
Abstract
Objective
A medial open-wedge high tibial osteotomy (MOWHTO) may increase the posterior tibial slope (PTS). The purpose of this study was to determine the effect of the osteotomy inclination angle (in the sagittal plane) in combination with different hinge positions (in the transverse plane) on the change in PTS due to a MOWHTO.
Methods
We developed a mathematical approach to determine the effect of the osteotomy inclination angle combined with different hinge positions. The change in PTS was determined for different osteotomy inclination angles, hinge positions, and intended wedge angles. Anterior-inclined, parallel, and posterior-inclined osteotomy inclination angles were simulated. Hinge positions varied between 5° anterolateral and −45° posterolateral. The wedge angles were 5°, 10°, and 15°. Moreover, 2 in silico osteotomies were performed to verify the results of the mathematical model.
Results
The PTS was maintained when the osteotomy cut was performed parallel to the tibial plateau with a lateral hinge position. The PTS changed when the osteotomy was not aligned in the sagittal plane, ranging between 0.0° and 0.6°. Different hinge positions, however, had a large effect on postoperative PTS change, ranging between 0.1° and 10.7°.
Conclusions
Our mathematical approach showed that the hinge position has a strong effect on the PTS. The sagittal osteotomy inclination angle had little effect on the PTS. An inclination angle parallel to the medial tibial plateau combined with a lateral hinge position does not change the PTS.
Keywords
Introduction
Medial open-wedge high tibial osteotomy (MOWHTO) is an established treatment for relatively young and active patients with an early stage of unicompartmental medial osteoarthritis and varus deformity of the knee.1 -3 MOWHTO redistributes the mechanical load from the medial to the lateral compartment in the coronal plane and, therefore, reduces the articular cartilage pressure in the medial compartment. This results in a reduction of pain and improvement of knee joint function. 1 However, in addition to coronal alignment, unintended changes may also occur in the sagittal plane due to a MOWHTO.4,5
Several studies indicate an increase of posterior tibial slope (PTS) due to a MOWHTO, which increases the tensile load on the anterior cruciate ligament (ACL) and affects knee stability.1,6,7 Sometimes, the osteotomy is performed with the intention to decrease the PTS as a treatment for ACL instability, for example, when one or more previous ACL reconstruction(s) failed or when there is a pre-existent high PTS in combination with an ACL rupture. In general, this increase in the tensile load on the ACL is not intended. Moreover, a change in the PTS results in a different distribution of the mechanical load on the articular surface. For example, an increased PTS results in anterior translation of the tibial plateau, resulting in decompression of the posterior femoral condyles. 8 Factors that could cause a PTS change during a MOWHTO are the sagittal osteotomy inclination angle and the hinge position.
Recently, several studies have investigated that to maintain the PTS, the sagittal osteotomy inclination angle should be parallel to the medial tibial plateau and the hinge should be located laterally.1,4,5,9 -11 Moreover, a posterolateral hinge position increases the PTS.5,9,12 However, several of these studies have also shown that performing the perfect osteotomy according to these requirements is difficult in practice.5,11 Whereas the effect of the osteotomy inclination angle and the effect of the hinge position on the PTS have been studied separately, we found no study which examines the combined effect.1,5,9 -12 This is unfortunate, since studying the effect of one parameter while not taking into account the other can lead to nonconclusive outcomes. Moon et al. 10 concluded that changes in PTS are probably greater if the hinge position is considered in addition to only the osteotomy inclination angle. This confirms the need for virtual model studies, especially since a MOWHTO is rarely performed perfectly.
In this study, we investigated the effect of the osteotomy inclination angle in combination with different hinge positions on the change in PTS in a MOWHTO using a mathematical model. We hypothesized that a posterior-inclined osteotomy and posterolateral hinge positions would increase the PTS. Moreover, we expected the PTS to decrease with an anterior-inclined osteotomy and anterolateral hinge positions. Finally, for illustration purposes, the results were presented in an in silico model.
Methods
We performed in silico MOWHTOs for a range of osteotomy inclination angles, hinge positions, and wedge angles. The osteotomy inclination angle (φ) was defined as the angle between the medial tibial plateau line and the osteotomy line.
