
Abstract
Background
The representation of women in otolaryngology has increased significantly over recent decades, yet discrepancies remain in certain subspecialties, including rhinology. Despite overall improvements in gender equity within otolaryngology, the specific demographic trends and scholarly productivity of fellowship-trained rhinologists have not been thoroughly examined.
Objective
We aimed to address this gap by examining demographic trends and academic productivity among rhinology fellowship graduates.
Methods
This cross-sectional study examined publicly available data to analyze fellowship-trained rhinologists in the United States, focusing on gender, career stage, practice setting, h-index, and academic rank. Statistical analyses included Fischer's exact test, Wilcoxon rank sum test, ANOVA, and η2.
Results
We included 477 fellowship-trained rhinologists who trained at 31 fellowships. No gender differences in career stage or practice type were found. Despite an absolute increase in women per year (0 to 9, η2 = 0.65), the percentage of women in rhinology fellowships has plateaued since 2002 (η2 = 0.001), averaging 21.1% (SD = 10.8%). Most fellowship-trained rhinologists were mid-career, with a median of 7 practice years; 55% worked in academics, mainly as assistant professors. Overall, women rhinologists had a slightly lower h-index than men (7 vs 9; P = .01), but when stratified by academic rank, there was no difference in h-index between men and women.
Conclusion
The percentage of women fellowship-trained rhinologists has not increased since 2002 (η2 = 0.001), remaining at a mean of 21.1%. Contrasting with other subspecialties, women and men rhinologists have similar h-indices by academic rank. However, there are still fewer women in rhinology overall than men.
Keywords
Introduction
Over the past 2 decades, the percentage of women otolaryngologists has increased from 21% (2000) 1 to 37.5% (2018-2022). 2 There has also been a substantial increase in the number of otolaryngology trainees, reflected in the growth of residency and fellowship positions. 3 Past otolaryngology studies have exposed racial and gender discrepancies in academic rank, leadership roles, and scholarly productivity measured by h-index and grants.4–13 Recently, investigations have taken this concept one step further to explore whether the same gender discrepancies remain for otolaryngology subspecialties, including head and neck, laryngology, and facial plastics.14–16 Despite extensive studies on the landscape of otolaryngology, trends in gender representation among fellowship-trained rhinologists have not been analyzed.
The number of otolaryngology residents choosing to do a fellowship has increased from 45.6% to 61.5% from 2011 to 2019. 17 Although data suggests that gender does not predict interest in fellowship training, 18 80% of fellowship-trained rhinologists were men between 2007 and 2017. 19 Within other subspecialties, there has been improvement in women's representation. From 1995 to 2022, there was an increase in the percentage of women head and neck graduates (η2 = 0.18). 14 In Canada, women's representation in pediatric otolaryngology and laryngology has risen to more than 50% over the past decade. 7
In academic otolaryngology, improvements in women's representation, including the number of women on the tenure track (2007 to 2018), have been noted 20 ; however, studies suggest that gender differences in scholarly productivity remain. A 2013 study revealed gender discrepancies in academic productivity in otolaryngology, showing that men exhibited higher scholarly activity earlier in their careers while women achieved productivity levels equal to their male counterparts later. 21 Another study evaluating female representation as residency and fellowship directors found that women directors had a lower mean h-index than men (11 vs 17.5), a discrepancy that remained even after controlling for rank and years in practice. 4 McCrary et al explored demographic trends and scholarly productivity in American Head and Neck Society fellows, showing that women began their careers with high productivity levels but decreased over time relative to men. 14 On the contrary, another study demonstrated parity in otology, rhinology, and facial plastics subspecialties at all career stages. 22 Likewise, another facial plastics study demonstrated similar h-indices after controlling for years in practice (1.13 vs 1.14, P = .575). 15
Considering women's representation in otolaryngology has increased, 2 yet rhinology remains 80% men, 19 we investigated demographic trends within rhinology. With increased gender representation in otolaryngology as a whole, we hypothesized that the percentage of women rhinologists would increase over time. Given the limited understanding of factors influencing early career success among fellowship-trained rhinologists, we also investigated academic position and scholarly productivity.
