
Abstract
Study Design
Retrospective, questionnaire survey.
Objective
The literature lacks a consensus on treatment of isolated orbital fracture. Our aim was to explore treatment schemes and outcomes of patients with isolated orbital fracture treated at a single tertiary care centre.
Methods
We performed a retrospective chart review and a cross-sectional questionnaire survey. We reviewed the medical records of all patients diagnosed with isolated orbital fracture at an outpatient referral clinic in an urban university hospital between 2010 and 2016. We included only patients with isolated inferior, medial, or inferomedial orbital fracture in the study cohort. We sent a questionnaire to these patients to assess the prevalence and severity of long-term symptoms.
Results
We included 246 patients in the study cohort, of which 96 (39%) were treated surgically and 150 (61%) non-surgically. Median time from injury to surgery was 11 days (range = 0–44, IQR = 8,15), and to sending the questionnaire 44 months (range = 16–93). The questionnaire was completed by 89 patients (36%), of whom 51 (57%) reported at least one mild long-term symptom, 24 (27%) at least one moderate long-term symptom, and 17 (19%) at least one severe long-term symptom.
Conclusions
Patients with isolated orbital fracture treated at our unit reported severe long-term symptoms more frequently than would have been expected based on earlier research. Patients at our unit were treated surgically more often than in other similar units, which suggests that surgical treatment may be chosen over non-surgical treatment unnecessarily often at our unit.
Introduction
Isolated orbital fracture, one of the most common midfacial fractures,1,2 is typically caused by a blunt facial trauma. 3 The fracture can be treated surgically or non-surgically by observation.4,5 The treatment aims to prevent long-term diplopia and evident malposition of the eye.4,5 When surgical treatment is deemed beneficial to the patient, surgery is traditionally recommended within 2 weeks of the injury, if there are no indications for urgent surgery. 4 However, lack of conclusive evidence persists on whether this time frame yields a superior outcome.6-8
The treatment of isolated orbital fracture lacks consensus; the recently proposed treatment guidelines are contradictory.5,9-14 The most debated topics are the selection between surgical and non-surgical treatment and the timing for surgical intervention.11,12,15 Disagreement over treatment is reflected in the divergence of treatment schemes between different units.12,16,17 Information on local treatment schemes and outcomes could enhance the quality and uniformity of treatment.
Our aim was to investigate the treatment schemes and outcomes of patients with isolated orbital fracture treated at the Department of Otorhinolaryngology – Head and Neck Surgery, Helsinki University Hospital (HUH), Finland. To explore treatment schemes, we retrospectively reviewed patients’ medical records. We assessed the outcomes of treatment by sending patients a questionnaire regarding long-term symptoms.
Materials and methods
Study Design and Patient Selection
We performed a retrospective chart review and a cross-sectional questionnaire survey. We reviewed the medical records of all patients diagnosed with isolated orbital fracture at the Department of Otorhinolaryngology – Head and Neck Surgery (HUH, Finland), later referred to as our unit, between 1 January 2010 and 31 December 2016. We identified the patients from the HUH patient database by a search for International Classification of Diseases 10th Revision (ICD-10) code S02.30 (fracture of the orbital floor, unspecified side). We sent a questionnaire to the patients to assess the prevalence and severity of long-term symptoms. We sent a reminder letter to non-respondents 4 weeks later.
Our unit provides public secondary and tertiary ear, nose, and throat services to an urban referral area of 1.6 million inhabitants. Patients with isolated orbital fracture from the referral area are treated both at our unit and at the Department of Oral and Maxillofacial Surgery (HUH, Finland).
Inclusion Criteria
The inclusion criteria were as follows: (1) isolated inferior, medial, or inferomedial orbital fracture diagnosed by computed tomography (CT); (2) first visit at our unit in 2010-2016; (3) patient age 16 years or older at the time of injury; (4) no concomitant or previous facial or skull fractures other than nasal bone fracture; (5) CT available with a slice thickness of ≤2.00 mm in the picture archiving and communication system (PACS); (6) injury took place in Finland; and (7) treatment of the fracture was performed at our unit. The presence and location of isolated orbital fracture were confirmed by reviewing the radiological reports and the CT scans. The surgeries were performed by experienced specialists or specialising physicians, who were always under direct supervision of an experienced specialist.
Study Variables
Reviewed were the following data: gender, age, type of treatment, time intervals in the care pathway, location of the fracture, injury aetiology, surgical approach, reconstruction material, postoperative hospitalization at our unit, and whether revision surgery was performed. The time intervals in the care pathway were measured from the day of injury to the first meeting with a physician, to the diagnostic CT, to the first visit at our unit, to the surgery, and to the last follow-up visit.