1
The osteotomy line was defined as the projection of the osteotomy plane in the sagittal plane. A posterior-inclined osteotomy was defined as being positive and an anterior-inclined osteotomy as negative (
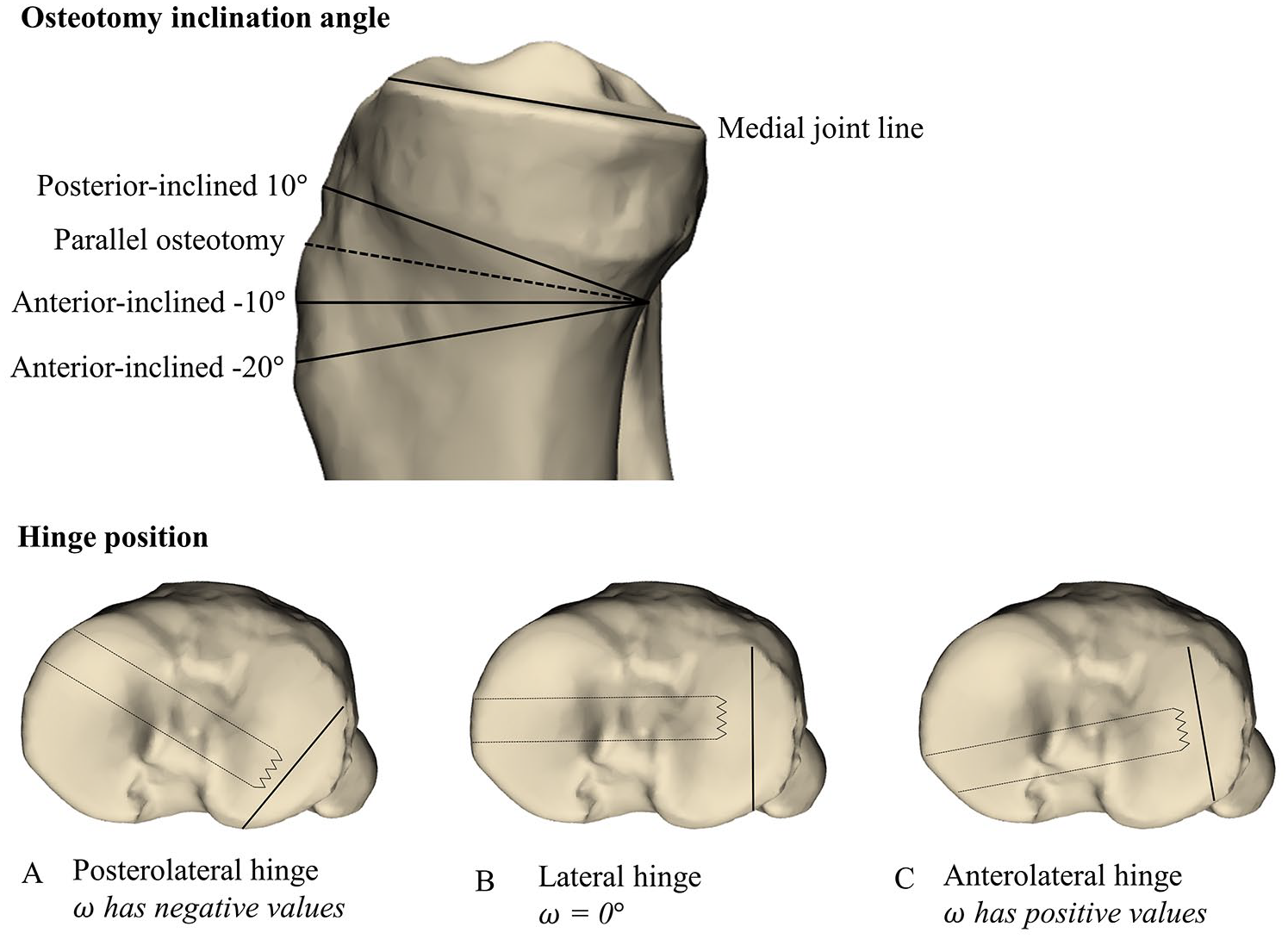
Osteotomy inclination angle: Medial view of the 3-dimensional model of a right knee with associated osteotomy inclination angles. The osteotomy inclination angle was defined as the angle between the medial tibial plateau line and the osteotomy line (dashed line). Posterior-inclined osteotomies were defined as positive. Anterior-inclined osteotomies as negative. Hinge position: Transverse view of the 3-dimensional model of a right knee with associated hinge positions (
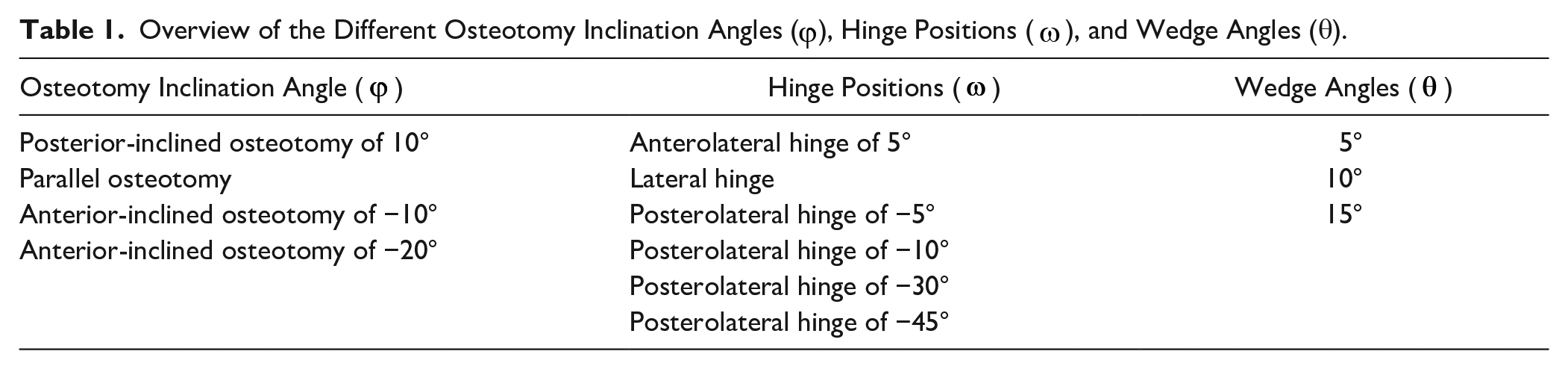
Overview of the Different Osteotomy Inclination Angles (
To describe the in silico osteotomy, we included a right-handed coordinate system which is defined as shown in
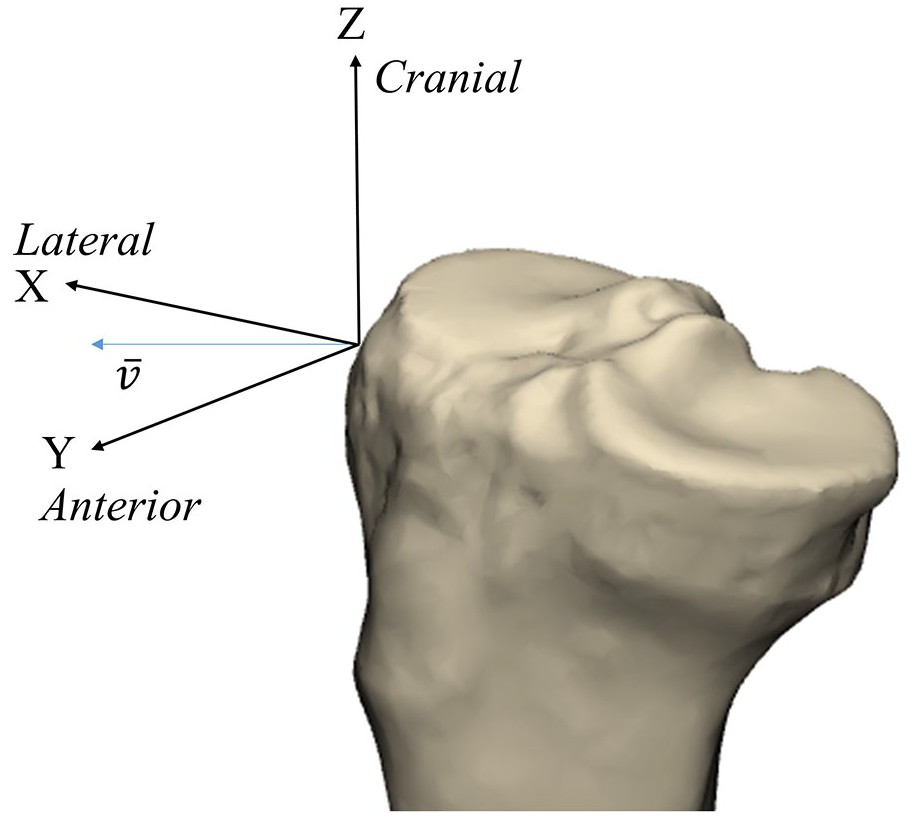
Definition of the axis for a 3-dimensional model of a right knee.
In practice, the MOWHTO consists of one rotation of the tibial plateau around the hinge axis, but for mathematical modeling, it is convenient to envision the in silico MOWHTO as a series of 5 consecutive rotations around one of the fixed axes of the coordinate system. These rotations describe the process of an osteotomy. By using the rotations, in silico osteotomies were performed, and the changes in PTS were measured. The rotation matrices are described in detail in Appendix A.
A tibia with PTS of 10° was used for modeling the effects of osteotomy inclination angles and hinge positions. The PTS was defined using the anatomical axis of the tibia. We performed 3 series of calculations:
Lateral hinge, variation of osteotomy inclination angle between −20° and 10°.
Parallel osteotomy, variation of hinge position between −45° and 5°.
Combination of varying osteotomy wedge angles and varying hinge positions.
In each case, the in silico osteotomies were performed, and the changes in PTS were measured.
