
Abstract
Background:
Unplanned extubations (UE) are directly associated with morbidity, mortality, and increased health care costs among critically-ill children. Multi-center implementation of the Solutions for Patient Safety Network prevention bundle has been successful, but UE rates remain a common cause of preventable health care harm.
Methods:
This was a longitudinal (2020–2025), multi-intervention quality improvement (QI) project in a single quaternary care pediatric intensive care unit (PICU) driven largely by a new QI respiratory therapist. Interventions built upon the initial implementation of the UE prevention bundle. The smart aim of this project was to sustainably decrease UE/100 invasive ventilation days in the PICU at Children’s of Alabama by 50% through multiple Plan-Do-Study-Act (PDSA) cycles.
Results:
The baseline event rate was 0.58 UE/100 invasive ventilation days. Criteria for a center line shift to 0.16 UE/100 invasive mechanical ventilation days (72.5% decrease) were met in the first quarter of 2023 following four PDSA cycles and sustained through the end of the project. There was no change in invasive ventilation days/patient/quarter, but the percentage of PICU patients exposed to invasive ventilation by quarter starting dropped from 42% to 33% beginning in the first quarter of 2021. There were no center line shifts in post-UE outcomes over the project period including re-intubation within 1 h, re-intubation with cardiopulmonary resuscitation, or no re-intubation.
Conclusions:
Through multiple interventions, UE/100 invasive ventilation days decreased by 72.5% and has been sustained from the first quarter of 2023 through the second quarter of 2025 without impacting balancing measures such as invasive ventilation duration. These results support the importance of building upon the Solutions for Patient Safety Network UE prevention bundle and having a dedicated champion to drive improvement and sustainability.
This is a visual representation of the abstract.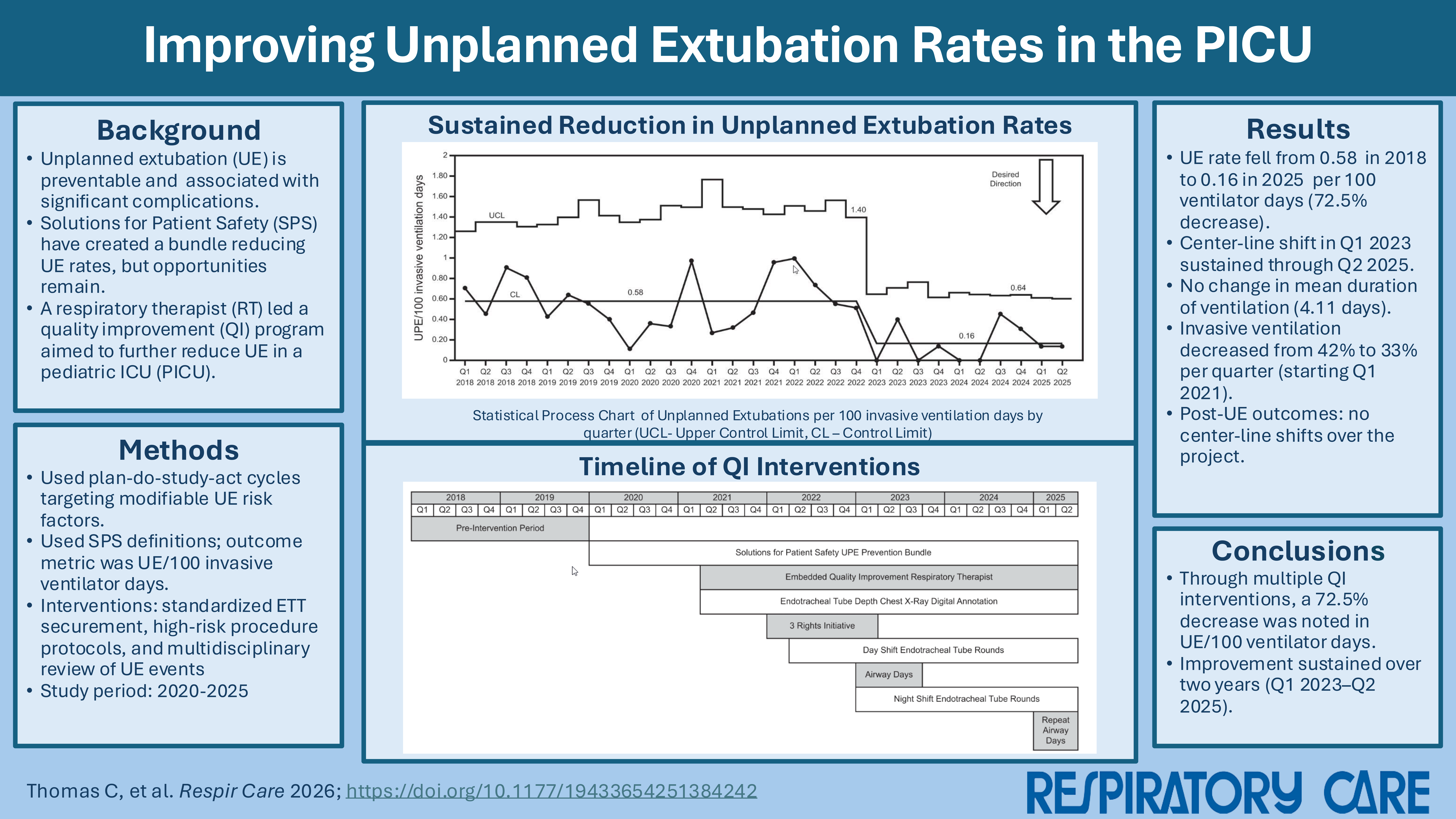
Introduction
Invasive mechanical ventilation is a common support modality required for ∼350,000 critically ill children annually in the United States.1–2 Extubation is the planned removal of the endotracheal tube (ETT) required for invasive ventilation. However, unplanned extubations (UE) are common in pediatric intensive care units (PICUs) with a reported rate that varies widely from 0.11 to 2.27/100 invasive ventilation days. 3 These events can result in significant increases in health care costs as well as morbidity and even mortality.4–6
There are concerted national efforts to limit these events through systematic quality improvement (QI). The most notable is the Solutions for Patient Safety (SPS) Network’s efforts that began in 2018 with the implementation of a UE prevention bundle. Standardized anatomic reference points/securement methods and protocols for high risk situations were the two required elements. The two recommended elements were active discussion of extubation readiness and multidisciplinary apparent cause analyses of UE events. Multi-center implementation of the bundle has led to a sustained 19.9% decrease in UE rates per 100 invasive mechanical ventilation days. 7 However, the burden remains higher than desired given the associated complications at 0.52 UPE/100 invasive ventilation days. There is a need to build upon the successes of the SPS UE prevention bundle and further decrease this preventable harm. Targeted interventions should focus on known modifiable factors such as inadequate ETT securement, invasive ventilation duration, and appropriate ETT protection during procedures and routine care.
