
Abstract
Aims
Precise evaluation of cartilage damage is essential for the better management of osteoarthritis and treatment of articular cartilage. For accurate evaluation of cartilage damage, direct visual and/or histological assessment of articular cartilage is preferred over radiological or magnetic resonance imaging (MRI) imaging. This study aimed to determine whether, and to what extent, visual macroscopic grading using International Cartilage Repair Society (ICRS) system correlates with microscopic evaluation using the Osteoarthritis Research Society International (OARSI) histopathological scoring in an ex-vivo setting.
Methods
A total of 70 articular cartilage sections obtained from 19 osteoarthritic human knees were macroscopically classified using the ICRS grading system and subsequently evaluated histologically using the OARSI scoring system. Spearman’s correlation and bivariate linear regression analyses were performed to assess the association between ICRS and OARSI scores. The reproducibility, reliability, and inter- and intra-observer consistency of the OARSI scoring were further evaluated using Bland-Altman analysis, correlation coefficients, Cohen’s kappa, Cronbach’s alpha, and intraclass correlation coefficients (ICC).
Results
Qualitative assessment revealed a progressive increase in OARSI histological scores corresponding to higher ICRS grades. Spearman’s correlation and regression analyses demonstrated a weak positive correlation between visual ICRS grading and histological OARSI scoring in early-stage lesions (ICRS grades 0-I; n = 29, r = 0.592, R² = 0.350, p < 0.001), a moderate correlation with the inclusion of moderate-stage lesions (ICRS grades 0-II; n = 47, r = 0.603, R² = 0.364, p < 0.001), and a strong correlation when severely degenerated cartilage was included (ICRS grades 0-III; n = 67, r = 0.811, R² = 0.657, P < 0.001). The analysis of histological OARSI scores demonstrated narrow limits of agreement and minimal inter-observer variability in the Bland-Altman plot, excellent inter- and intra-observer agreement (ICC > 0.85), and almost perfect reliability (Cronbach’s α > 0.95).
Conclusion
The results of the study demonstrated a stage-dependent association between macroscopic and histological assessments of osteoarthritic cartilage. The findings indicate that macroscopic ICRS grading may serve as a reliable tool for evaluating moderate to advanced stages of cartilage degeneration. However, its utility in early-stage lesions appears limited due to a weaker correlation with OARSI histological scores. Thus, while macroscopic visual evaluation should be interpreted with caution in early-stage degeneration, histological assessment using the OARSI scoring system remains a valuable tool for accurately identifying early degenerative changes.
Introduction
The assessment of cartilage degenerations is of critical importance, as it aids in making decisions regarding operative treatment strategies, guides intraoperative procedures, and serves as a key factor in evaluating the effectiveness of treatments for various cartilage disorders, including osteoarthritis.1 -4 However, due to limitations in resolution and sensitivity, the accurate evaluation of cartilage damage using radiographs (x-ray/CT) or magnetic resonance imaging (MRI) has been challenging.5 -9 The direct assessment methods for the evaluation of articular cartilage provide better, reliable and precise information in research as well as in clinical settings. The two direct evaluation methods, visual assessment and histology, are used to assess the stage of cartilage degeneration. Identifying a correlation between visual and histological grading methods is crucial to determine whether, and to what extent, macroscopic visual grading aligns with microscopic evaluation using a histopathological scoring system. Such an analysis can provide deeper insight into the accuracy and robustness of cartilage assessments methods and help identify any potential limitations in the visual evaluation of articular cartilage. This, in turn, may indicate the need for refinements in visual assessment protocols, if necessary.