For illustration purposes, an existing CT scan (slice thickness 2 mm; 120 kV; 60 mAs; Siemens Medical Solutions, Erlangen, Germany) of the lower limb of one patient was anonymized and imported into Mimics 23.0 (Materialise, Leuven, Belgium), to create a 3-dimensional (3D) bone model of the right tibia and fibula. The segmented 3D model was transferred to 3-Matic (Materialise) to perform an in silico MOWHTO. The PTS was defined as the angle between the line along the medial tibial plateau and the line perpendicular to the anatomical axis of the tibia (
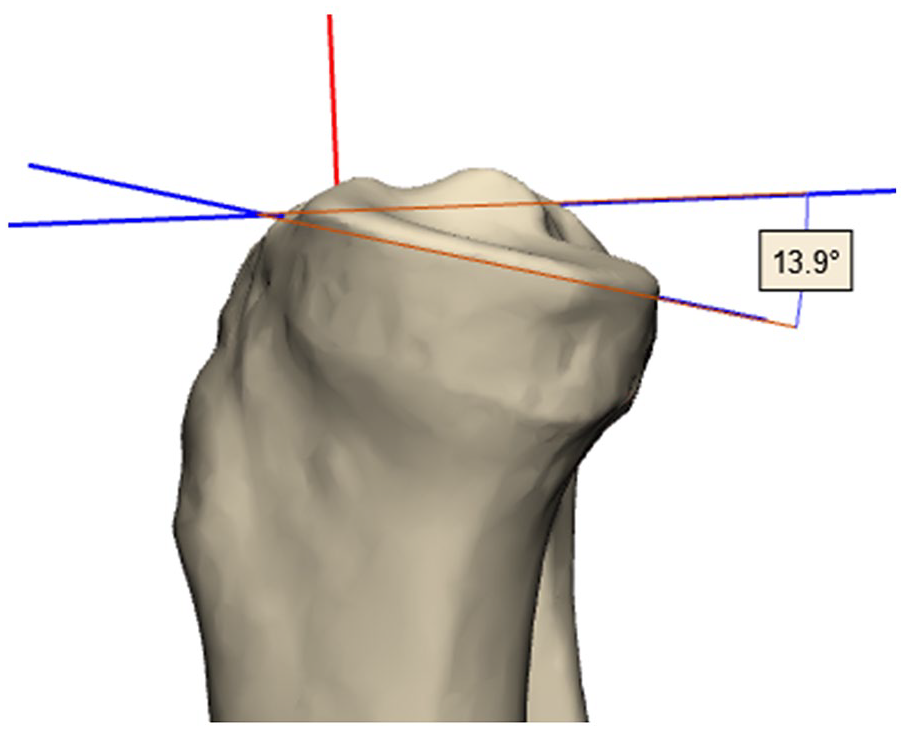
Medial view of the measurement of the posterior tibial slope. In the sagittal plane, the posterior tibial slope was defined as the angle between the line along the medial tibial plateau and the line perpendicular to the anatomical axis of the tibia. The anatomical axis is represented by the red line. The measured posterior tibial slope in this figure is 13.9°.
Results
A minimal change in PTS was found due to MOWHTO with a lateral hinge position (ω = 0) but with different osteotomy inclination angles, see
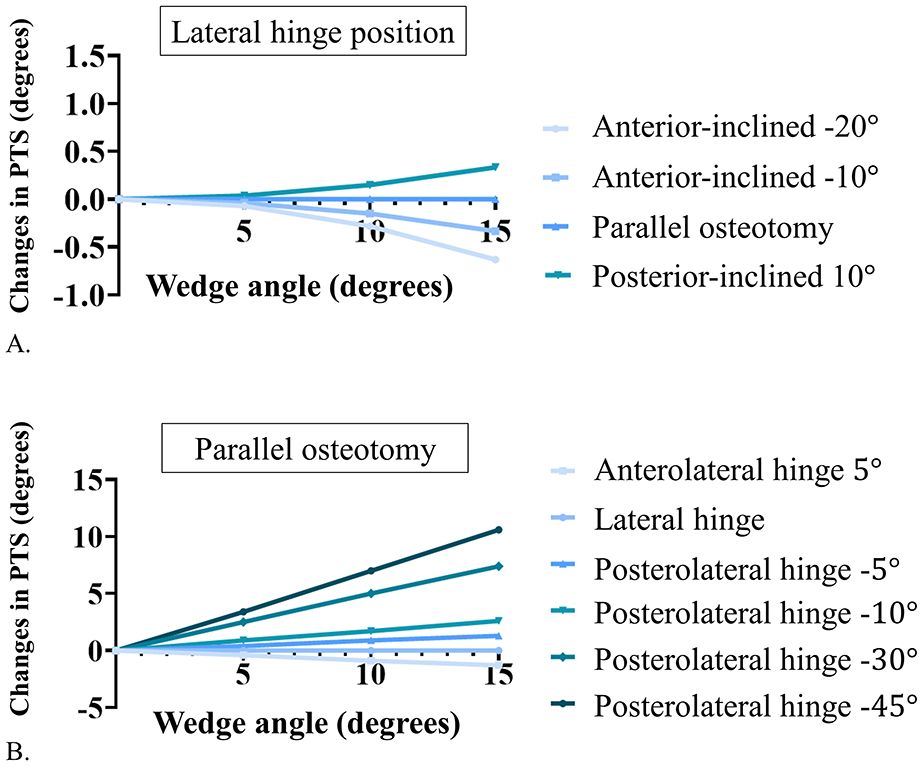
Changes in posterior tibial slope for different wedge angles. (A) shows changes in posterior tibial slope for a lateral hinge position for different osteotomy inclination angles and wedge angles. (B) shows changes in posterior tibial slope based on parallel osteotomy for different hinge positions and wedge angles. Note that the Y-axis in Figure B is 10x larger than in Figure A.
