
Abstract
Purpose
To compare the clinical and biological outcomes of minced autologous cartilage transplantation versus hyaluronic acid–based scaffold with bone marrow aspirate concentrate (HA-BMAC) in the treatment of full-thickness cartilage lesions of the knee.
Methods
A total of 41 patients treated with minced autologous cartilage transplantation were retrospectively analyzed. Using propensity score matching, a control group of 41 patients was selected from a large cohort treated with HA-BMAC-based cartilage repair. Minced cartilage was harvested from unloaded cartilage and fibrin-glued into the defect. Bone marrow aspirate concentrate (BMAC) was obtained from the iliac crest, centrifuge concentrated, and seeded onto a hyaluronic acid scaffold. Clinical outcomes were assessed using the Knee Injury Outcome Score (KOOS) score. Magnetic resonance imaging (MRI) evaluations were performed preoperatively with AMADEUS score and at 1-year follow-up using the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART)-2 score.
Results
The groups were comparable in terms of age, sex, lesion size, and location. Significant improvements were observed in all KOOS subscales in both cartilage repair groups, with no statistical difference between them at 1-year follow-up. MOCART-2 scores showed a trend toward superior biological healing in the minced cartilage group (mean score: 77) compared to the BMAC group (mean score: 73). Excellent healing (MOCART >80) was observed in 51% of minced cartilage cases versus 38% of BMAC cases.
Conclusion
Both minced cartilage transplantation and HA-BMAC treatments resulted in comparable subjective clinical outcomes. However, minced cartilage transplantation demonstrated a tendency for enhanced biological healing based on MRI compared to HA-BMAC. This suggests potential advantages of minced cartilage transplantation over HA-BMAC cartilage repair.
Keywords
Introduction
Single-stage cartilage repair procedures have emerged as an appealing option due to their potential cost-effectiveness and the reduced burden of requiring only one surgical intervention, as opposed to autologous chondrocyte implantation (ACI).1 -3 Minced cartilage transplantation, as a single-stage cartilage repair technique, has evolved over the last 15 years, with both preclinical and clinical data suggesting that the technique can provide effective cartilage repair with high levels of hyaline cartilage formation, as well as significant improvements in clinical outcomes.4 -8 Another 1-step repair technique involves the use of multipotent cells derived from bone marrow aspirate concentrate (BMAC), combined with biological scaffolds. BMAC-based cartilage repair has demonstrated promising short- to mid-term clinical outcomes, with recent reports suggesting that BMAC-based treatment using a hyaluronic acid–based scaffold seeded with bone marrow aspirate concentrate (HA-BMAC) can yield encouraging long-term results. 9 Small case series have shown sustained clinical improvement for up to 14 years.10 -14
The outcomes of the HA-BMAC technique have been compared to those of microfracture-based marrow stimulation, with findings indicating better and more sustained subjective outcome improvements following the HA-BMAC procedure. 15 HA-BMAC outcomes have also been compared to those of ACI, with comparable subjective outcome improvements observed. These results have been reported in the management of both large chondral defects and lesions involving osteochondral tissue. 16
However, minced cartilage transplantation lacks comparative studies to identify potential benefits over other cartilage repair methods. One systematic review of HA-BMAC-based cartilage repair concluded that scientific evidence supporting the clinical benefit of the technique remains limited and that larger, comparative, and higher-quality clinical studies are needed. 17 There remains, therefore, a critical need for comparative studies of these recently introduced 1-step cartilage repair techniques to assess their relative clinical and biological efficacy in cartilage repair.
The present study aimed to compare clinical outcomes and biological cartilage repair responses of 2 one-step cartilage repair techniques for the treatment of full-thickness cartilage lesions in the knee: minced cartilage transplantation and HA-BMAC. It was hypothesized that minced cartilage transplantation would result in better cartilage repair tissue formation than HA-BMAC, as evidenced by magnetic resonance imaging (MRI)-based healing responses.
Material and Methods
Study Design
This study was designed as a single-center comparative analysis of 2 retrospective treatment cohorts. Consecutive patients who underwent cartilage repair using either minced cartilage transplantation or the HA-BMAC technique between 2013 and 2024 were identified from a prospectively maintained institutional database, which captured validated patient-reported outcomes and routine postoperative MRI assessments. Demographic, surgical, and imaging data were extracted from electronic medical records. Ethical approval was obtained from the regional ethics committee (ID: 1-45-70-118-24).