There are several grading scores systems exist for the assessment of osteoarthritic, repaired and engineered cartilage; however, only a limited number among them have been validated. The utilization of validated scoring system can enhance exchanges of information reliably necessary for communications between clinical professional (e.g., surgeon, pathologist) as well as researchers. International Cartilage Repair Society (ICRS) scoring system was introduced to facilitate the convenient and credible comparison of cartilage direct assessment based on the visual morphology
Histological evaluation remains one of the most direct and informative methods for assessing structural changes in articular cartilage. Over the past several years, the Histology/Histochemical Grading System (HHGS),
12
along with its various modified versions, has been widely utilized to evaluate cartilage degradation. Recently, the Osteoarthritis Research Society International (OARSI) developed an alternative grading system with the objective of providing a more refined and standardized approach to the assessment of osteoarthritic cartilage pathology
Although the ICRS grading system and the OARSI scoring method are fundamentally different, both are commonly used to directly assess changes in cartilage. However, to date, no study has quantitatively correlated these two approaches specifically in human articular cartilage. While previous efforts have been made to correlate other cartilage assessment scoring systems a direct quantitative comparison between the ICRS and OARSI systems remains unavailable.14 -17 Determining whether the ICRS grade, based on macroscopic evaluation, accurately reflects histopathological changes represented by the OARSI score would provide validation of visual assessment as a reliable indicator of cartilage degeneration. Such validation could, in turn, reduce the need for additional invasive biopsies required for histopathological evaluation. Therefore, the aim of this study was to investigate the quantitative association between macroscopic evaluation using the ICRS grading system and histopathological evaluation using the OARSI scoring system in osteoarthritic human cartilage. By analyzing degenerated osteoarthritic cartilage (ex vivo), the study seeks to determine the extent to which macroscopic ICRS grading reflects histological changes assessed by the OARSI system. The hypothesis of the study was that the macroscopic ICRS grading system would exhibit a positive correlation with the histopathological OARSI scoring system in osteoarthritic cartilage, as both are widely recognized clinical methods for evaluating cartilage degeneration.
Materials and Methods
Sample Collection
Osteoarthritic cartilage sections were collected during routine arthroplasty procedure while normal cartilage tissue section was purchased by a commercial provider (Articular Engineering, USA). The purchased samples were accompanied by appropriate documentation, including ethical clearances, donor age, gender, and tissue’s anatomical location. The patients undergoing arthroplasty had already been confirmed to have osteoarthritic knees through radiography, in accordance with standard clinical procedures. Approval for the use of human tissue was granted by the Regional Committee for Medical Research Ethics (2013-265 REK), Norway, and the informed consent of the patients were obtained. All samples included in the study was acquired from the femoral condyle section of the knee. The specific location of load bearing areas in knee such as lateral or medial were also recorded. Total 70 cartilage sections (n = 70) were obtained from the 19 candidates over the age 55 years. Furthermore, the contributions of each candidate are included in the Supplemental Appendix
Macroscopic Evaluation
The articular surface of cartilage sections acquired from the osteoarthritic knees was visually evaluated and graded by orthopedic surgeon during arthroplasty. All associated data—including osteoarthritic grade, anatomical location (medial or lateral), age, gender, and other relevant clinical details—were systematically documented in the records. The macroscopic assessment and classification of osteoarthritic cartilage were conducted in accordance with the standard ICRS grading system, ranging from grade 0 to IV
Once the ICRS grade was independently confirmed by both orthopedic surgeons, the precisely identified cartilage area was isolated using a 4-mm punch biopsy and preserved in formalin for further processing. The surgeons reconfirmed that each biopsied section corresponded accurately to the assigned ICRS grade. It was ensured that no overlap of different grades of tissue occurred within a single tissue section, thereby minimizing the risk of including heterogeneous tissue within a specimen. The biopsied samples were then forwarded to the histology laboratory for further processing, with all relevant data systematically documented. This ensured that the same cartilage sections assessed macroscopically using the ICRS grading system were subsequently analyzed histologically according to the OARSI criteria. This procedure was applied consistently to all samples. One histological slide was prepared from each ICRS-graded tissue section, yielding a total of 70 slides from 70 distinct samples. Following standard histological protocols, 5-µm-thick sections were cut perpendicular to the articular surface and stained with hematoxylin and eosin (H&E). All 70 slides were then independently scored according to the OARSI system. Out of a total 70 cartilage sections, macroscopic ICRS assessment classified 11 sections as grade 0, 18 sections as grade I, 18 sections as grade II, 20 sections as grade III, and 3 sections as grade IV.
