
Abstract
Objective
The present study aims to compare the presence and severity of patellofemoral osteoarthritis between patients with root lesions and non-root lesions.
Design
A total of 102 patients were included in this study (51 root lesions and 51 non-root lesions). The root lesion cohort was matched to a non-root lesion cohort based on sex, body mass index, and age at the time of surgery. Radiographic evaluation with modified Outerbridge scoring of MRI of the knee was performed to determine the severity of degeneration of the knee joint preoperatively. Mann-Whitney and Independent t tests were used to compare the groups.
Results
The root lesion group had statistically greater Outerbridge patella scores (M = 2.45 ± 1.12) and trochlear scores (M = 2.27 ± 1.37) than the non-root lesion patients (M = 1.78 ± 1.30, P = 0.006, and M = 1.55 ± 1.40, P = 0.010, respectively). When using a new scale for grading patellofemoral arthritis, the root lesion group had statistically greater scores (M = 8.33 ± 3.38) than the non-root lesion patients (M = 5.67 ± 3.07) (P < 0.001).
Conclusion
Patients with root lesions have a greater degree of patellofemoral cartilage lesions than patients without root lesions. The presence of cartilage lesions preoperatively in root lesion patients has presented the question of whether repair is worthwhile or if one should delay surgery until arthroplasty is indicated. Future research should be carried out on outcomes of root repair surgery in patients with patellofemoral cartilage lesions, in addition to considering the patient’s age, activity level, and other risk factors.
Introduction
The menisci have a vital role in shock absorption, protection of the adjoining articular surfaces, load distribution, and stabilization of the knee joint. During weight-bearing, the posterior horn of the medial meniscus bears the most impact. 1 Posterior root medial meniscal injuries are more common than lateral root tears, 2 with a root tear being defined as a radial discontinuity within 1 cm of the meniscus root footprint.3 -5 Root tears compromise the biomechanics of the knee joint by increasing the tibiofemoral contact pressures.3,6 In addition, root tears are associated with more severe cartilage lesions on both the medial femoral condyle and medial tibial plateau than bucket handle and vertical tears. 7 In the lateral compartment, posterior root tears lead to significant increases in external rotation and lateral tibial translation when compared with the intact knee. 6 Various studies have demonstrated that when root attachments are disrupted, loads can no longer be distributed evenly, resulting in a greater occurrence of cartilage degeneration.3,6 -8 In addition, a posterior root tear can lead to meniscal extrusion. 3 Previous studies have proposed that there is a strong association between severity of cartilage degeneration and extent of extrusion of the medial meniscus.9 -14
When a root tear occurs, surgical repair may be recommended to restore joint biomechanics, while a meniscectomy has the potential to accelerate the degeneration of the cartilage.6,12,15 -17 Root repairs have been found to be associated with lower rates of osteoarthritis and total knee replacement than total meniscectomy.15,18 Specifically, surgical repair of posterior root tears of the medial meniscus is desirable in an attempt to slow the onset of degenerative changes.11,12,14 Repair has been shown to restore the peak contact pressure back to baseline, suggesting that root repair can be successful in restoring joint biomechanics to within normal conditions. 12
While previous studies have focused on the clinical consequences of a root lesion, risk factors predisposing to a root lesion have started to gain more attention. It has been reported that even cartilage defects outside the medial compartment are associated with root lesions. Patients who had a medial meniscal root tear were 5.8-times more likely to have chondral defects of the patella than patients with lateral tears. 19 Other risk factors reported for a medial meniscus posterior root tear included age,2,5 female sex,2,5,13 higher body mass index (BMI),2,5 increased Kellgren-Lawrence grade, 2 greater varus mechanical axis angle, 2 and lower sports participation 2 than those with other meniscal tears.
The present study aims to compare the severity of patellofemoral cartilage lesions between 2 cohorts of patients, those with root lesions and those without root lesions. The current literature has focused on the development of osteoarthritis after a meniscus operation; however, this study’s main focus is assessing the preoperative degree of patellofemoral cartilage lesions in patients with different types of meniscal pathologies.
Methods
After institutional review board approval (IRB ID no.: 2020-2123), an institutional database within the Hospital for Special Surgery was retrospectively reviewed to identify patients of 2 sports fellowship–trained orthopedic surgeons who had a root repair procedure between the years of 2017 and 2022. The root lesion cohort was selected from patients who had a root repair. The non-root lesion cohort was selected from patients who had meniscectomies indicating that they did not have a root lesion. The groups were matched based on sex, BMI, and age at the time of surgery. There were 51 patients who were successfully matched; 102 patients in total. A patient characteristic analysis was performed on the 102 patients included in the study. A further analysis of baseline scores was conducted to ensure groups were matched. Mean age, BMI, and number of previous procedures were not significantly different between groups (
Table 1
). Similarly, the number of patients with patella subluxation and the mean Caton-Deschamps ratio between the groups were not statistically significant (P = 0.69,
Table 2
; P = 0.427,
Patient Characteristics Between Root Repair and Meniscectomy Groups.