Methods
This cross-sectional study analyzed data on fellowship-trained rhinologists to determine gender, career stage, practice setting, h-index, and academic rank of graduates. Data was collected from publicly available sources for all U.S. rhinology fellowship programs that were listed on the American Rhinologic Society (ARS) website. Data regarding demographics, practice location, and educational background were obtained from surgeons’ institutional web profiles, U.S. News and World Report, Doximity, LinkedIn, and the National Provider Identifier (NPI) registry. Gender, self-identified on NPI registry profiles, was collected using the NPI registry. Demographic variables were verified by confirming that at least 2 sources provided identical and recent information.
The practice setting was categorized as either private practice or academic, with academic defined as the title of an assistant, associate, or full professor. Consistent with other reports, early career was defined as less than 5 years in practice.14,15 Mid-career was 6 to 10 years in practice, and the late career was defined as more than 11 years in practice. 14 Education and self-identified gender were obtained from Doximity and U.S. News and World Report. h-index, number of publications, and citations were determined via Scopus author search. The highest h-index was selected for individuals with multiple listings on Scopus. Data was collected in January of 2024.
Statistical Analyses
Data normality was assessed using the Shapiro–Wilk test. Fischer's exact test, Pearson's Chi-squared test, and Wilcoxon rank sum test were used. Linear regression and η2 were used to determine effect size. A P-value less than .05 was statistically significant. Data were analyzed in R Studio Version 1.3.1093 (RStudioInc., Boston, MA).