Histological Staining and Scoring
The cartilage sections were excised using a surgical scalpel, oriented perpendicular to the articular surface. All sections were preserved in neutral buffered formalin (10%) at the temperature of 4 degree centigrade prior to histological processing. Histological slides were prepared using standard Hematoxylin and Eosin (H&E) and Safranin-O with Fast Green staining. Sakura Tissue-Tek Prisma automatic stainer and coverslipper was used to prepare the histology slides. Based on the OARSI histopathologic evaluation template, 13 each slide was independently scored from 0 to 6 by three histopathologists (inter-observer analysis). For intra-observer analysis, the interval between two measurements by the same histopathologist was kept at a minimum of two weeks.
Statistical Data Analysis
Reproducibility Analysis
The reproducibility of the OARSI scoring system was assessed using Bland-Altman graphical analysis. Intra-observer reproducibility was calculated as the difference between two scores from a single observer and the mean of those scores. Inter-observer reproducibility was determined by calculating the difference between individual observer scores and the average of all observers. The Bland-Altman plot displayed the upper and lower limits of agreement, which were determined by adding and subtracting twice the standard deviation (SD) of the differences from the mean difference.18,19 The coefficient of repeatability (CR) is a statistical measure used in Bland-Altman analysis to quantify the agreement between two sets of measurements. The CR is calculated as 1.96 times the standard deviation of the differences between the two measurement sets, providing a quantitative estimate of measurement reproducibility. A smaller CR indicates stronger agreement, suggesting minimal variability between repeated measurements. In contrast, a larger CR represents greater variability and, therefore, poorer agreement between the measurements. 18
Reliability Analysis
Reliability refers to the ability of a measurement to produce consistent results under similar conditions. This concept includes the internal consistency of a scale, which is assessed using Cronbach’s alpha (α), a metric that evaluates the correlation between observers. The value of “α” at least 0.7 is generally considered acceptable for reliability, while values between 0.7 and 0.9 indicating good reliability, and values above 0.9 signifying excellent reliability. 20 Another approach is via Kappa (κ) analysis. “κ” is a concordance coefficient that adjusts for errors attributable to chance and is used to estimate intra- and inter-observer variation.21,22 Based on Landis’ classification, κ values are interpreted as follows: poor (<0), slight (0-0.2), weak (0.21-0.4), moderate (0.41-0.6), substantial (0.61-0.8), and almost perfect (0.81-1.0). Fleiss’ kappa was applied to assess inter-observer reliability, while Cohen’s kappa was used for intra-observer reliability. A “κ” value of ≥0.80 is widely accepted as the threshold for a classification system to be considered reliable. 23
Variability Analysis
The intra- and inter-observer variability were evaluated by determining the intraclass correlation coefficient (ICC). The ICC values were computed using a two-way random-effects analysis of variance (ANOVA), with absolute agreement type and single measures. Based on Fleiss’ guidelines, ICC values were interpreted as follows: values less than 0.40 considered poor reliability, values between 0.40 and 0.75 reflect fair to good reliability, and values greater than 0.75 signify excellent reliability. 24
Correlation Analysis
The correlation between the first and second observations for each observer was assessed using Spearman’s rank correlation coefficient (ρ). 25 The Spearman’s correlation and the bivariate linear regression analysis were performed to examine the association between the ICRS grade and OARSI score of osteoarthritic articular cartilage. The magnitude of correlation coefficient (r) and coefficient of determination (R2) were evaluated. The assumptions associated to the analyses were verified and the level of significance (P < 0.05) was indicated with the analysis. In addition to the measurement of statistical significance level, residual-plot was also analyzed to confirm that model is unbiased. The mean values were represented with the corresponding standard deviations. The box-plot shows the median value and inter-quartile range. Data analysis was performed using GraphPad Prism (version 10.4.2) and MATLAB (R2021a, MathWorks Inc.).
Results
The indicative area of macroscopically assessed ICRS grade I, II, III, and IV by orthopedic surgeon is illustrated (

Panels (A)-(D) show representative images corresponding to visually assigned ICRS grades I, II, III, and IV, respectively. Panels (E)-(H) display the corresponding safranin-o/fast green-stained histological sections images of osteoarthritic articular cartilage for each respective ICRS grade.
