
Abstract
Purpose: Osteoarthritis of the knee is a complex interaction of biological, mechanical, and biochemical factors that are further complicated by injury, which accelerates pathological processes within the joint. As a result, athletes, particularly those with a history of knee injury, have an earlier onset and higher prevalence of osteoarthritis that would be expected based on their age. This can present a clinical dilemma to the physician managing the patient who, despite the presence of radiologically confirmed disease, has few symptoms and wishes to maintain an active lifestyle. Methods: We reviewed meta-analyses and systematic reviews of randomized controlled trials about clinical management of knee osteoarthritis with special interest on effect sizes. Results: Numerous management options have undergone the rigor of clinical trials and subsequently have been summarized in meta-analyses and systematic reviews, the results of which offer evidence regarding varying degrees of effect. Based on the available evidence, most summaries and clinical practice guidelines suggest a regimen of patient education, self-management, weight control, and exercise supported by individualized pain management strategies. Other noninvasive or less invasive strategies are available that have varying degrees of effect. Conclusions: Although the evidence supporting many of the clinical management options might be considered modest, those effects are sufficient to permit an active lifestyle and have, given the prevalence of the disease, a public health impact.
The issue of osteoarthritis (OA) in the retired athlete can hardly be considered to be a recent development. Although it is hard to trace back to a time when OA was a new observation in athletes, Muckle 1 discussed the “footballer’s meniscus,” which included bucket handle or oblique tears of both meniscal horns that resulted in pain, swelling, and instability with many players showing signs but no symptoms. Injury was frequently associated with damage to the hyaline cartilage; players were delayed in returning to play; and when they did return, their “poor match agility” forced many to decrease their level of play. Importantly, repeat operations were associated with the onset of OA. The players with the worst outcomes were those with a lateral meniscectomy from the dominant leg. Professionals developed OA sooner (3-5 years post surgery) than did amateurs (5-7 years). As the average age of the index injury was 24 years, players displayed evidence of OA earlier than might be expected for their age. Muckle’s comment about the presence of radiographic signs in the absence of clinical symptoms underlines that the clinician’s role is directed at treating the patient’s symptoms, not the underlying disease.
Although the role of injury in the manifestation of knee OA is common knowledge, where athletic activity fits in the spectrum of risk factors can influence disease management decisions. Risk factors for OA, like most other sports injuries, can be categorized as either modifiable or nonmodifiable ( Table 1 ). In general, the obese, female African American, with a varus defect of the knee, and who frequently squats or kneels, has a high risk of developing knee OA. The athlete, especially one with a history of a knee injury, who has gained substantial weight after retirement and has not maintained good neuromuscular control of the muscles around the knee, hip, and ankle seems to develop OA at an earlier age than might be expected in the nonathletic population.2-5
Risk Factors for Osteoarthritis
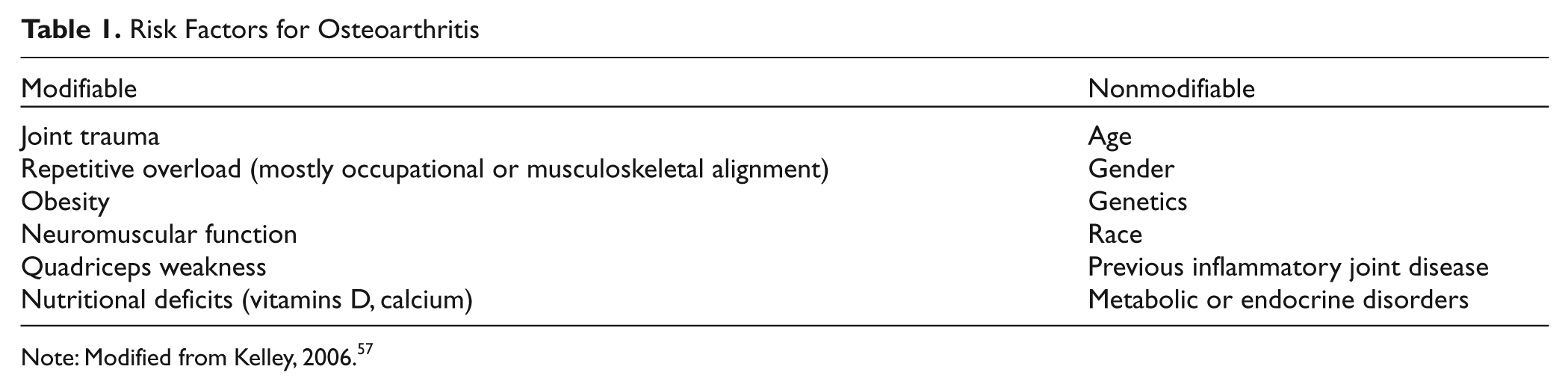
Note: Modified from Kelley, 2006. 57
It has been suggested that simply playing soccer may be a contributing factor for knee OA.3,6-11 Injury, however, specifically meniscal injury, seems to play a greater role4,7,12,13 and may have more influence on management decisions. Athletes cannot change their injury history, but they can manage their weight as well as strive to maintain optimal muscle function of the lower extremity to minimize the magnitude of the repetitive loads of daily activities and use the muscular system to absorb much of the load to delay, or prevent, the progression of OA. The front line in disease management includes a variety of strategies to support the athlete’s ability to continue routine activities.
