95% CI = [−0.82, 0.45], p = .58, r = .01) was not statistically significant. This pattern suggests that when people experienced higher levels of positive relational experiences that were accompanied by more variability (less stable positive relational experiences), they reported more daily stress and experienced greater overall SBP.
Results of Analyses Predicting Stress and Coping From Relational Experiences and Variability
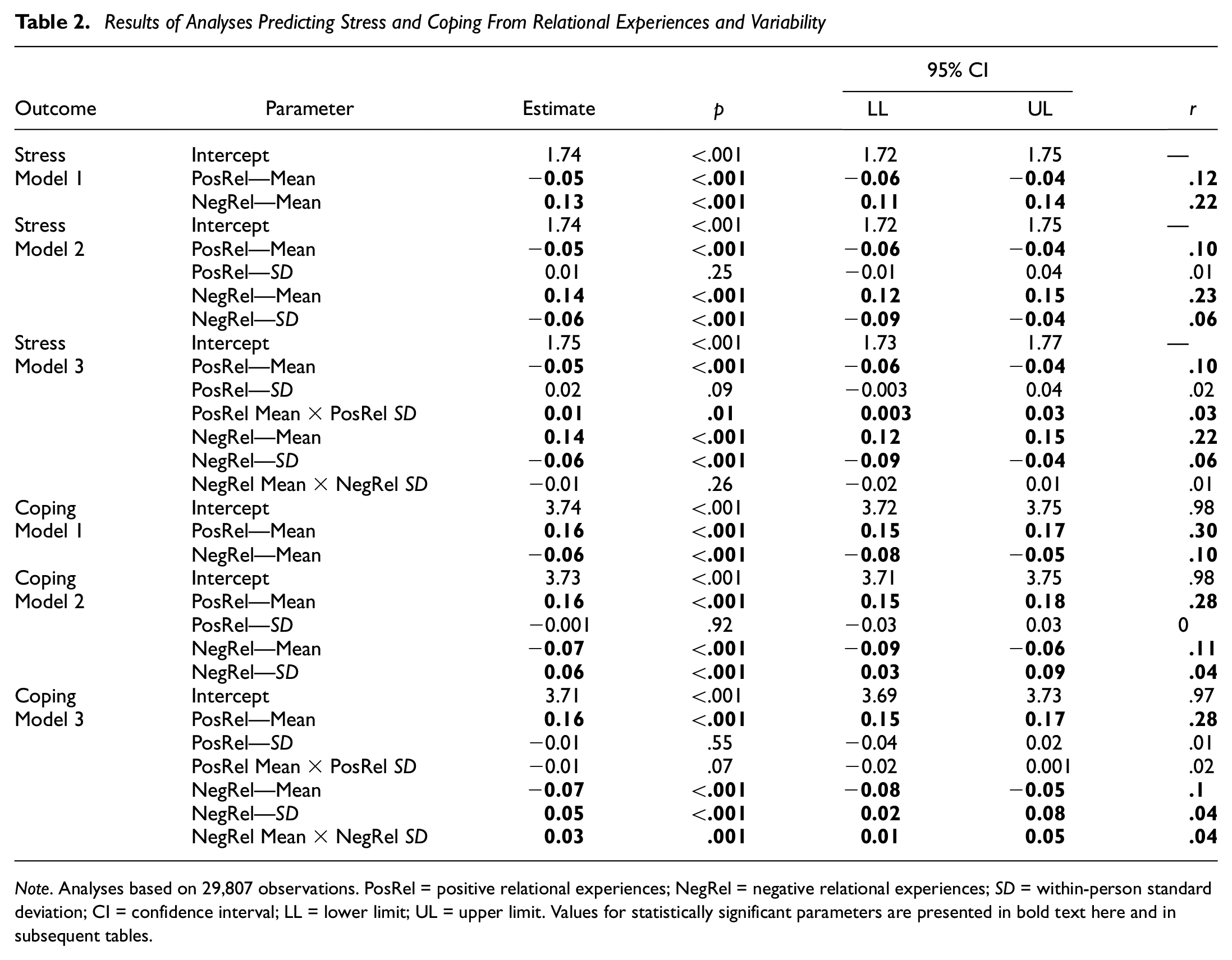
Note. Analyses based on 29,807 observations. PosRel = positive relational experiences; NegRel = negative relational experiences; SD = within-person standard deviation; CI = confidence interval; LL = lower limit; UL = upper limit. Values for statistically significant parameters are presented in bold text here and in subsequent tables.