Results
A total of 477 fellowship-trained rhinologists were included in this study. There were no gender baseline-covariate differences in years in practice, career stage, practice type, or academic rank (Table 1). Between 1989 and 2023, the number of fellowships increased from 1 to 27 (η2 = 0.92) and fellowship positions from 1 to 35 (η2 = 0.91) (Figure 1A). The absolute number of women graduates per year increased from 0 to 9 (η2 = 0.65). However, the percentage of women rhinology fellowship graduates has not increased since 2002 (η2 = 0.001), remaining at a mean of 21.1% (SD = 10.8) (Figure 1B).
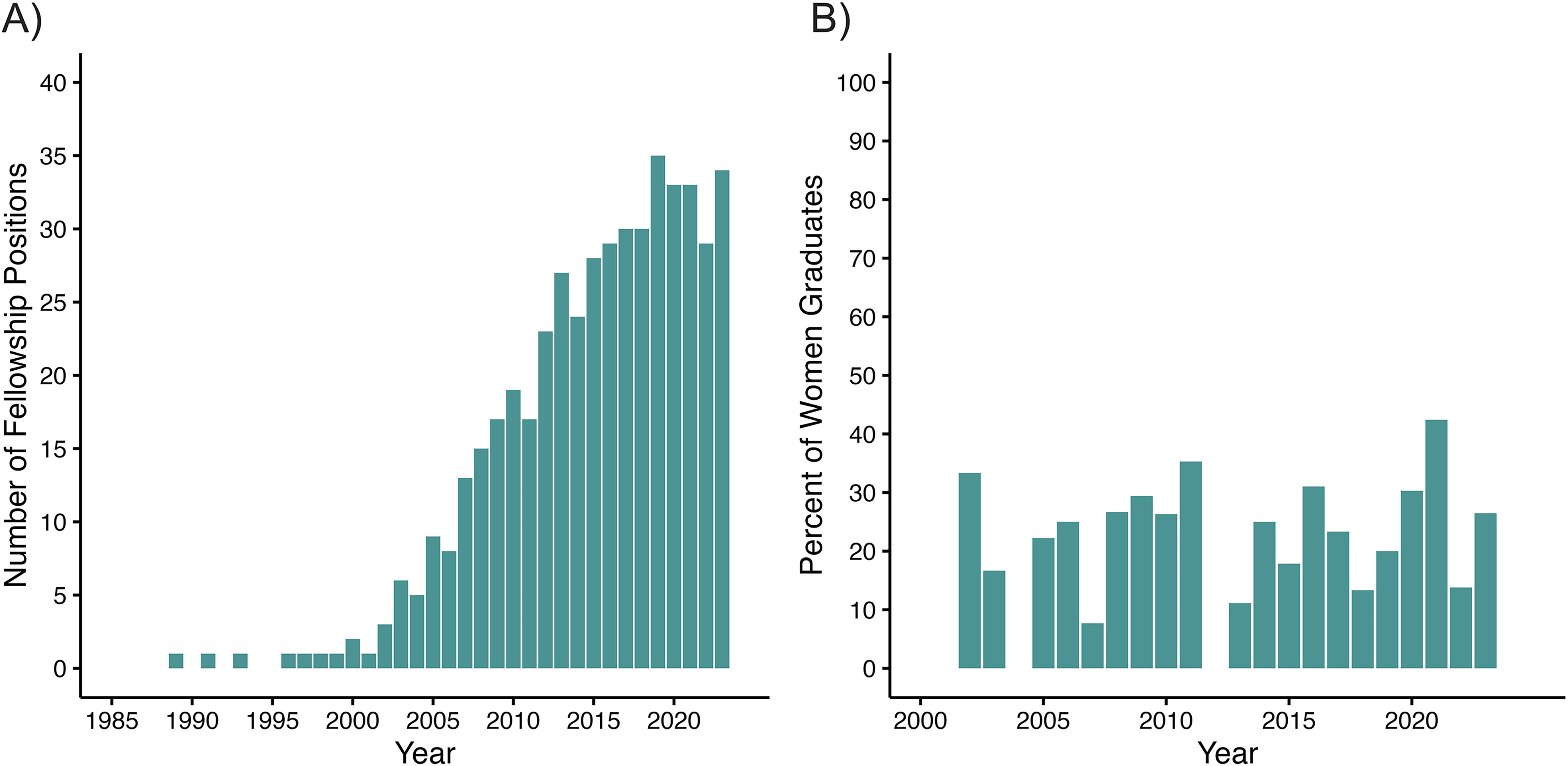
Fellowship positions have increased since the early 2000s but have plateaued in recent years; however, the percentage of women has remained stable since 2002. (A) The number of fellowship positions by year. From 1989 to 2023, there was a large increase in the number of positions (η2 = 0.91). (B) The percentage of women fellowship graduates by year. From 2002 to 2023, there was not an increase in the percentage of women graduates (η2 = 0.001).
Characteristics of Women and Men Rhinology Fellowship Graduates.
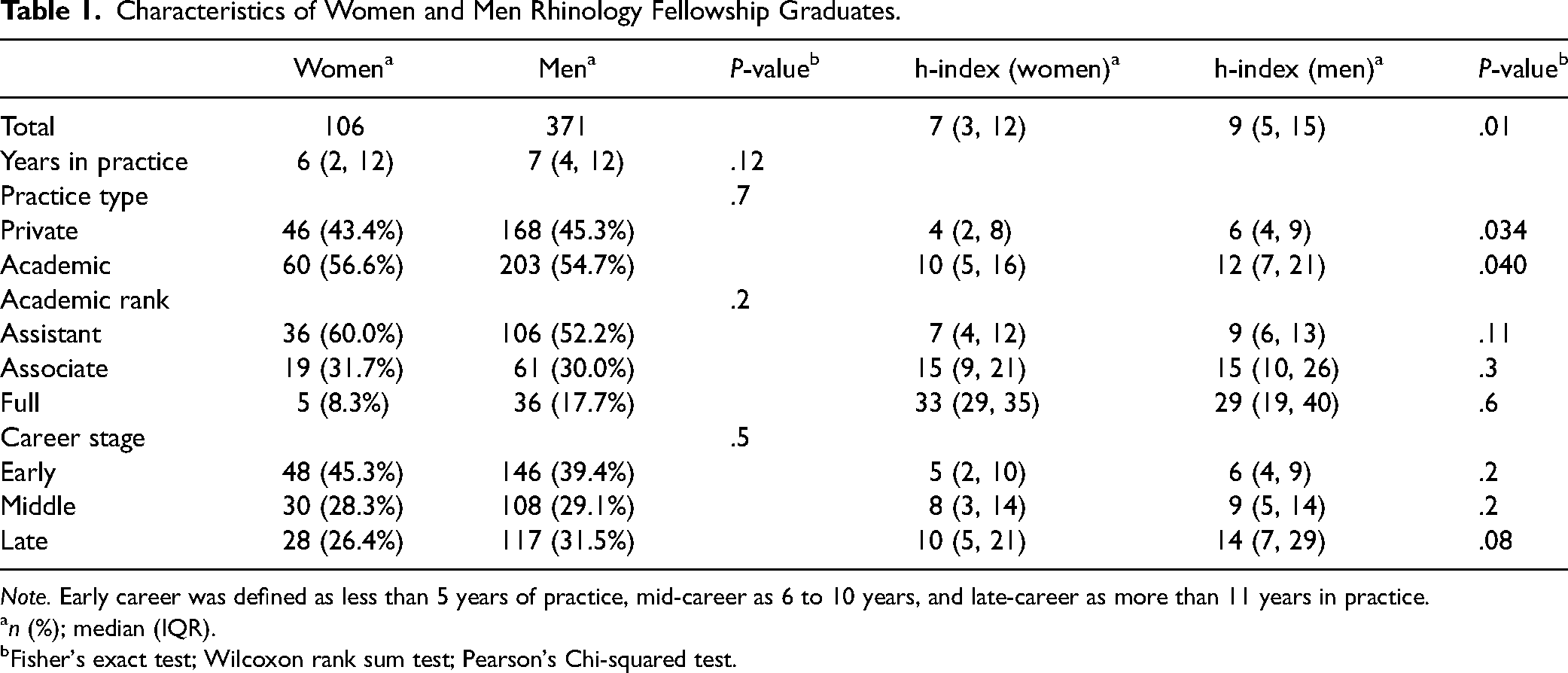
Note. Early career was defined as less than 5 years of practice, mid-career as 6 to 10 years, and late-career as more than 11 years in practice.
n (%); median (IQR).
Fisher's exact test; Wilcoxon rank sum test; Pearson's Chi-squared test.
