
Abstract
Introduction
Nasal valve compromise is an important cause of airflow obstruction. The nasal valves, where the greatest airflow resistance is located, are further divided into external and internal nasal valves.1,2 The external nasal valve is defined as a part of the vestibule that is bounded by the lateral crus of the lower lateral cartilage and fibrofatty tissue of the alar rim laterally, the caudal septum positioned between the medial crura of the lower lateral cartilages medially, and the nasal floor inferiorly. 3 External nasal valve obstruction could be either static or dynamic. Static obstruction results from a narrowed nostril as in stenosis of the pyriform aperture, deviated caudal septum, anterior nasal spine (ANS) encroachment, and post-surgical vestibular skin cicatricial stenosis.4,5 While dynamic obstruction results from the collapse of the lateral nasal wall. Also known as zone 2 lateral wall insufficiency. 6
The ANS is a small midline protruding bone between the alveolar bone and the nasal pyriform. It holds the attachment for the caudal nasal septum providing support to the nasal tip and projection to both the nose and the upper lip.7,8 To achieve a high functional and esthetic outcome, the ANS can be removed, 9 recontoured, 10 fixed in position, 7 augmented, 8 or fractured and relocated. 11 The relation of the ANS is very close to the medial crural footplates and any shift or tilt of the spine will cause the footplates to encroach the nasal opening. Such a deformity should be corrected to remove its influence on the surrounding structures in the caudal part of the nose. 12
This case report aims to describe a novel approach to address nasal obstruction due to a severely deviated ANS and caudal septal deviation by relocation of the ANS combined with the modified extracorporeal septoplasty and anterior septal reconstruction (ASR).13,14
Case Report
A 42-year-old male referred to the senior author’s (S.M.) clinic for treatment of nasal obstruction that has been present all his life. The obstruction was mainly on the left side that usually exacerbates during sleep, exercise and flu season. Nasal steroids were taken for 6 months without improvement. The patient was diagnosed with obstructive sleep apnea and reported difficulty adapting to positive pressure therapy. Patient denied a history of trauma to the nose or previous nasal procedures.
