
Abstract
Study Design
Systematic review and meta-analysis.
Objective
The clinical decision to pursue harmonic scalpel (HS) method vs conventional hemostasis to treat head and neck cancers has been arguably predicated on the clinical outcomes observed. This study aims to evaluate the surgical outcomes of neck dissection between both techniques and perform an updated meta-analysis using the available literature.
Methods
We searched PubMed, Scopus, and Cochrane Library through 31st December 2021, according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Outcome metrics included operative time and intraoperative blood loss. Secondary outcomes consisted of length of hospital stay, length of drain stay, total drain output, and postoperative complications. A meta-analysis was conducted using Review Manager Version 5.3 (RevMan) software employing the Random Effects Model.
Results
We identified 114 articles, out of which 10 randomized control trials (RCTs) analyzing a combined total of 558 patients met the inclusion criteria after title and full-text screening. Meta-analysis shows the group treated with HS had a significantly shorter operative time. [MD = −23.21, 95% CI (−34.30, −12.12) P value <.0001 I2 = 92%] but an insignificant lesser intraoperative blood loss [MD = −61.53, 95% CI (−88.61, −34.45) P < .00001 I2 = 79%].
Conclusions
This study confirms that that HS use in neck dissection yields a reduced operative time and intra operative blood loss relative to conventional hemostasis. Furthermore, our paper shows no superiority of HS method over conventional hemostasis where length of hospital stays, length of drain stays, and postoperative complications are concerned. Future RCTs with high-level evidence may further elucidate the relative effectiveness of HS method over conventional hemostasis in treating head and neck cancers.
Introduction
Most head and neck cancers (HNC) originating from the oral cavity, nasopharynx, oropharynx, larynx, and hypopharynx, are predominantly squamous cells (HNSCC) in nature. 1 According to GLOBOCAN 2020, the worldwide incidence of head and neck cancers originating from the lip and oral cavity, larynx, nasopharynx, oropharynx, and hypopharynx is 2.0%, 1.0%, .7%, .5%, and .4%, respectively.2,3
By 2030, this escalating occurrence is anticipated to increase by 30% (i.e.,, 1.08 million new cases annually). 4 Neck dissection (ND) plays a crucial role in the treatment of HNC and is classically performed with one of the 3 objectives: therapeutic, opportune, or elective. 5 In principle, the indication of neck dissection in HNC is a problem of risk-benefit evaluation between the probability of neck metastases of complications associated with neck dissection and the possible prognostic influence of late diagnosis of metastasis during follow-up. 5 The continuous enhancement of surgical approaches and the introduction of novel surgical devices have remained vital to head and neck surgeons over the years, so as to minimize risk and maximize efficacy.
The conventional hemostasis techniques in use for ENT surgeries, such as tying and knots, resorbable ligature, and bipolar diathermy were augmented by the introduction of the novel Harmonic Scalpel® (HS) in the 1990s, influenced by the latter’s favorable use in other surgical fields. 5 The mechanism of the HS is based on transforming electrical energy into mechanical movement of 55.5 kHz frequency. Vibrating 55,500 times per second, the HS blade denatures protein in the tissue to form a sticky coagulum. The pressure exerted on the tissue by the blade surface collapses blood vessels and allows the coagulum to form a hemostatic seal. 6 HS has been found to be especially useful in thyroid surgery, parotid surgery, and tonsillectomies because it serves 4 broad functions during surgery, namely: cutting of the tissues, approximation of the tissues, cavitation, and coagulation. 7 With regard to ND, the popularity of HS is gradually increasing, as research and trials continue to report benefits within intra-, peri-, and postoperative parameters. In addition to a significant reduction in operative time and intraoperative bleeding, 8 intra-procedure benefits such as its precision in ligating arteries as small as 2–5 mm, reduced thermal effects on surrounding tissues, faster re-epithelization, and greater tensile strength than that by laser or electrosurgical instruments, have all contributed to the increasing usage of HS in neck dissection. 6 To add, clear margins and a bloodless field allow for thorough histological examination of the entire specimen and radical extirpation of the whole lesion with a low recurrence rate and better prognosis. 6
Various studies examine the benefits of HS in a broad spectrum of head and neck surgeries. 8 However, the evaluation of its use in ND’s is limited and the existing trials tend to have each examined limited aspects. Our study primarily aimed to review the literature and update the existing meta-analysis (2015) of the randomized control trials (RCT’s) that compare the surgical techniques of HS and traditional methods in ND. 8 With an aim to expand the array of variables analyzed and highlight areas that would compound literature by further research, this meta-analysis factored in the length of drain stay and postoperative complications, in addition to intraoperative blood loss, operation time, hospital stay, and drainage volume as outcomes of both surgical techniques.