The presence of long-term symptoms was evaluated subjectively by the patients through a questionnaire. The questionnaire assessed the following symptoms: diplopia at peripheral gaze, posterior displacement of the eye, anterior displacement of the eye, numbness on the cheek area, difficulty focussing the gaze, pain when moving the eyes, eyes are at different levels, visible lesion on the skin, eyes open asymmetrically, and other symptoms. For every existing long-term symptom, patients were asked to grade the severity of the symptom as mild, moderate, or severe. Mild symptoms were defined as not causing disturbance in everyday life, moderate symptoms as causing disturbance in everyday life, and severe symptoms as limiting everyday life.
Statistical Methods
Statistical data analysis was performed with SPSS (Statistical Package for Social Sciences, version 27, 2020; IBM, Armonk, NY, USA). A Chi-square test of independence was conducted between location of the fracture and treatment modality. Post hoc analysis was conducted by converting standardized adjusted residuals into Bonferroni-adjusted P-values.
Ethical Considerations
The study protocol was approved by Helsinki University Ethics Review Board, and written informed consent was obtained from all patients who responded to the questionnaire survey.
Results
Patient Inclusion
The database search revealed 589 patients assigned ICD-10 code S02.30. After reviewing the medical records, we included 246 patients in the study cohort. The flowchart of patient selection is presented in Figure 1. Selection of patients to the study cohort.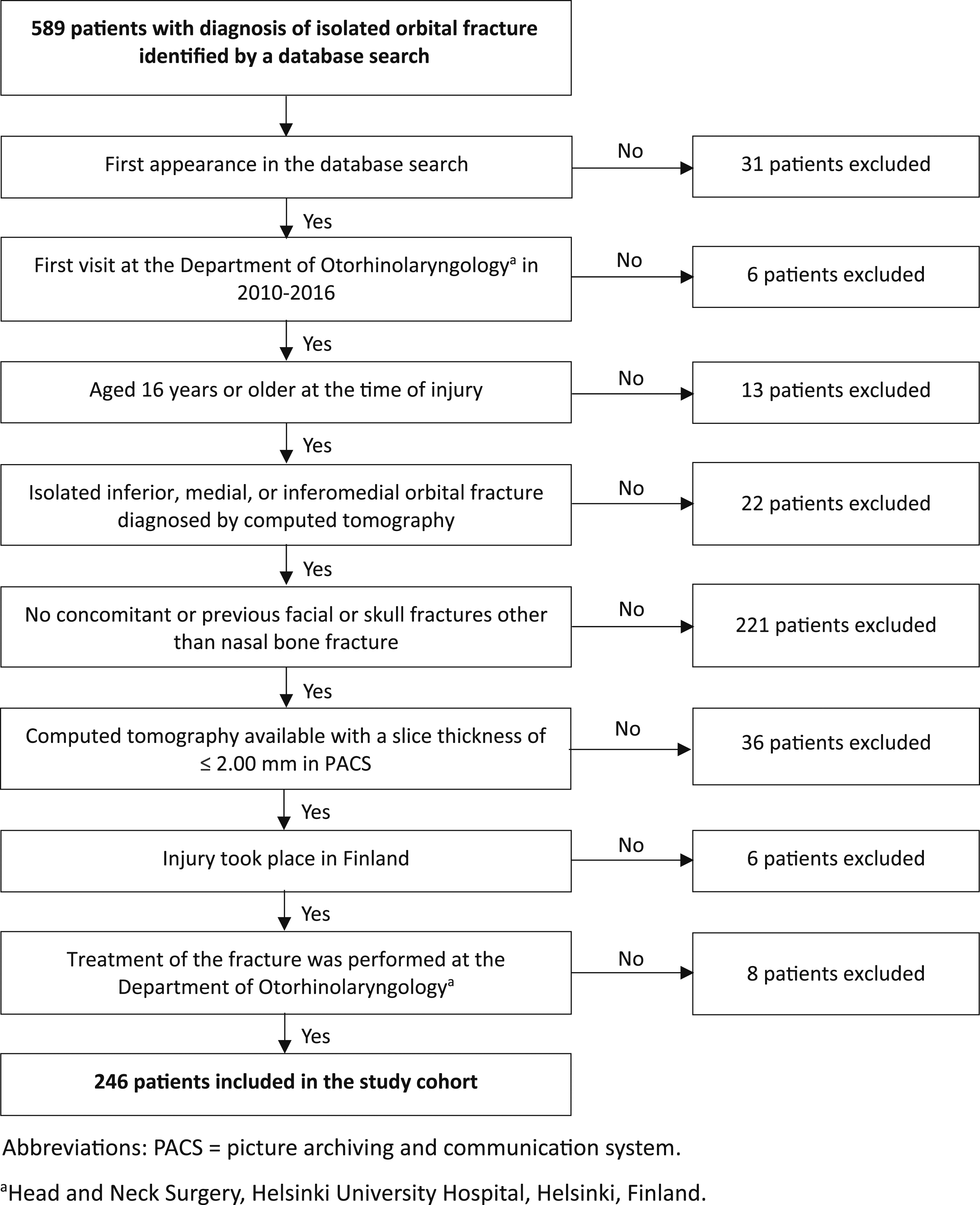
Demographics and Injury Aetiology
The patients in the study cohort ranged in age from 16 to 97 years (median 40 years). There were 175 men (71.1%) and 71 women (28.9%). Injury was caused by violence in 116 (47.2%), falling or slipping in 68 (27.6%), sports in 44 (17.9%), and other injury aetiology in 18 (7.3%) patients.