Results of Multilevel Analyses Predicting SBP Reactivity From Relational Experiences and Fluctuations
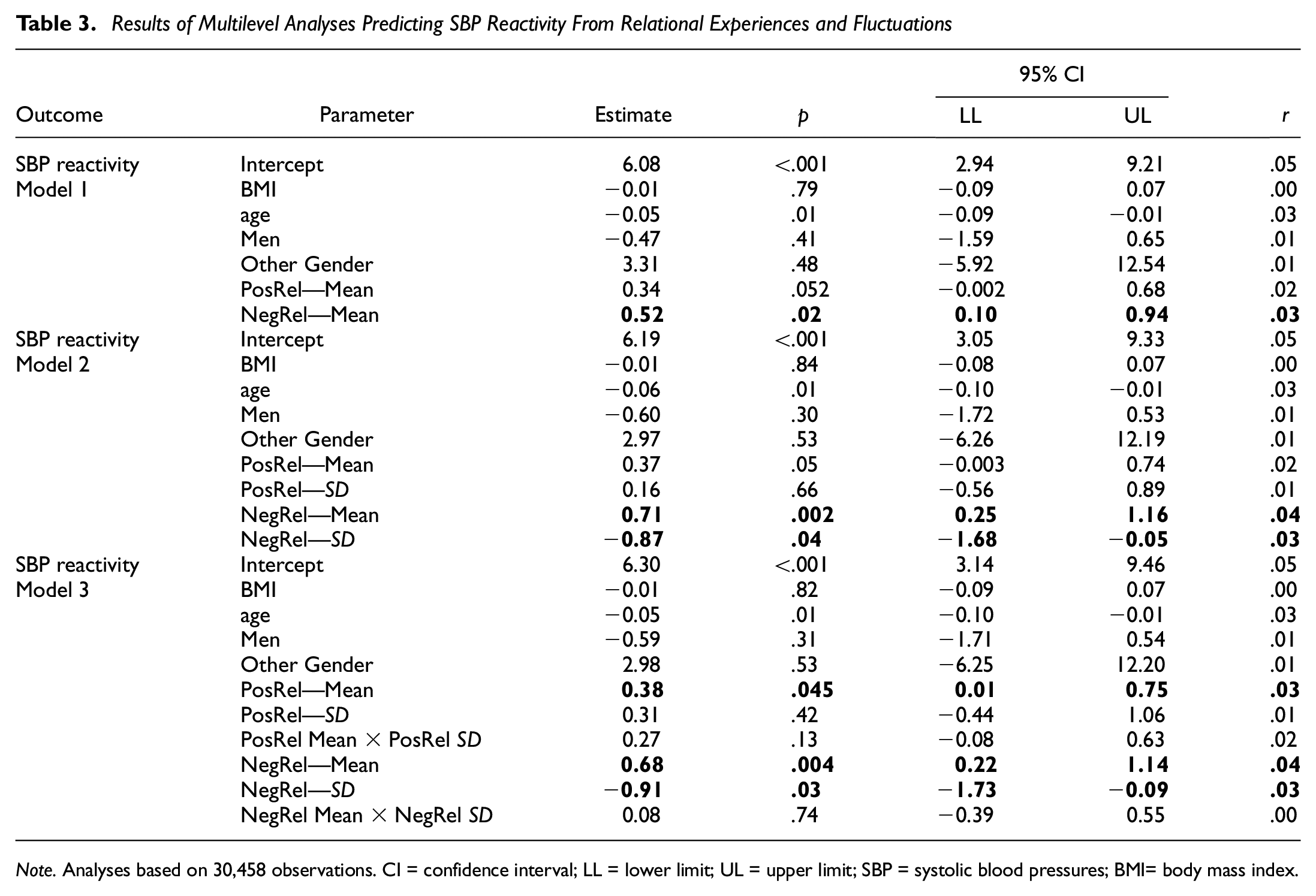
Note. Analyses based on 30,458 observations. CI = confidence interval; LL = lower limit; UL = upper limit; SBP = systolic blood pressures; BMI= body mass index.