Tilted Patellas Between Root Repair and Meniscectomy Groups.

Caton-Deschamps Ratio Between Root Repair and Meniscectomy Groups.

Any patient who was missing preoperative MRI images was excluded from the study. Individual medical records were reviewed to obtain patient information including age, sex, BMI, laterality, date of surgery, concomitant procedures, and previous procedures.
Radiographic evaluation of the knee was performed to determine the severity of degeneration of the knee joint preoperatively. The groups were randomized, and a blinded fellowship-trained orthopedic surgeon performed the magnetic resonance imaging analysis. All postoperative MRI scans were reviewed retrospectively from our imaging record. MRIs were obtained on 1.5T or 3.0T MRI systems. MRI imaging was in both the sagittal and axial views in T1 and T2 acquisitions. A modified Outerbridge scoring was performed, alongside a new method of patellofemoral scoring, to assess the patellofemoral joint in several subcategories of the patella and trochlea—cartilage, bone, synovium, and alignment. Outerbridge assigns a grade of 0 through IV to the chondral area—grade 0 (normal cartilage), grade I (superficial fibrillation or swelling), grade II (partial-thickness defect with fissures that do not exceed 0.5 inches in diameter or reach subchondral bone), grade III (fissuring of the cartilage with a diameter > 0.5 inches, with an area reaching subchondral bone), and grade IV (erosion of the articular cartilage that exposes the subchondral bone). 20 The new patellofemoral arthrosis scoring system is described in Table 4 and Figure 1 .
Patellofemoral Scoring.
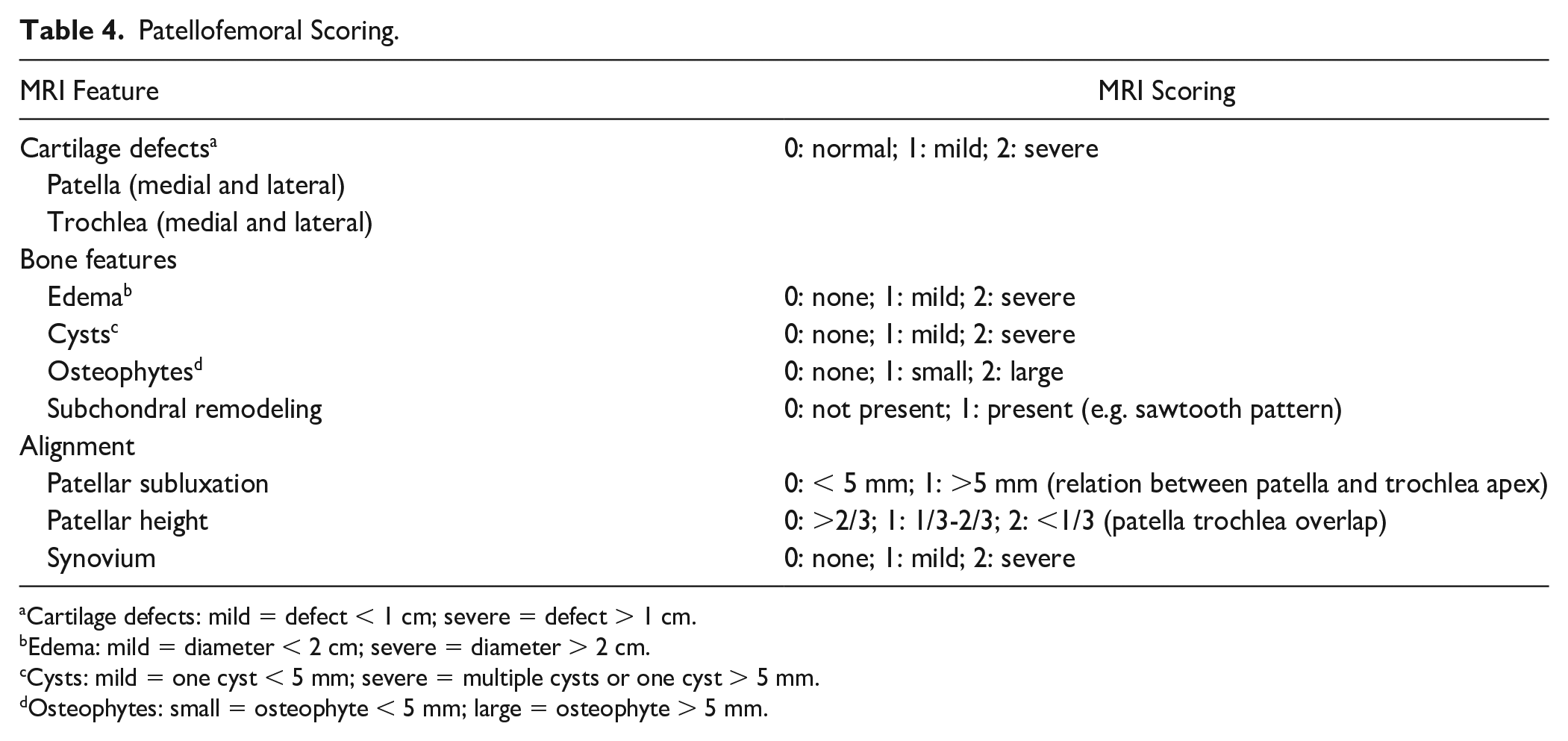
Cartilage defects: mild = defect < 1 cm; severe = defect > 1 cm.