In this manuscript we describe a longitudinal, multi-intervention QI project aimed at sustainably decreasing UE/100 invasive ventilation days in a single quaternary care PICU. This effort was driven by a newly developed, embedded QI respiratory therapist (RT) in the PICU.
QUICK LOOK
Current knowledge
Despite successful efforts to improve rates of pediatric unplanned extubations (UE), they remain an important cause of preventable harm that leads to increased health care costs.
What this paper contributes to our knowledge
Through multiple QI interventions we achieved a decrease in the UE/100 invasive ventilation days rate of 72.5% that has been sustained for over two years. These results support the importance of building upon the Solutions for Patient Safety Network prevention bundle and that of a dedicated champion to drive improvement and sustainability.
Methods
Setting and baseline practices
Children’s of Alabama is a quaternary care, free-standing, pediatric hospital. The PICU has 24 beds with 1,800–2,000 annual admissions with approximately 30–40% requiring invasive ventilation via an ETT. Two clinical teams composed of an attending physician, fellow physician, resident physicians, and nurse practitioners round on patients daily. There is dedicated RT coverage 24/7 with 3–5 RTs covering per shift based on patient census and acuity. Attending physician coverage is present 24/7. Separate from the PICU, there are two intermediate care units, a neonatal intensive care unit, and a cardiovascular intensive care unit. Neither of the other ICUs participated in this UPE QI work.
All patients requiring invasive mechanical ventilation via an ETT are managed with Servo-U ventilators (Getinge, Gothenburg, Sweden). Cuffed ETTs ranging between 3.0 mm and 7.5 mm inner diameter are used almost exclusively (Medtronic, Minneapolis, MN, USA). ETTs are secured based on patient age, size, and clinical status following manufacturer specifications. Infants and small children have ETTs secured with the appropriately sized Neobar (NeoTech, Valencia, CA, USA). ETTs ≥ 5.0 mm are secured with an AnchorFast device (Hollister, Libertyville, IL, USA). Patients with facial trauma, contraindications to the Neobar or AnchorFast, or with a nasal ETT receive cloth tape securement.
All data were obtained from local internal QI datasets and dashboards focused on UE. The manuscript was prepared following the SQUIRE guidelines for reporting QI projects. The project was assessed using the University of Alabama QI Self-Determination Tool and found to not meet the federal definition of human subjects research.
QI respiratory therapist
The PICU QI RT position was created in early 2021. The position’s primary directive was to ensure high quality respiratory care delivery to all patients in the PICU through the participation in quality assurance and improvement initiatives. The PICU QI RT rounds with the clinical teams each weekday in the PICU. There is also a PICU QI nurse position that works collaboratively with the PICU QI RT. The PICU QI nurse and QI RT alternate rounding with each of the two teams daily. A single RT has been in the role since being hired in the third quarter of 2021.