Results of Multilevel Analyses Predicting DBP Reactivity From Relational Experiences and Fluctuations
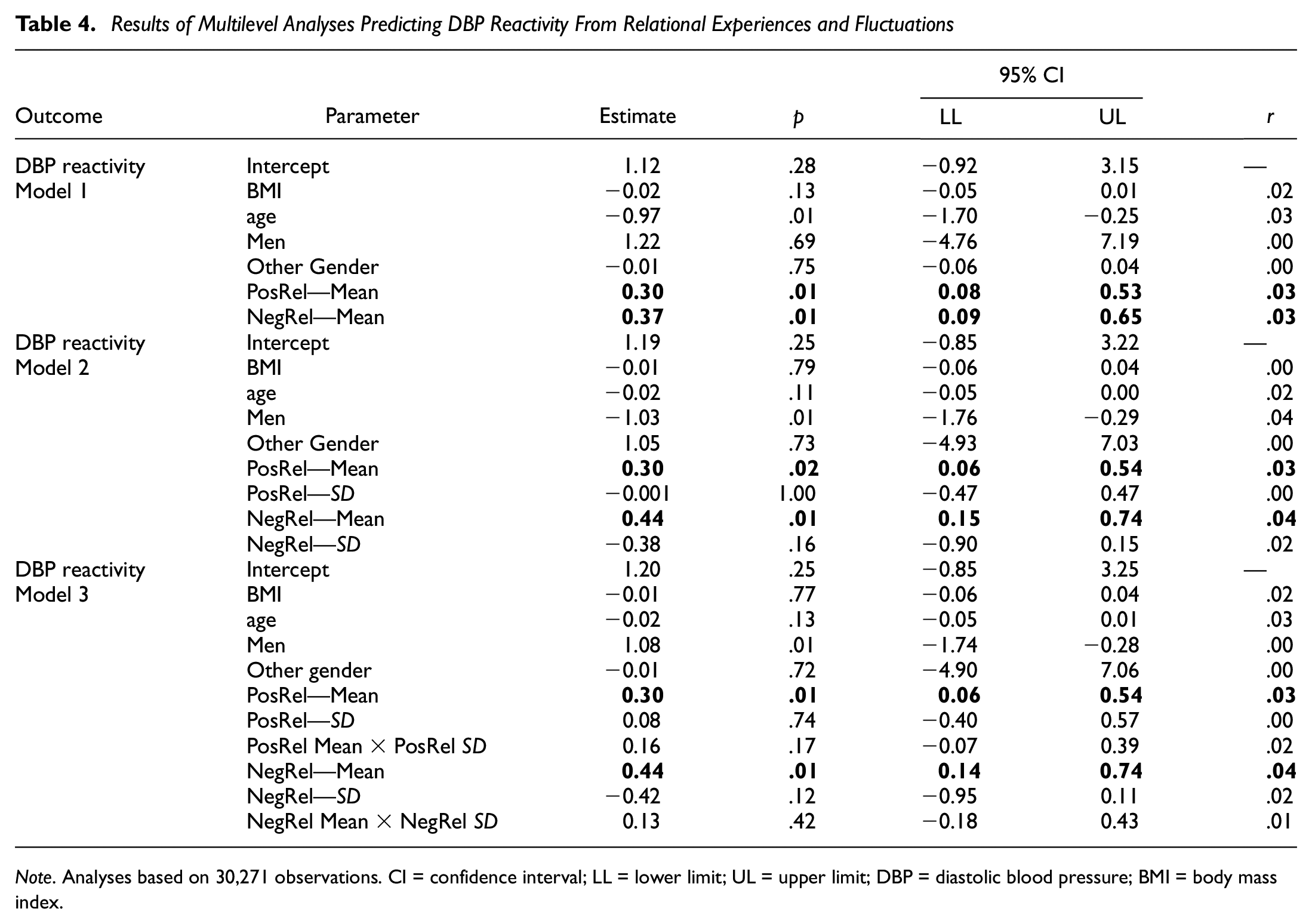
Note. Analyses based on 30,271 observations. CI = confidence interval; LL = lower limit; UL = upper limit; DBP = diastolic blood pressure; BMI = body mass index.