Patient Selection
Inclusion criteria were (1) a minimum of 12 months of clinical follow-up, (2) focal full-thickness chondral defects ≥1 cm2 classified as grade IV by the International Cartilage Repair Society (ICRS), located on the patella, trochlea, or femoral condyle, (3) age between 18 and 40 years, and (4) body mass index (BMI) between 20 and 30 kg/m2. Concomitant procedures were performed as indicated, including high tibial osteotomy, tibial tubercle osteotomy, anterior cruciate ligament (ACL) reconstruction, and medial patellofemoral ligament (MPFL) reconstruction. Exclusion criteria included multiple prior intra-articular corticosteroid injections, osteonecrosis, tricompartmental knee osteoarthritis, neurovascular pathology, or any systemic illness.
Surgical Technique
Minced Cartilage Transplantation
A medial or lateral mini-arthrotomy approach was used, and the lesion was inspected and measured. The defect was debrided with a curette until a stable, healthy cartilage rim was obtained. The hyaline cartilage harvested from the debrided material was collected and minced into small fragments (approximately 1 mm) using a scalpel or a shaver with a collective filter (Graftnet, Arthrex, Naples, Florida). If an insufficient amount of cartilage was harvested, additional healthy cartilage was obtained from the intercondylar notch using curved osteotomes. The minced cartilage was then placed into the defect and sealed with fibrin glue or a combination of fibrin glue and a membrane (Hyalofast, Anika Pharma, Frankfurt, Germany). 6 In cases of osteochondral lesions requiring bone transplantation, trabecular bone cylinders were harvested from the proximal tibia, fragmented into bone chips, and impacted into the osseous defect to restore the subchondral bone level.
Hyaluronic Acid–based Scaffold with Bone Marrow Aspirate Concentrate Technique
The operative extremity and ipsilateral iliac crest were prepared in a sterile fashion. Diagnostic arthroscopy confirmed eligibility for HA-BMAC–based cartilage repair and allowed for the treatment of associated pathologies. A 20-mL bone marrow aspirate was harvested from the ipsilateral iliac crest using a standardized aspiration system and then processed in a commercially available centrifugation device (BioCUE Bone Marrow Aspirate Concentration System; Biomet, Warsaw, Indiana), yielding 2 to 4 mL of nucleated cell–rich BMAC. A mini-arthrotomy was performed to expose full-thickness chondral lesions. Unstable cartilage was removed, and lesion borders were shaped to stable vertical margins. The defect base was uniformly debrided to remove the calcified cartilage layer without breaching the subchondral plate. A hyaluronic acid–based fibermesh scaffold (Hyalofast; Anika Therapeutics, Bedford, Massachusetts) was trimmed to match the defect size, saturated with BMAC concentrate, and allowed to soak for 5 to 10 minutes. The BMAC-loaded scaffold was then fixed to the defect bed using fibrin glue (Tisseel; Baxter, Deerfield, Illinois), followed by an additional superficial layer for final fixation. After a 5-minute polymerization period, the knee was cycled through full flexion–extension under direct visualization to confirm construct stability. Osteochondral lesions were managed in the same manner as described for minced cartilage transplantation. 18
Postoperative Rehabilitation
A standardized rehabilitation protocol was used for all patients. A hinged brace limited the range of motion (ROM) to 0–20° for the first 2 weeks:
Patellofemoral lesions: Partial weightbearing with crutches was allowed for 2 weeks, followed by gradual ROM progression and full weightbearing from weeks 3–6.
Tibiofemoral lesions: Partial weightbearing was permitted for 6 weeks, with unrestricted ROM allowed after 2 weeks. Quadriceps strengthening commenced at week 6, and stationary cycling began at week 8.
All patients underwent physiotherapist-supervised rehabilitation for 12 weeks.
Clinical Outcome Measures
Patient-reported outcomes were collected preoperatively at 12 months using the KOOS (Knee Injury Outcome Score) that consists of 5 subscores investigation symptoms, pain, activities of daily living (ADL), sports, and quality of life, each ranging from 0 to 100, with 0 being the poorest outcome. 19
A semi-quantitative global clinical outcome assessment was recorded at 12 months and categorized as:
A: Symptom-free knee with high functional level.