Harvey and Hunter 14 argued that calling OA a “degenerative joint disease” minimizes the contribution of genetic, biochemical, mechanical, nutritional, and biological factors and that appropriate management of the disease needs to address each factor. Further, Lohmander and colleagues 13 stated that “osteoarthritis development in the injured joints is caused by intra-articular pathogenic processes initiated at the time of injury, combined with long-term changes in dynamic joint loading.” (pg. 1756) The focus of this review will be on systematic reviews and meta-analyses to present effect sizes (Note 1) in order to compare treatment effectiveness on a level playing field. We will outline the management options of OA for the retired athlete with specific focus on education and activity options to maintain and improve neuromuscular function of the lower extremity that will, we hope, modify those changes in dynamic joint loading.
Self-Management Practices
Education and Regular Patient Contact
A first step in managing the retired player with OA is supplying information about the importance of self-management. Players need to know that personal decisions and behaviors will influence how their OA affects their daily activities. Numerous recommendations stress the importance of patient education, consistent with what has been presented by the Arthritis Foundation. 15 The patient who understands the nature of OA, along with the benefits of changes in activity, exercise, and lifestyle modification, can realize a significant reduction in pain, even though the effect is not large. Recent reviews16-18 indicate that at low cost with few adverse effects, the well-informed patient makes more positive decisions regarding lifestyle. In addition, regular contact from the health care provider’s office aids in compliance, and therefore the patient experiences less pain. What specific individual aspect of a comprehensive self-management program produces the greatest effect is unknown. Regardless, that a small effect on a large fraction of the population should have a public health impact at a low cost or risk argues in favor of the central role of patients in the management of their disease.
Reduction in Body Mass
Given the interaction of regular physical training and caloric intake, athletes have an advantage when it comes to weight maintenance. Once they retire or reduce their commitment to their sport, however, many athletes fail to reduce caloric intake and thus gain body mass. For example, some of the leanest players in the National Football League (defensive backs and receivers) gain an average of 15 to 20 pounds in retirement (Marshall and Guskiewicz, 2011; personal communication). An increase in mass is known to increase loads on weightbearing joints, which likely exacerbates the development of OA through mechanical and metabolic means. 19 In addition, a high-fat diet leading to obesity (in mice) has been shown to induce osteoarthritic changes in the knee as well as decreased motor performance and selected behavior traits. 20 Patients who are overweight (body mass index >25) should be counseled to lose a minimum of 5% of their body mass through appropriate exercise and dietary modification; each unit reduction in body mass reduces load by 4 units. 21 This goes along with other well-known health benefits of similar weight loss.
