
Abstract
Objective
The purpose of this study is to characterize the presentation, outcomes, and barriers to care for White and non-White patients undergoing endoscopic sinus surgery (ESS).
Background
ESS is often successful in providing long-term relief for patients suffering from chronic rhinosinusitis (CRS). Literature that uses robust measures of socioeconomic status (SES) and barriers to care to assess ESS outcomes is limited.
Methods
A retrospective matched cohort study of patients who underwent ESS for CRS between 1/1/2015 and 6/1/2021 at a single tertiary care academic center was conducted. White and non-White patients were matched 1-to-1 by sex and age (± 5 years). SES was evaluated using the area of deprivation index (ADI).
Results
Of the 298 patients included in the study, 149 are White and 149 are non-White, 111 (37.2%) have CRS with nasal polyposis (CRSwNP), 141 (47.3%) had allergic rhinitis, 90 (30.2%) had asthma and 22 (7.4%) required revision ESS. Non-White patients were 3.62 times more likely to present with CRSwNP (95% confidence interval [CI] 2.2-5.96) and had 2.87 times increased odds for requiring revision ESS than age and sex-matched White patients (95% CI 1.090-7.545). The median ADI for non-White (6.00) patients was higher than for White patients (3.00) (P < .001) and 21.5% more non-White patients presented with Medicaid (P < .001).
Conclusion
Non-White patients undergoing ESS for CRS are more likely to present from areas with fewer resources and be underinsured. Using robust measures of SES, such as ADI, may allow for care to be tailored to patients with barriers to care.
Keywords
Background
Chronic rhinosinusitis (CRS) is a common inflammatory condition characterized by paranasal sinus inflammation that significantly impacts the quality of life.1–4 CRS impacts millions of Americans of all races and costs up to $6 billion annually.4,5 Functional endoscopic sinus surgery (ESS) is the standard of care procedure for treating CRS refractory to adequate medical therapy and has proven to be effective in improving both subjective and objective measures of disease burden. 5 However, ESS can fail to control symptoms and patients and between 4% and 19.1% of patients require revision ESS. 6
Race plays an important role in determining access to surgical treatments and postoperative complications in a multitude of fields.7–10 However, little is known about the link between race and ESS outcomes, as minority patients are often underrepresented in clinical trials within rhinology. 11 Furthermore, only 10% of the literature regarding the impact of race in studies assessing CRS provides information regarding race and ethnicity. 12 The current literature is conflicting. Bergmark et al 13 demonstrated that patients with CRS that presented to a rhinology center had similar metrics for CRS severity and prepresentation medical management regardless of race/ethnicity, education status, or zip code-based income level. However, a large prospective cohort study conducted by Konsur et al 14 demonstrated that African American patients with CRS had less frequent follow-up and worse SNOT-22 scores after 40 months of follow-up. Decreased access to care and infrequent follow-up have also been associated with disease severity as adult Black patients with CRS have been shown to have more frequent hospitalizations due to asthma, and Black children undergo disproportionately higher rates of urgent and emergent ESS. Racial disparities have been shown to manifest at a pathologic level, with Black patients having greater eosinophil counts in the nasal mucosa. 15 While the reason for this is unclear, it is hypothesized that this is due to decreased access to care leading to more severe disease presentation for Black patients. 15 Race and ethnicity have been shown to have a significant impact on presentation and immediate postoperative outcomes following ESS.12,16,17
The literature regarding the impact of socioeconomic status (SES) on ESS outcomes is also limited and conflicting. A 2016 prospective case-control study conducted by Philpott et al 18 determined there was no difference in SES in those diagnosed with CRS and those without CRS. Having Medicaid, however, has been shown to predict increased eosinophil count in the nasal mucosa and worse overall health outcomes.13,15 In addition to being limited in quantity, studies assessing the impact of race and SES on CRS outcomes often use broad and unidimensional measures of SES such census-based household income and insurance status. While important, these factors do not account for other aspects of disparity such as education, employment, and housing quality. In recent years, more robust metrics of SES have been developed to account for a multitude of factors including the area of deprivation index (ADI).