B: Significant symptom improvement with occasional activity-related pain or swelling.
C: Limited improvement with persistent symptoms restricting function.
Postoperative complications and reoperations were documented.
Magnetic Resonance Imaging Evaluation
Preoperative 3-T MRI scans were assessed using the AMADEUS (Area Measurement and Depth and Underlying Structures) scoring system to quantify chondral and osteochondral defect severity. 20 Intraoperative cartilage injury severity grading was performed according to the ICRS (International Cartilage Repair Society) grading system. 21 Hyaline cartilage or repair tissue was analyzed using the MOCART-2 system (Magnetic Resonance Observation of Cartilage Repair Tissue), which semi-quantitatively evaluates seven individual aspects of cartilage repair. MRI scans for MOCART scoring were obtained at 12 months postoperatively. 22
Statistical Analysis
To control for selection bias and confounding factors, the cohorts were matched using propensity scores.23,24 A propensity score was calculated for each patient using logistic regression with the following independent variables: age, sex, cartilage lesion size, and previous surgery in the index knee. The cohorts were matched 1:1 using nearest-neighbor matching with a caliper of 0.1. Baseline variables were compared using standardized mean differences (SMDs), with SMD < 0.1 indicating balanced variables.
A power analysis was performed for the MOCART-2 score outcome. There is no defined minimal clinical important difference (MCID) for MOCART-2 score so this was set to a 10-point difference for group comparison in the present study. With a standard deviation for the MOCART-2 score of 11 points, an MCID of 10 points, a power of 0.8, and an alpha of 0.05, power analyses revealed needed group sizes of 19 patients to ensure detection of a 10 point difference in MOCART score. Continuous variables were summarized as mean ± standard deviation. Categorical variables were reported as median and range. AMADEUS and MOCART-2 scores were presented as mean ± standard deviation. Changes in KOOS subscores from baseline to follow-up were analyzed using 2-tailed paired t-tests. Comparison of MOCART-2 scores between anatomical locations was analyzed using 2-tailed paired t-tests. Comparison of high-level MOCART-2 scores (>80) was analyzed using the Chi-square test. A P-value < 0.05 was considered statistically significant. Analyses were performed using STATA version 18 (StataCorp, College Station, Texas).
Results
A total of 41 patients treated with minced cartilage transplantation and 41 patients in a matched cohort treated with HA-BMAC-based cartilage repair were included. Patient demographics, previous surgeries, and concomitant procedures are summarized in
Patient Characteristics, Previous Surgeries, and Concomitant Surgical Procedures.

BMI = body mass index; MPFL = medial patellofemoral ligament reconstruction; OAT = autologous osteochondral transplantation; OCD = osteochondritis dissecans; TTO = tibial tuberosity osteotomy; ACL-R = anterior cruciate ligament reconstruction.
Cartilage Lesion Characteristics.