Exercise
The exercise options available to the OA patient are somewhat limited because many options overload the knee to the point of increased pain and reduced function. Thus, only 30% of patients with early OA (Kellgren-Lawrence grade II or less; i.e., no joint space narrowing) meet U.S. Centers for Disease Control and Prevention or American College of Sports Medicine recommendations for daily physical activity, and only 1% perform any vigorous physical activity (>6.0 metabolic equivalents). 22
In vitro cartilage health is dependent on compression from cyclic, dynamic loading, properties of which are closely coupled with cartilage biology that increases chondrocyte anabolism as well as extracellular matrix components. 23 In vivo, moderate exercise also has an anabolic effect on cartilage. In older individuals, however, the loading from high-intensity exercise (or sudden onset of exercise or immobilization) can lead to degenerative changes in the collagen network. 24
Injury does not affect just the meniscus or articular cartilage. After rehabilitation from a knee injury, it is not unusual for the patient’s injured extremity to have enduring muscle weakness (frequently out of proportion to the loss of muscle mass, 25 suggestive of some manner of inhibition), reduced range of motion, and diminished proprioception that may continue to be evident years later. Weak quadriceps are deficient in their shock attenuation capabilities, transmitting loads across the knee at higher rates and magnitudes that effectively alter normal knee mechanics, 26 which could be a factor in accelerating the progression of OA on damaged tissues. 27 But the simple concept of exercise per se playing a role in the development of OA does not appear to be true, as there are no differences in the rate or radiographic evidence of OA after 2 decades of habitual running by middle-aged runners. 28
There is ample evidence that the strength of the thigh musculature in patients with OA can be improved, 29 but whether this results in greater muscle cross-sectional area, improved activation patterns, or slowed disease progression is unknown. 30 Although increasing the relative strength of the thigh muscles does appear to reduce the risk of developing OA in women, this has not been the case in men. 31 Further, evidence that increasing muscle strength will protect against OA in those with established OA is lacking. Despite muscle weakness being a factor in OA development, evidence supporting the benefits of increasing muscle strength is not compelling, possibly because of subject selection (e.g., patients with knee malalignment) or definition (slowed progression verified by radiographs). Regardless, it seems reasonable to speculate that the contributory mechanical factors of posttraumatic OA include persistent weakness, muscle inhibition, and the resulting joint instability. If this arthrogenic muscle inhibition (an inability to achieve full, voluntary activation of the quadriceps) 27 could be corrected, the progression toward OA might be retarded.
Although testing of this specific hypothesis continues to evolve, clinical trials on various aspects of exercise consistently report small to moderate effect sizes demonstrating that improvements in selected fitness factors do indeed reduce pain (a known factor in muscle activation) and improve function.29,30,32,33 Aerobic exercises like walking may only produce small to moderate effects in pain reduction and disability, but walking also leads to consistent moderate to large effects in the global assessment of benefit. 34
The systematic review by Roddy and colleagues 33 presents specific exercise recommendations based on evidence from the literature. They suggest an individualized program of strength and low-impact aerobic training to reduce pain and improve function and overall health that can be done individually or in a group setting and is based on patient-specific factors (e.g., age, comorbidities). Any program needs to be supported with education and feedback to promote a healthy lifestyle and maintain compliance.
These recommendations form the foundation of the Arthritis Foundation’s “Moving Is the Best Medicine” initiative. The American Geriatrics Society has produced an exercise prescription specifically for adults with OA pain that emphasizes flexibility, strengthening, and aerobic exercise ( Table 2 ). 35 Despite the lack of convincing evidence surrounding the mechanisms behind reductions in pain and disability, clinical trials of these protocols consistently demonstrate practical improvement by the patient, and therefore they should be considered as primary treatment modalities. 36
Exercise Prescription for Adults with Osteoarthritis
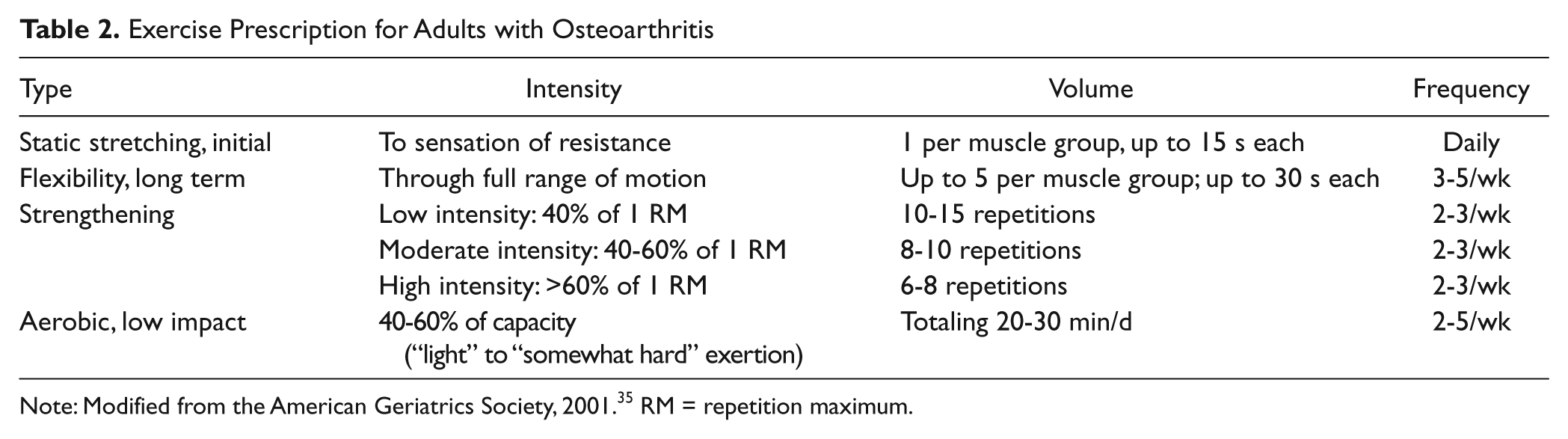
Note: Modified from the American Geriatrics Society, 2001. 35 RM = repetition maximum.