Measurements and outcomes
The primary outcome was UE/100 invasive ventilation days. The definition of a UE followed that used by the SPS Network: any dislodgement of an ETT from the airway that is not intentional with the exclusion of tracheostomies. 7 Ventilator days are defined as the presence of an ETT for any period during a given calendar day. Outcomes of UE were classified into three categories: re-intubation within 1 h, re-intubation with cardiopulmonary resuscitation, or no re-intubation. The smart aim of this QI project was to sustainably decrease the rate of UE/100 invasive mechanical ventilation days in the PICU at Children’s of Alabama by 50% through multiple Plan-Study-Do-Act (PDSA) cycles.
Interventions
The interventions for each PDSA cycle are described in Table 1 along with process measures for each. The PICU QI RT was responsible for the implementation, monitoring, and sustainability of each intervention with the support of PICU and RT hospital leadership. The Performance Improvement Department at Children’s of Alabama supported these efforts through the UE multidisciplinary team that meets regularly to oversee all UE efforts across the organization.
Interventions to improve rates of unplanned extubations
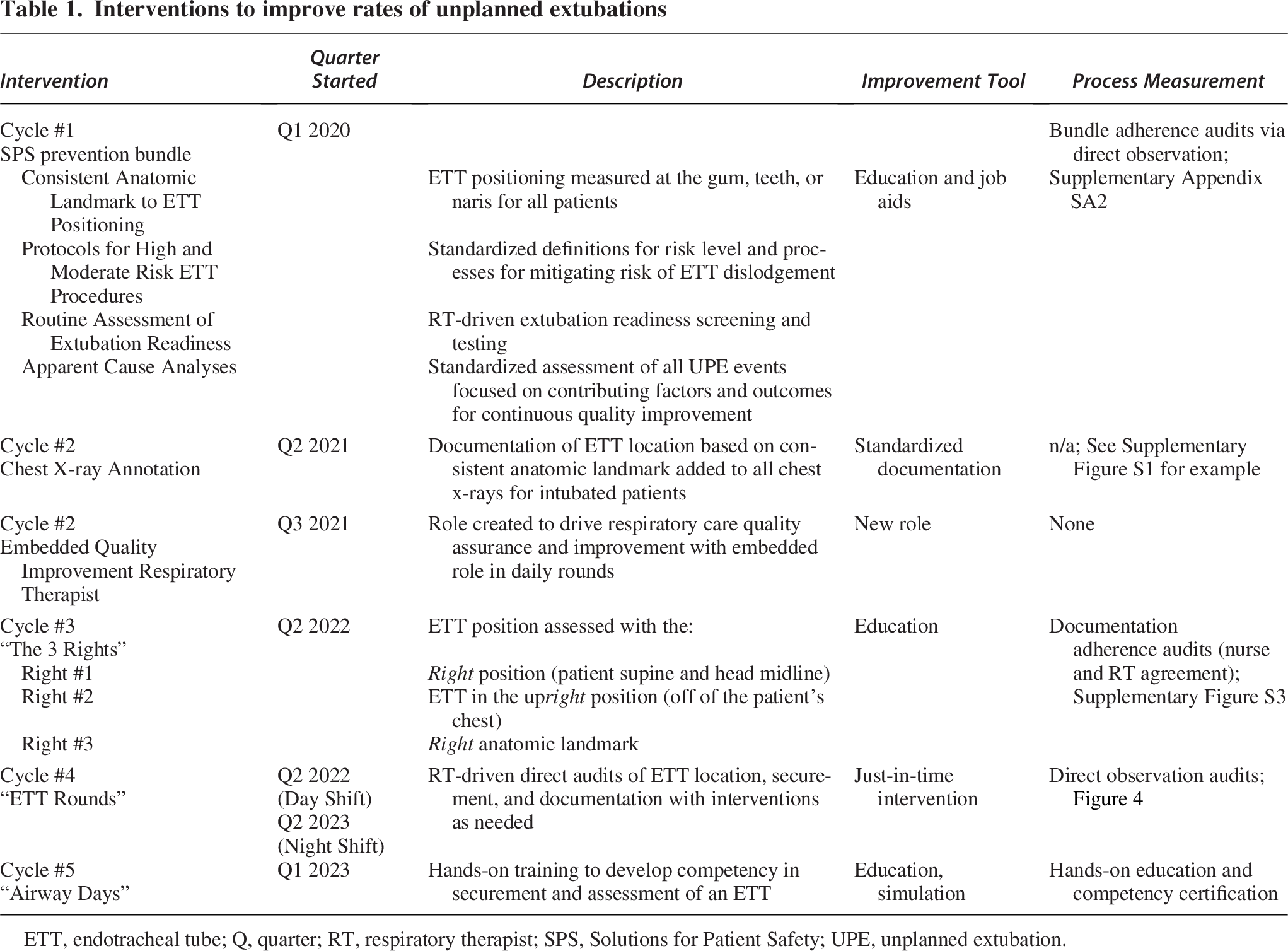
ETT, endotracheal tube; Q, quarter; RT, respiratory therapist; SPS, Solutions for Patient Safety; UPE, unplanned extubation.