The purpose of this study is to characterize outcomes and presentations of White and non-White patients undergoing ESS for CRS using comprehensive measures of socioeconomic factors and barriers to care.
Methods
Study Design
This is a single-center retrospective matched cohort study of patients undergoing first-time ESS for CRS between 1/1/2015 and 6/1/2021 (n = 298).
Study Population
Study participants were identified using CPT codes 31267, 31276, 31255, 31254, 31256, 31259, 31257, 31253, for ESS. In total, 1445 patients were identified using CPT codes with confirmed ESS. Individual patient charts were then examined to identify patients between the ages of 18 to 89 with a diagnosis of CRS as defined by the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020 who have not had prior ESS. 19 There were 688 patients who underwent prior ESS and 52 outside of the 18 to 89 age range were excluded. Twenty-three patients were excluded due to cystic fibrosis or sinonasal tumors. A total of 682 patients between the ages of 18 and 89 who underwent primary ESS between 1/1/2015 and 6/1/2021 were identified.
White and non-White patients were matched automatically 1-to-1 by sex and age (± 5 years). After matching, a total of 298 patients were included (149 White and 149 non-White patients), and matches were not found for 385 patients. Race in this study was independent of ethnicity, therefore, Hispanic patients were categorized based on race. Variables collected included demographic factors such as age, sex, race, Zip Code; sinonasal comorbidities such as diagnosis of asthma, allergic rhinitis, nasal polyposis, aspirin sensitivity, and Samter's Triad. Preoperative SNOT-22 and 6-week postoperative SNOT-22 were also collected.20–23 Response to SNOT-22 was determined using the minimal clinically important difference of 9 points. Diagnosis of immune disease, defined as the presence of a diagnosed autoimmune disease (ie rheumatoid arthritis, Crohn's disease, granulomatosis with polyangiitis) or immune deficiency (ie, common variable immune deficiency, human immunodeficiency virus, or hematologic malignancy), was collected. Patients were considered lost to follow-up if they had less than 3 visits with rhinologists within 12 months of surgery. Patients were considered to have a “lapse in care” if they had less than 3 visits with a rhinologist within 12 months of surgery but then returned for more visits following the initial 12-months postoperative period. All endoscopic sinus surgeries were performed by 2 fellowship-trained rhinologists at an academic medical center in Cleveland, OH.
Area of Deprivation Index
SES was determined using the ADI, a composite measure of 17 factors including income, education, employment, transportation access, and housing quality to provide neighborhood level insight into SES. 24 ADI ranges from 1 to 10 with higher numbers indicating a greater degree of deprivation. 24 In total, 9-digit zip code was used to extract ADI for each patient. The ability to use neighborhood-level 9-digit zip code is the main advantage of ADI over other measures of SES such as social vulnerability index (SVI) and census tract data as these variables provide county-level measures as opposed to more granular neighborhood-level data.
Statistical Methods
Demographic and clinical characteristics were presented using means with standard deviations for parametric variables and medians with ranges for nonparametric variables. Frequencies and percentages were utilized for categorical variables. Categorical variables were compared using Chi-square tests. Additional comparisons among patient groups were performed using independent sample t-tests or Mann-Whitney U test, as appropriate. Multivariate linear regression was utilized to characterize the presentation and outcomes of individuals based on ADI. Binary logistic regression was used to evaluate the odds of revision sinus surgery based on race, disease presentation, and ADI. Odds ratios (OR), proportion difference (PD) with 95% confidence intervals (CI), median difference, and mean difference were used for effect size as appropriate. All analyses were performed using SPSS Version 28 (IBM SPSS Statistics 28). P values less than .05 were considered statistically significant.
Results
Study Population
A total of 298 patients (149 White and 149 non-White) underwent primary ESS between 1/1/2015 and 6/1/2021 and were included in the cohort matching. Of these patients, 202 (68%) were female, and the median age was 41 years (range: 18-86). The large majority of patients in the non-White cohort were Black (n = 131, 88%). Three patients were Asian (2%) and 15 (10%) indicated “Other” race. Of the 149 White patients, 2 (1%) identified as Hispanic and the remaining 147 (99%) were non-Hispanic. Baseline demographics are presented in Table 1.