On examination, the septum showed caudal septal deviation to the left and moderate bilateral turbinate hypertrophy. A positive Cottle maneuver determined the presence of left nasal valve obstruction. Review of his pre-operative CT scan showed bilateral turbinate hypertrophy, deviations of the perpendicular plate of ethmoid, and a shifted ANS to the left side (Figure 1). Pre-operative CT showing deviated ANS.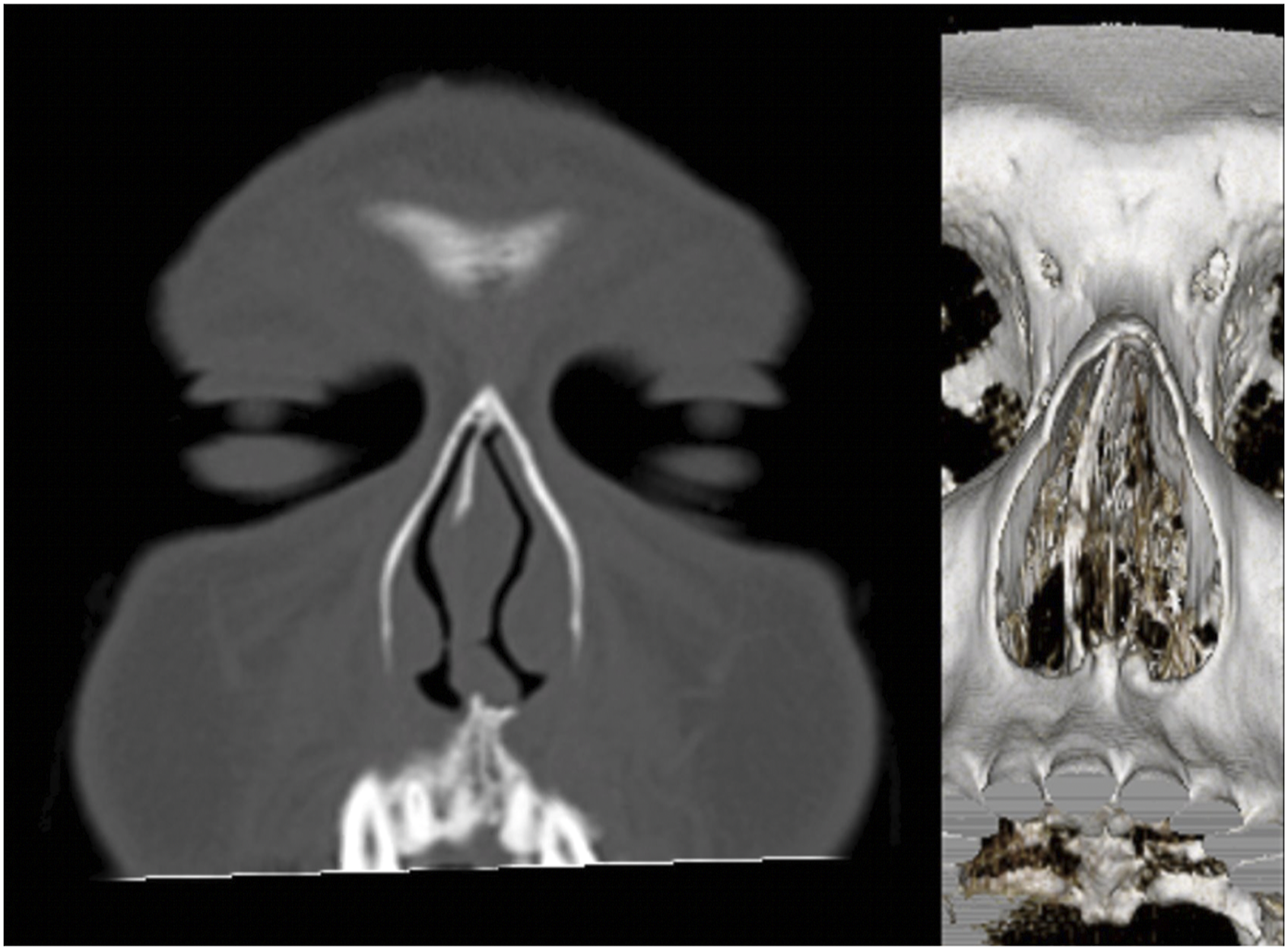
The patient was scheduled for a functional rhinoplasty to relieve his nasal obstruction and correct the caudal septal deviation. The procedure was performed using a standard open rhinoplasty approach combined with anterior septal reconstruction and anterior nasal spine relocation. The patient was managed as an outpatient. Medications and wound care instructions were given. Intranasal Doyle splints, external taping, and nasal splits were left in place for 7 days post-operatively. Follow-up at 1 and 2 weeks confirmed a stable repair and improvement in nasal breathing.
Surgical Technique
The septum was approached using a left hemitransfixation incision and full subperichondrial dissection of the septum was done on the left side reaching the bony septum posteriorly with exposure of the septal spur. Dissection continued down to the nasal floor, the dorsum, and around the antero-caudal region to access the right subperichondrial plane and expose the septum completely.
A standard external rhinoplasty approach was connecting a transcolumellar incision to bilateral marginal incisions. The upper lateral cartilages were then released from the dorsal septum allowing full visualization of the septum. To access the anterior nasal spine, the intercrural and interdomal ligaments were separated. Electrocautery was used over the premaxilla preserving the overlying ANS periosteum. The septum was incised preserving at least 15 mm from the keystone bony junction, with at least a 10 mm vertical height near the keystone area, and tapered to 10 mm at its most anterior end creating the dorsal strut. Cartilage inferior to that incision including the anterior septal angle was carefully excised as well as any bony deviations in the perpendicular plate of ethmoid. Care was taken not to torque on the skull base.