Treatment Modality, Surgical Approach, and Reconstruction Material
Of the patients, 96 (39%) were treated surgically and 150 (61%) non-surgically. Of the surgically treated patients, surgery took place within 2 weeks in 67 patients (70%) and within 4 weeks in 89 patients (94%). Surgical approach was transconjunctival in 91 patients (95%) and subciliar in 5 patients (5%). Reconstruction material was titanium mesh in 88 patients (92%), resorbable implant in 2 patients (2%), and no reconstruction material was used in 6 patients (6%). Postoperative CT was performed on 83 patients (87%). Revision surgery was performed on 5 patients (5%).
Location of Fracture
Contingency table of location of the fracture and type of treatment in patients with isolated orbital fracture.
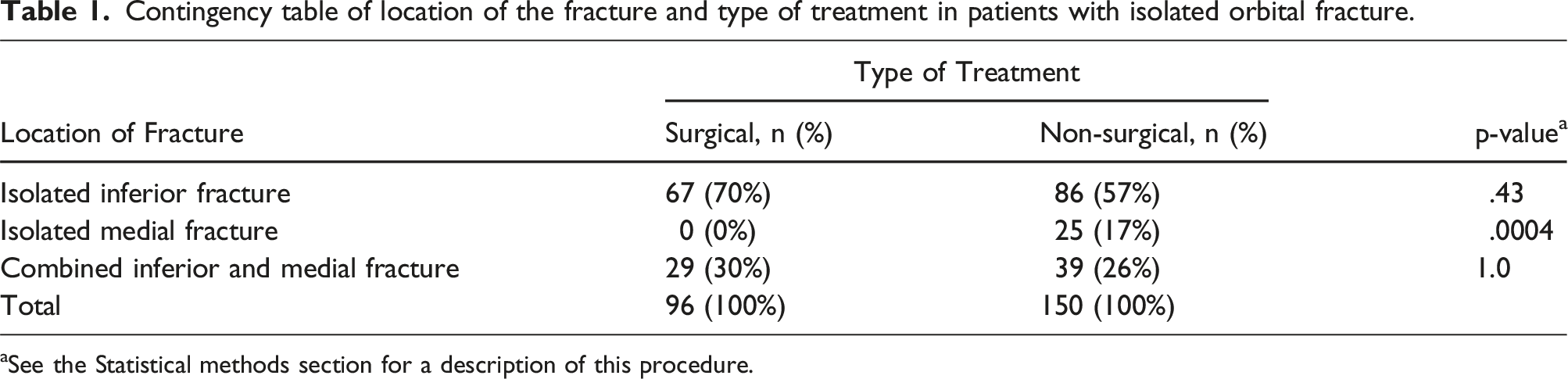
aSee the Statistical methods section for a description of this procedure.