At the time of analysis, the majority of rhinologists were categorized as mid-career, and the median years in practice was 7 (IQR 3, 12). Fifty-five percent (263/477) reported working in academics, and most were assistant professors (54%, 140/255). The overall median h-index was 8 (IQR 5, 15). While practice type, career stage, and academic rank were similar among women and men, there were statistically significant gender-based differences in the h-index (Table 1).
Gender differences in h-index were observed across practice types. Within both private and academic practices, women rhinologists tended to have slightly lower h-indices (private: 4 [IQR 2, 8] vs 6 [IQR 4, 9]; P = .034, academic: 10 [IQR 5, 16] vs 12 [IQR 7, 21]; P = .040). There were no gender-based differences in h-index in subgroup analysis based on career stage. Likewise, in subgroup analysis based on academic rank, there were no statistically significant differences in the median h-index at any rank (assistant, associate, or full professor).
Overall, women rhinologists had a lower median h-index than men (7 [IQR 3, 12] vs 9 [IQR 5, 15]; P = .01). When analyzing rhinologists in academics, women had a lower h-index than men (10 [IQR 5, 16] vs 12 [IQR 7, 21]; P = .04). At the assistant professor level, women had a nonstatistically significant lower h-index to men (7 [IQR 4, 12] vs 9 [IQR 6, 13]; P = .11). At the associate professor level h-index between men and women was equal (15 [IQR 9, 21] vs 15 [IQR 10, 26]; P = .3) and at full professor levels women had a nonstatistically significant higher h-index than then men at the same rank (33 [IQR 29, 35] vs 29 [IQR 9, 39]; P = .06). When characterizing based on years after training, in early career, h-index was similar between women and men (5 [IQR 2, 10] vs 6 [IQR 4, 9]; P = .2).