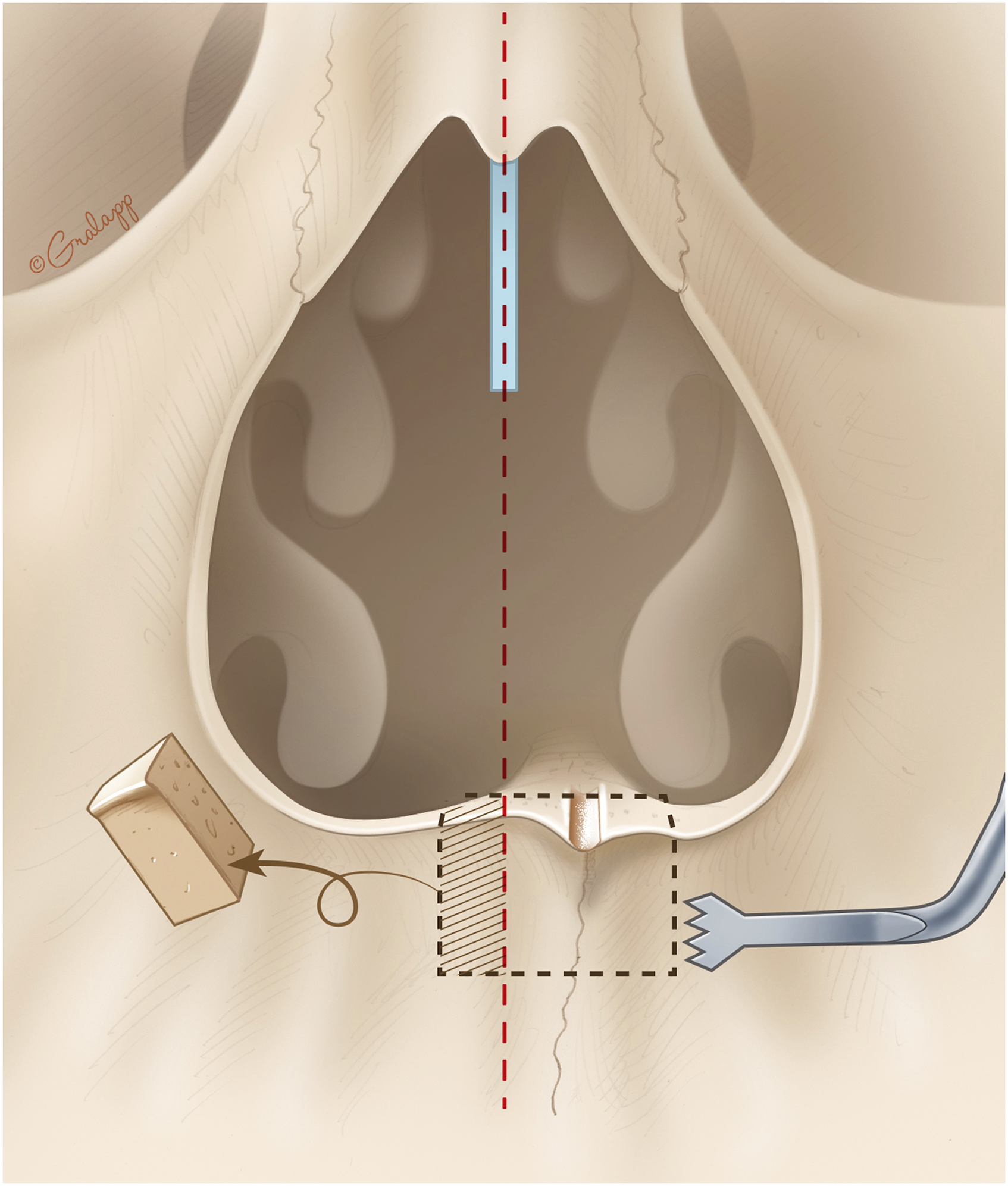
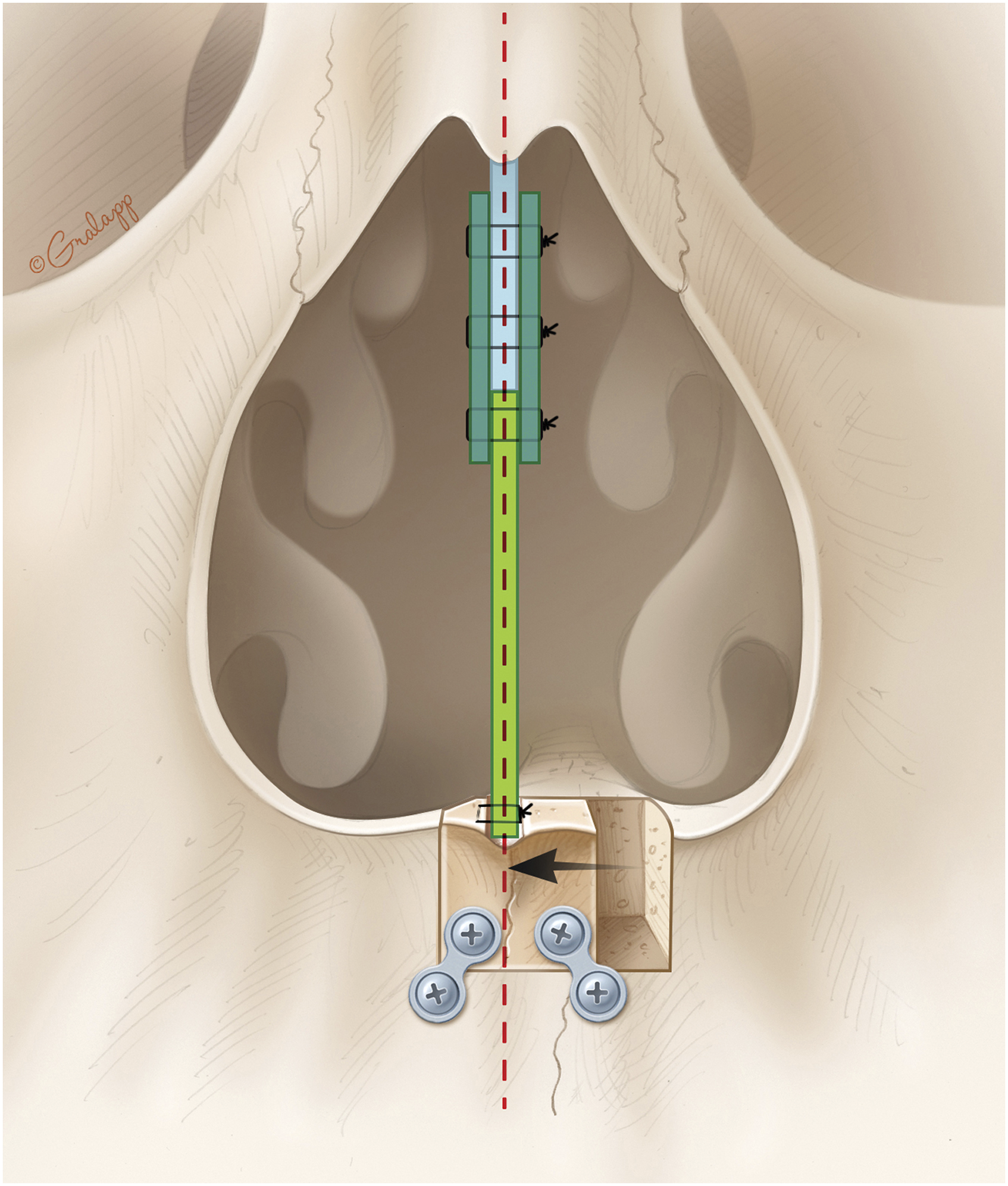
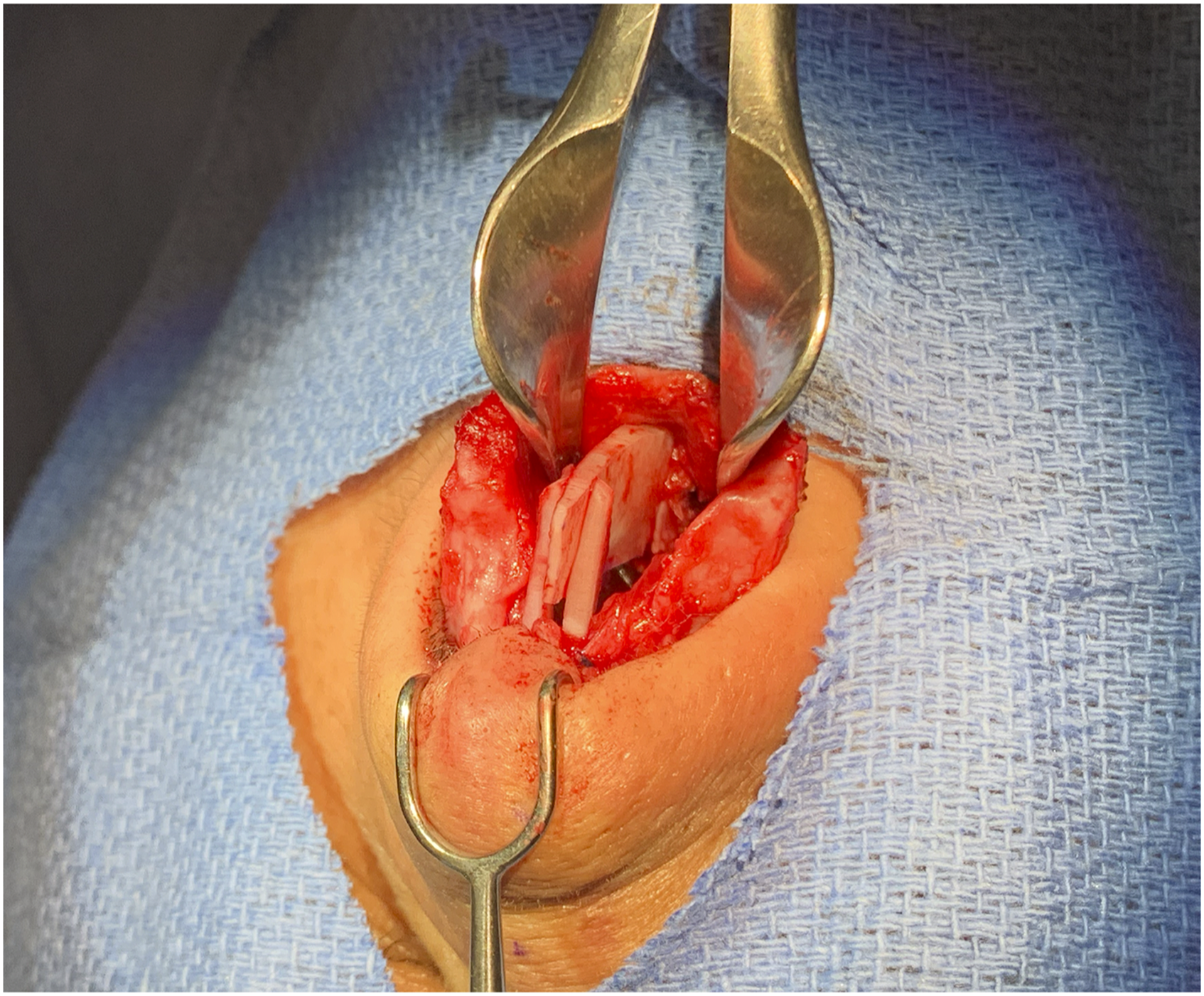
The maxillary spine was found to be shifted 4 mm to the left side away from the upper lip midline (Figure 2). Using the straight piezo saw, maxillary osteotomy was performed creating a rectangular en-bloc harboring the ANS and an ostectomy of 3 mm was performed on the right side. Care was taken to avoid injury to the neurovascular bundle of the upper incisors (Figure 3). This resulted in a mobile ANS allowing its relocation to settle in the midline. For stability, the relocated ANS was fixed in place using two .5 mm microplates and four 3.5 mm screws. This was performed by taking the ANS on the side table for precise drilling and application of bilateral microplates and screws (Figure 4). The spine was repositioned back on the premaxilla and fixation was completed. The straightest possible portion of the septal cartilage was fashioned into an ASR graft and placed on the newly positioned ANS. Two extended spreader grafts were sutured in place and fixed to the ASR graft (Figure 5 and 6). A tongue-in-groove suture was taken to adjust tip rotation and achieve tip support as described previously.