Time Intervals in the Care Pathway
Median time from injury to the first meeting with a physician was zero days (mean 1, range 0–30, IQR = 0,1), to diagnostic CT 1 day (mean 2, range 0–53, IQR = 0,2), and to the first visit at our unit 2 days (mean 4.1, range 0–48, IQR = 1,5). Median time from injury to surgical treatment was 11 days (mean 12.3, range 0–44, IQR = 8,15). Median postoperative hospitalization at our unit was .5 day (mean .6, range 0–4, IQR = 0,1). Median time from injury to the last follow-up visit in surgically treated patients was 30 days (mean 42, range 7–190, IQR = 23,47) and in non-surgically treated patients 6 days (mean 7.4, range 0–62, IQR = 2,9). Time intervals in the early care pathway are presented in Figure 2. Interquartile ranges of time intervals in the early care pathway in patients with isolated orbital fracture.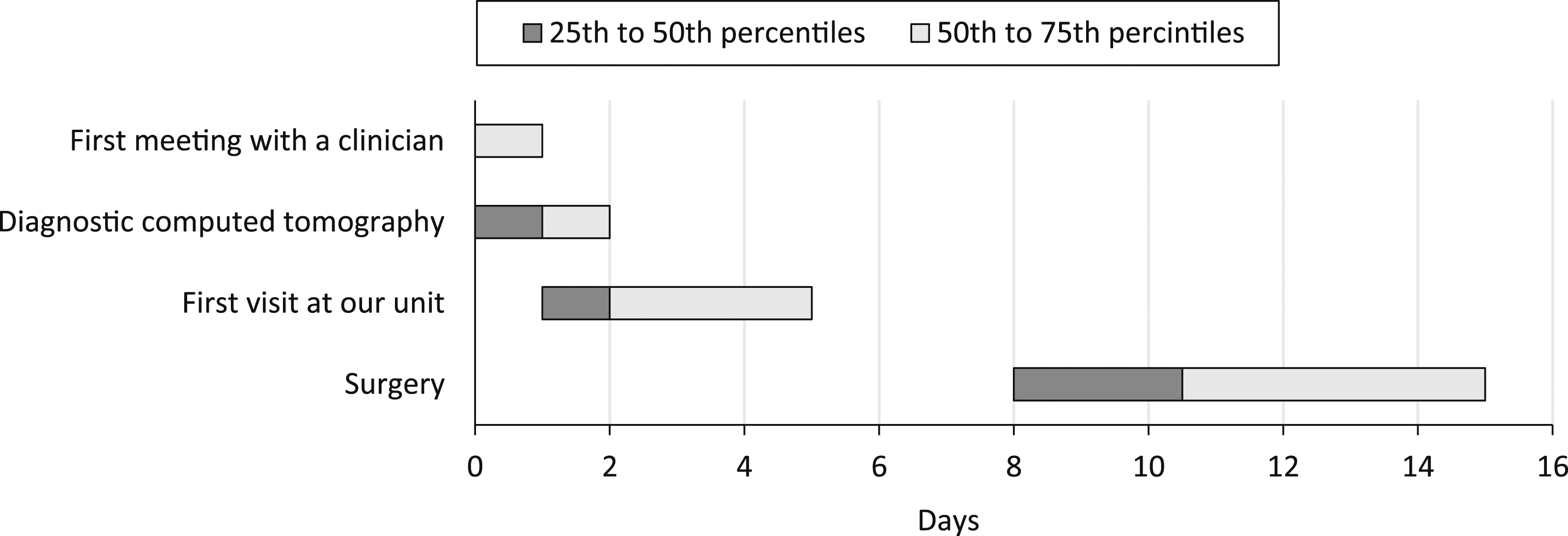
Questionnaire and Long-Term Symptoms
The questionnaire was completed by 89 patients (36%). The patients ranged in age from 17 to 91 years (median 47), and 53 (60%) were men and 36 (40%) women. Of the respondents, 43 (48%) were treated surgically and 46 (52%) non-surgically. Median time interval from injury to sending the first survey letter in surgically treated patients was 44 months (mean 52, range 16–93, IQR = 28,75) and in non-surgically treated patients 46 months (mean 50, range 13–94, IQR = 25,71).