Medical Management
Analgesics
The primary goal of using analgesics is pain reduction to improve function and lessen disability. Targets for medications range from cellular components and cytokines to larger objectives like bone, cartilage, neurons, and the vascular supply.
The most common analgesic for mild to moderate pain is acetaminophen. For many, it is the first treatment option for pain relief; having only analgesic properties, acetaminophen is for pain reduction only. It has no impact on the underlying disease. In patients with symptomatic OA, the effect size for pain reduction in placebo-controlled trials has been stable at around 0.14 with no significant effects on stiffness or physical function. 37 Because of toxic metabolites, caution is necessary for the patient with kidney or liver disease as well as for patients who ingest even moderate quantities of alcohol. In general, however, standard doses (up to 4 g/d) are well tolerated with few side effects.
The anti-inflammatory and analgesic effects of nonsteroidal anti-inflammatory drugs (NSAIDs) reduce pain with an effect size reported to be 0.29 in placebo-controlled trials 38 and 0.20 compared with acetaminophen, 39 despite having no modifying effect on the underlying disease. 40 NSAIDs are, however, linked to gastrointestinal side effects that are worse when NSAIDs are combined with high doses of acetaminophen. 41
Topical NSAIDs have been recommended for symptomatic OA, and although the published effect size of 0.44 argues in favor of their use, there is the possibility of a publication bias with an underreporting of negative results.18,42 Topicals continue as a viable treatment option for pain relief because they are as effective as oral NSAIDs and possibly safer. 43
Opioids
Should acetaminophen or NSAIDs be ineffective for pain relief, opioids are typically the next treatment option, and the reported effect size of 0.78 indicates that these medications produce significant pain relief but less improvement in physical function (effect size = 0.31). 44 An effect size of this magnitude for pain reduction needs to be tempered because up to 25% of patients enrolled in trials of opioids voluntarily withdraw, leaving the remaining results as examples of a best-case scenario; in addition, opioids have a wide range of side effects.
Glucosamine and Chondroitin
Glucosamine is a component of joint cartilage and chondroitin sulfate that provides much of cartilage’s resistance to compression. The results of numerous clinical trials indicate that the effect size for glucosamine or chondroitin supplementation on pain relief is 0.46 and 0.79, respectively, but when only the highest quality trials are considered, these values fall to 0.29 and 0.005, respectively. 18 In addition, there are questions of publication bias, blinding, and relationships with funding sources. There has been a steady decline in the effect sizes and narrowing of the confidence intervals for both glucosamine (since 1981, from 2.24 to 0.58) and chondroitin (since 1996, from 1.4 to 0.75). 18 When only the highest quality studies are considered, the overall effect of glucosamine is modest and chondroitin has little benefit for the OA patient.
Acupuncture
The quest for pain relief and improved quality of life may lead a patient to inquire about acupuncture. To date, 11 randomized trials have compared acupuncture versus sham treatments, routine care, and patients on waiting lists. Trials comparing patients versus controls show a reasonable effect size of 0.58 for pain relief 45 that decreases to 0.35 when compared with sham acupuncture and diminishes further over time (0.13 after 6 months).18,45 Thus, although acupuncture might be a reasonable option for short-term pain relief, the data do not support long-term use.