The first PDSA cycle included the implementation of the SPS UE prevention bundle. This bundle included Apparent Cause Analyses for all UEs that were discussed at each hospital UE Performance Improvement meeting. Supplementary Appendix SA1 includes the audit form and the relevant job aids. In the second PDSA cycle, digital annotation of ETT position using a standardized landmark (teeth, gum, or naris) was added to all chest x-rays for patients with ETTs (Supplementary Figure S1). A licensed clinician had to confirm and report the depth. Importantly, daily chest x-rays were generally performed on all intubated patients <20 kg each evening in the PICU. Patients ≥ 20 kg had daily images based on the clinical scenario. The third PDSA cycle was triggered when frequent discrepancies between RT and nurse documentation on ETT depth was noted during routine audits by the PICU QI RT. This led to “The 3 Rights” education intervention for determining ETT depth. “The 3 Rights” include 1) the head in the right position, 2) ETT in the upright position, and 3) the right landmark. “ETT Rounds” were the fourth PDSA cycle where in-person audits and just-in-time interventions were performed to ensure proper securement, location, and documentation for all intubated patients. Finally, the fifth PDSA cycle included hands-on training for airway securement using airway simulators. All members of the interdisciplinary team were invited to attend with RTs and bedside nurses being required to fulfill a core competency.