At least 1 self-reported long-term symptom was present in 38 surgically treated patients (88%) and in 35 non-surgically treated patients (76%). The predominantly reported long-term symptom was diplopia at peripheral gaze, reported by 19 of the surgically treated patients (44%) and by 11 of the non-surgically treated patients (24%). Figure 3 shows the prevalence of different self-reported long-term symptoms in surgically and non-surgically treated patients. Self-reported long-term symptoms in surgically (n=43) and non-surgically (n=46) treated patients with isolated orbital fracture.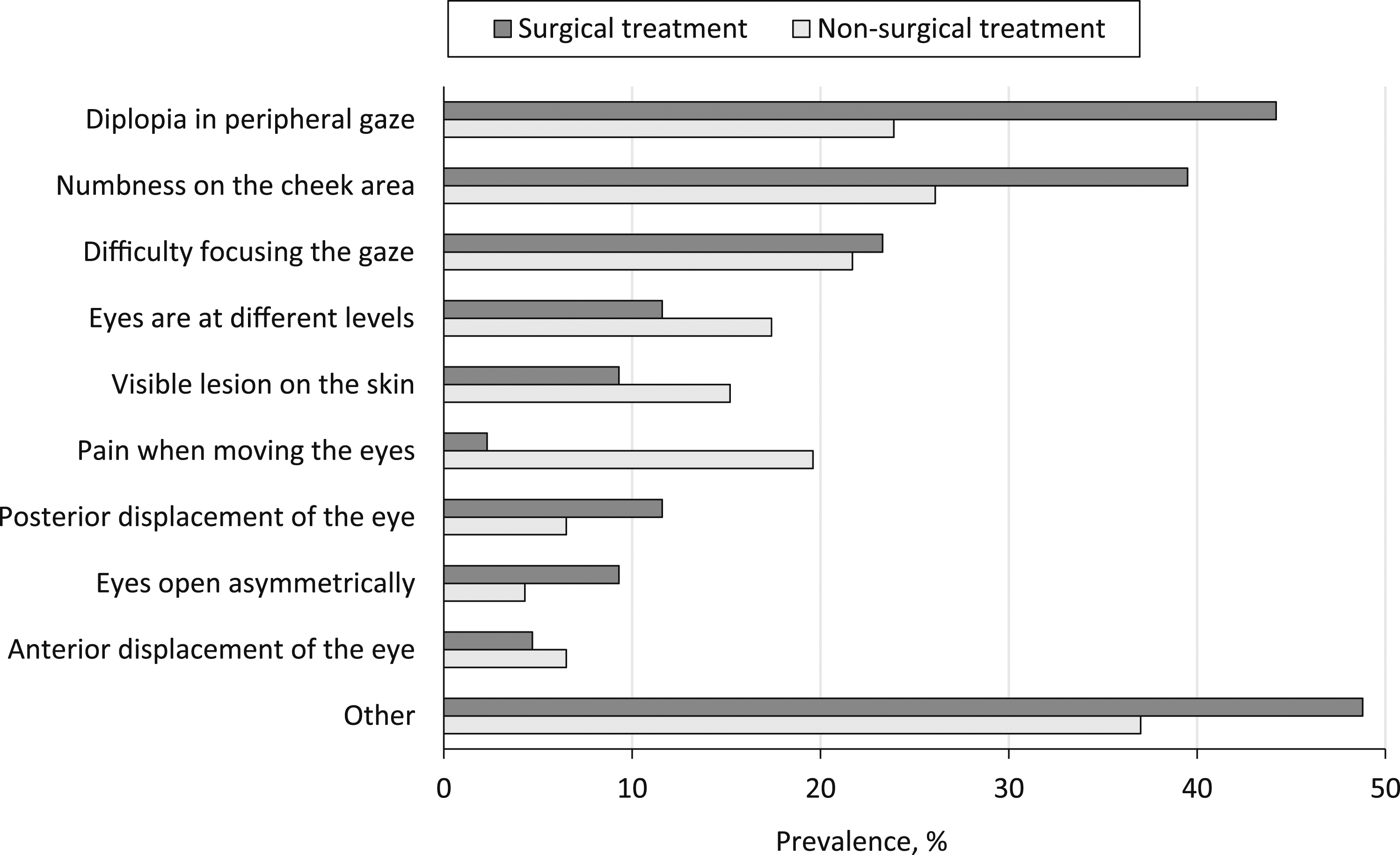
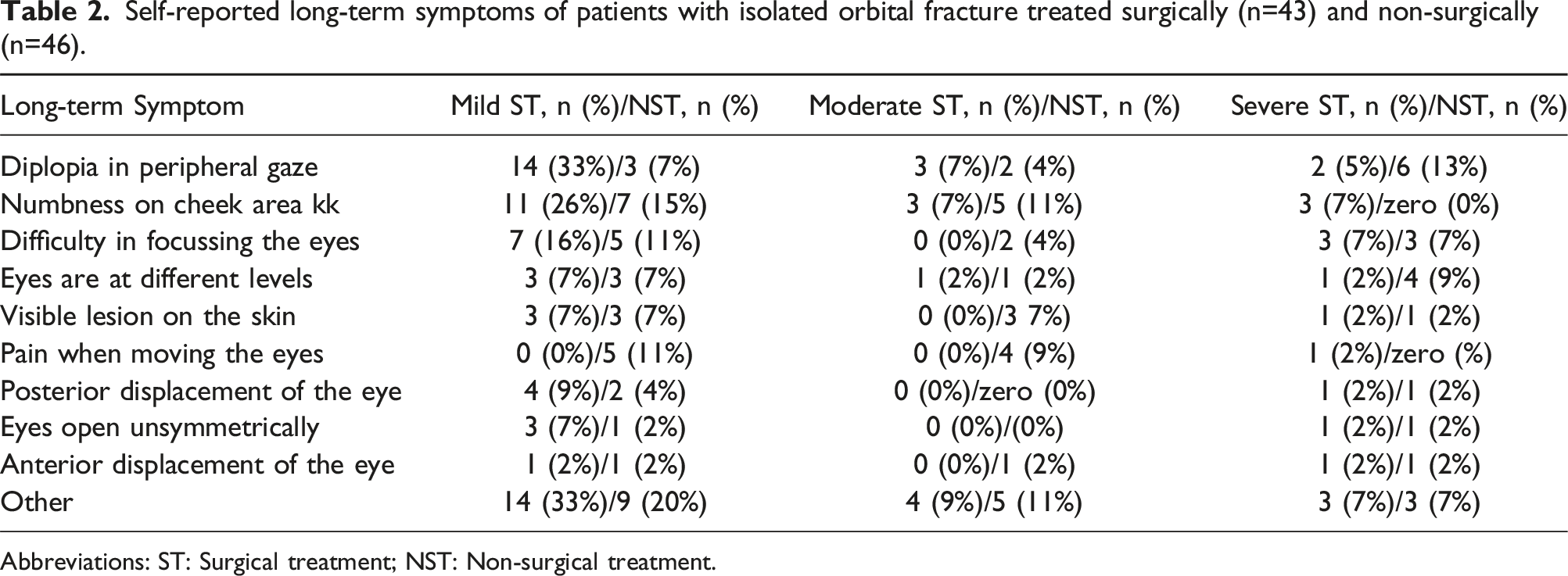
Of all respondents, 16 (18%) reported no symptoms, 51 (57%) reported at least one mild symptom, 24 (27%) reported at least one moderate symptom, and 17 (19%) reported at least 1 severe symptom. Figure 4 shows the prevalence of self-reported long-term symptoms of different severities in surgically and non-surgically treated patients. Table 2 presents the prevalence of different self-reported long-term symptoms of different severities in surgically and non-surgically treated patients. Severity of self-reported long-term symptoms in surgically (n=43) and non-surgically (n=46) treated patients with isolated orbital fracture. Self-reported long-term symptoms of patients with isolated orbital fracture treated surgically (n=43) and non-surgically (n=46). Abbreviations: ST: Surgical treatment; NST: Non-surgical treatment.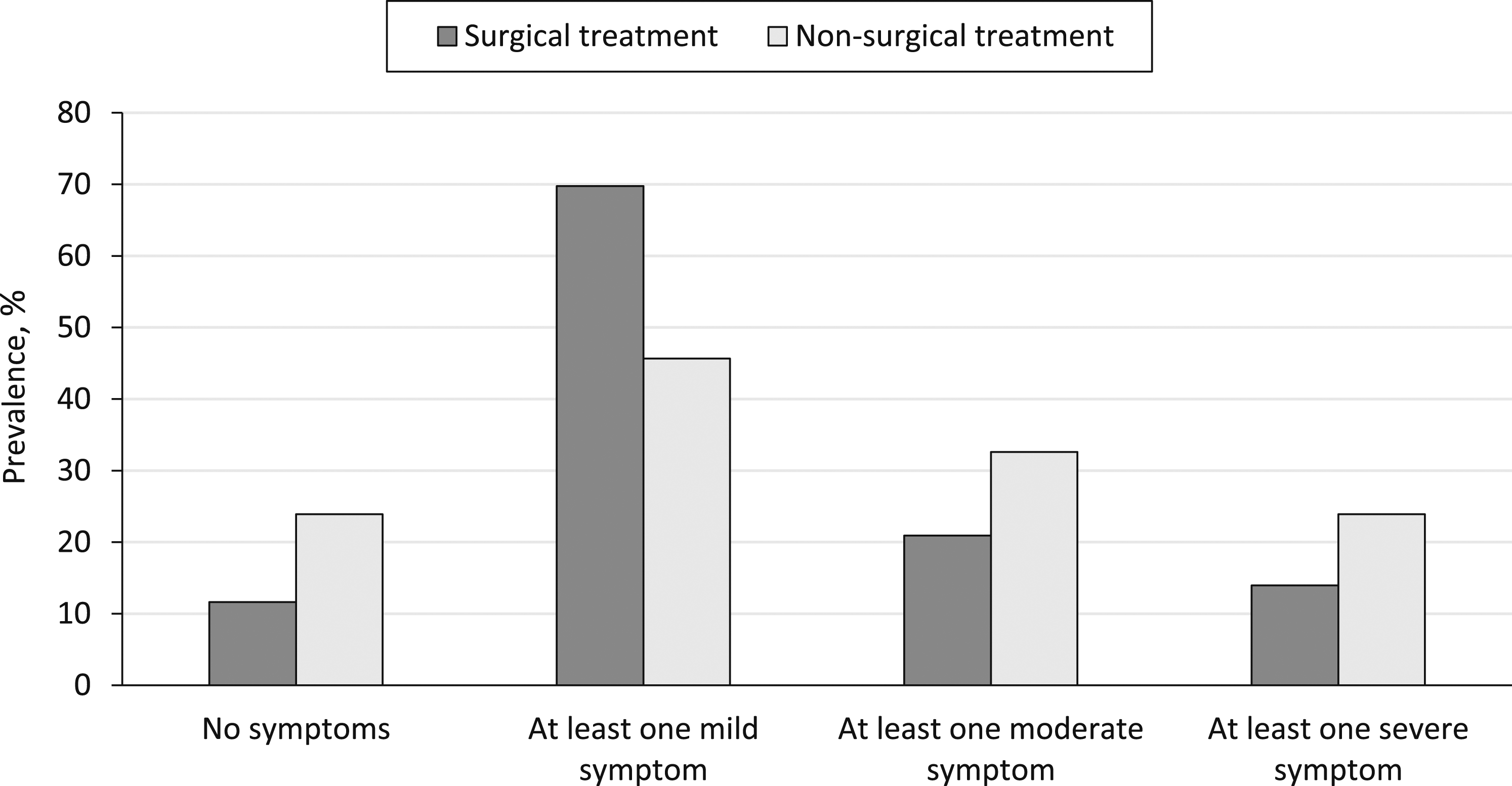
Discussion