Baseline Demographics, Comorbidities, and Outcomes.
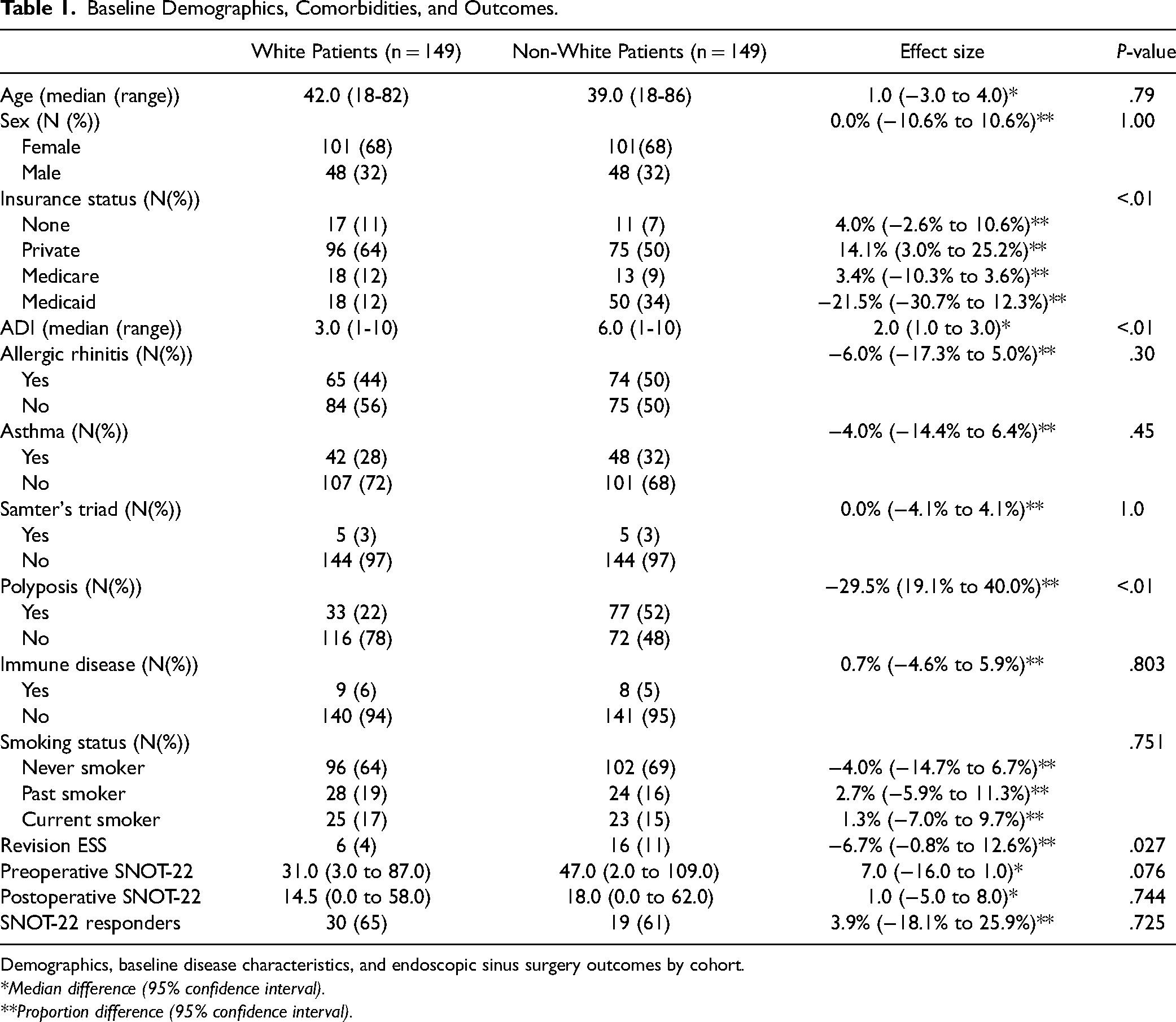
Demographics, baseline disease characteristics, and endoscopic sinus surgery outcomes by cohort.