Methods
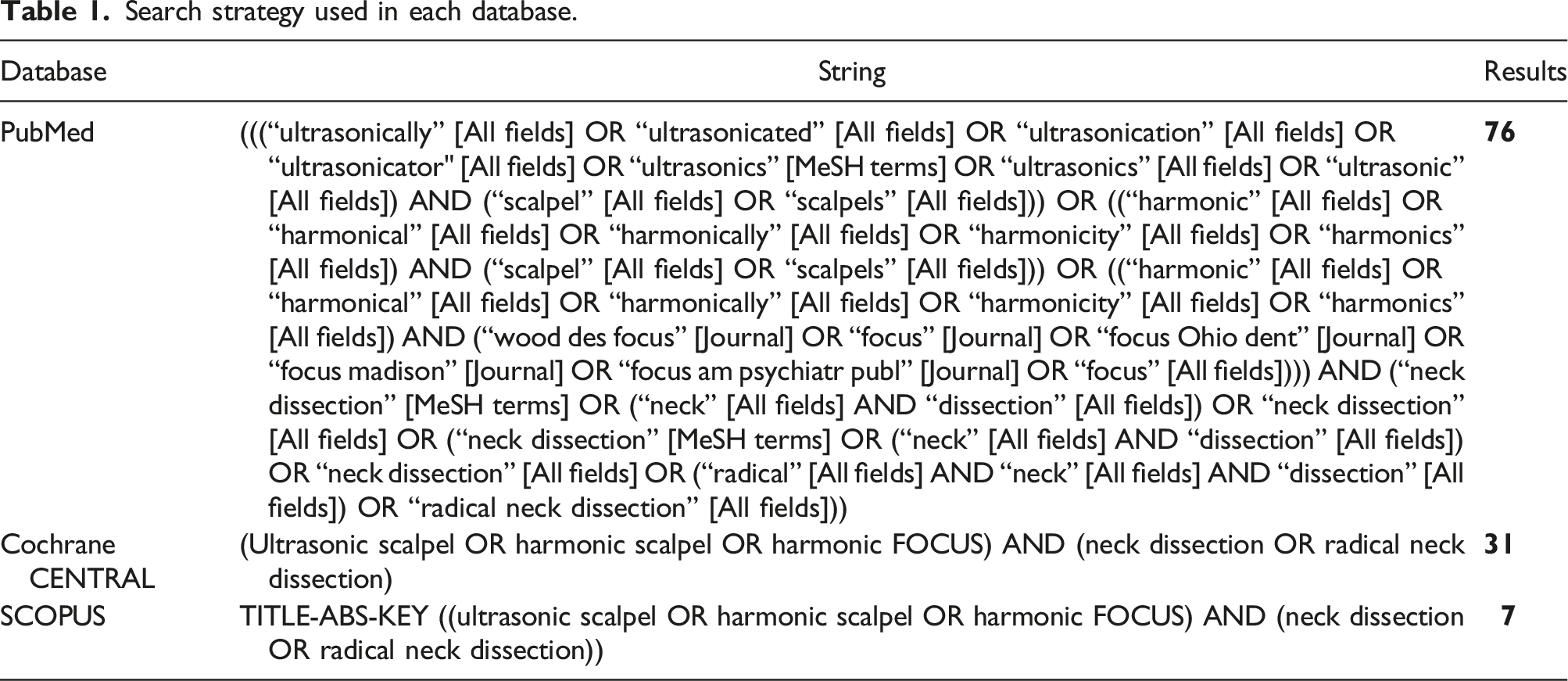
Search Strategy
Search strategy used in each database.
Study Selection
We exported the articles retrieved through the initial systematic search to EndNote (Clarivate Analytics, Thomson Reuters Corporation, Philadelphia, Pennsylvania) Reference Library software and deleted the duplicates. The remaining publications were initially screened based on the title and abstract, and then the reviewers read the complete text to determine relevance. Two reviewers (I. H. and S. A. S.) worked independently to screen the articles for inclusion. In the event of a disagreement, a third reviewer (O.M.S) was consulted.
Inclusion Criteria
We included the studies that reported patients with any histological type of head and neck cancer undergoing neck dissection without any prior therapy. The study must compare the outcomes of the HS and conventional hemostasis in neck dissection. Outcome metrics must include operative time or intraoperative blood loss. Randomized controlled trials (R.C.T.s) with no restrictions on publication status were included.
Exclusion Criterion
We excluded the studies if they were non-randomized. We also excluded the case reports, letters to the author, comments, non-human studies, and reviews. Studies published in a language other than English were not considered.
Outcomes of Interest
The primary outcomes of interest were operative time and intraoperative blood loss. Other outcomes of interest were: (a) Length of hospital stay; (b) Length of drain stay; (c) Total drain output; and (d) Postoperative complications.
Data Extraction and Quality Assessment
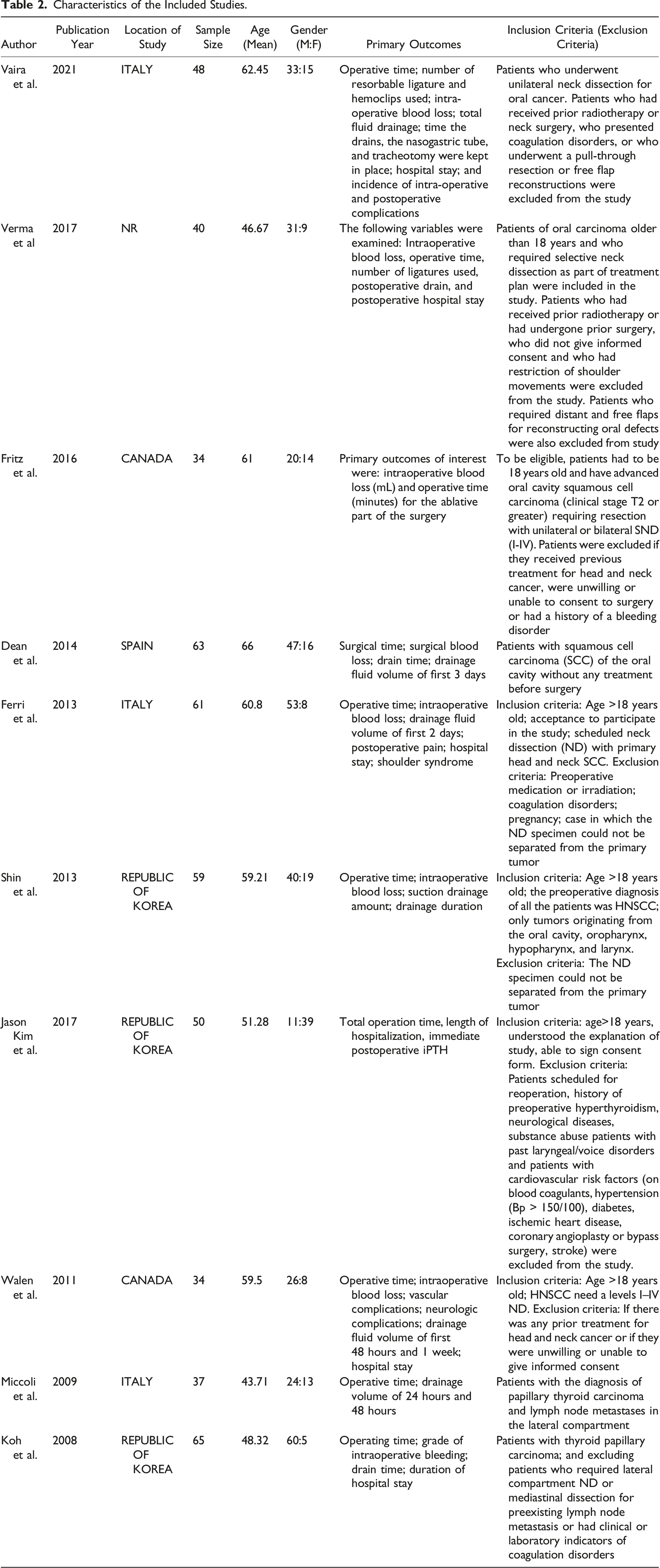
The reviewers entered the study’s characteristics including author, publication year, location of study, sample size, baseline demographics (age and gender of the sample population), and primary outcomes data into a predesigned Excel spreadsheet. Two independent reviewers (I.H. and S.A.S.) used the Cochrane Risk of Bias Tool to assess the quality of the included RCT’s. The criteria include random sequence creation, blinding of participants and staff, blinding outcome evaluation, insufficient outcome data, selective outcome reporting, allocation concealment, and other biases.