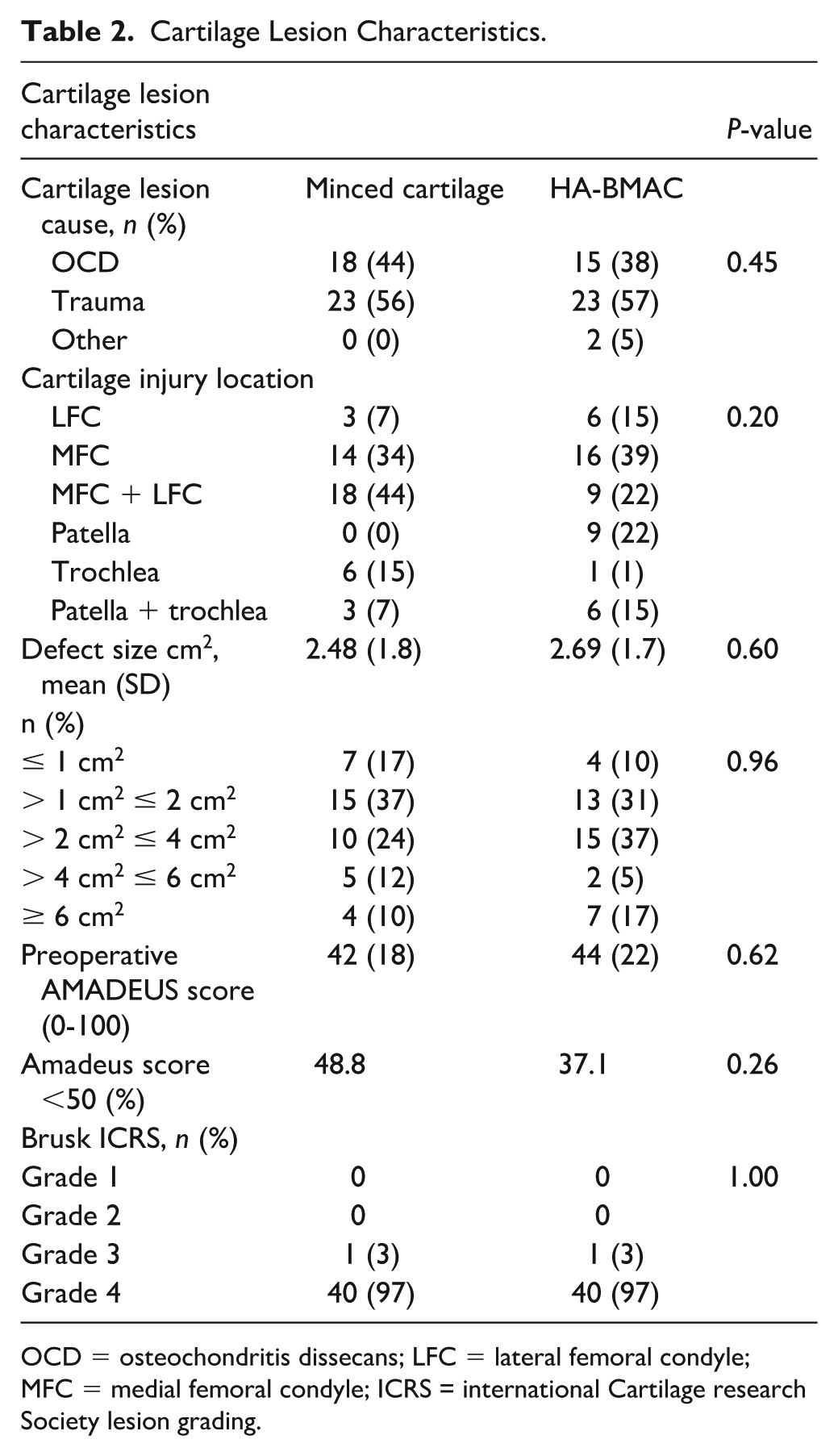
OCD = osteochondritis dissecans; LFC = lateral femoral condyle; MFC = medial femoral condyle; ICRS = international Cartilage research Society lesion grading.
Patient-Reported Outcomes
Completeness for KOOS scores was 30%. Significant improvements were observed across all KOOS subscales from baseline to 12-month follow-up in both the minced cartilage and HA-BMAC groups, with median score increases ranging from 6 to 34 points—exceeding the established minimal clinically important difference for each subscale. The greatest improvements were seen in KOOS–ADL (+30 points) and KOOS–Symptoms (+25 points). Detailed KOOS results are shown in
Patient-Reported Outcomes Based on KOOS Scores—(A) demonstrates preoperative and 1-year follow-up scores for both minced cartilage and HA-BMAC cohorts and (B) demonstrates 1-year follow-up scores for both minced cartilage and HA-BMAC cohorts.

Radiological Outcomes
Preoperative lesion severity, assessed using the AMADEUS score, showed a mean score of 42 for the minced cartilage group and 44 for the HA-BMAC group, indicating substantial baseline cartilage lesion severity.
Seventy-two out of the 82 patients (88%) completed the 1-year follow-up MRI evaluation. The mean MOCART-2 score at 12-month follow-up was 77.4 for the minced cartilage group and 73.3 for the HA-BMAC group, with a tendency for better MOCART scores in the minced cartilage group (P = 0.08). MOCART-2 subclass analyses revealed significantly better scores for defect filling, bone defect healing, and subchondral changes in the minced cartilage group compared to the HA-BMAC group (
MOCART Scores at 1-Year Follow-up.