Edema: mild = diameter < 2 cm; severe = diameter > 2 cm.
Cysts: mild = one cyst < 5 mm; severe = multiple cysts or one cyst > 5 mm.
Osteophytes: small = osteophyte < 5 mm; large = osteophyte > 5 mm.
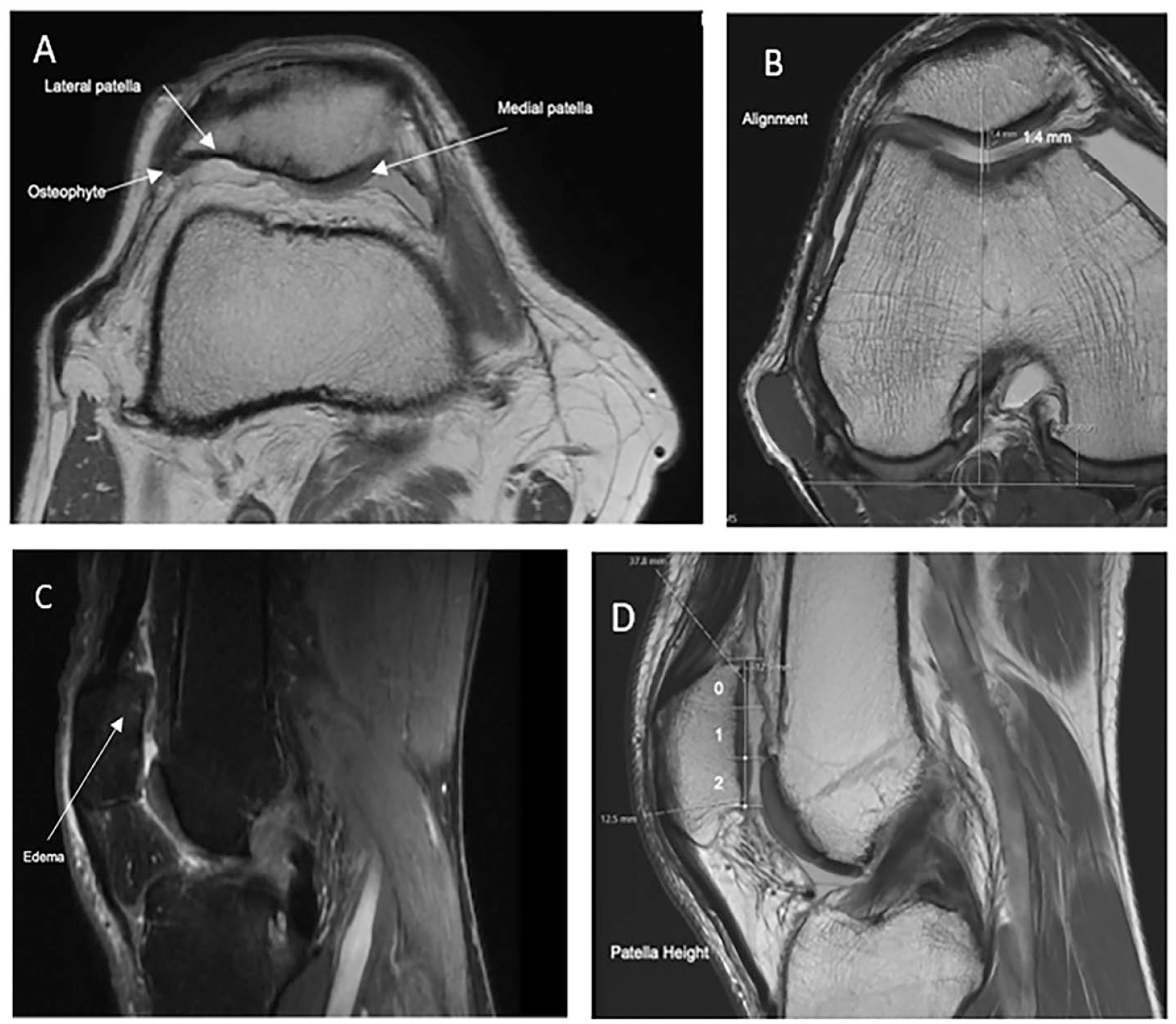
New patellofemoral scoring system with descriptive images: (
Statistical Methods
Statistics (mean, standard deviation) were analyzed for patient characteristics, including sex, BMI, and age at the time of surgery. Kolmogorov-Smirnov test was used to normalize the continuous variables. Mann-Whitney u-tests and independent t tests were used to compare the groups. Independent t test was used to analyze the relationship between lesion type (root and non-root repair) and patellofemoral scoring (new method). Mann-Whitney test was used to examine the relationship between lesion type (root and non-root repair) and both Outerbridge trochlea and patella grading. In addition, data were analyzed for frequency of patellar dislocation and patellar height. All analyses were performed with Microsoft Excel (2019; Microsoft, Redmond, WA) and SPSS software (SPSS for Windows release 22, SPSS Inc., Chicago, IL). P values ≤ 0.05 were considered statistically significant.
Results