An assessment of the risk of bias was categorized as “Low risk of bias,” “Unclear risk of bias,” or “High risk of bias in each area” in accordance with the guidelines from the Cochrane Handbook, with notes outlining the specific reasons for each categorization in the risk of bias table. The reviewers settled any disagreements by dialogue.
Statistical Analysis
We used the Review Manager (Version 5.3, Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, 2014) for all statistical analyses. We calculated the mean differences (MD) for the surgical time, intraoperative bleeding, amount drainage, and hospital stay. A random-effect model was used to collect and analyze the results. The Higgins I2 statistic was used to evaluate statistical heterogeneity, defined as the variation in outcomes between the trials. A value of 25%–50% was considered mild, 50%–75% as moderate, and >75% as severe heterogeneity. We carried out the subgroup based on squamous cell carcinoma (SCC) and non-SCC . Evidence of publication bias was tested with Egger and Begg’s methods and visually assessed using funnel plots. Visual inspection of the funnel plot was used to determine the publication bias. In all cases, a P-value of less than .05 was considered significant.
Results
Literature Search Results
Figure 1 highlights the PRISMA flow chart and gives a summary of the literature search. The initial search revealed a pool of 114 articles that went through the screening process. After excluding studies based on not meeting the inclusion criteria, not having relevant data, and not being in the English language, a total of 10 studies were gathered to be included in the final meta-analysis. All the 10 studies were RCTs consisting of a combined pool of 558 patients undergoing neck dissection. PRISMA 2009 flow diagram.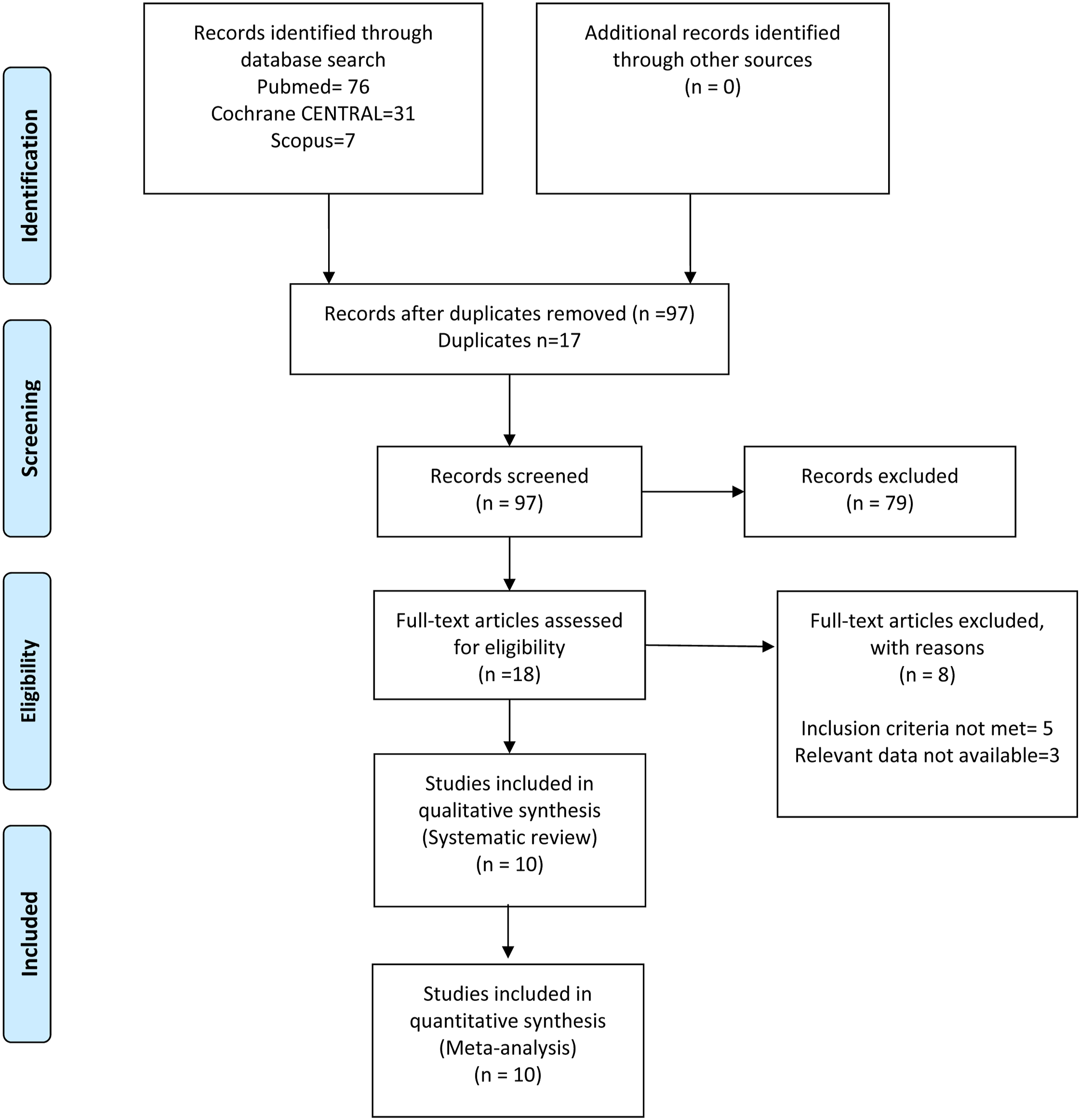
Study Characteristics and Quality Assessment
Characteristics of the Included Studies.