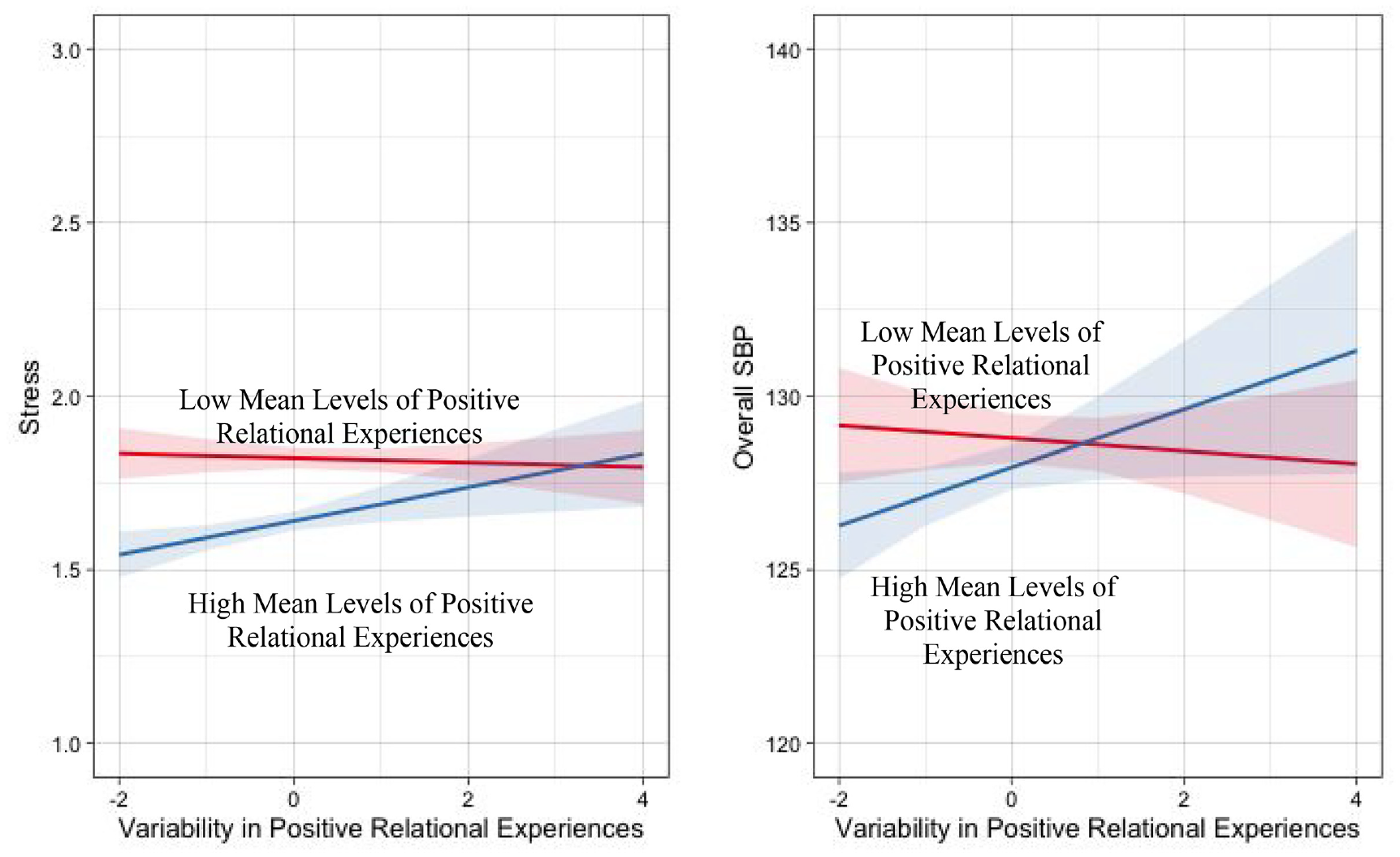
The Interactions Between Variability and Mean Levels of Positive Relational Experiences in Predicting Stress and SBP in Everyday Life
Greater mean levels of negative relational experiences were significantly associated with greater stress, worse coping, a greater stress-to-coping ratio, greater SBP reactivity, greater DBP reactivity, and greater overall DBP. Effect sizes for mean levels of negative relational experiences in predicting these outcomes ranged from small to moderate (r = .03–.23). Greater variability in negative relational experiences was associated with lower stress, better coping, a lower stress-to-coping ratio, lower SBP reactivity, and greater HR reactivity.
Effect sizes for variability in negative relational experiences in predicting these outcomes were small (r = .03–.06). The interaction between mean levels and variability in negative relational experiences were only significant in predicting coping. This interaction is presented in Figure 2, and we probed simple slopes using the same approach as above. When mean levels of negative relational experiences were high, greater variability in negative relational experiences was significantly associated with better coping (B = .10, 95% CI = [0.06, 0.14], p < .001, r = .06). In other words, higher mean levels of negative experiences were associated with better coping when there was more variability in negative relationship experiences. When mean levels of negative relational experience were low, however, variability in negative relational experiences was not associated with coping (B = .007, 95% CI = [−0.03, 0.05], p = .72, r = .001).
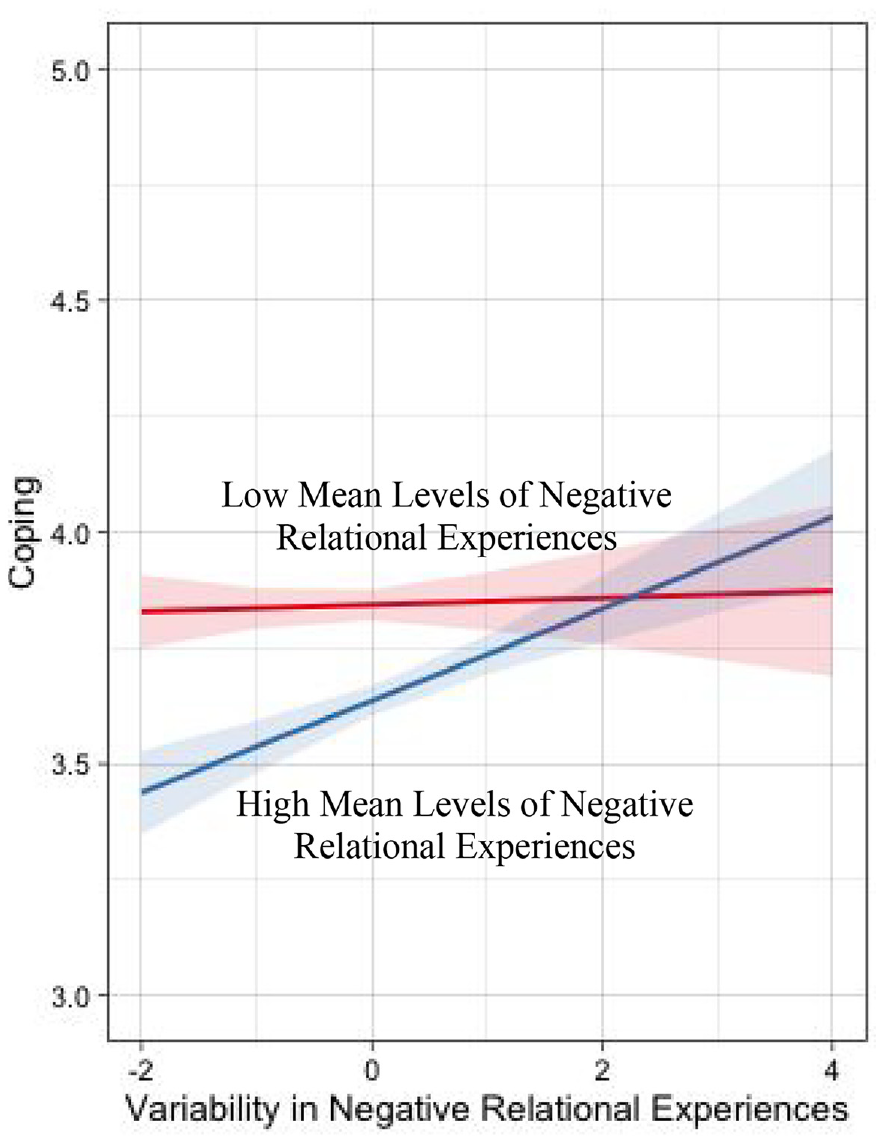