Co-interventions
During the PDSA cycle timelines described above, there was a parallel effort to adopt all bundle elements of the Society for Critical Care Medicine’s ICU Liberation Bundle. 8 Several projects focused on RT-driven extubation readiness assessment, analgosedation, and delirium prevention were undertaken. These have been published separately.9–11
Statistical analysis
In accordance with QI methodology, UE/100 invasive mechanical ventilation days was presented in a U-statistical process control chart using QI Macros (KnowWare International, Denver, Colorado) for Excel (Microsoft, Redmond, Washington). Upper and lower control limits were calculated as three standard deviations (σ) above the center line. Eight consecutive points below the center line were required to qualify for a center line shift. This rule correlates with a P value <.01. 12
Results
Prior to any interventions (Q1 2018–Q4 2019), the mean UE/100 invasive ventilation days was 0.58. PDSA cycle #1 began in Q1 2020. The predefined threshold for special cause variation was met in Q1 2023, leading to a decrease in the center line to 0.16 UPE/100 invasive ventilation days. This represents a 72.5% decrease in the UPE rate that has been sustained through Q2 2025. These results are shown in the U-statistical process control chart in Figure 1 along with a timeline of interventions and co-interventions. Mean invasive ventilation duration is shown as an individuals’ statistical process control chart in Supplementary Figure S2a. Over the project period, there was no center line shift with an average of 4.11 invasive ventilation days/subject/quarter. In contrast, there was an absolute 9% drop (42% to 33%) in the percentage of PICU subjects exposed to invasive ventilation by quarter, starting in the first quarter of 2021. This was sustained throughout the remainder of the project period (Supplementary Figure S2b).
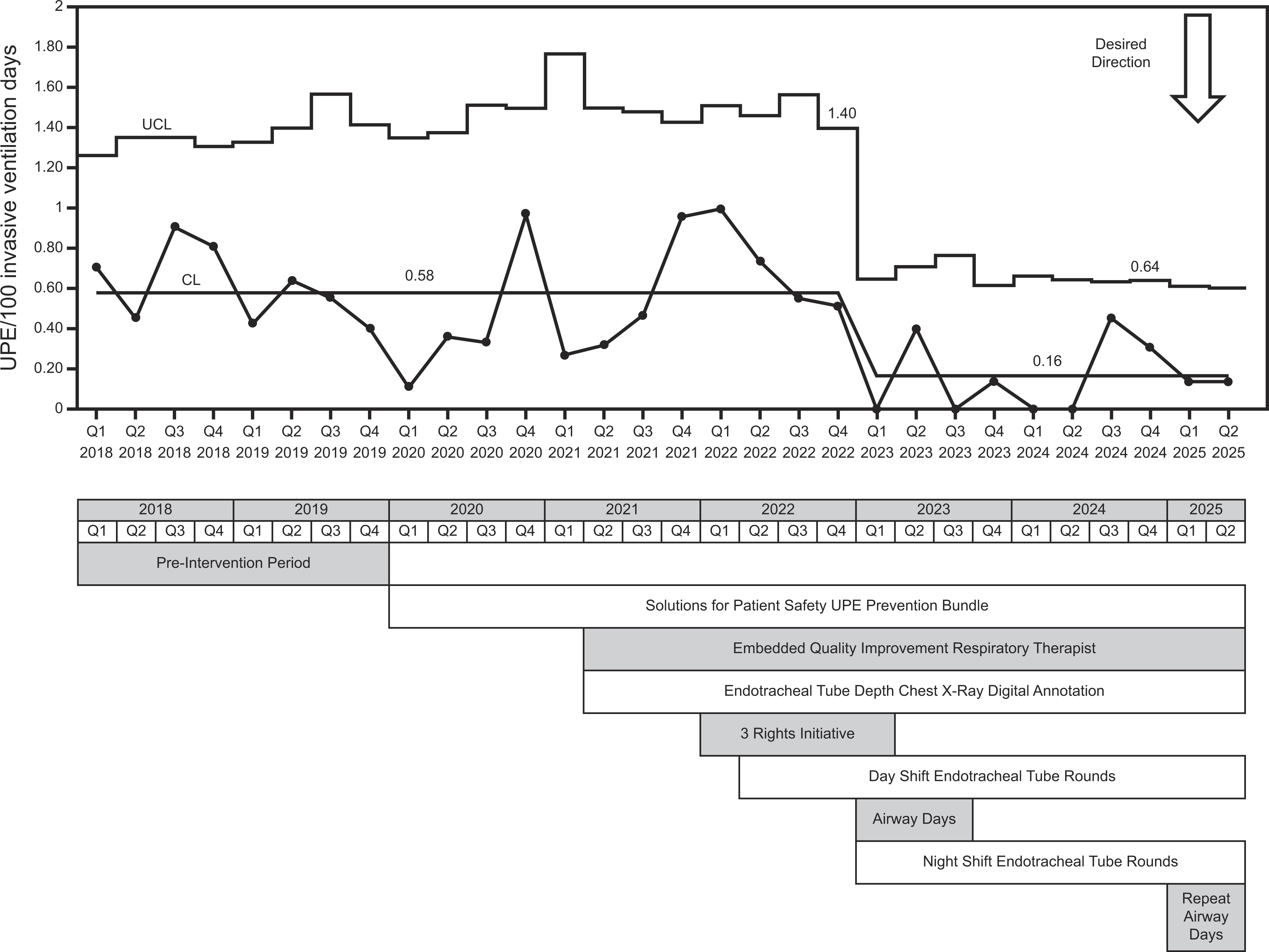
U-statistical process control chart (above) and timeline of process changes (below) and their associations with changes in unplanned extubation rate per 100 invasive ventilation days by quarter.
The median age among all UE events was 25 months (IQR 5–83 mo). Outcomes for all UEs annually are shown in Figure 2 On average following a UE, 45% (annual maximum: 66.7% in 2023; minimum: 38.5% in 2018) did not require re-intubation, 51% (annual maximum: 61.5% in 2018; minimum: 33.3% in 2023) required re-intubation within 1 h, and 6% (annual maximum: 33.3% in 2024; minimum 0% in 2018, 2020, and 2023) were re-intubated with cardiopulmonary resuscitation ongoing. There were no center line shifts in these post-UPE outcomes over the project period (Supplementary Figure S3A-C).
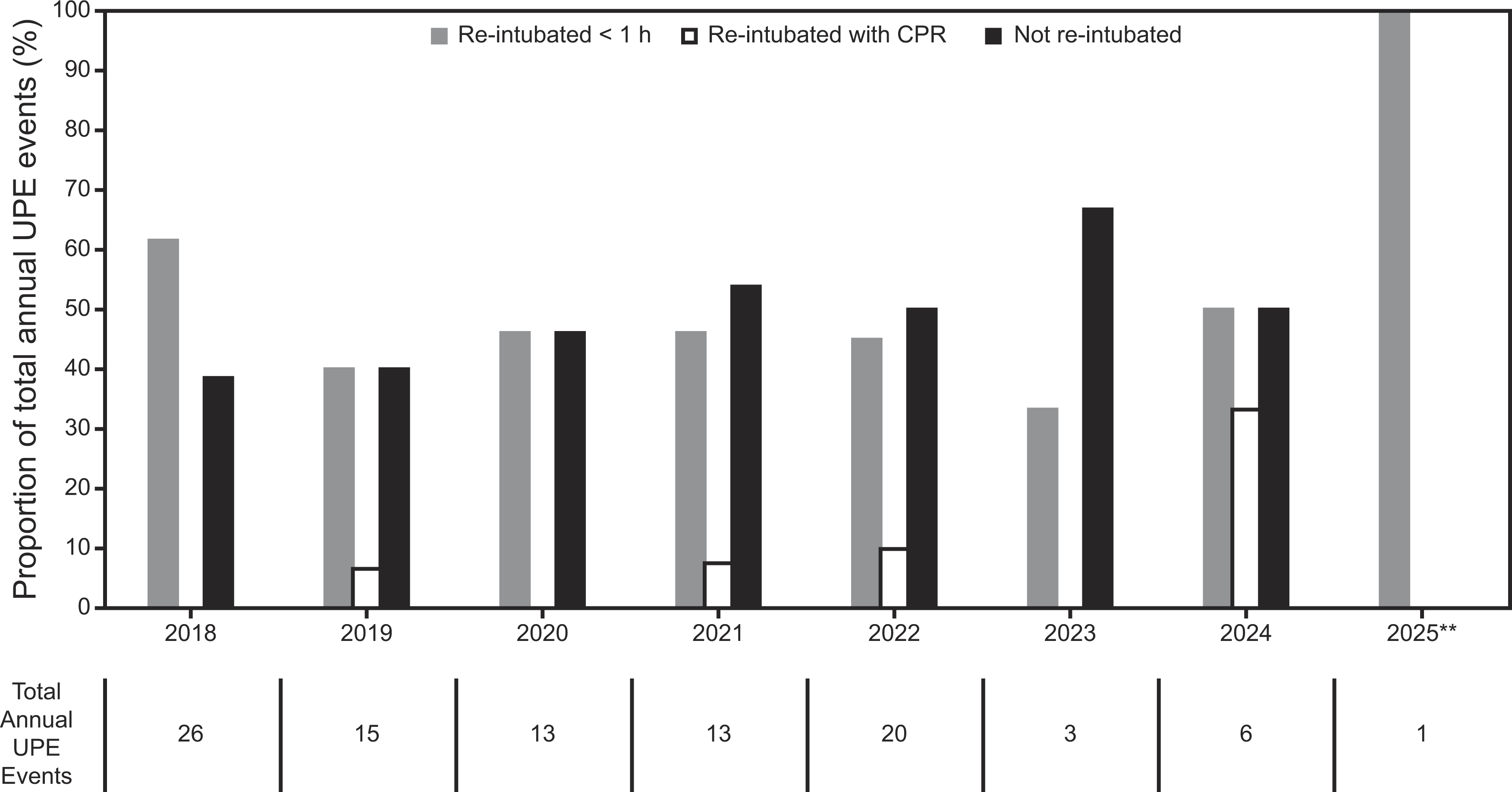
Annual outcomes following an unplanned extubation. CPR, cardiopulmonary resuscitation. **Q1 and Q2 only.