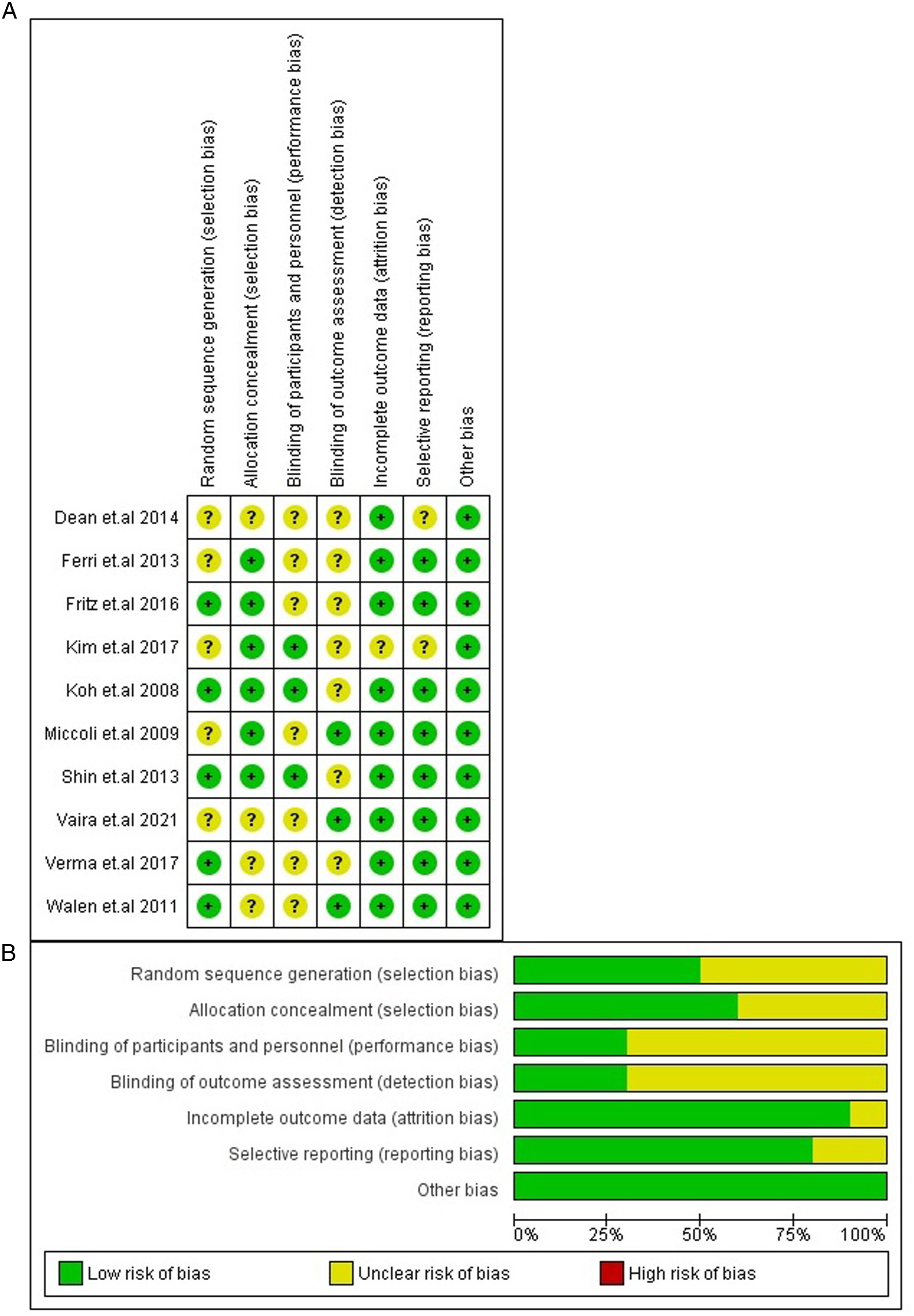
Risk of bias assessment.
Primary Outcomes
Operating Time
All 10 studies (Koh,
12
Miccoli,
13
Shin et al.,
14
Ferri,
15
Walen,
16
Verma,
7
Vaira,
9
Kim,
10
Fritz
11
and Dean
17
) successfully reported the operative times. The operative time for HS was significantly lower as compared to conventional dissection [MD = −23.21, 95% CI (−34.30, −12.12) P value <.0001 I2 = 92%; Figure 3(a)]. Forest plot for subgroup analysis.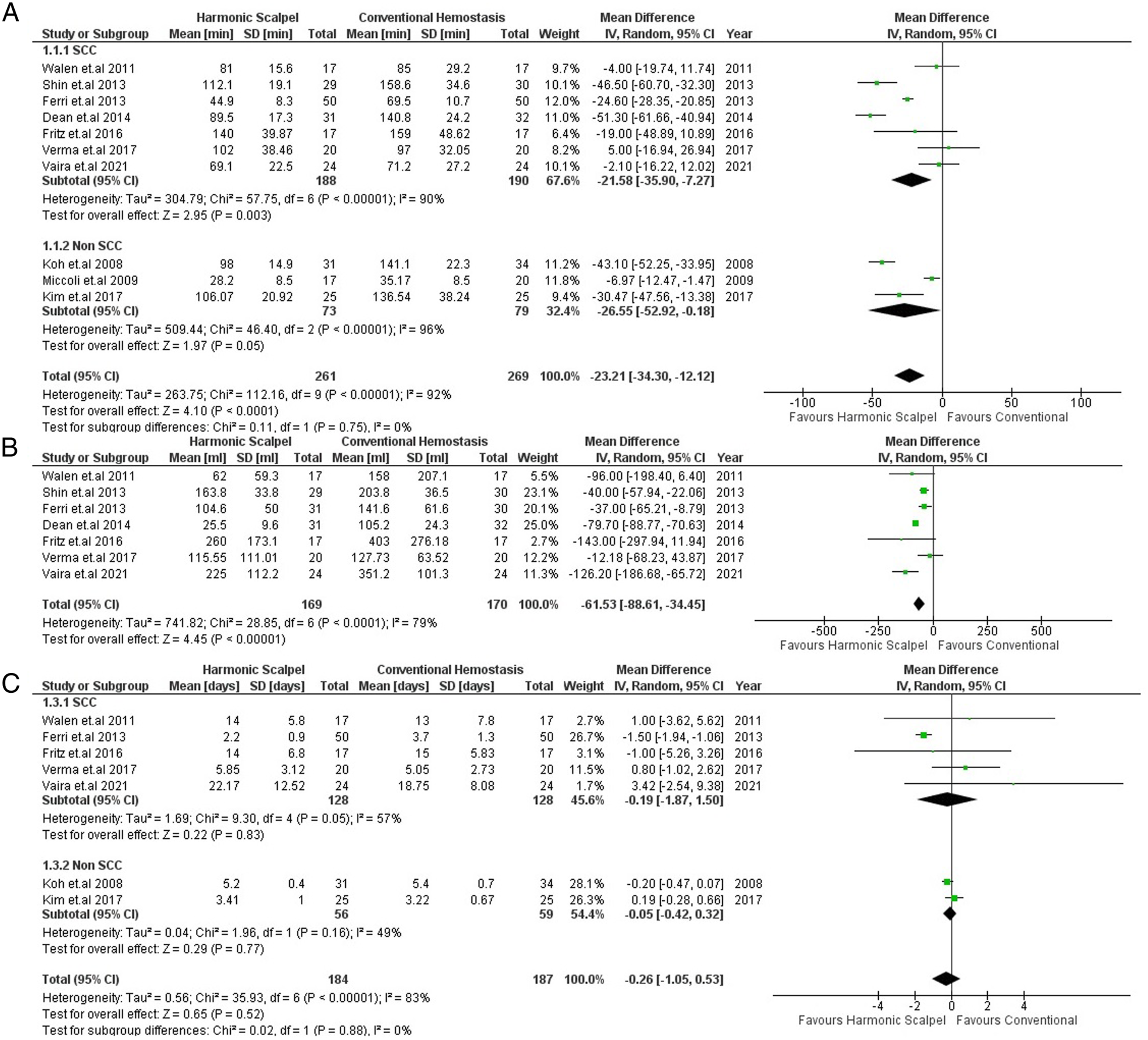
Intraoperative Blood Loss
Pooled analysis of 7 studies (Shin et al., 14 Ferri, 15 Walen, 16 Verma, 7 Vaira, 9 Fritz 11 and Dean 17 ) showed that HS significantly lowers intraoperative blood loss [MD = −61.53, 95% CI (−88.61, −34.45) P < .00001 I2 = 79%; Figure 3(b)].
Secondary Outcomes
Length of Hospital Stay