*Median difference (95% confidence interval).
**Proportion difference (95% confidence interval).
Barriers to Care
Non-White patients receiving ESS presented from areas of with higher deprivation indices (6 (range 1-10)) than White patients (3 range (1-10)) (Median difference = 2.0; 95% CI: 1.0-3.0; P < .01). Non-White patients were also more likely to present with Medicaid as their insurer (34%) than their age and sex-matched White counterparts (12%) (PD: 21.5%, 95% CI: 12.3%-30.7%) and White patients were more likely to present with private insurance (64% vs 50%; 14.1% difference, 95% CI: 3.0%-25.2%). Multivariate analysis was conducted to better characterize disease outcomes and presentations of patients based on ADI. When controlling for other variables, race (β = 1.75; 95% CI: 1.033-2.463; P < .01) and requiring revision sinus surgery (β = 1.32; 95% CI: 0.03-2.60) were independently associated with ADI. The results of this linear regression are presented in Table 2.
Factors Associated with Area of Deprivation Index (ADI).
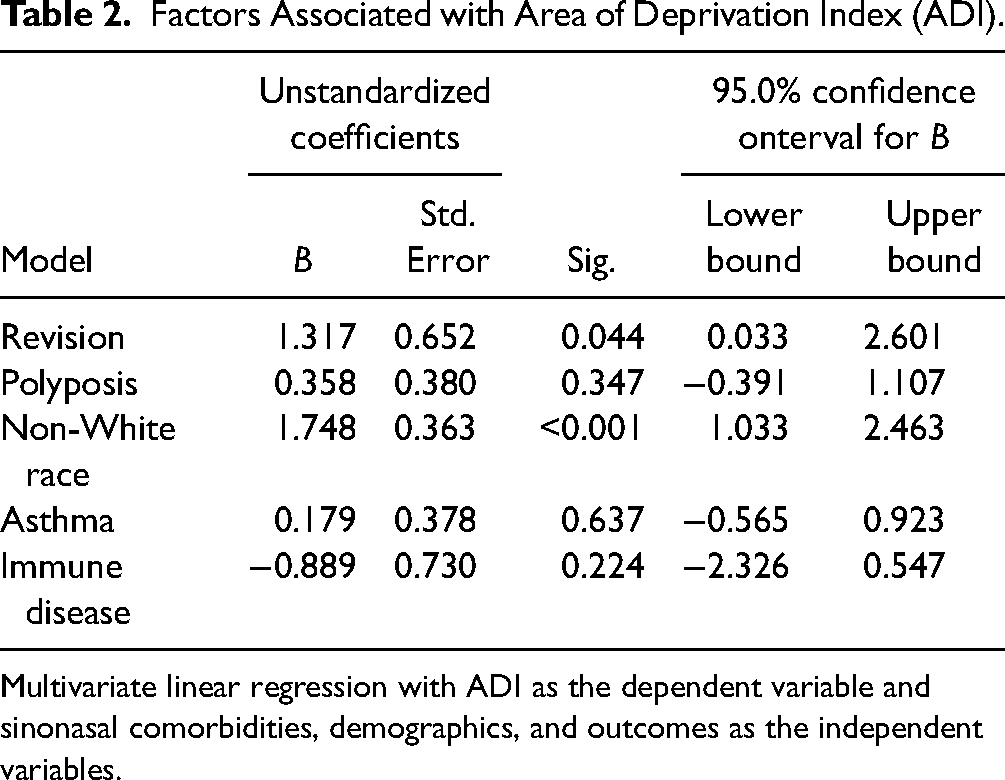
Multivariate linear regression with ADI as the dependent variable and sinonasal comorbidities, demographics, and outcomes as the independent variables.