Other Management Options
A number of other options have been investigated with varying degrees of methodological rigor and have shown varying degrees of success but might be considered for selected patients. 46 For example, patients with varus or valgus knee malalignment might be treated with specific braces. Patients with high loads on the medial compartment can be prescribed lateral heel wedges. Patellar taping, range of motion exercises, flexibility, and free-floating positional devices have been studied, but the results are mostly inconclusive (bracing) or devices have not been recommended (heel wedges, free-floating devices). Those devices recommended by the American Academy of Orthopaedic Surgeons are low cost, low harm, and low level of evidence (range of motion, flexibility) or appear to be effective in the short term (taping), but the studies on which these recommendation are based have design issues. 46
Injection Therapy
Corticosteroids
Intra-articular injection of corticosteroids for short-term pain relief in the OA patient is a therapeutic option with a long history of reliable data to support its use for rapid, if somewhat brief, pain relief. The pain relief from a single injection of corticosteroids is considerable in the first week, with an effect size of 0.72, but this falls to 0.28 by 4 weeks and 0.21 by 6 weeks. 47 In the short term, the effect size for pain relief in knees injected every 3 months for 2 years was 0.67 after the first year but only 0.25 after the second year. In addition, corticosteroids have little effect on stiffness or physical function. 47
Viscosupplementation
Intra-articular injections of hyaluronic acid (HA) to treat OA have become an option for patients in need of a treatment beyond routine exercise and analgesics but not requiring, or wanting, surgical intervention. Hyaluronan is one of the chief components of the extracellular matrix, contributes to cell proliferation and migration, coats each cell, and contributes to the tissue’s resistance to compression. It is thought that when HA is injected, it supplements the viscosity of the joint fluid and lubricates and cushions the joint, producing an analgesic effect.
Bellamy and coworkers 48 reported effect sizes (vs. placebo) between 0.54 and 0.61 for pain relief, improvement in physical function, and reduction in stiffness but reported issues regarding publication bias and significant heterogeneity when comparing the higher molecular weight hylan with the lower molecular weight HA. 18 For example, the meta-analysis by Reichenbach and colleagues 49 showed that when very strict controls were in place (e.g., blinding, concealment), the effect size for pain control approached zero. When compared with corticosteroids, in the first 4 weeks, there is little difference in pain reduction or a slight early advantage for corticosteroids vs. intraarticular injections of hyaluronic acid.
Platelet-Rich Plasma
Platelet-rich plasma (PRP) and other products that contain platelet-derived growth factors are bioactive components of whole blood that is injected into tissue with poor healing potential or sometimes as an intra-operative “gel.” Since the 1970s, the basic science literature has reported on whether PRP augments tissue regeneration through recruitment, proliferation, and differentiation of involved cells, showing median benefit duration of about 9 months in patients with knee OA. 50 Foster et al. 51 pointed out that the most reports are Level 4 case series, that basic science research still needs to define the many details regarding the cellular mechanisms of action, that current trials are statistically underpowered, and that study designs need to be carefully considered. PRP may be a significant new therapy for treating sports injuries in the future, “but there remains a significant amount of work before this becomes the standard of care.” (pg. 2271)
Surgical Interventions
Lavage and Debridement
Should nonsurgical management therapies prove ineffective, surgical intervention is considered. A full treatment of surgery is beyond the scope of this paper, and specific options are dealt with elsewhere in this supplement.
In 2002, Moseley et al. 52 reported the first randomized trial of arthroscopic procedures (debridement, lavage, sham) in a group of patients with knee OA and reported no group differences for pain or any other secondary pain or function variables. Whether the same results would be evident in patients with preexisting OA and new mechanical symptoms is unknown. Later systematic reviews showed little to no improvement in joint symptoms from lavage and irrigation.53,54
High Tibial Osteotomy and Arthroplasty
A number of studies of high tibial osteotomy (HTO) have been reviewed by the Cochrane Collaboration. The variability in surgical procedures, data collection, and reporting made any pooling of outcomes problematic. Nonetheless, the authors concluded there was “silver”-level evidence that valgus HTO is effective at reducing pain and improving function 55 while also allowing patients to return to preoperative activity frequency and duration, albeit with some modification and activity selection. 56 When unicompartmental arthroplasty and total knee arthroplasty are each compared with HTO, all 3 procedures improve function, with the unilateral procedure leading to fewer postoperative complications and a lower revision rate versus HTO.
