
Abstract
Background: Participation in football can put both male and female players at an increased risk for knee osteoarthritis. There is a higher prevalence of focal chondral defects in the knee of athletes compared to nonathletes. The management of chondral defects in the football player is complex and multifactorial. Objective: The aim of this study is to provide an overview of the current strategies for rehabilitation after articular cartilage repair of the knee in the football player. Design: A review of current literature and the scientific evidence for rehabilitation after articular cartilage repair of the knee. Conclusions: Articular cartilage repair has been shown to allow return to sport but rehabilitation timescales are lengthy. Successful rehabilitation for a return to football after articular cartilage repair of the knee requires the player to be able to accept the load of the sport. This necessitates a multidisciplinary approach to rehabilitation, especially in the transition from therapy to performance care. It should be recognized that not all players will return to football after articular cartilage repair. The evidence base for rehabilitative practice after articular cartilage repair is increasing but remains sparse in areas.
Introduction
The management of chondral defects in the football player is complex and multifactorial. Physical activity, including participation in football, has positive health outcomes. 1 However, participation in football can put both male and female players at an increased risk for knee osteoarthritis that often leads to functional limitations later in life.2-7 This football-related increased risk for degenerative joint disease can be explained in two ways. First, a major risk factor is a history of significant knee joint injury, 8 especially meniscal or anterior cruciate ligament (ACL) injuries.3,9-11,4,12, 13 Second, the sports-specific demands of football include high levels of impact and torsional loading that present an increased risk for players who are insufficiently trained to meet these demands.3,11
Football is associated with one of the highest rates of knee injuries in sport,14,15 and knee ligament injuries account for more than 30% of the total time lost from football for elite male and female players. 16 Injuries to the articular cartilage surfaces of the knee joint are commonly associated with ACL injury 17 and there is a higher prevalence of focal chondral defects in the knee in athletes compared to nonathletes. 