The Interaction Between Variability and Mean Levels of Negative Relational Experiences in Predicting Coping in Everyday Life
Results of analysis which (a) included a different number of check-ins and (b) included the number of check-ins each participant completed as a moderator are included in the OSM (see Supplemental Tables 4–32). Results of these analyses were largely the same as the ones presented above, suggesting the number of check-ins participants completed did not have a large influence on the overall pattern of findings.
Results of analyses in which we controlled for gender, age, BMI, socioeconomic status, and race for all outcomes are included in Supplemental Tables 33 to 47. Results of these analyses were nearly identical as those presented in our primary analyses, suggesting that inclusion of demographic covariates did not substantially alter our findings.
General Discussion
We drew on a highly powered study that implemented an app-based research approach to examine how positive and negative relational experiences predicted stress, coping, BP, BP reactivity, and HR reactivity in daily life. With respect to psychological outcomes, we observed that (a) greater mean levels of positive and lower negative relational experiences predicted lower self-reported stress and better coping in daily life, and (b) greater variability (i.e., less stability) in negative (but not positive) relational experiences consistently predicted lower stress and better coping. With respect to physiological outcomes, mean levels of both positive and negative relational experiences were associated with participants’ physiological experiences in daily life, such that negative relationship experiences predicted a maladaptive physiological