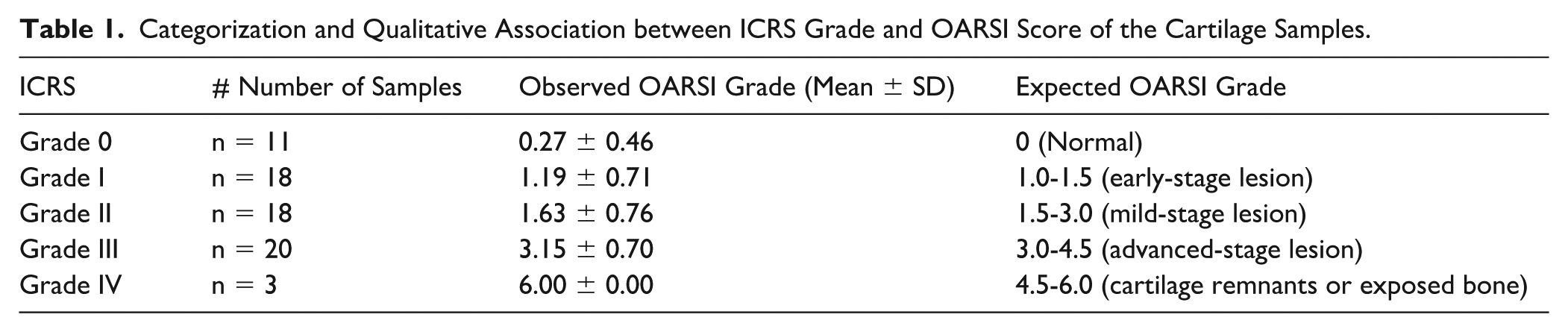
The OARSI score was observed to gradually increase with the enhancement in ICRS grades. Average OARSI scores of cartilage samples have shown the good agreement with ICRS grading of cartilage degeneration (
Categorization and Qualitative Association between ICRS Grade and OARSI Score of the Cartilage Samples.
Statistical analysis for the quantitative correlation between the ICRS scores assigned visually and, OARSI scores assigned histo-pathologically to the same cartilage sections were assessed by the magnitude of correlation coefficient (r) and coefficient of determination (R2). The moderate positive association (n = 67, r = 0.811, R2 = 0.657, P < 0.001) between ICRS grade and OARSI score was observed (

OARSI score as a function of ICRS grade of osteoarthritic articular cartilage (n = 67 sections). A positive association (r = 0.811, R2 = 0.657) between the histopathological OARSI scores and macroscopic ICRS grades was observed. Tissue sections of ICRS grade IV (n = 3 sections) were excluded.
Quantitative Association between ICRS Grade and OARSI Score of the Cartilage Samples.

Reproducibility Analysis

Bland-Altman plot for OARSI reproducibility analysis. Differences between the first and second scoring sessions by each of the three independent observers (histopathologists) are plotted against the average of the two scores to assess intra-observer agreement.
Intra- and Inter-observer Reproducibility Using Bland-Altman Analysis.

Δ1 = difference of mean between the first and second scores. Δ2 = difference of mean between score of observer and average of three observers.
Reliability Analysis
The results of the reliability analysis of OARSI scores are summarized in
Reliability Analysis Using the Kappa Coefficient (with Standard OARSI Scores).

Classification of Observations as Low, Moderate, and Severe Grading.

Reliability Analysis Using the Kappa Coefficient (with Classification into Low, Moderate, and Severe Grades).

Reliability Analysis Using Cronbach’s Alpha Coefficient.

T1 = first time observation. T2 = second time observation.
Variability Analysis
The ICC values for intra-observer analysis ranged from 0.940 to 0.961, while the inter-observer ICC values for the first- and second-time observations by all three observers were 0.868 and 0.892, respectively (
Intra- and Inter-Observer Variability Analysis (2-Way Random Effect, Single Measure, Type Absolute Agreement) Using ICC Coefficient.

ICC = intraclass correlation coefficients; CI = confidence interval.