15
The upper lateral cartilages were repaired and fixed to the nasal dorsum. The hemitransfixation, marginal, and transcolumellar were closed in a standard fashion. Nasal tip position, nostril symmetry, and columella were all checked. As well as adequate contour and tip support. Bilateral Doyle splints were placed, and standard taping and splinting were applied. The anterior nasal spine is shifted to the left side. The light blue structure is the preserved dorsal septal strut. The straight piezo saw is used to do a 3 mm ostectomy on the right side of the anterior nasal spine and rectangular osteotomies are done to reposition the spine in the maxillary midline. Anterior nasal spine with bilateral Microplates, that will provide internal fixation, in position. The caudal strut (light green) supported by two extended spreader grafts (dark green) is fixed to the dorsal strut (light blue) superiorly and to the ANS periosteum inferiorly. The Relocated nasal spine is fixed to the premaxilla with microplates and screws in the midline. The newly reconstructed anterior septum provides a stable infrastructure for the nasal framework.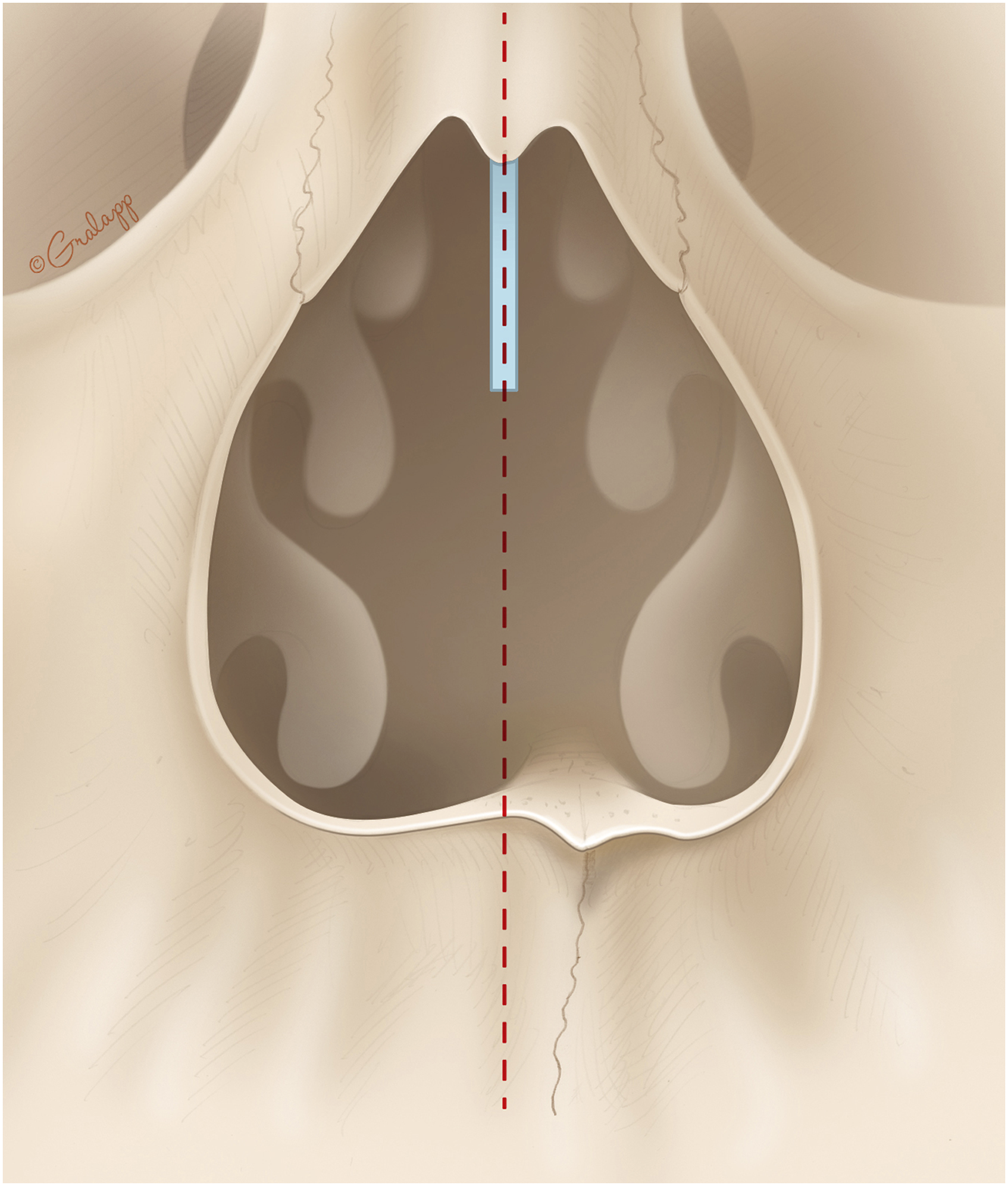

Discussion
Several techniques have been used to correct caudal septal deviation. Including the swinging door caudal septum repositioning. 16 Extracorporeal septoplasty, first described by Peer and later popularized by Gubisch, is a method to reconstruct severe caudal septal deviations.13,17-19 The main drawback with this technique is the tendency to have dorsal irregularity arising from the total disjunction of the keystone area. The anterior septal reconstruction (ASR) is convenient for saving the valued nasal keystone region, the bone and cartilage junction of the upper and middle thirds of the nose, providing a dorsal strut for a stable septal foundation.13,14 The anterior nasal septum is the pointing bone lying most anteriorly on the premaxilla where the caudal septum rests. 20 Historically overlooked as a possible cause for caudal septal deviation, abnormalities in the nasal spine can often be the source of distortion of the lower nose. Therefore, it is very important to identify and correct any deviation of the ANS.
Reconstruction of the septum in the midline requires continuity between the premaxilla/pyriform aperture and the anterior nasal angle (ANA). As such, the septal construct must either sit on an intact, stable nasal spine or the pyriform aperture itself. The former is favored for two reasons. First, the required length of the septal replacement graft is reduced. Second, the nasal spine itself may cause deformity and/or obstruction of the nasal airway. Thus, correction of its position is preferable.