Sinus Surgery Outcomes
All patients included in this study underwent ESS for CRS and 22 (7.4%) underwent revision sinus surgery. Non-White patients were at 2.9 times increased odds (95% CI: 1.1-7.5) for requiring revision sinus surgery than age and sex matched White patients. White patients that required revision sinus surgery were from areas of greater deprivation (ADI = 4.5) than White patients that did not require revision sinus surgery (Median difference 2.0; 95% CI: −1.0 to 3.0). This trend also applies to non-White patients as non-White patients that required revision ESS are from areas with higher ADI scores (7.5) than those that did not require revisions surgery (6.0) (1.0, 95% CI: 0.0-3.0). This is presented in Figure 1. Binary logistic regression demonstrated that ADI was associated with revision sinus surgery (OR 1.3, 95% CI: 1.0 to 1.6). Non-White patients had a 3.4 times increased odds of revision sinus surgery (95% CI: 0.9-14.7) when controlling for ADI, polyposis, and baseline SNOT-22.
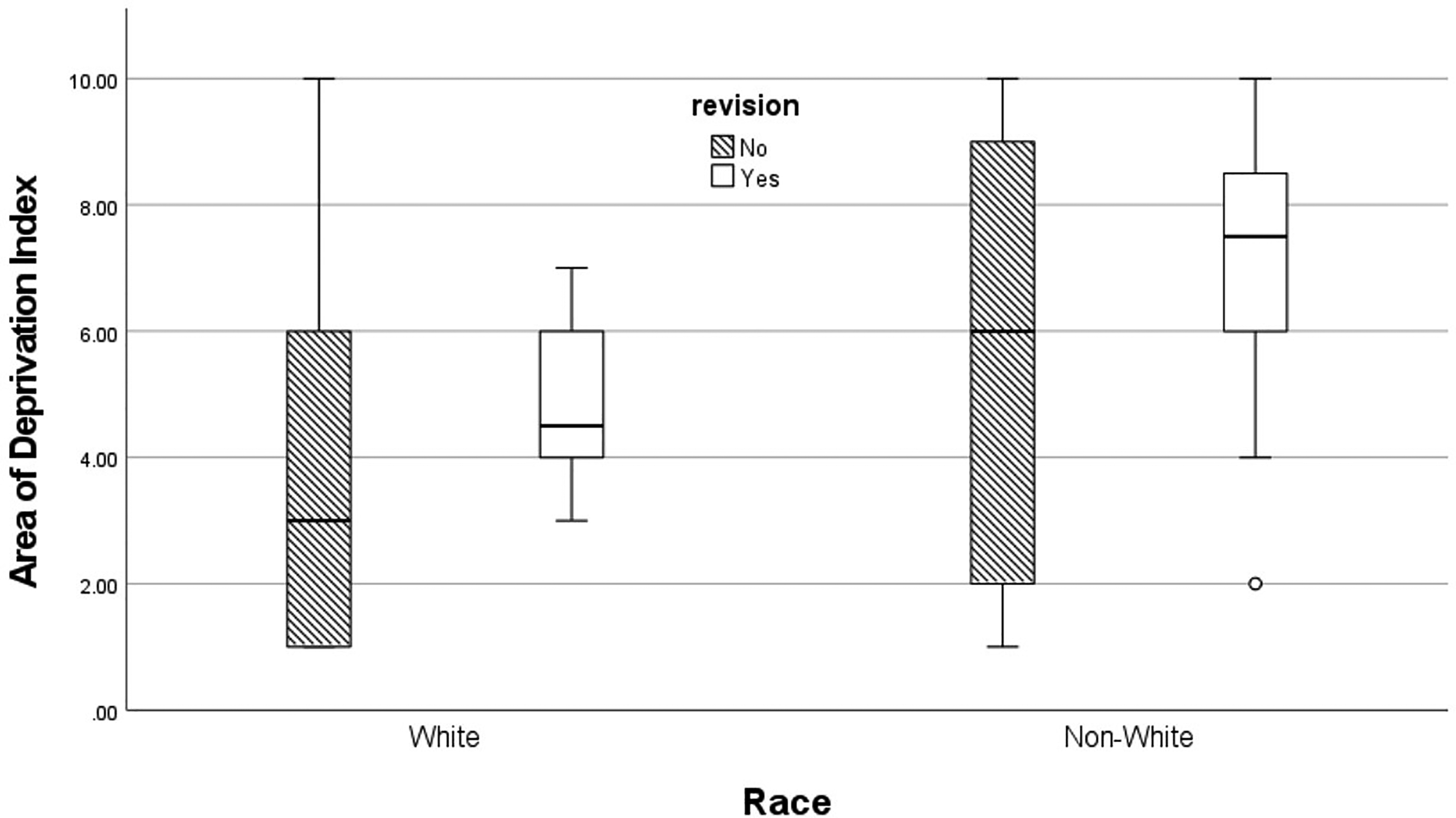
Box plot of area of deprivation index by race for patients that have and have not undergone revision sinus surgery.