The changes in PTS resulting from different hinge positions, with a perfectly parallel osteotomy (φ = 0), are illustrated in
The Difference in Posterior Tibial Slope for Different Hinge Positions (
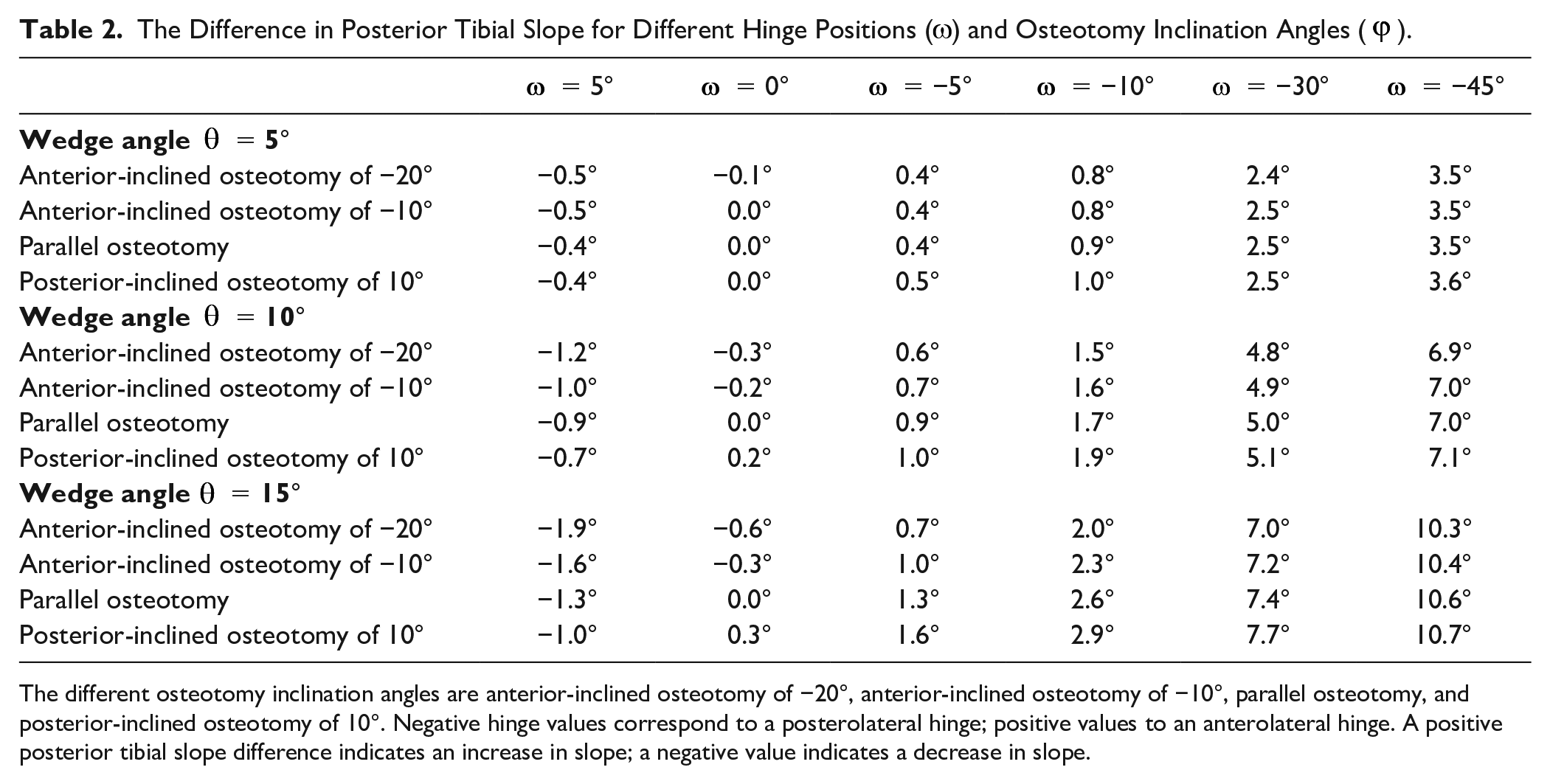
The different osteotomy inclination angles are anterior-inclined osteotomy of −20°, anterior-inclined osteotomy of −10°, parallel osteotomy, and posterior-inclined osteotomy of 10°. Negative hinge values correspond to a posterolateral hinge; positive values to an anterolateral hinge. A positive posterior tibial slope difference indicates an increase in slope; a negative value indicates a decrease in slope.