Modified Outerbridge imaging analysis was used to compare preoperative MRIs between groups. As shown in Table 5 , the root lesion group had statistically worse Outerbridge patella and trochlea scores (M = 2.45 ± 1.12 and M = 2.27 ± 1.37, respectively) when compared to the non-root lesion patients (M = 1.78 ± 1.30 and 1.55 ± 1.4, respectively), with P = 0.006 and P = 0.010 for the root lesion and non-root lesion groups, respectively. When using the patellofemoral scoring system, the root lesion group had statistically greater (worse) scores (M = 8.33 ± 3.38) than non-root lesion patients (M = 5.67 ± 3.07) ( Table 6 , P < 0.001).
Mean Outerbridge Scoring Between Root Repair and Meniscectomy Group.

Mean Patellofemoral Scoring Between Root Repair and Meniscectomy Groups.

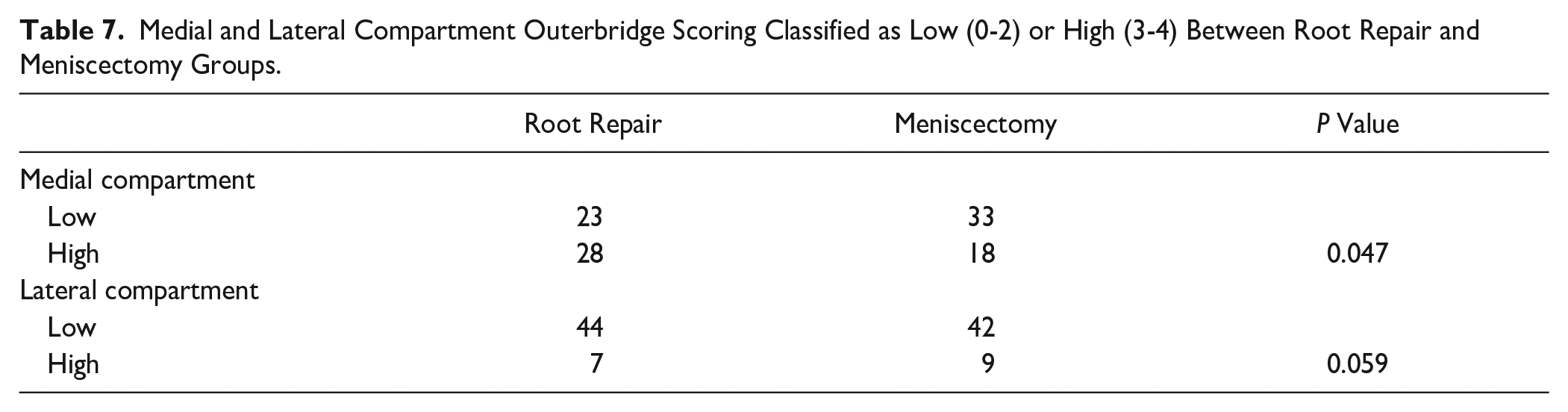
Modified outerbridge imaging analysis was also used to examine the medial and lateral compartments. When analyzing the medial compartment, the root lesion group had significantly more knees classified as higher grade using Outerbridge scoring than the non-root lesion group ( Table 7 , P = 0.047). However, when analyzing the lateral compartment, there was no statistically significant difference between the root lesion and non-root lesion cohorts ( Table 7 , P = 0.059).