In this cohort, patients who received ESS most frequently presented from a neighborhood with an ADI of one (n = 63, 21%). However, patients requiring revision surgery are concentrated in areas of high deprivation as demonstrated in Figure 2. Only 2 patients that required revision sinus surgery (9.0%) were from areas with an ADI of 3 or lower, but 120 patients (41.1%) represented areas from these well-resourced areas. On the other hand, 13 revision sinus surgery patients (59%) lived in areas with an ADI of 7 or greater, areas that only made up 23% of the study population.
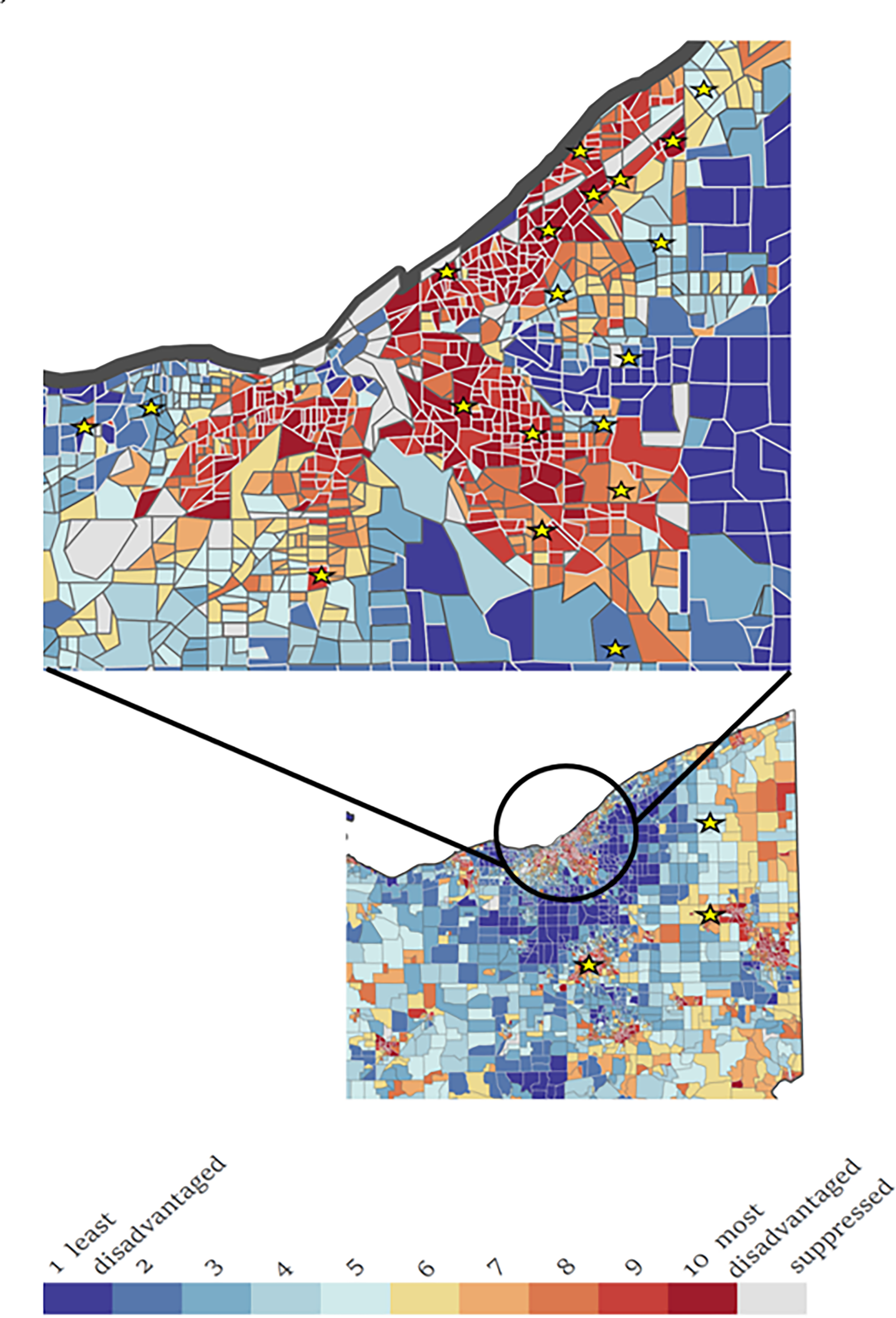
Area of deprivation heat map with patients that required revision sinus surgery indicated.