Correlation Analysis
The ρ values of the intra-observer analysis (n = 67, P < 0.05) for observers X, Y, and Z were 0.941, 0.973, and 0.972, respectively, while the overall ρ value of the inter-observer analysis (n = 201, P < 0.05) for all three observers was 0.964 (

Correlation analysis between the first and second scoring sessions by observer X (A), observer Y (B), observer Z (C), and the combined correlation across all three observers (histopathologists) (D), based on the OARSI scoring system.
Correlation Analysis Using Spearman’s Coefficient.

Discussion
The osteoarthritic degenerative process is primarily characterized by the progressive loss of articular cartilage thickness, ultimately leading to functional failure of the affected synovial joint. An imbalance in the homeostatic process of cartilage disrupts the natural turnover of extracellular matrix components, such as proteoglycans, hyaluronic acid, collagen, and water content. Common pathological features associated with cartilage degeneration include surface erosion, collagen fibrillation, clefts, flaking, thinning, and chondrocyte clustering. To detect such microstructural changes, histological evaluation remains the most definitive method for assessing the degree of articular cartilage degradation. However, the risks and potential clinical complications associated with repeated invasive biopsies of articular cartilage present a significant concern in histological analysis-based studies. Consequently, approaches that minimize the need for biopsy while still enabling accurate assessment of cartilage condition are highly desirable and have gained increasing attention in recent years.2 -4,26,27 In current clinical practice, during intraoperative joint surgical procedures or arthroscopy, orthopedic surgeons typically assess the condition of articular cartilage through visual inspection, primarily using the ICRS scoring system. The articular surface of cartilage sections acquired from the osteoarthritic knees was visually evaluated and graded by orthopedic surgeon during arthroplasty. In this study, such visual evaluations using the ICRS grade system are validated against histological assessments based on the OARSI scoring system for the same cartilage lesions. While previous studies have reported correlations between visual ICRS scoring and histological assessments such as the Mankin (HHGS) and Outerbridge grading systems,14 -17,28 to our knowledge, no study to date has quantitatively correlated ICRS scores with the standard OARSI histological scores. The moderate positive association observed between ICRS and OARSI scores in this analysis aligns with previous findings that reported similar correlations between macroscopic evaluations and various other types of histological grading systems. These results support the view that macroscopic evaluation—such as that performed during intraoperative surgery or arthroscopy—can serve as an effective method for assessing osteoarthritic cartilage degeneration. However, the study also highlights the need for caution during visual macroscopic assessments, particularly when evaluating early- to mild-stage cartilage lesions (i.e., ICRS grade I and II), where a weaker positive association was observed in the result. Such complexity in early- to mild-stage cartilage lesions arise because the structural changes characteristic of early cartilage degeneration, such as collagen remodeling, may not be readily apparent through standard arthroscopic or histological assessment. Emerging evidence suggests that subtle alterations in cartilage morphology can be visualized using the advanced imaging technique known as second harmonic generation (SHG) microscopy.3,4,29
Earlier studies have investigated the relationship between macroscopic and microscopic grading systems in the evaluation of articular cartilage degeneration, with the objective of determining the reliability of visual assessment in capturing underlying histopathological changes. Kleemann et al., 28 reported a significant correlation (R² = 0.74, P < 0.01) between ICRS macroscopic grades and Mankin histological scores in tibial plateau specimens. However, their study indicated the limited ability of macroscopic evaluation to discriminate early degenerative changes, particularly between ICRS grade 0 and grade I, which lack distinct visual markers. Further, Acebes et al., 16 demonstrated a good agreement between arthroscopic grading and histological evaluation using the HHGS score, with a weighted kappa coefficient of 0.619, particularly for early-stage lesions. Nonetheless, it was indicated that arthroscopic assessments frequently overestimated the severity of advanced lesions.
In the present study, a moderate to strong positive correlation was observed between ICRS and OARSI scores, with Spearman’s correlation coefficients ranging from 0.592 to 0.811, depending on the range of ICRS-graded samples included in the respective groups (
However, the study also highlights limitations of visual macroscopic assessment in early-stage cartilage lesions. A poor association was observed between macroscopic and microscopic assessments for ICRS grades 0 and I, suggesting that early degenerative changes may not be consistently identified through visual inspection alone. These findings are consistent with previous reports indicating that subtle histological changes—such as early matrix disruption or proteoglycan loss—are often not detectable macroscopically. 30 Therefore, the use of macroscopic grading should be approached with caution when evaluating early-stage lesions, as reliance on visual cues alone may underestimate the true extent of cartilage degeneration. In such cases, histological evaluation might be required to ensure accurate classification and improve diagnostic sensitivity.