profile (greater SBP reactivity, greater DBP reactivity, and greater overall DBP), whereas positive relational experiences predicted greater SBP reactivity but lower HR reactivity. In addition, we also found evidence of an interaction between mean levels and variability in relational experiences in predicting stress, coping, and overall SBP, such that the influence of variability depended on context. Implications of these results are discussed below.
Numerous researchers have recently called for a better understanding of the mechanisms by which close relationships influence health (e.g., Farrell & Stanton, 2019; Sbarra & Coan, 2018; Slatcher & Selcuk, 2017). In the current research, although we did not directly test for mediation between the health-relevant daily processes and long-term health outcomes (e.g., disease diagnosis or mortality), our results shed light on some unanswered questions in this literature. In particular, our results suggest that (a) mean levels of both negative and positive relational contribute to health-relevant psychosocial (stress and coping) and physiological (BP and HR) processes in daily life (depending on the specific outcome of interest), but that (b) negative relational variability is more consistently linked with these outcomes in daily life than positive relational variability. Only one prior study, to our knowledge, had included both positive and negative aspects of relational experiences in a study examining health-relevant outcomes (Slatcher et al., 2015), so it was heretofore unclear whether relational positivity or negativity would be most influential. Our results clarify this work by suggesting that both positive and negative relational experiences clearly matter.