The median preoperative SNOT-22 scores for all included patients was 43 (2-109) and median postoperative SNOT-22 score was 16 (0-62). Of the 298 patients included in the study, 77 completed both preoperative and postoperative SNOT-22 s with 49 (63.6%) having a clinically significant decline in score. There was not a a clinically meaningful difference in preoperative SNOT-22 scores (47.0 vs 31.0; median difference 7.0; 95% CI −1.0 to 16.0) or postoperative SNOT-22 scores (18.0 vs 14.5; median difference 1.0 95% CI:–5.0 to 8.0) between non-White and White patients. There was also no difference in the SNOT-22 response rates between age and sex matched White (65%) and non-White patients (61%) (PD 3.9%; 95% CI: −18.1% to 25.9%).
Disease Characteristics
Sinonasal comorbidities are summarized in Table 1. Non-White patients had 3.8 increased odds (95% CI: 2.3-6.2) for having CRS w/ nasal polyposis (CRSwNP) than age and sex-matched White patients. There was no significant difference in the rates of allergic rhinitis (OR 1.3; 95% CI: 0.8-2.0), asthma (OR 1.2; 95% CI: 0.7-2.0), samter's triad (OR 1.0; 95% CI: 0.3-3.5), or immune disease (OR 0.8; 95% CI: 0.3-2.4) between White and non-White patients.
There was no difference in mean follow-up time between White patients (11.8 months range 2-56 months) and non-White patients (12.8 range 2-56 months)\, nor was there a difference in time from diagnosis to surgery between White (2.5 months; range 0-56 months) and non-White patients (2.0 months 0-55 months). However, more non-White patients were lost to follow-up (27, 18.1%) than age and sex-matched White patients (13, 8.7%) and White patients were less likely to have lapses in care (79.2% non-White patients had no lapses in care vs 86.6% White patients).
Discussion
The purpose of this study is to characterize the differences in presentation and outcomes of White and non-White patients who received ESS for CRS using ADI as a comprehensive metric for SES. Non-White patients presented from areas of greater deprivation than White patients. This indicates that non-White CRS patients often presented from areas that were socially, economically, and geographically disadvantaged compared to White patients. Race was also associated with disease presentation and treatment outcome. Non-White patients were more likely to have CRSwNP than age and sex-matched White patients. Non-White patients were also significantly more likely to require revision sinus surgery than age and sex matched White patients. Multivariate analysis demonstrated that non-White race and revision sinus surgery were the only variables independently associated with ADI. This provides more insight into the impact that SES can have on the presentation and outcomes of ESS.
An integral and unique finding in this study is the significantly higher ADI in non-White patients than their White counterparts. Higher ADI was also associated with worse outcomes as both White and non-White patients who required revision surgery were from more socioeconomically disadvantaged areas than patients who did not require revision surgery. Although ADI is a widely used metric in other fields such as cardiology, 25 general surgery, 26 and orthopedics, 27 this is the first study to assess the association between ADI and ESS outcomes. Previous studies have typically relied solely on census-track median household income based on zip code which is not specific or nuanced enough to encapsulate all facets of SES. ADI captures a range of factors related to SES such as housing, education, access, to healthcare, and transportation, which are not fully captured by other measures of SES such as median income and insurance status.28,29 Other composite measures of SES exist including the SVI. However, ADI provides the most granular neighborhood-level data. By capturing these different dimensions of SES, ADI provides a more nuanced understanding of how social determinants of health influence health outcomes.