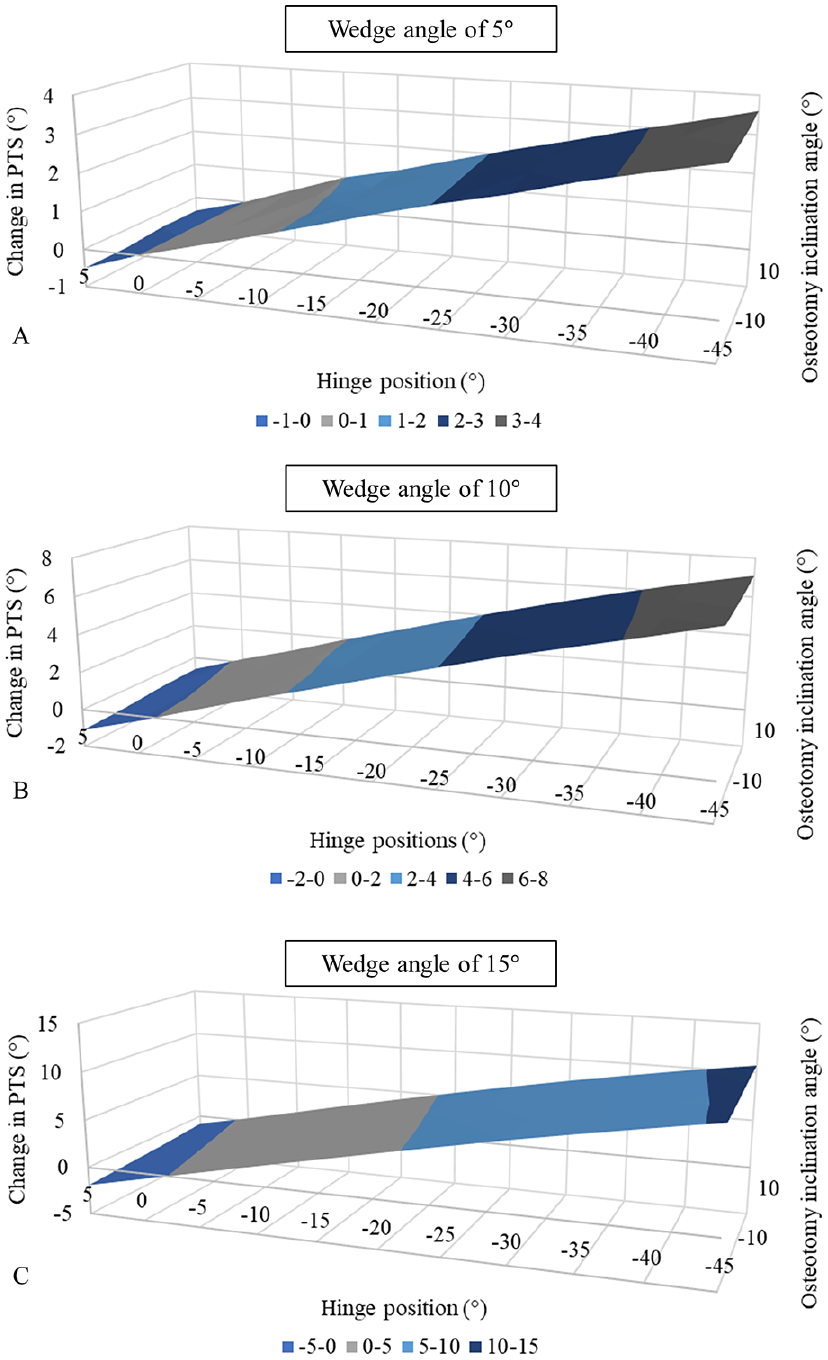
Combined effect of osteotomy inclination angle and hinge position on changes in posterior tibial slope for different wedge angles.