Complications and Reoperations
A total of 5 patients (12%) underwent reoperation following the minced cartilage procedure. All 5 cases were due to cartilage graft hypertrophy, which was managed with arthroscopic debridement. A total of 9 patients (22%) underwent reoperation following the HA-BMAC procedure. Seven of the reoperations were due to graft hypertrophy (17%), which was treated with arthroscopic debridement. One case of localized synovitis occurred, treated with arthroscopic synovectomy, and 1 case involved tibial cystic formation related to an ACL reconstruction, which was treated with screw removal and allograft bone transplantation.
Discussion
The primary finding of this study was that cartilage repair with minced cartilage transplantation demonstrated slightly better biological cartilage healing responses than HA-BMAC-based cartilage repair, as assessed by MRI healing scores. A secondary finding was that subjective outcomes were similar between the 2 cartilage repair groups.
This is the first study to compare minced cartilage repair with HA-BMAC and scaffold-based cartilage repair methods, with the interesting finding of favorable healing responses for the minced cartilage technique, particularly regarding defect filling, bone defect healing, and subchondral normalization. Minced cartilage transplantation has been compared to microfracture in a matched cohort study design like the present study. This study found similar outcomes regarding subjective results using the international knee documentation commitee (IKDC) subjective score and similar reoperation rates. 25 In another matched-pair study, minced cartilage transplantation, ACI with matrix-induced autologous chondrocyte implantation (MACI) technique, and microfracture with collagen scaffold (autologous matrix-induced chondrogenesis [AMIC]) technique were investigated in 16 patients per repair technique group. This study found similar subjective outcomes for the 3 cartilage repair techniques. 26 These results confirm the findings of the present study, with no difference between minced cartilage repair and another advanced repair technique regarding subjective outcome improvements. However, neither of the 2 studies mentioned included systematic imaging data for the evaluation of healing responses, as in the present study.
Autologous minced cartilage transplantation has been investigated in several studies by Saltzman et al.7,8 They found overall MOCART-2 scores improving from 64 to 70 between 2 and 5 years of follow-up. The MOCART-2 score of 77 at 12 months in the present study for minced cartilage transplantation confirms these previous findings of good repair tissue properties with minced cartilage transplantation. A potential biological reason for the better cartilage repair response could be that minced cartilage provides viable hyaline tissue directly into the cartilage defect. This tissue has been shown to survive over time during the healing process and contribute additional chondrocytes to the repair tissue through outgrowth from the minced cartilage fragments.6,27
HA-BMAC–based cartilage repair requires bioactive cells to act through humoral activation pathways to create a healing response, working synergistically with synovial, perichondral, and subchondral cells. These more complex interactions can challenge the tissue repair response compared to the transplantation of fully differentiated cartilage tissue, as seen with minced cartilage transplantation. 8
Previous studies comparing HA-BMAC have evaluated outcomes with both microfracture and ACI. In a study by Gobbi et al., 25 HA-BMAC repairs and 25 microfracture repairs were compared. The study found that HA-BMAC-based repair had better subjective Patient-Reported Outcome Measure (PROM) scores, which were also maintained over time, compared to microfracture-based repairs. 15 Another study comparing HA-BMAC and ACI found nearly identical subjective outcome improvements and MRI-based healing responses. 16 These findings suggest that HA-BMAC-based cartilage repair may be superior to microfracture-based repair and comparable to ACI-based repair.
A potential negative impact of previous cartilage repair procedures such as microfracture on the outcome after subsequent cartilage repair procedures is known to exist. 28 In the present study, a proportion of 12% and 22% patients in both the HA-BMAC and the minced cartilage group, respectively, had previous microfracture treatment. This is a relatively even distribution of this potentially negatively influencing previous procedure. This differential effect of previous microfracture is therefore expected to be limited in the present study. Also, concomitant procedures in combination with the present cartilage repair procedures could impact outcomes due to increased surgical morbidity. In the present study, the primary concomitant procedure was autologous bone transplantation performed in cases with significant bony defects in combination with the cartilage lesion. In the present study, proportion of 34% and 41% patients in the HA-BMAC and the minced cartilage group, respectively, had concomitant bone transplantation treatment. Also, a small proportion had femoral or tibial osteotomy for alignment corrections. There were 4% and 2% patients in the HA-BMAC and the minced cartilage group, respectively. This is a relatively even distribution of concomitant procedures. So, it is not expected to influence to impact the comparative outcome in a severely negative way.