An important strength of this study is the matched cohort design which allows for the direct comparison of age and sex matched White and non-White patients. This comparison uncovered various important differences in presentation and outcomes between patients. Non-White patients presented differently than age and sex-matched White patients both in disease severity with greater rates of non-White patients presenting with CRSwNP. Non-White patients also had significantly higher revision rates than White patients. In addition to potentially more severe disease burden at presentation, this study uncovers potential explanations to this phenomenon. Non-White patients were more likely to be underinsured and present from more deprived neighborhoods. This may have had consequences on postoperative medical care as non-White patients were more likely to be lost to follow-up. Although limited in scope, literature on the impact of race and SES on CRS outcomes is growing. A national database study conducted by Soler et al 12 showed that African American and Hispanic CRS patients were more likely to delay treatment for cost concerns compared to White patients. Furthermore, minority patients were less likely to see a specialist and undergo surgery for CRS. 12 Minority patients often present later in their disease course with more severe disease presentation. 12 Konsur et al also demonstrated that White patients were evaluated by allergists more frequently than Black and Hispanic patients.14 There is evidence that these disparities manifest in pathologic differences with studies demonstrating an increased number of eosinophils in the nasal mucosa of Black patients. 30 This study builds on the existing literature by demonstrating the unique barriers to care of White and non-White ESS patients by using robust measures of socioeconomic factors.
There are several important limitations to this study. Retrospective studies rely on nonsystematic documentation that may introduce differences in information presentation and quality. Short follow-up time also may have artificially lowered the overall revision rate. Long-term database studies have demonstrated that mean time to revision surgery for patients with CRS is 4.5 years and that 10-year revision rates for ESS may be as high as 16%. This study collected data over a 6-year period and thus patients with later initial surgery were less likely to have a recorded revision surgery in this study. It is also possible that patients evaluated in this study obtained revision surgery at another institution. As a result, it is likely that the overall revision rate of 7.4% is lower than the true revision rate of ESS for these patients. Furthermore, patients included in this study were categorized as White and non-White, but this study is best suited to comment on outcomes of White and Black patient outcomes as other races were not well represented in this cohort. Including Hispanic patients in the White cohort may have artificially reduced the disparities found in this study as previous studies have shown outcomes in Hispanic patients are often worse than their non-Hispanic counterparts. However, the low number of Hispanic patients included in this cohort likely minimizes this effect. Another limitation to this study is the relatively limited SNOT-22 data due to inconsistencies with postoperative follow up, postoperative SNOT-22 s were not administered to all patients and were often administered at inconsistent time intervals. Because of this limitation, analysis of symptom outcomes is inconclusive, however, there is an adequate sample of SNOT-22 scores to compare outcomes between the groups.
This study benefits from the unique matched cohort design which allows a direct comparison of the presentation and outcomes of age and sex-matched CRS patients that underwent ESS. Although prospective randomized trials are the only method to assess causality, conducting a prospective study would have limited the sample size. Other retrospective study designs, such as a case-control study, were considered but this would have also significantly limited sample size due to a relatively low number of revisions. This study is also strengthened by using ADI as a robust measure of SES. ADI as a predictor of outcomes has been used in very few studies in rhinology.31,32 The data in the study indicates that race and ADI are important factors that should be considered when tailoring postoperative care for patients undergoing ESS. Further research is needed to uncover the impact of race and ADI on presentation and outcomes of patients with CRS.
Conclusion
Non-White patients undergoing ESS for CRS are more likely to present from areas with fewer resources and are more likely to be underinsured. These socioeconomic factors are associated with poorer outcomes, with increased rates of revision sinus surgery, and less consistent follow-up in non-White patients. Using robust measures of SES, such as ADI, in a clinical setting may allow for postoperative management to be tailored to patients with barriers to care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by the Case Western Reserve/University Hospitals Institutional Review Board (IRB) STUDY20201015. Informed consent was not obtained for this retrospective review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.