The histological OARSI analysis demonstrated excellent inter- and intra-observer agreement (ICC > 0.85), along with almost perfect reliability (Cronbach’s α > 0.95), thereby supporting the robustness of the histological OARSI scoring system as a standard reference. Moreover, the Bland-Altman analysis for the OARSI scores demonstrated narrow limits of agreement and low mean differences among the scores assigned by the three independent histopathologists. No systematic bias was observed, and the majority of inter-observer differences found within the accepted confidence intervals. These findings indicated minimal observer variability, thereby affirming the high reproducibility and consistency of the OARSI histological grading system.
This study employed a systematic comparison of two widely recognized clinical grading frameworks—the ICRS and OARSI systems—providing more insights into the degree of agreement between visual and microscopic cartilage assessment methods. These findings are consistent with those of Kleemann et al., 28 who reported a significant correlation between ICRS grades and histological Mankin scores, while also highlighting the challenges of detecting early degenerative changes through macroscopic visual assessment. Moreover, this study systematically evaluated a comprehensive quantitative approach to the OARSI histological scoring system, which offers a contemporary and clinically relevant framework for cartilage assessment. Various statistical performance measures were employed, including Bland-Altman analysis, correlation coefficients, kappa statistics, Cronbach’s alpha, and the ICC coefficient. The results demonstrated consistent and reliable OARSI scoring in both intra-observer and inter-observer evaluations.
In the present study, only a small number of ICRS grade IV tissue sections (n = 3) were selectively included. ICRS grade IV represents the most advanced stage of osteoarthritic degeneration, characterized by extensive cartilage loss and exposure of the subchondral bone. This decision was based on the understanding that severely degenerated cartilage can be graded with high confidence and consistency using both the ICRS and OARSI classification systems, making observer disagreement unlikely and offering limited additional clinical insight. Including a larger proportion of such samples could artificially inflate the correlation between the two grading systems due to the inherent grading certainty in advanced-stage pathology, thereby introducing potential bias into the correlation analysis. In contrast, discrepancies between grading systems are more likely to occur in early to moderate stages of degeneration, where the interpretation of morphological and structural changes tends to be more variable. Given that the primary objective of this study was to evaluate the association between macroscopic visual and histological grading methods, the analysis focused on large number of early to moderate-stage cartilage lesions to facilitate a more meaningful and informative correlative assessment that captures significant inter-system grading variability.
Limitations
As a limitation of this study, the analysis was conducted using the ex-vivo osteoarthritic cartilage sections acquired from the human knees. The in-vivo ICRS grading score may differ from the ex-vivo grading score due to variations in assessment conditions and visualization. This refers to the potential discrepancies between cartilage grading performed using arthroscopy within knee-joint (in vivo) and visual grading conducted on excised tissue specimens (ex vivo) outside the knee-joint In this context, in vivo typically refers the assessment made intraoperatively during arthrotomy, where the articular surface is visually inspected under time constraints, variable lighting, joint positioning, and potential bleeding, all of which may influence the perception and interpretation of cartilage condition. By contrast, ex-vivo grading—as applied in this study—was conducted on extracted cartilage specimens during arthroplasty, allowing for better illumination, stabilization, and more deliberate inspection of tissue characteristics. This controlled environment may reduce observational variability and may reveal surface or subsurface features that are less apparent during in-vivo assessments. As the results of this study, based on ex-vivo ICRS grading, demonstrated good correlation with histological OARSI scores, particularly in moderate to advanced-stage degeneration. However, it is important to recognize that in-vivo ICRS assessments, especially during arthroscopy, may be subject to greater variability due to limited field of view, reduced tactile feedback, and the presence of synovial fluid or soft tissue that can obscure fine surface details. Therefore, while the ex-vivo findings of this study provide more insights and validation for the ICRS grading system (especially for moderate to advanced grade of cartilage lesion), it may not fully capture the real-time variability encountered during in-vivo surgical procedures. Future comparative studies between in-vivo and ex-vivo ICRS assignments could further elucidate this variability and help improve standardization across clinical and research settings. Therefore, the result of the study should be accounted with caution. Due to ethical and practical constraints associated with invasive biopsy of healthy human knee joints, conducting such a correlative study in an in-vivo setting is challenging. Furthermore, such study in animal and induced osteoarthritis model can enhance the validity. However, the induced osteoarthritis model in animal cannot directly compared to human primary osteoarthritic degenerations. Nevertheless, the detailed knowledge and enhanced understanding between the correlation of different grading system for articular cartilage can assist in finding the most suitable approach for the cartilage assessments in the benefit of patient.