The results of adherence audits with the SPS UPE prevention bundle are shown in Figure 3. An upward center line to 100% adherence occurred in the first quarter of 2021. Leading up to and following “The 3 Rights” intervention, chart audits were performed to identify discrepancies in nurse and RT documentation on ETT position. This is shown as a U-statistical process control chart in Supplementary Figure S4. There was a mean of 20% discrepancies across the periods analyzed and criteria for a center line shift were not met. However, there was a general trend toward fewer discrepancies with six of the last eight months below the center line. Figure 4 shows the percentage of ETT rounding events where a just-in-time intervention (eg, tube re-taping) was performed. At the start of ETT rounds, interventions were performed 18% of the time. In the second quarter of 2023, there was a downward shift in the center line to 7% (a relative 61.1% drop). Finally, attendance at the first Airway Days was as follows: 47% (8/17) for physicians, 75% (3/4) for nurse practitioners, 92% (23/25) for RTs, and 98% (111/113) for nurses.
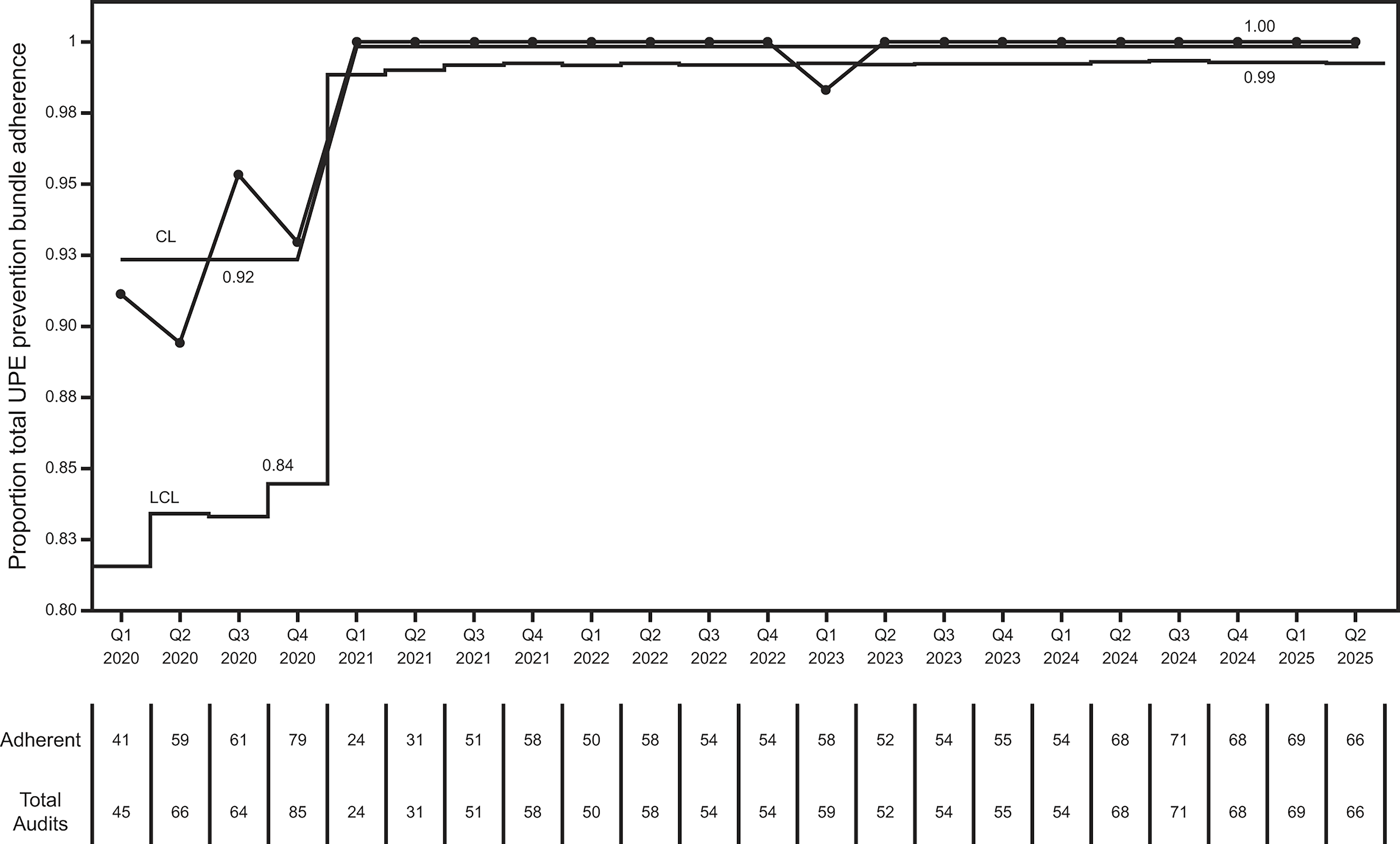
U-statistical process control chart showing total Solutions for Patient Safety unplanned extubation prevention bundle adherence over time based on audits.
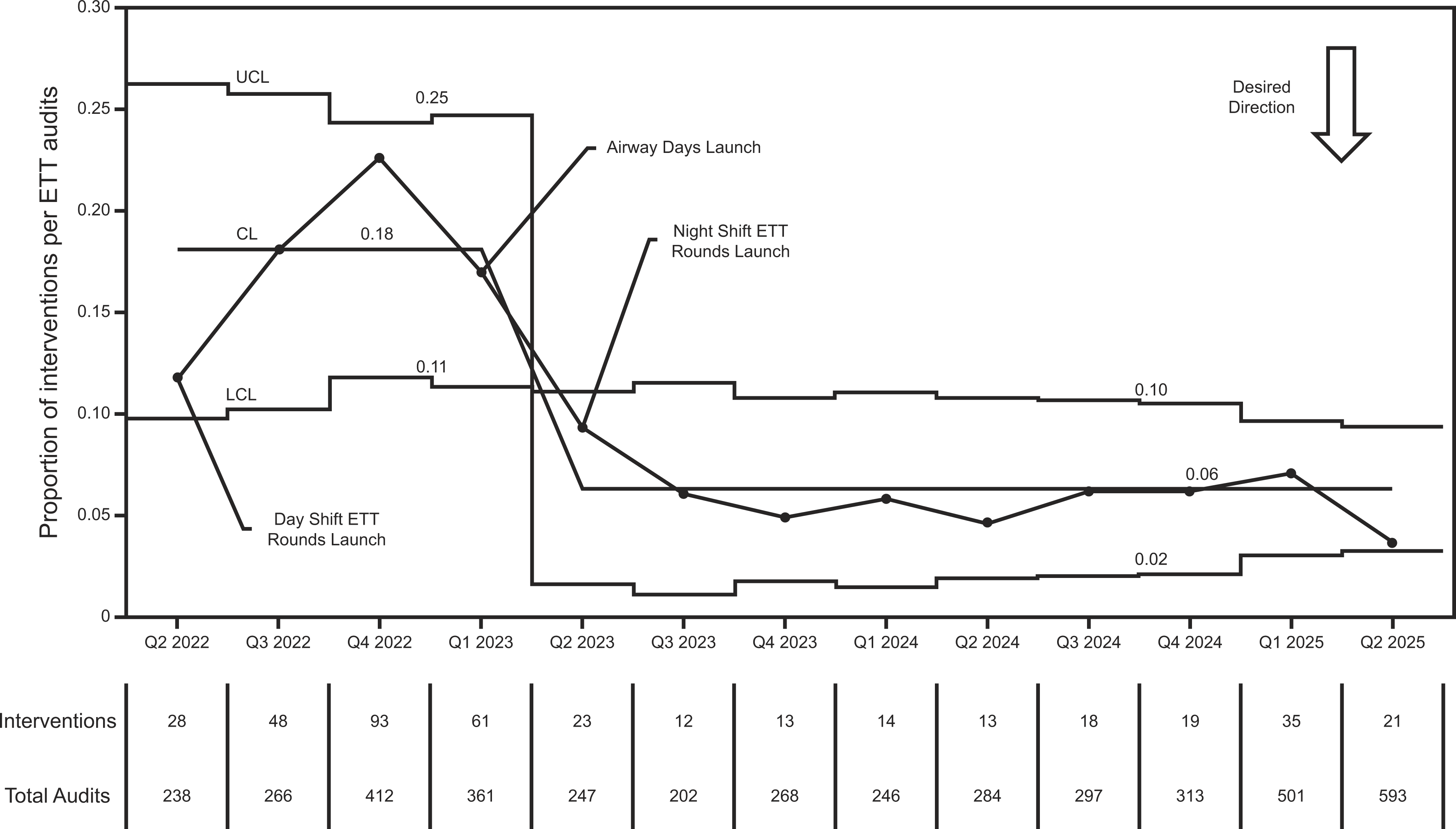
U-statistical process control chart showing total interventions as a percentage of total ETT rounds over time. ETT, endotracheal tube.