In Silico Test
The presurgical PTS of the 3D model of the included tibia was 13.9°. After performing a 10° MOWHTO with an osteotomy inclination angle parallel to the medial tibial plateau and a lateral hinge position, the PTS remained 13.9° (
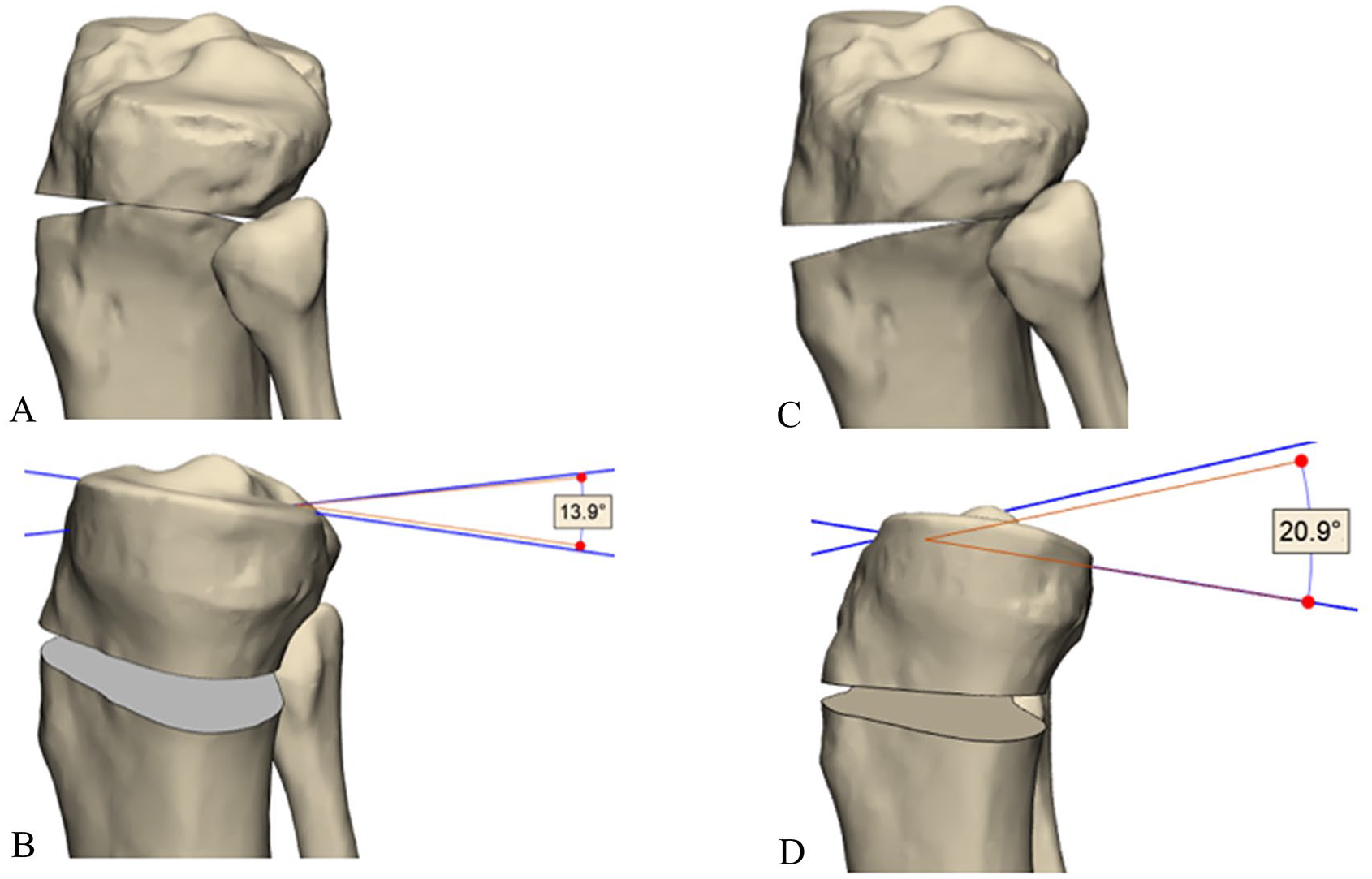
Results of the virtual osteotomy. (A) shows a 3-dimensional lateral view of an osteotomy inclination angle parallel to the medial tibial plateau and a lateral hinge position. (B) shows a 3-dimensional medial view of the measurement of the posterior tibial slope using the proximal tibial anatomic axis method. The measured posterior tibial slope was 13.9°. (C) shows a 3-dimensional lateral view of the anterior-inclined osteotomy of −10° and a posterolateral hinge position of −45°. (D) shows a 3-dimensional medial view of the measurement of the posterior tibial slope using the proximal tibial anatomic axis method. The measured posterior tibial slope was 20.9°.
Discussion
In this study, we determined the effect of the osteotomy inclination angle combined with different hinge positions on the change in PTS in a MOWHTO using a mathematical approach. The most important finding of this combined effect demonstrated that the hinge position had a strong effect on the PTS, in contrast to the osteotomy inclination angle. As a result of different osteotomy inclination angles, the PTS changed by a maximum of 0.6° in a lateral hinge condition, which may not be clinically relevant. The different hinge positions resulted in PTS changes up to 10.7°. Therefore, the hinge position had a stronger effect on PTS changes compared to the inclination angle.