Long-term symptoms were reported by 88% of surgically treated patients and by 76% of non-surgically treated patients with isolated orbital fracture treated at our unit. In previous studies, the prevalence of long-term symptoms in patients with isolated orbital fracture has ranged widely, and it is usually measured per individual symptom.18-21 Discrepancy in the data is partly due to the varying definitions of long-term symptoms.18-21 In a study by Rajantie et al, 20 23% of the surgically treated patients with isolated orbital fracture reported no complications 6 months after injury. In a study by Jansen et al, 18 no complications were found in 17% of surgically treated patients and in 70% of non-surgically treated patients with isolated orbital fracture at a 12-month follow-up. Long-term symptoms seem to be, thus, a common complaint after an isolated orbital fracture in both surgically and non-surgically treated patients.
In our study, 57% of the respondents reported at least one mild long-term symptom, 27% at least one moderate symptom, and 19% at least one severe symptom. Only a few reports have focused on the severity of the long-term symptoms from the patient’s perspective. In the study by Rajantie et al, 20 patients’ quality of life appeared to decrease only temporarily after isolated orbital fracture. A similar result was obtained by Lubamba et al, 22 who found that quality of life was minimally affected in surgically treated patients with orbital fracture. Likewise, Hartwig et al 23 reported that patients with surgically treated orbital fracture were mostly satisfied with the outcome. The high prevalence of severe long-term symptoms in our study is, thus, contradictory to the results of earlier research.
We found that diplopia at peripheral gaze was the predominantly reported long-term symptom, reported by 44% of the surgically treated patients and by 24% of the non-surgically treated patients. Jensen et al 18 found diplopia in 67% of surgically treated patients and in 11% of non-surgically treated patients after a follow up of at least 3 months. Kasaee et al 24 found diplopia in 7% of surgically treated patients and in 1% of non-surgically treated patients 6 months after the injury. Our study supports the view that diplopia is a common long-term symptom in both surgically and non-surgically treated patients with isolated orbital fracture. Also, our study corresponds with the results of earlier research that has found long-term diplopia to be more common in surgically treated patients than in non-surgically treated patients.
Diplopia after isolated orbital fracture can have mechanical, paralytic, and sensory aetiology. Diplopia caused by macroscopic entrapment of the orbital tissues is the only type of diplopia that surgical treatment can alleviate. 25 Nonetheless, diplopia is often considered an indication for surgical treatment even without evidence of restriction caused by entrapment of the orbital soft tissues.4,5 The high prevalence of long-term diplopia in surgically treated patients in our study is consistent with the presumption that surgical treatment has a limited ability to prevent long-term diplopia in patients with isolated orbital fracture.