18 Articular cartilage repair (ACR) has been shown to allow return to sport,19-21 with timescales for return ranging from 6 to 18 months (Table 1).22-27 With more than 265 million people playing football worldwide, 28 the prevention and treatment of chondral injuries is a priority issue. There is currently no consensus on the rehabilitation of chondral injuries. Clinical algorithms have been published outlining surgical treatment options for chondral injuries.29-31 Further considerations for a football player considering ACR surgery include consideration of their level of play, the time into the season, and their career status.24,27,10 Following ACR, the ultimate rehabilitation goals are, where possible and desired, to return the player to football at the same level without compensations and to prevent injury recurrence and longer term sequelae. However, it should be recognized that ACR rehabilitation is lengthy and generally longer for football compared with lower impact sports. Pertinently, not all players will be able to or will choose to return to football after ACR.
Return to Sport Timescales Following Articular Cartilage Repair
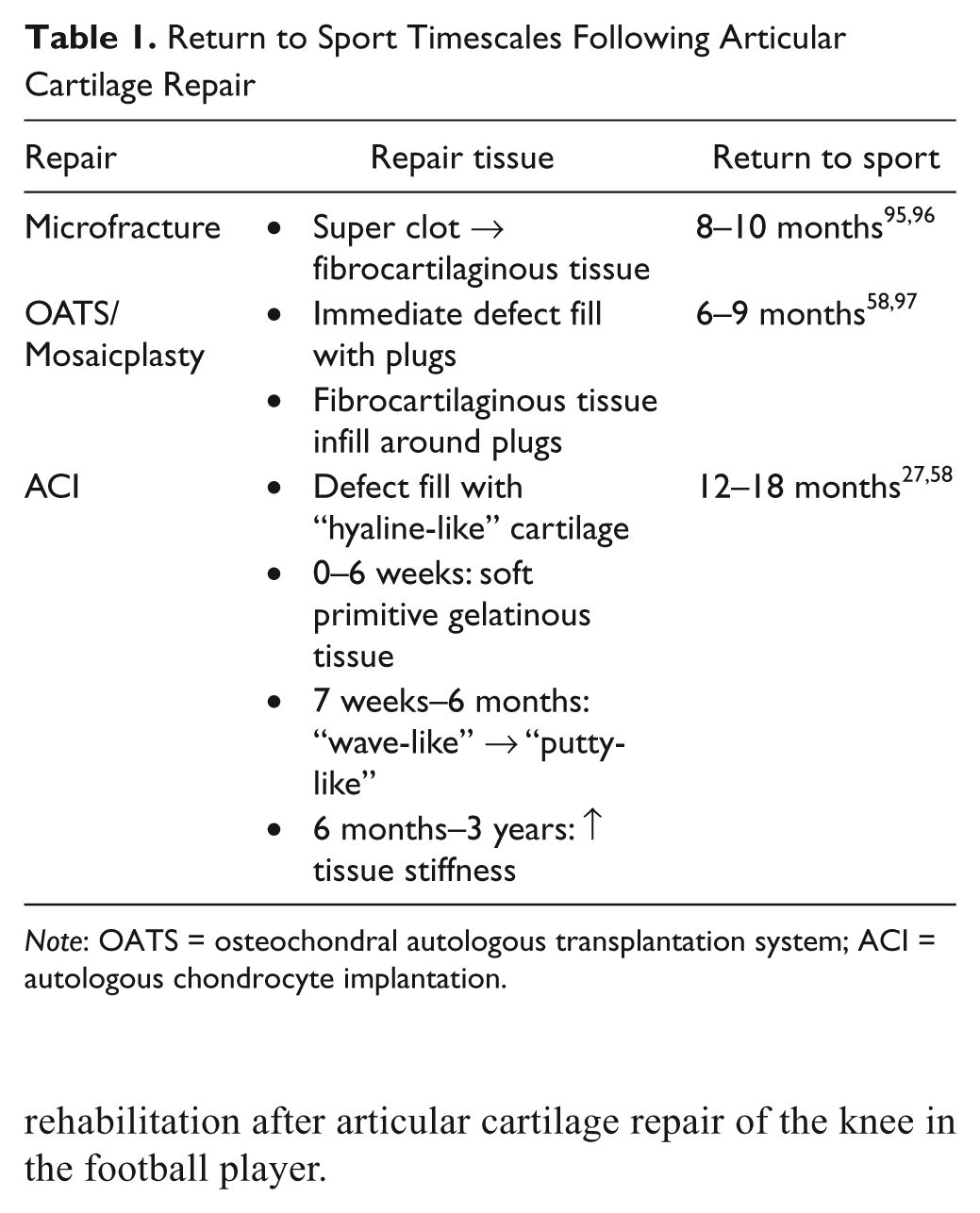
Note: OATS = osteochondral autologous transplantation system; ACI = autologous chondrocyte implantation.
The aim of this study is to provide a short overview of the current strategies and scientific evidence on rehabilitation after articular cartilage repair of the knee in the football player.
Cellular and Molecular Perspective of Healing after Articular Cartilage Repair
In contrast to childhood, the adult athlete is not able to intrinsically repair traumatic or repetitive overload injuries to the articular cartilage.32-34 This is, besides mechanisms like cell apoptosis and for example the presence of catabolic enzymes, due to the inability of differentiated chondrocytes to multiply themselves sufficiently in the tissue to reach the site of injury by migration in the extracellular matrix (ECM).35,36 A higher grade cartilage injury (III° or IV° according to the ICRS grading system of cartilage lesions 37 ) leads to a shift in the balance toward cartilage degradation.38-40 This results in greater deformation of the cartilage under the enormous impact forces of sports and thereby structural damage of the ECM. 41
The biological processes that influence the immediate rehabilitation after surgical treatment are comparable to those involved in general wound healing. The basis of wound healing is a nonspecific occlusion of the severed tissue structures to form a scar tissue that is directly linked to the invasiveness of the procedure. Molecular biological wound healing is controlled by a specific sequence of several growth factors and cytokines, which are responsible for the corresponding phases of wound healing.42,43 Depending on the extent of tissue laceration during surgery, an adequate inflammatory reaction of the organism is established to eliminate structural defects.