One of the primary novel contributions of this research is in extending the nascent research examining relational variability to the domains of stress, coping, and physiology. Critically, prior research examining relational variability was inconsistent, with some studies suggesting relational variability was associated with maladaptive outcomes (Arriaga et al., 2006; Campbell et al., 2010; Girme et al., 2018), while others studies suggesting it was associated with mixed or beneficial outcomes (Don et al., 2022; Overall, 2020). In this work, people who reported greater variability in their negative relational experiences reported lower stress, better coping, and lower SBP reactivity. Consistent with the work of Overall (2020), one possible explanation for this pattern of findings is that variability in negative relational experiences specifically may be beneficial, because negative experiences like conflict can be detrimental if consistent throughout one’s life. As such, consistency or stability in negative relational experiences may be maladaptive because it represents an inability to respond flexibly to the demands of the situation (Overall, 2020). More broadly, our work extends the literature by demonstrating that it is not just mean levels of negative relational experiences that contribute to health-relevant processes in daily life, but that relational variability also matters. 4 Given that we only examined a few outcomes in this work, future research is needed examine how relational variability contributes to other psychosocial, physiological, and behavioral factors that contribute to physical health.
It is important to consider the size of the effects we identified, and whether they are practically meaningful. Generally speaking, the effect sizes for mean levels of relational experiences were stronger in predicting the outcomes of interest than variability in relational experiences. Moreover, relational experiences tended to be a stronger predictor of stress and coping than the physiological outcomes we examined. Despite generally small effect sizes, we believe these findings are practically meaningful. For instance, throughout our analyses, we found a small but consistent effect: That negative relational experiences tended to predict a maladaptive cardiovascular profile in everyday life. Although this effect is small, to the extent that negative relational experiences contribute to elevated BP throughout everyday life, across the course of time this maladaptive cardiovascular profile associated with negative relational experiences may accumulate into long-term physiological harm, or negative health outcomes (e.g., Götz et al., 2022).
Limitations and Constraints on Generality
This study is not without limitations. First, while our sample was drawn from across the world, three-quarters of the participants were White individuals, and over two-thirds were from the United States. As such, our sample is not representative of most relationships globally, and because our goal is to derive conclusions about the general link between relationships and health, this work requires replication among samples with more ethnic, sociodemographic, and geographic diversity. Second, our results are correlational, and bidirectionality is possible in our findings: For instance, prior research demonstrates that stress influences relationship processes (e.g., Neff & Karney, 2009). While the goal of this work was to identify the plausible ways in which relationships connect to health-relevant processes in daily life, future research is needed to causally test (a) directionality and (b) the precise mechanisms by which relationship influence physical health. Third, participants in this study received feedback on their physiology throughout the course of the study, and it is possible that this type of feedback influenced their behavior or subsequent physiology. We do feel, however, that this type of physiological feedback is unlikely to influence the association between aggregated relational experiences and the outcomes we examined, but this facet of our study design must be considered when generalizing these results to the general population. Finally, we also note that there were large number of people in this study who did a small number of check-ins, although in supplemental analyses we found check-in number did not meaningfully influence the results.
Conclusion
We forged new ground by examining how mean levels and variability in relational experiences predicted psychological and physiological processes in daily life that are relevant to physical health. The quality of our relationships can determine who lives and dies; this research points to some pathways through which relationships may contribute to or undermine physical health.
Supplemental Material
sj-docx-1-spp-10.1177_19485506231156018 – Supplemental material for The Good, the Bad, and the Variable: Examining Stress and Blood Pressure Responses to Close Relationships
Supplemental material, sj-docx-1-spp-10.1177_19485506231156018 for The Good, the Bad, and the Variable: Examining Stress and Blood Pressure Responses to Close Relationships by Brian P. Don, Amie M. Gordon and Wendy Berry Mendes in Social Psychological and Personality Science
Footnotes
Correction (April 2023):
This article was updated to add in the Methods section that The Human Research Protection Program of University of California, San Francisco approved this research and to include the reference citation for Gordon & Mendes, 2021.
Handling Editor: Richard Slatcher
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by NIA (R24AG048), NIMH (T32MH019391), and Samsung LTD.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.