Seven studies (Koh, 12 Ferri, 15 Walen, 16 Verma, 7 Vaira, 9 Kim, 10 and Fritz 11 ) reported length of hospital stay. Analyzing their results revealed no significant difference in the length of hospital stay of the patients regardless of the technique being used [MD = −.26, 95% CI (−1.05, .53) P = .52, I2 = 83%; Figure 3(c)].
Total Drain Output
Of the 9 studies (Koh,
12
Miccoli,
13
Shin et al.,
14
Ferri,
15
Walen,
16
Verma,
7
Vaira,
9
Fritz
11
and Dean
17
) that had reported the total drain output, it was observed that using HS significantly decreased the volume of fluid collected in the drain, compared with conventional hemostasis [MD = −28.22, 95% CI (−52.56, −3.89); P = .02 I2 = 95%; Figure 4(a)]. Forest plot for subgroup analysis.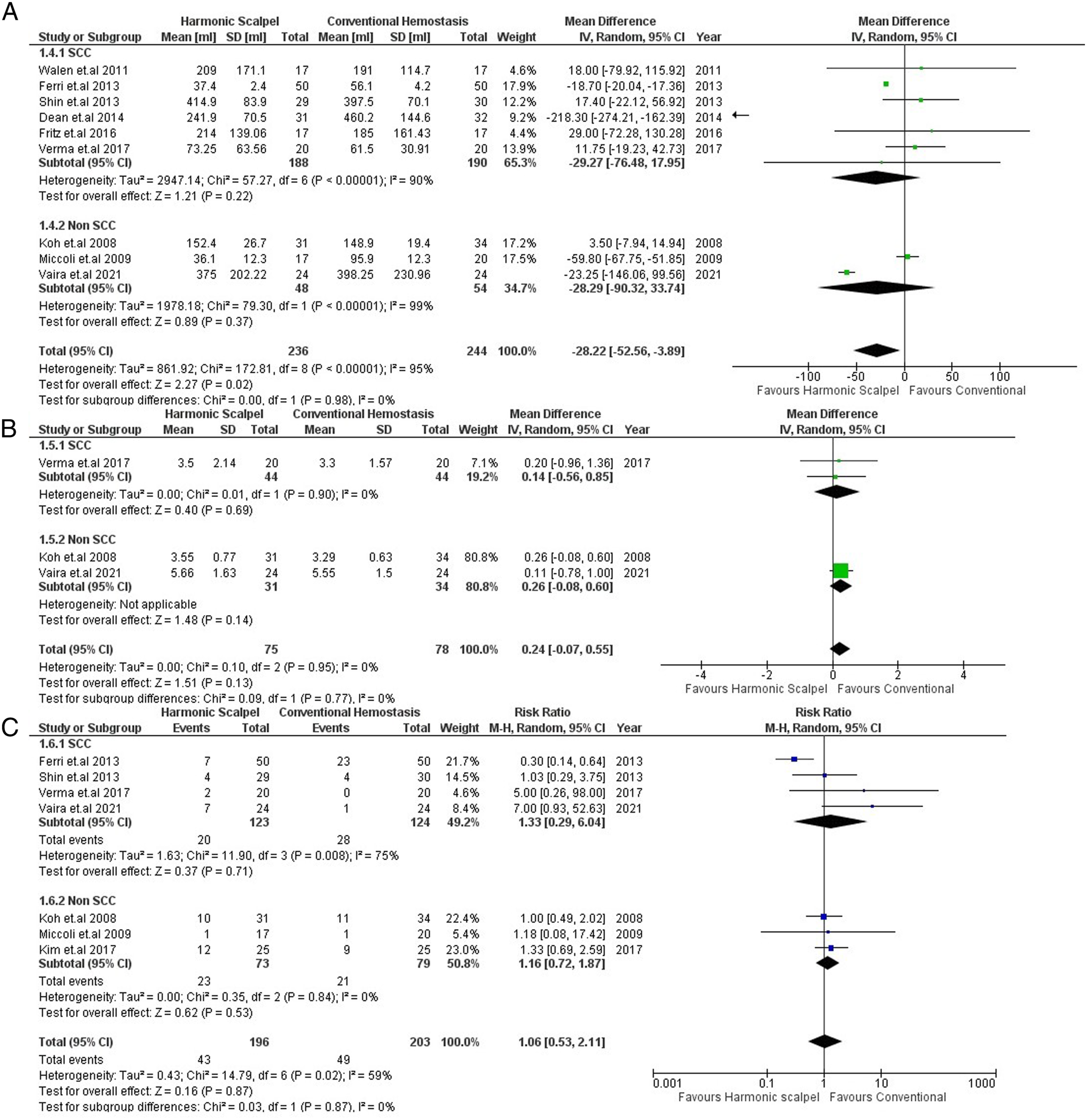
Length of Drain Stay
Among the 10 studies, only 3 (Koh, 12 Verma, 7 Vaira, 9 ) were able to provide data on the time duration the drain was kept in the patients. No significant difference in length of drain stay was observed between the 2 techniques [MD = .24, 95% CI (−.07, .55) P = .13, I2 = 0%; Figure 4(b)].