Generalization of the results of the questionnaire survey is susceptible to bias. First, the response rate to the questionnaire survey was only 36%. Patients with long-term symptoms may have been more likely to complete the questionnaire, creating a selection bias favouring higher prevalence of long-term symptoms. Second, the presence and severity of long-term symptoms were evaluated subjectively, which may yield different results than objective measurements. 23 For example, Hartwig et al 23 found that patients with orbital fracture reported diplopia less frequently than was found in orthoptic evaluation.
At our unit, 39% of patients with isolated orbital fracture were treated surgically. In other recent studies with urban populations, the proportion of surgically treated patients has been lower.9,12,17,18 For example, Pöytsiä et al 17 noted that 28% of patients with isolated orbital fracture were treated surgically. Also, Jansen et al 18 reported that 21% of patients with isolated orbital fracture were treated surgically. Neither of these studies reported secondary surgical treatment in non-surgically treated patients. In both studies, the outcome was acceptable in every non-surgically treated patient. It seems unlikely that the higher proportion of surgically treated patients at our unit would be caused by more severe injuries because demographics and injury aetiologies of the patients were similar between the studies. Thus, surgical treatment may be chosen over non-surgical treatment more frequently than necessary at our unit.
In our study, we included patients who underwent either immediate or non-immediate surgical treatment for isolated orbital fracture. The clear majority of isolated orbital fractures do not require immediate surgery.26,27 Thus, the time intervals in the care pathway in our study mostly reflect the time intervals of the patients who underwent non-immediate treatment of isolated orbital fractures.
Of the surgically treated patients, 70% were operated within 2 weeks of injury and 94% within 4 weeks of injury. The mean time interval from injury to the surgery was 12 days. In surveys, most surgeons prefer to perform the surgery within 2 weeks post-injury.28,29 In recent retrospective studies, the mean time interval from injury to the surgery has ranged from 4 to 8 days.17,30,31 Thus, it seems that surgeries at our unit are usually performed within the widely preferred timeframe of 2 weeks. However, it also seems that surgeries are performed later at our unit than in other units. The effect of the comparatively late timing of surgery on the outcome cannot be determined, because there is a lack of high-quality studies on the effect of surgical timing on outcome. 7
We found that 98% of patients were diagnosed within 7 days of injury and that 97% of the patients had arrived at our unit within 14 days after injury. Therefore, it seems that patient delay or diagnostic delay rarely prevent evaluation and surgery within 2 weeks of the injury at our unit. Thus, there must be other reasons for the late timing of the surgery at our unit. These reasons could include local practices or lack of resources, such as limited availability of operating rooms or personnel.
All 25 patients with isolated medial orbital fractures were treated non-surgically at our unit. In the literature, indications are debated for the surgical treatment of isolated medial orbital fracture; recommendations range from advocating surgery only for patients with certain symptoms to advocating surgery for every patient with the fracture.32,33 In some studies, the decision on the treatment modality is suggested to be guided by radiological findings.34,35 In a retrospective study by Snell et al, 36 the proportion of surgically treated patients with isolated medial orbital fracture was 38%, which is higher than in our study.
Conclusion
Patients with isolated orbital fracture treated at our unit reported severe long-term symptoms more frequently than would have been expected based on earlier research. Diplopia in peripheral gaze was the most frequently reported long-term symptom, and it was more common in surgically treated patients than in non-surgically treated patients. Patients at our unit were treated surgically more often than in other similar units, which suggests that surgical treatment may be chosen over non-surgical treatment unnecessarily often at our unit.
Footnotes
Acknowledgements
We thank Tommy Wilkman, MD, PhD, for providing the Swedish translation of the questionnaire. There was no financial compensation for this contribution.
Author Contributions
Maunula had full access to all data of the study and assumes responsibility for the integrity of the data and the accuracy of data analysis. Concept and design: Maunula, Blomgren, Sinkkonen, Tapiovaara. Acquisition, analysis, or interpretation of data: Maunula. Draughting of the manuscript: Blomgren, Maunula, Sinkkonen, Tapiovaara. Critical revision of the manuscript for important intellectual content: Blomgren, Sinkkonen, Tapiovaara. Statistical analysis: Maunula. Administrative, technical, or material support: Tapiovaara, Nyman. Supervision: Blomgren, Sinkkonen, Tapiovaara.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.