Discussion
The field of otolaryngology has seen a notable increase in women's representation over the last decade, reflecting broader trends toward gender equity in medicine. This progress is encouraging; however, when examining subspecialties like rhinology, disparities persist. While there has been a drastic increase in rhinology fellowship programs (η2 = 0.92), our data show the percentage of women rhinologists has plateaued since 2002, remaining at 21%. This stagnation raises questions about potential barriers to gender parity in this subspecialty.
One reason for the limited representation of women in rhinology may be the lack of available role models and mentors in the field. The low percentage of women already present may create a cycle where fewer women choose to enter the specialty due to insufficient visible representation and mentorship opportunities. Systemic issues, such as unequal access to networking opportunities, research funding, and leadership roles, may also play a role. These biases may discourage women from pursuing this subspecialty or create further obstacles during their training and career advancement.
Despite these barriers, our results do not elucidate differences in h-index based on academic rank or career stage. At the assistant, associate, and full professor levels, h-index was not statistically different between women and men. These findings contrast previous research in other otolaryngology subspecialties, which found differences in productivity at the assistant level, which tended to diminish as their careers progressed.21,22
One hypothesis for these findings is that women entering rhinology may already represent a highly self-selected, research-minded group. Additionally, increasing awareness of gender disparities in academic medicine may have prompted institutions to adopt more equitable practices, particularly in recent years, thus narrowing the productivity gap. It is also possible that the collaborative nature of rhinology research fosters environments where individual demographic factors have less influence on productivity. Lastly, there are limitations in using the h-index as a metric for scholarly productivity.
The h-index does not account for variations in citation practices across disciplines, potentially disadvantaging researchers in fields with lower citation rates. Additionally, it overlooks collaborative contributions and the relative importance of highly cited papers. The metric can be influenced by name changes or inconsistent author identification, which may disproportionately affect certain groups: those who change their names after marriage, those with hyphenated last names, and those with 2 last names. While the h-index is a useful tool, it should be interpreted alongside other qualitative and quantitative measures to provide a more comprehensive view of scholarly impact.
Incorporating qualitative assessments into evaluations of scholarly productivity can address the limitations of quantitative metrics like the h-index. Peer reviews and narrative evaluations provide context that numbers alone can't capture, enhancing our understanding of a researcher's contributions. Additionally, implementing persistent identifiers like ORCID IDs ensures consistent attribution of publications and citations by reducing errors in name-based identification.
Our study is limited to publicly available data, which only includes individuals who successfully matched into rhinology fellowships. Given our restricted analysis, we were unable to evaluate differences in matched and unmatched applicants, nor determine whether women are less likely to match into rhinology or less likely to apply to rhinology fellowships. Thus, to better understand why this disparity exists, an important focus for future research should be analyzing more comprehensive data on all fellowship applicants.
Given that demographic information was restricted to publicly available profiles, this data is susceptible to inaccuracies and may be constricted based on website settings. Although our gender data fell into 2 categories, gender exists along a spectrum, and binary categorization may fail to represent many individuals. This limitation underscores the need for more inclusive data collection practices that respect and reflect the diversity of gender identities within the field. Additionally, this analysis is limited by a lack of race and ethnic demographic data, restricting our ability to understand the impact of race and gender intersectionality. The absence of such data prevents a comprehensive understanding of how systemic inequities affect individuals differently based on the interplay of race, ethnicity, and gender. Future research should aim to incorporate these dimensions to provide a more holistic view of diversity and equity within rhinology and other medical subspecialties.
Conclusion
The percentage of fellowship-trained women rhinologists does not mirror the percentage of women otolaryngologists. Since 2002, there has been a plateau of women rhinologists at 21%, indicating the need for further initiatives to encourage gender equity. There were no h-index differences by academic rank. Recognizing the challenges women rhinologists face is crucial for addressing gender disparities and representation, and stagnant female representation underscores the need for further gender equity initiatives. Future research should also explore racial diversity to address inclusion in otolaryngology comprehensively.
Footnotes
Authors’ Note
This article has been presented as a poster presentation at the ARS at Academy in Miami, FL on September 27–28, 2024.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was determined to be exempt by the Office of Human Research Ethics at the University of North Carolina—Chapel Hill (IRB#23-3122).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.