The ICRS grading is typically applied to a broader surface area of the articular cartilage that is visually accessible during surgery or arthroscopy. This visual assessment allowing surgeons to grade as a representative lesion within the exposed surface. However, the histological scoring—such as the OARSI system—is performed on fixed, sectioned tissue blocks that represent only a small, localized region of the cartilage. A macroscopically graded region may encompass heterogeneous tissue, including different grades of degenerated areas, while the corresponding histological section may capture only a small focal region from the entire lesion—potentially under- or overestimating degeneration severity. However, in the present study, such variation was minimized by acquiring a 4-mm diameter biopsied tissue section from the representative cartilage lesion. Furthermore, whether the biopsied whole tissue section accurately represents the ICRS grade lesion was reconfirmed by orthopedic surgeon before storing it into the formalin and processing it for histology. Thus, the limitation arising from spatial discrepancies—particularly those contributing to grading variability in heterogeneous cartilage lesions—was effectively mitigated and did not constitute a significant concern in the present study.
Conclusions
Progressive increases in ICRS grades were associated with thinning and morphological disorganization of the osteoarthritic cartilage matrix. Qualitatively, visual macroscopic grading showed good agreement with histological scores, as indicated by a consistent increase in mean OARSI histological scores with advancing ICRS grades. Spearman’s correlation and regression analyses between ICRS grading and OARSI scoring revealed a relatively weak positive correlation in early-stage lesions, a moderate correlation with the inclusion of moderate-stage lesions, and a strong correlation when severely degenerated cartilage was included. These findings demonstrate a stage-dependent association between macroscopic and histological assessments of osteoarthritic cartilage. Furthermore, statistical performance measures—including Bland-Altman analysis, correlation coefficients, kappa statistics, Cronbach’s alpha, and intraclass correlation coefficients (ICC)—confirmed that OARSI assessments conducted by both intra- and inter-observers were reproducible, reliable, and consistent. In conclusion, the findings suggest that visual macroscopic ICRS assessment may serve as a reliable method for evaluating moderate to advanced stages of osteoarthritic cartilage degeneration; however, its application in early-stage lesions should be approached with caution due to the reduced correlation with OARSI histological scores. Furthermore, the inclusion of histological analysis can be beneficial for the detection of early degenerative changes, particularly when accurate tissue characterization is essential.
Supplemental Material
sj-docx-1-car-10.1177_19476035251393150 – Supplemental material for Assessment of the Correlation between Macroscopic ICRS Grading and Histopathological OARSI Scoring in Osteoarthritic Cartilage: An Ex-Vivo Analysis
Supplemental material, sj-docx-1-car-10.1177_19476035251393150 for Assessment of the Correlation between Macroscopic ICRS Grading and Histopathological OARSI Scoring in Osteoarthritic Cartilage: An Ex-Vivo Analysis by Gavish Uppal, Tarun Goyal, Anup Kumar, Ruchi Sinha, Manjit Kaur and Rajesh Kumar in CARTILAGE
Footnotes
Ethical Considerations
Ethical approval was granted by the Regional Committee for Medical Research Ethics (REK 2013-265), Norway. Only anonymized data were used in this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author (R.K.) acknowledges support from the Ramalingaswami Re-entry Fellowship, Department of Biotechnology (DBT), Government of India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.