Postoperative Complications
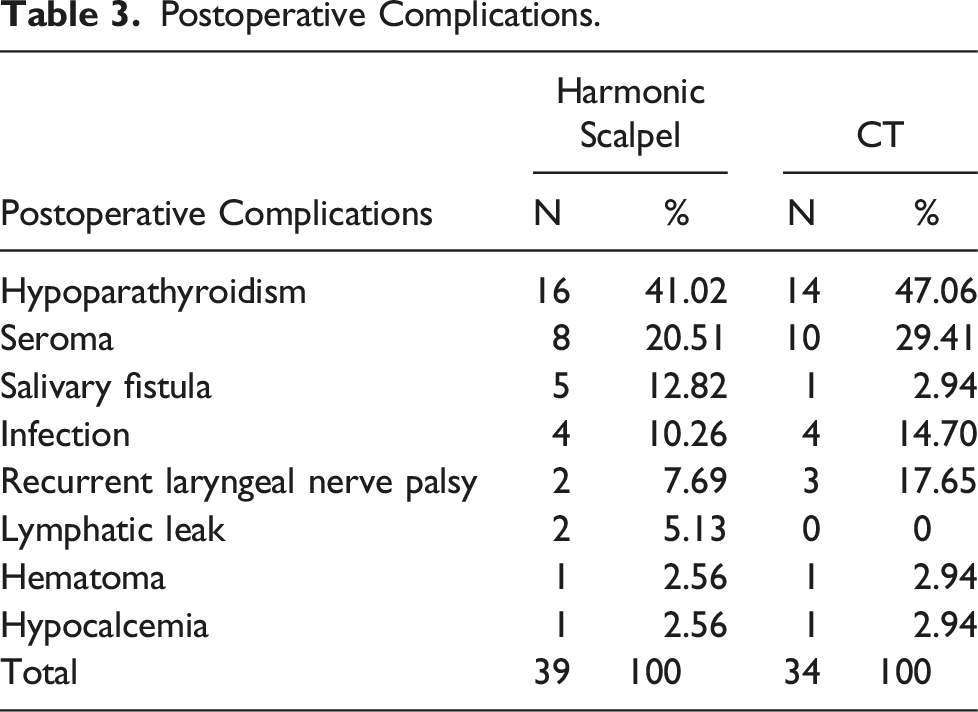
Postoperative Complications.
Subgroup Analysis
Subgroup analysis based on the histological type of head and neck cancer was carried out for all outcomes. There were no significant differences between the SCC and non-SCC subgroups for all outcomes, including operative time (P value for subgroup differences = .75), length of hospital stay (P value for subgroup differences = .88), total drain output (P value for subgroup differences = .98), length of drain stay (P value for subgroup differences = .77), and postoperative complications (P value for subgroup differences = .87) [Figures 3 and 4]. However, there was no significant difference in total drain output between HS and conventional procedures in both SCC and non-SCC subgroups (SCC: MD = −29.27 [−76.48, 17.95], P = .22, I2 = 90%); (non-SCC: MD = −28.29 [−90.32, 33.74], P = .37, I2 = 99%; Figure 4(a)).