The separate impact of the hyaluronic acid scaffold for the overall cartilage repair response is difficult to assess. A study by Tan et al. investigated isolated implantation of a hyaluronic acid scaffold as an isolated cartilage repair technique in 46 patients with grade 4 cartilage lesions. This study found clinically relevant improvement in KOOS scores that were similar to the improvements found in the present study for KOOS pain and symptoms but not as good as those found for KOOS sport and KOOS quality of life. No overall imaging data were presented in that study. This comparison indicated that a hyaluronic scaffold implantation alone for cartilage repair can provide clinically relevant subjective outcome improvement, but the combination of scaffold and minced cartilage results in better overall subjective outcome improvement including sports function and quality of life. 29 The separate impact of minced cartilage transplantation has been investigated in studies by Saltzman et al.7,8 as mentioned above. They found MOCART-2 scores at 70 between 2 and 5 years of follow-up. The MOCART-2 score of 77 at 12 months in the present study for minced cartilage transplantation with a scaffold suggests a slightly better healing response with the combined minced cartilage and scaffold. But the difference is marginal, so overall isolated minced cartilage can result in a significant cartilage repair response that is not necessarily further improved by a scaffold addition.
In the present study, the primary complication was cartilage graft overgrowth, which resulted in reoperation for overgrowth debridement in 12% of cases with minced cartilage transplantation and 17% of cases treated with HA-BMAC. Thus, a slightly higher incidence of this complication was seen with HA-BMAC compared to minced cartilage transplantation. Gobbi et al. 9 reported no reoperations due to graft hypertrophy, but failure rates requiring revision were observed in 13% of HA-BMAC cases, whereas no failures requiring revision were seen in the present study for HA-BMAC. Previous studies on minced cartilage transplantation have shown graft overgrowth in 4% of cases, 7 which was lower than the 12% finding in the present study. However, the 4% finding was based on a smaller case series of 23 patients, which adds some statistical uncertainty to the estimate. Nonetheless, graft hypertrophy remains the primary complication for any advanced cartilage repair method and has also been observed in ACI as another cell-based cartilage repair technique, with an incidence of 25%. 30
The clinical implications of the present study suggest that minced cartilage transplantation demonstrates favorable cartilage repair healing responses that are superior to the HA-BMAC cell-based cartilage repair technique. This could indicate that minced cartilage transplantation is a clinically valid cartilage repair method that can be more widely used due to its consistently good outcomes, both regarding subjective outcomes and cartilage lesion healing responses.
The most significant strength of this study is its comparative design using a propensity-matching method to obtain a clinically relevant control group for the minced cartilage transplantation cohort. Another strength was that nearly all patients had MRI cartilage repair evaluations at 1-year follow-up, allowing for better imaging-based biological healing response evaluations.
This study has some limitations. The completeness of patient-reported outcomes was low, which necessitates careful evaluation of these PROM parameters. In addition, MRI data for cartilage repair tissue do not evaluate the biomechanical structural integrity of the tissue or the histological tissue composition. This could result in MRI-based analyses classifying the cartilage repair tissue as having better quality than the true structural integrity of the repair tissue.
Conclusion
Both minced cartilage transplantation and HA-BMAC treatments resulted in comparable subjective clinical outcomes. However, minced cartilage transplantation demonstrated a tendency for enhanced biological healing compared to HA-BMAC, as evidenced by MRI, suggesting potential advantages of minced cartilage transplantation over HA-BMAC-based cartilage repair.
Footnotes
Ethical Considerations
Ethical approval was obtained from the regional ethics committee (ID: 1-45-70-118-24).
Consent to Participate
Informed consent for medical file data retrieval was excepted by regional ethics committee (ID: 1-45-70-118-24).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded entirely by the Orthopedic Department at Aarhus University Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Aggregated data are available from the corresponding author. Individual patient data are not available due to the ethical data transfer rules at Aarhus University Hospital.