Medial and Lateral Compartment Outerbridge Scoring Classified as Low (0-2) or High (3-4) Between Root Repair and Meniscectomy Groups.
Discussion
In a study conducted by Matheny et al., 19 patients with a medial root tear were 5 times more likely to have an articular cartilage defect with an Outerbridge score of grade 2 or greater. The results of our study confirmed this correlation, as it was found that patients with root lesions had more severe patellofemoral cartilage damage than patients with non-root lesions. This study went further to classify chondral wear separately for the patella and trochlea. Meniscal root repair is a relatively new procedure when compared to meniscectomy. Considering that patients who had a root lesion and underwent a root repair had more severe preoperative patellofemoral cartilage lesions, it is important to consider how beneficial a root repair may be if these patients may need a total knee arthroplasty (TKA) in the future.
Root repairs have been found to have better patient-reported outcomes at a 10-year follow-up than partial meniscectomies. 21 When comparing postoperative long-term outcomes, a higher rate of osteoarthritis and conversion to TKA has been observed in patients who had a meniscectomy than in those who had a root repair.15,21 This supports the claim that a root repair delays the progression of arthrosis. Furthermore, the root repair group showed significantly improved clinical scores, whereas the meniscectomy group did not. 21 Conversely, Perry et al. 22 found that repair did not significantly improve meniscal extrusion. Research has shown a significant association between severity of cartilage degeneration and extent of extrusion of the medial meniscus.3,23,24
When considering surgical options in patients with a root repair, unicompartmental knee arthroplasty (UKA) has been reported to be a good alternative to preserve function and quality of life when nonoperative measures have failed.25,26 Root repair may be a better option for patients who want to delay arthroplasty, while UKA can allow immediate weight-bearing and a faster return to activities of daily living.
Some limitations of the present study include the small sample size, retrospective analysis, and 1 evaluator. Root repair is a less common and newer procedure than meniscectomy, limiting the number in each group. In addition, there was only one evaluator who completed the MRI scoring. However, to eliminate bias, the evaluator was blinded, and the cases were randomized.
Conclusion
Patients with posteromedial meniscal root lesions had more severe patellofemoral cartilage degeneration than patients without root lesions. Future research will focus on whether or not patellofemoral chondral wear portends a worse outcome in patients undergoing root repairs.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Andreas Gomoll receives consulting fee from Vericel Corporation, Bioventus LLC, Organogenesis, Inc., Smith & Nephew, Joint Restoration Foundation, Inc., Flexion Therapeutics, Inc., and Moximed, Inc; honoraria from Vericel Corporation and Fidia Pharma USA Inc.; hospitality payments from Bioventus LLC, Organogenesis, Inc., Smith & Nephew, Joint Restoration Foundation, Inc., Pacira Therapeutics, Flexion Therapeutics, Inc., and Aesculap Biologics, LLC; royalty or license from Organogenesis, Inc.; compensation for services other than consulting, including serving as faculty or as a speaker at a venue other than a continuing education program, from Pacira Therapeutics; Compensation for serving as faculty or as a speaker for a nonaccredited and noncertified continuing education program from Linvatec Corporation; and has stocks in Engage Uni LLC. Dr. Sabrina Strickland receives honoraria from Vericel Corporation and Joint Restoration Foundation, Inc.; consulting fee from Vericel Corporation and Flexion Therapeutics, Inc.; hospitality payments from Vericel Corporation, Flexion Therapeutics, Inc., Bioventus LLC, Aesculap Biologics, LLC, Zimmer Biomet Holdings, Inc., Fidia Pharma USA Inc., DePuy Synthes Sales, Inc., Joint Restoration Foundation, Inc., Smith + Nephew, Inc., Dynasplint Systems Inc., Pacira Therapeutics, and Organogenesis, Inc.; compensation for services other than consulting, including serving as faculty or as a speaker at a venue other than a continuing education program, from Smith + Nephew, Inc.; and gift from Engage Uni LLC.
Ethical Approval
This study was approved by the Hospital for Special Surgery Institutional Review Board (2020-2123).