Discussion
Through multiple interventions driven by an embedded PICU QI RT, we surpassed our SMART (specific, measurable, actionable/attainable, relevant, time bound) aim goal of decreasing the UE/100 invasive ventilation days by 50%. We observed a decrease of 72.5% that has been sustained from the first quarter of 2023 through the second quarter of 2025. There was no discernable change in adverse re-intubation outcomes for subjects experiencing a UE. Process measures for each intervention generally demonstrated improvement over the course of each intervention. Interestingly, the improvement in the primary outcome was associated with a decrease in the percentage of subjects exposed to invasive ventilation, but no change in average invasive ventilation duration.
When the SPS UE prevention bundle was implemented in our PICU, our center line (0.58 UE/100 invasive ventilation days) was nearly the same as that reported by the national collaborative (0.52 UE/100 invasive ventilation days). Direct observation audits revealed sustained 100% adherence with the bundle by the first quarter of 2021. However, improvement in our UE rate required two years and additional interventions. This experience suggests that the SPS UE prevention bundle is a strong foundation, but additional efforts are needed for further improvement.
While the interventions themselves are important, we hypothesize that a key driver of improvement was the consistent vigilance of the embedded QI RT as a champion for improvement. Indeed, there is evidence that clinical champions increase adoption of best practices and innovations.13–16 A 2015 case-control study found a $36,692 increase in health care costs associated with each pediatric UE event. 6 It stands to reason that costs have only risen in the decade since. As such, an investment in a dedicated QI RT may yield significant return on investment for health care organizations. However, no formal cost-effectiveness evaluation was undertaken as part of this work.
While mean invasive ventilation duration was stable throughout the project, the percentage of subjects exposed to invasive ventilation decreased significantly. This was noted around the time when the pandemic started and persisted after its end. While the pandemic may have influenced intubation practice, there has also been a national trend toward using less invasive ventilation and more noninvasive ventilation or high-flow nasal cannula in pediatrics.17–19 At the same time, the U.S. PICU population is becoming more chronic and complex. 20 These factors may have changed the epidemiology of patients receiving invasive mechanical ventilation at our center. In turn, this could have lowered overall risk of a UE occurring and confounded the results. There are no available data to suggest this same trend is occurring nationally at this time, although the possibility cannot be excluded.
In parallel to the UPE QI interventions, there were concurrent ventilator liberation interventions. Importantly, this was a recommended element of the original SPS UE prevention bundle. The first included RT-driven extubation readiness eligibility screening and testing with a standardized spontaneous breathing trial.9,11 This could have contributed to the decline in UE rates observed by standardizing planned extubation processes and timing. The second included the implementation of a benzodiazepine-sparing analgosedation clinical pathway for invasively ventilated patients. 10 While there was no change in delirium rates during that project, it is possible that rates changed following the analysis period through the marked reduction in benzodiazepine exposure demonstrated. In addition, there could have been a change in sub-clinical (eg, not treated pharmacologically) delirium. Less delirium logically could translate to less risk of patient-caused UE, but evidence is lacking and any contribution is theoretical.
We did not have data on daily nurse and RT staffing ratios. Inappropriate staffing ratios are a known risk factor for UE. 21 While this is a limitation, our PICU maintains 1:1 nurse to patient ratios for most intubated patients and 1:2 ratios for others based on standard criteria. In addition, this work took place in a large, well-resourced center. This could limit generalizability to some centers. Future directions of this QI work are ongoing to ensure sustainability. Since the initial Airway Days, there has been significant staff turnover. Moreover, there was noted increase in ETT interventions during ETT Rounds in the first quarter of 2025. As a result, repeat Airway Days are ongoing to ensure competency of all bedside staff. Process adherence metrics are continuously followed and reviewed monthly at the unit QI meeting. Areas in need of further intervention to ensure sustainability will be identified and addressed through that vigilance system.
Conclusions
Through multiple QI interventions we achieved a decrease in the UE/100 invasive ventilation days rate of 72.5%. This has been sustained for over two years. These results support the importance of building upon the SPS Network prevention bundle and having a dedicated champion to drive improvement and sustainability. Finally, our experience suggests a potential significant return on investment for a dedicated QI RT in other similar PICUs.
Footnotes
Acknowledgments
The authors would like to thank all the nurses, respiratory therapists, prescribers, and other members of the multidisciplinary team in the PICU at Children’s of Alabama for their hard work and collaboration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.