The treatment of specific cartilage defects can be distinguished between tissue transplants and cell-based regenerative techniques. The tissue transplantation techniques include the autologous osteochondral transplantation system (OATS) or tissue-engineered cartilage transplants.44,45 These methods carry the advantage that a primary load-stable cartilage tissue is anchored in the bone defect. Solely healing of the press-fit implanted cylinder and the integration with the surrounding cartilage requires temporary unloading similar to that in fracture healing. 44 In the cell-based techniques, potent cells (cultured chondrocytes in autologous chondrocyte implantation [ACI], bone marrow cells in the microfracture, and autologous matrix-induced chondrogenesis) are introduced in the defects alone or in combination with biomaterials.46-48 In an initial phase, the cells attach to the defect ground and then differentiate into specific metabolic active chondrocytes under the local biochemical and biomechanical conditions. The initially developed and even undirected collagen I network converts into a more or less sufficient repair tissue.49,50 As there is a lack of human data in this context, even taking into account all limitations of experimental models, those studies have identified three stages in cartilage regeneration.50,51 Phase I (Proliferative Phase, 0–12 weeks): After cell attachment, a nonspecific, soft repair tissue is formed. Phase II (Transition Phase, 3–6 months): A specific integration into the local environment and the improvement of the structural quality of the repair cartilage can be observed. Up to Phase II, the regeneration steps are similar in both the ACI as well as in the bone marrow–based technique. 52 Phase III (Remodelling and Maturation Phase, 6–24months): The final adaptation of the cartilage is made to the biomechanical needs of the various joint compartments. This process includes a period of up to 2 years, as seen in magnetic resonance imaging (MRI) studies. 53 The ACI proved to be superior in the quality of the regenerate tissue achieved compared with marrow stimulation techniques resulting in a longer maturation process. 54 Because of the very complex healing processes, to secure good results, a standardized rehabilitation depending on the methods, the defect location, and the associated injuries are required. 55
Rehabilitation after Articular Cartilage Repair
The primary objective for rehabilitation following ACR is the provision of an optimal environment for the functional recovery and adaptation of the chondral repair tissue, the knee, and the individual. Initial return to sport after ACR can range from 6 to 18 months as shown in Table 1. 19 The range in timescale for return to sport reflects the differences in the immediate postsurgery nature of the repair tissue across the ACR procedures29,56,57,21,58 and the speed at which the new tissue regains sufficient stiffness to accept the sports-specific load. 19 Postoperative ACR rehabilitation can both optimize or inhibit the process of repair tissue maturation. 59 The precise content and timelines for any ACR rehabilitation program will be dependent on a number of patient- and lesion-specific factors. These factors have been previously identified within the literature.55,19,60-66 In addition to these patient- and lesion-specific factors, for athletes there is also the need for a sport-specific approach to rehabilitation.50
Football-Specific Approach to ACR Rehabilitation
The construction of an ACR rehabilitation program for a football player requires an understanding of the demands of the sport especially in terms of the loading imposed on the repair tissue. Kreuz et al. demonstrated that physical training improves long-term results after ACI of the knee and should be performed for at least 2 years after surgery. 67 However, matching the physical training to optimize the adaptation while minimizing the risk of micro- or macropathological overload to the repair tissue is a challenge.
The early postoperative rehabilitative phase allows the body to recover from the effect of the surgical intervention and aims at providing sufficient protection for the repair tissue while minimizing the deleterious impact of reduced loading. Basic science evidence supports the use of continuous passive motion (CPM)68-70; however, there is limited evidence to support its impact on functional outcomes.