Guyuron and Behmand 12 stressed the importance of having a midline ANS and the presence of any tilt or displacement should be corrected. The position of the ANS can be adjusted by doing a greenstick fracture at its base by a 4 mm osteotome. After correcting the caudal septal deviation with excision and placing it in the midline, a caudal strut is placed to provide nasal tip support and improve projection. The support of the spine in the midline position then becomes dependent on the corrected lower lateral cartilages and a straight septum. Ng et al 11 described a similar technique using a 3 mm chisel with a 30-to-45-degree angle from the horizontal plane with or without raising a mucoperichondrial flap. The nasal spine is to be fractured without violating its junction with the caudal septal cartilage. A similar method for ANS relocation was described by Constantine et al 21 where ANS removal is combined with caudal septum suturing to the premaxilla as an alternative method. Such a technique does not ensure ANS stability and a shift to its original position is conceivable. Gubisch 22 describes how a side-to-side spine to septum fixation suffices to address minor deviations of the spine. For major deviations, ANS osteotomy followed by open reduction and microplate internal fixation is warranted. One case report of internal fixation of an ANS after trauma was performed via an upper gingival incision. 7 Cleft lips are a common cause of severely deviated ANS that could be adjusted during orthognathic surgery, by means of spine released from the premaxilla by reciprocating saw and fixation to the targeted location by interosseous wires. This procedure is performed with the deviated septum still attached to the ANS. 23
Conclusion
To our knowledge, this is the first report of sliding ostectomy and internal fixation of the nasal spine in rhinoplasty. This case description presents a method to slide and rigidly fixate the ANS to a central position on the premaxilla utilizing ASR to correct the caudal septal deviation associated with ANS malposition via an open rhinoplasty approach.
The institutional review board has determined that this project does not meet the definition of research as defined in 45 CFR 46.102(d), nor the definition of clinical investigation as defined in 21 CFR 50.3(c).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by American Heart Association AHA #19CDA34660245 award to T.F.C