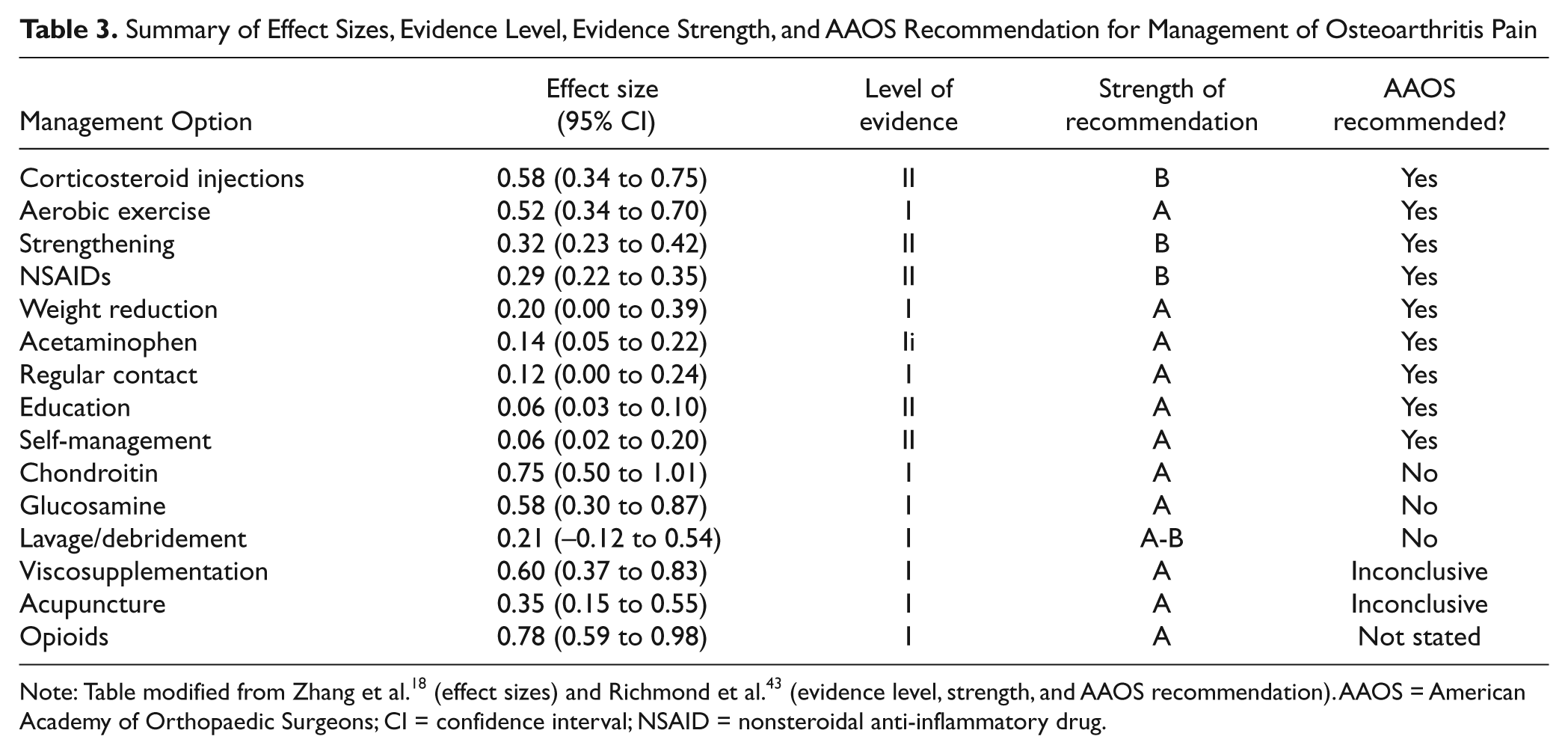
In summary, competitive sports, especially at an elite level, may increase the risk of OA, and it is not unusual for many athletes to have a higher grade of OA than would be expected for their age. Although many athletes have signs of OA, many have fewer symptoms than would be expected based on their level of radiologic disease. This may reflect the fact that their history of skilled neuromuscular function consistent with their sport activity can protect them from symptom-based limitations in their daily activities. The available evidence for managing OA in these patients, especially those who wish to continue with some level of activity, suggests that self-management, including moderate low-impact exercise, (Table 3) is effective at controlling pain and improving function. Exercise per se does not appear to accelerate the development of knee OA, and the mere presence of OA does not affect disability. Obesity, knee trauma, occupational stresses, or malalignment, however, will increase the risk of OA. Appropriate measures are effective in staying active and managing pain.
Summary of Effect Sizes, Evidence Level, Evidence Strength, and AAOS Recommendation for Management of Osteoarthritis Pain
Footnotes
The authors received no financial support for the research and/or authorship of this article.
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
1.
Effect size is a descriptive measure of the strength of a treatment effect. Originating in the social sciences, it is commonly used in meta-analyses to summarize data from multiple studies. Social scientists sometimes categorize effect sizes as small (0.2-0.3), moderate (around 0.5), and large (≥0.8).