Cartilage requires mechanical stimuli for optimal adaptation. 71 Static compression and immobilization inhibit ECM biosynthesis whereas moderate dynamic compression and low shear loading stimulates ECM biosynthesis.72-77 Intermittent cyclic loading can be initiated with heel slides, the use of a stationary cycle with minimal resistance, or in an aquatic therapy environment once the surgical incision has healed. Loading can be slowly and progressively increased throughout the rehabilitation phases but requires close monitoring for signs of pathological overload. Because of the very different joint kinetics, separate rehabilitation programs are required for the tibiofemoral and patellofemoral joint. Generally, rehabilitation for patellofemoral ACR allows a faster progression of weight bearing (in extension) but requires a slower progression of range of motion when compared to tibiofemoral repairs. To minimize stress on the repair tissue, it is necessary to know the articulation range for the repair tissue and select appropriate exercises based on an understanding of the force and stress magnitudes that are generated with particular rehabilitation exercises.78,74,79,80
The introduction of sports specificity should be at the earliest opportunity without compromising the recovery of the player. Cardiovascular fitness can be maintained, or at least the decline slowed, through the use of arm ergometers (hand cycles) or partial weight bearing environments such as in aquatic therapy81,82 or differential air pressure treadmills. 83 Rehabilitation in a pool environment is a good way to reintroduce some early sports specificity, for example, heading a football to a therapist on poolside. Therapists should be cognizant that patients tend to exert more weight than they should in partial weight bearing 84 and that ACR surgery has been shown to result in gait dysfunction up to a year after surgery. 85 Rehabilitation behavior can be optimized through the strategic inclusion of goal-setting, the provision of social support, the generation of knee self-efficacy, and the management of psychological responses throughout the rehabilitation process.86-89
Return to Football
Return to high-impact activities, such as football, is often delayed to diminish the risk of damaging the implant secondary to adverse or premature loading. The paucity of research surrounding evidence-based return-to-play criteria and the inability to adequately assess the maturity of the graft continues to encourage conservative and lengthy management of the competitive athlete. 59 There is little high-level evidence to support one ACR procedure over another. However, promising short- and midterm outcome publications with a fair rate of return to preinjury level of sports can be achieved with cartilage repair and restoration in the athlete. 21 In addition, there have been several studies recently published to promote the notion of a more accelerated approach to postoperative ACI management.59,90-93 However, the current research supports an average time for return to full activity following ACI surgery ranging from 12 to 24 months. 51
When defining the criteria for return to sport, there is an emphasis on full restoration of strength and balance. It is critical to address the underlying pathokinematics, strength imbalances, and balance deficiencies at this time. Restoring optimal gluteal, posterior hip, and lateral hip strength and neuromuscular control will be critically important if any dynamic valgus or excessive lateral compartment loading at the knee was recognized on evaluation (Figure 1). It is important to continue to include manual therapy in this late phase of treatment.92,91,55 Joint mobilization of the patella, hip, femur and tibia-fibula may be indicated at this time.
Restoration of optimal gluteal, trunk and hip strength and neuromuscular control is important following ACR of the knee.
Sporting activities that are biomechanically demanding (football) should be incorporated when uniplanar activities can be completed successfully without subsequent joint effusion or any semblance of pathokinematic movement deficiencies, approximately the 10- to 18-month mark. However, a qualitative assessment is utilized with respect to activity progression rather than a quantitative one. Furthermore, if there was a concomitant surgical procedure performed at the time of the ACR, the physical therapist will factor this information into the exercise progression equation.55,91,64,63
Returning to field base activities can resume after completing a clinical rehabilitation protocol successfully. On functional testing, field activities can commence when there is less than a 20% strength deficit in knee flexion/extension and the ability to run on treadmill for 10 minutes at 8 km/h without pain or effusion. 59 Ideally, field sessions should include football-specific therapeutic activity (using the ball), should be 90 minutes in duration, and should occur 3 to 5 times per week. The sessions should increase in intensity and frequency without the observation of any adverse reaction to the functional stimuli. 59 The on-field therapeutic exercises have been divided into 5 phases:
Global coordination and straight-plane activities
Eccentric loading, single-leg plyometrics, and deceleration maneuvers
Running with change of direction, increase in aerobic intensity
Running backward, short distance passing, on-target shooting
Cutting, pivoting, sport-specific patterns simulating a match-level intensity and duration
It is critical to treat this injury as a multidisciplinary team that is actively engaged and communicating on a very frequent basis. The information that each discipline has to offer to the rehabilitation puzzle is paramount to the operative and functional success of the patient. Rehabilitation following ACR requires a thorough understanding of joint kinematics, and knowledge of the biologic and biomechanical properties of articular cartilage. 50 A dialogue should ensue prior to the surgical intervention and should continue well after physical therapy discharge, where the patient may resume therapeutic activities under the guidance of a certified athletic trainer, graduate sports therapist or a strength and conditioning professional. 94 This dialogue should be very specific with respect to what movement patterns can be safely integrated and which should be incorporated as qualitative milestones have been achieved. This dialogue should be inclusive of the coaching and management staff, as well as the entire medical community involved with the player, respectively.
Conclusions
Articular cartilage injuries can be career ending and player considerations should include the risk of reinjury and the risk of future disability. Successful rehabilitation for a return to football after articular cartilage repair of the knee requires the player to be able to accept the load of the sport from physiological, biomechanical, and psychological perspectives. This necessitates a multidisciplinary approach to rehabilitation especially in the transition from therapy to performance care.
Footnotes
The authors received no financial support for the research, authorship, and/or publication of this article.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.