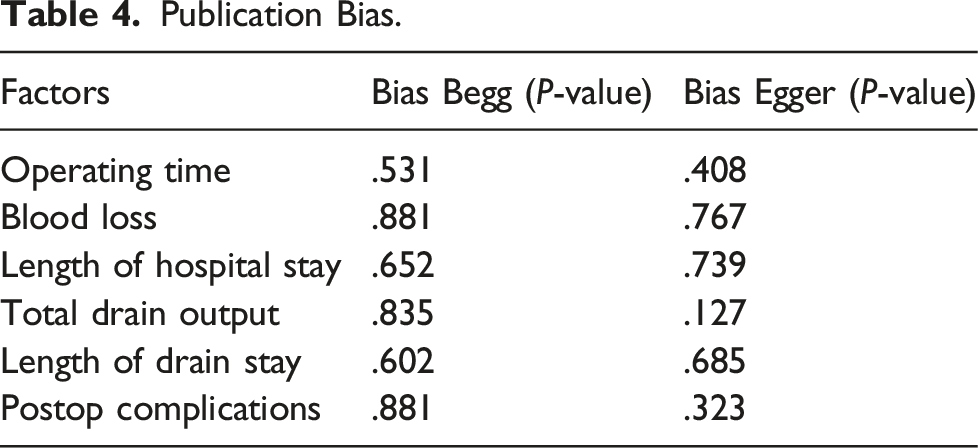
Publication bias
The funnel plots of publication bias are illustrated in Figure 5. No significant publication bias was seen among all the outcomes, and the individual P-values of Begg–Mazumdar’s rank correlation test and Egger’s regression test are presented in Table 4. Funnel plot for publication bias. SCC: Squamous cell carcinoma, SE: Standard error MD: Mean difference. Publication Bias.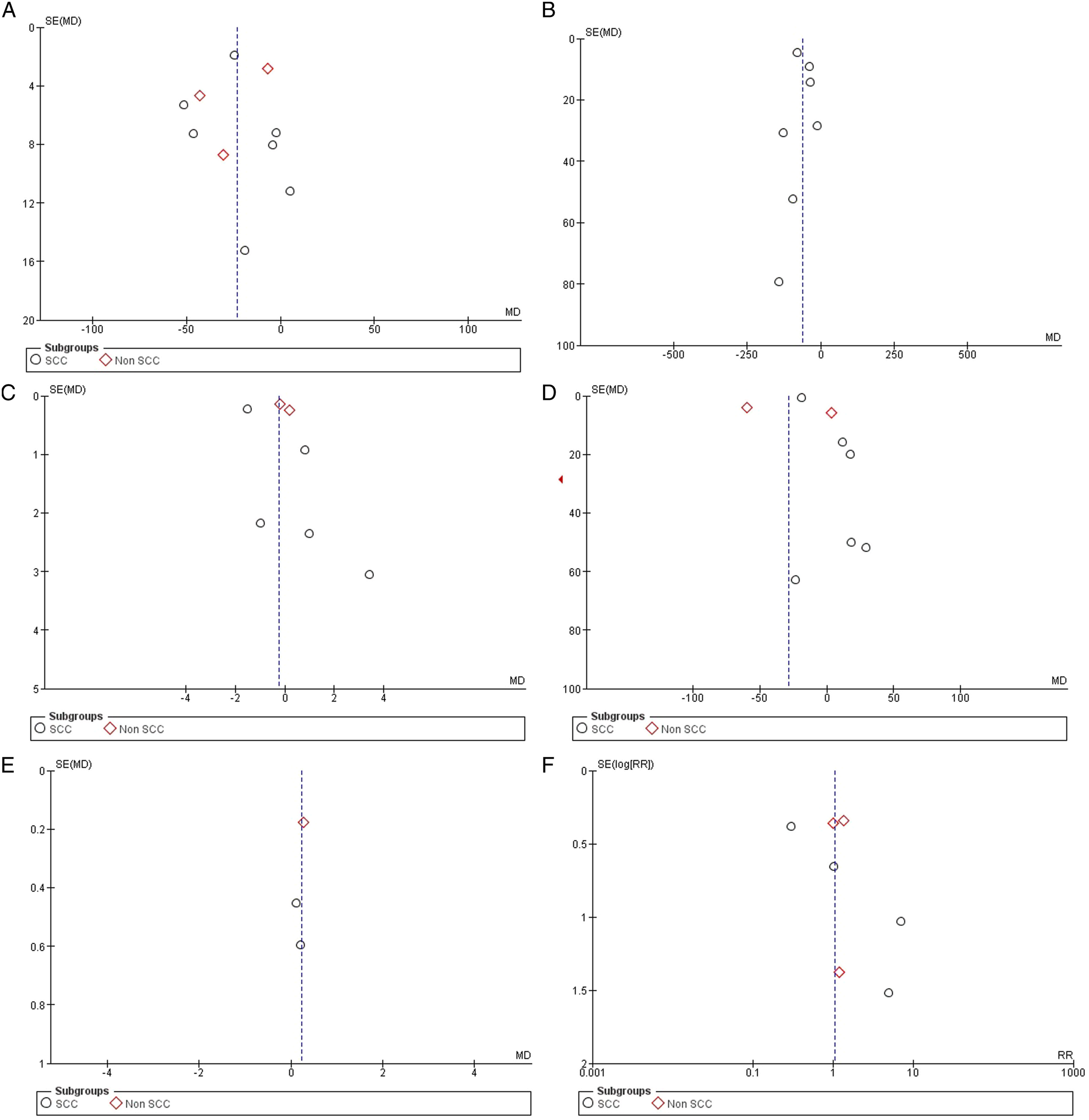
Discussion
Our meta-analysis of 558 patients undergoing ND using either the HS or conventional techniques, highlights the differences in outcomes achieved from both procedures. Existing literature displays the superiority of the HS technique when assessing intraoperative blood loss and operative time. 8 However, this is the first meta-analysis that assesses the duration of drain placement and postoperative complications.
Amongst outcomes assessed in previous studies, our study was consistent with findings of the HS having decreased operative time and intraoperative blood loss as compared to the conventional techniques. We also observed similar results as those known, when comparing length of hospital stay, confirming no difference in outcome between the 2 techniques. 8 In contrast to the study conducted by Ren ZH et al., our study showed significant difference in total drain output when comparing the 2 techniques.
Regarding the new outcomes assessed, our study found no significant differences between either technique in the duration of placement for the drain or postoperative outcomes.
This meta-analysis corroborated the known, reductive effect of HS on operating time. All of the 10 included studies (Koh, 12 Miccoli, 13 Shin et al., 14 Ferri, 15 Walen, 16 Verma, 7 Vaira, 9 Kim, 10 Fritz 11 and Dean 17 ) evaluated this outcome, and the overall mean reduction in time with the use of HS as opposed to conventional techniques was 23.21 minutes [MD = −23.21, 95% CI (−34.30, −12.12) P value <.0001 I2 = 92%].
Although significant, this finding portrayed great statistical heterogeneity of 92%. Discernible reasons for these differences include: differences in “start and stop points” for the operative time calculations across the trials,7,16 exclusivity of use of HS throughout the procedure vs the elevation of the cervical skin flap or some other step being performed with the monopolar scalpel/another conventional instrument in the HS group as well. 9 Further, nonuniform study cohorts including cases with variation in malignancies being treated and thus, different types of ND being performed to address different levels of neck nodes formed another major reason for discrepancies.7,13,15,16
Across previous exploration into HS in medical literature, the reduction in operative time has been attributed to the fact that performing the whole procedure with one instrument serving 4 functions, saves time in changing instruments (alternating cold knife to scissors to bipolar forceps, for example). 18 A virtually bloodless field, as in HS, permits increased visibility for the surgeon and facilitates identification of anatomical structures, thereby reducing dissection time.14,18 The vessel tying time is also reduced in the few cases where the HS is not able to perform hemostasis correctly. 18
Moreover, this meta-analysis expanded on the stated effect of the HS on intraoperative bleeding. 8 Pooled analysis of 7 studies (Shin et al., 14 Ferri, 15 Walen, 16 Verma, 7 Vaira, 9 Fritz 11 and Dean 17 ) showed that HS significantly lowers intraoperative blood loss [MD = −61.53, 95% CI (−88.61, −34.45) P < .00001 I2 = 79%].