The position of the hinge appeared to be an important parameter to determine changes in the PTS. Frings et al. 15 investigate the impact of variable hinge positioning and osteotomy gap height on alignment in both the sagittal and coronal planes, using 20 uniplanar MOWHTOs in solid-foam proximal tibia models. They concluded that changes in PTS can be minimized by positioning the hinge in a straight lateral alignment. Other studies presented the same results.4,5,9,12,15 However, performing a lateral hinge can be difficult.4,5 First, a study suggested that the Kirschner wire, used to guide the osteotomy, should be placed from the medial to the lateral cortex of the proximal tibia rather than from the anteromedial to the posterolateral side. 9 Second, a lateral hinge position can be achieved by inspecting the osteotomy using the gap ratio.5,9 The gap ratio is the ratio of anterior gap to posterior gap in a true lateral view in the MOWHTO. 5 The gap ratio increases with a posterolateral hinge.
Furthermore, our results indicated that the effect of the osteotomy inclination angle on the PTS was marginal. The PTS increased due to a posterior-inclined osteotomy, while remaining the same in case of a parallel osteotomy and decreased due to the anterior-inclined osteotomy. This was also reported by other studies.1,10,11 Chung et al.1,10 concluded that a parallel osteotomy inclination angle was required to overcome changes in PTS. Moon et al. 10 reported in a virtual simulation of a square column model that an osteotomy inclination angle parallel to the medial joint line caused no change in PTS. Moreover, the PTS increased in the posterior-inclined osteotomy and decreased in the anterior-inclined osteotomy. This was consistent with the results found in our study for a laterally oriented hinge. Also, Lee et al. 11 concluded that the osteotomy should be performed parallel to the medial joint line to avoid PTS changes, but at the same time, they showed that performing a parallel osteotomy was difficult in practice. On the contrary, our results showed that due to different inclination angles, the PTS changed by a maximum of 0.6° in a lateral hinge condition, which does not appear to be clinically relevant. 16
Several studies have investigated the change in PTS due to a MOWHTO. Nha et al. 17 reported an increase in PTS of 2.0° and Giffin et al. 18 concluded an increase of 4.4° due to a MOWHTO. Our mathematical approach showed that a hinge position, which varies between 5° anterolateral and −10° posterolateral yielded a PTS change comparable to the literature. The effect of the osteotomy inclination angle on changes in PTS is negligible. Therefore, orthopedic surgeons should make every effort to perform a lateral hinge position to avoid unintended PTS changes.
This study had several limitations. First, this study is a mathematical, theoretical model. The influence of other factors, such as soft tissue, the absence of the proximal tibiofibular joint, surgical techniques, and the trapezoid concept of the tibia, was not considered in our mathematical model. This may limit the translation of mathematical model to the clinical setting. However, it is important to mention that the strength of a mathematical model is that only one simulation is needed, and it is applicable to all situations without being influenced by external variables. In addition, we only presented the results for an average PTS of 10°. Second, this mathematical model does not consider the effect of the investigated parameters on tibial rotation. Third, in our study, we performed a horizontal oblique osteotomy targeting the tip of the fibular head. However, to preserve the tibial tubercle and the patellar height, often a biplanar osteotomy will be performed intraoperatively. 19 We expect this does not affect the results of this study, as the horizontal oblique osteotomy remains the same in a biplanar osteotomy. Fourth, in our research, we considered the imposed wedge angle while not accounting for the resulting correction in the coronal plane. We realize that the wedge angle is usually not equal to the correction angle, except when the hinge is perfectly perpendicular to the coronal plane. An unintended, nonlateral hinge position combined with a sagittal osteotomy inclination angle will cause undercorrection or overcorrection.5,9,12,20 Our study did not investigate this, as our primary focus was on examining the impact of the osteotomy inclination angle and hinge position on PTS changes, rather than the resulting correction. This will be interesting to investigate in future research, as explored by Frings et al. 15 by solid-foam proximal tibia models. Finally, there is a shared commitment in the literature to minimizing PTS changes after MOWTHO. To our knowledge, no previous studies have addressed the definition of clinically relevant PTS changes, making this a crucial area for future research.
Despite these limitations, our mathematical approach has the advantage to study the combined effect of the osteotomy inclination angle and hinge position. Studying the effect of one parameter without taking the others into account can lead to nonconclusive outcomes. Moreover, this method enabled us to vary several parameters separately or combined, across any range we wanted to consider, and without taking measurement errors into account.
Conclusion
Our mathematical approach showed that the hinge position has a much stronger effect on changing the PTS than the osteotomy inclination angle. An osteotomy parallel to the medial tibial plateau with a lateral hinge position results in no change in PTS. We hope that this study will create awareness among orthopedic surgeons about the importance of a lateral hinge positing to reduce PTS changes during a MOWHTO.
Footnotes
Appendix A
Authors’ Note
Investigation performed at University Medical Center Utrecht, The Netherlands.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgements and Funding
The software (Mimics and 3-Matic) used in this study was provided by the 3D Lab of the UMC Utrecht.
Ethical Approval
Not applicable.