This deduction of the hemostatic capacity of HS was challenged by the lack of mention of the method used to calculate blood loss in various studies. Additionally, the recent trial by Vaira et al. (2021) 9 that found a significant reduction in blood loss questioned the clinical relevance of a reduction of just over 100 mL with the use of HS. 9 Since more than 25% of the cases of HNSCC are diagnosed in the elderly population (>65 years) with extensive comorbidities, a statistic that is expected to surge up to 60% by 2030, 19 any reduction of operative time and intraoperative blood loss is a step forward in finding the surgical technique most appropriate for combatting HNSCC in the age group. The lasting hemostasis of HS extends to arteries up to 2 mm in diameter and veins up to 5 mm in diameter.6,18
Total drain output was significantly lower when using HS, compared with conventional hemostasis [MD = −28.22, 95% CI (−52.56, −3.89); P = .02 I2 = 95%].
A reduction in the amount of fluid drained post-surgery, desirable due to wound protection from bacterial contamination and better conditions for wound healing, 20 has been achieved more commonly with the use of HS in thyroidectomies and mastectomies.21,22 This has been linked to result from reduced intraoperative bleeding with HS allowing for more precise control of small vessels and has led to surgeons choosing to not place drains in cases with very low bleeding. 22 In alignment to the study conducted by Faisal M et al., when used for Modified Radical Mastectomy, HS showed significant reduction in total drainage volume. This can be attributed to superior hemostasis with less lateral thermal injury offered by harmonic technique dissection. 23 Additionally, the inflammatory response in the surgical site is diminished, fewer lymphatic vessels are damaged with proper closure for damaged lymphatic vessels, and the surgical site produces less oozing surfaces. Together these factors reduce postoperative drainage volume. 23
Seven studies (Koh, 12 Ferri, 15 Walen, 16 Verma, 7 Vaira, 9 Kim, 10 and Fritz 11 ) reported length of hospital stay. Analyzing their results revealed no significant difference in the length of hospital stay of the patients regardless of the technique being used [MD = −.26, 95% CI (−1.05, .53) P = .52, I2 = 83%]. This can be attributed to the fact that most patients prefer to stay as inpatients until the drains are removed completely. For these reasons, the length of hospital stay was relatively long in both groups.
As for the outcomes assessed by this meta-analysis for the first time, neither HS nor the conventional methods for ND were found superior in terms of duration of drain stay. With only 3 (Koh, 12 Verma, 7 and Vaira 9 )of the 10 trials assessing the former outcome, again, a void in available data surfaced that urges for the inclusion of this variable in further clinical evaluations of HS in ND’s.
Postoperative complications in head and neck surgery largely encompass hemorrhage, hematoma, seroma, chylous leakage, and neurologic complications as well as the more widely encountered postoperative neck and shoulder syndrome, seen in 30–70% cases of ND. 15 Given the precision of the instrument and that the thermal spread of HS is limited to 0–2 mm beyond the tissue grasped within the forceps of the device, the resulting tissue injury would expectedly be low. 15 However, high-power ultrasonic dissection may result in considerable heat production and accompanying tissue damage, especially when activation time exceeds 10 seconds.24,25 Animal studies have shown lasting fibroblastic reaction and delayed healing process, which in extrapolation, explains the seroma formation reported by other authors after mastectomy and axillary dissection. 26 In the recent trial by Vaira et al., 9 the few reported postoperative complications due to HS use included salivary fistulas and lymphatic leaks, plausibly due to decreased ability of the harmonic instruments to permanently close glandular structures and lymphatic ducts. 9 Thus, the need to consider supplementing HS use with a closure technique such as electrocautery or classic knot-tying for these cases emerges and serves as an additional avenue for further research regarding HS in ND. 9
In order to build a holistic picture of the efficacy of HS use in ND in head and neck cancers, evaluated outcomes in future will have to include cost vs efficacy, oncological safety, and the postoperative experience/well-being of the patient. 18 The outcome of postoperative pain measured via a uniform pain scale across trials would enable a cohesive comparison of the factor between different sets of techniques used in surgery. In addition, postoperative quality of life could effectively be gauged by charting the complications occurring at a 90-day follow-up, conducted in all patients. Recurrence of the cancer is another outcome which can be assessed by following the patients inducted in future trials for the long term and by possibly publishing the results in subsequent articles after the trials. Lastly, assessing “surgeon friendliness” of the instruments can be factored in by including the number of surgeons required per team in ND conducted via HS as opposed to conventional techniques, as well as by their required level of skill/experience to conduct both kinds of procedures and the learning curves associated with each sort of technique.
Limitations
The results of this meta-analysis are restricted by a few limitations. Due to the availability of only 10 published studies on the theme, the number of cases used for analysis was also small. Further, the level of statistical heterogeneity prevalent amongst these studies was noteworthy, as was the publication bias depicted by the asymmetry in the funnel plot. Several of the trials provided incomplete information regarding the blinding, allocation concealment, and randomization, thereby limiting judgment about the quality of these randomized controlled trials.
Conclusion
This meta-analysis validated the established evidence regarding the reductive effect of HS use in neck dissection, relating to the parameters of operative time and intraoperative bleeding. It also confirmed the lack of superiority of the HS method over conventional techniques, where length of hospital stay is concerned. Expanding on available data, this article additionally evaluated the outcomes of length of drain stay and postoperative complications, finding no significant differences between surgeries using HS vs those using traditional methods. Albeit limited in power of its quantitative analysis by the aforementioned limitations, this article demonstrates HS as being an effective method for continued consideration in HNC neck dissection. Future randomized controlled trials consisting of larger sample sizes and including the added outcomes listed above are required to authenticate our findings and improve understanding of the comparative use of HS vs conventional methods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
No IRB approval was required for the article as human subjects were not involved.