
Abstract

Introduction
Home-care ventilators are vital for managing chronic respiratory failure in the growing population requiring long-term mechanical ventilation. Recent literature has revealed significant variability in ventilator performance, particularly regarding triggering function, pressurization capacity, and patient-ventilator synchronization. 1 Bench studies using lung models have become the standard methodology for evaluating the ventilator performance under controlled conditions. 2 These evaluations are crucial for matching ventilators to patient-specific clinical needs, rather than relying solely on manufacturer specifications. 3
Despite extensive research, a critical gap exists in the accuracy of tidal volume delivery. Although previous studies have evaluated triggering, pressurization, and synchronization, 4 limited attention has been paid to the accuracy of the delivered tidal volume across models. This gap is concerning because accurate tidal volume delivery is fundamental for effective therapy and patient safety. 5 Reliance solely on the manufacturer specifications may lead to suboptimal ventilator selection. 6 Two critical dimensions require investigation: the variability among different home-care ventilator models with identical settings and how each home-care ventilator’s performance changes under different compliance and airway resistance conditions. Understanding these discrepancies is essential to optimize ventilation strategies and prevent complications.
The purpose of this study was to evaluate the performance of six commercially available home-care ventilators by measuring the discrepancies between the set and actual measured tidal volumes under varying compliance and airway resistance conditions. This study provides evidence-based data to guide home-care ventilator selection based on patient-specific respiratory mechanics.
Methods
Home-care ventilators and breathing circuits
The following six home-care ventilators were evaluated in this study: Trilogy Evo (Philips, Pittsburgh, PA), Vivo45LS (Breas Medical, San Diego, CA), ASTRAL150 (ResMed, San Diego, CA), EO-150 (EOVE, Air Liquide, France), LUISA (Löwenstein Medical), Germany, and prismaVENT50-C (Löwenstein Medical, Germany). For all home-care ventilators, except ASTRAL150, the IS active dispo circuit (model: 5191175, Intersurgical) was used. ASTRAL150 was tested with its dedicated ResMed expiratory valve flex circuit (22-mm Astral).
Experimental setup and test conditions
A bench test was conducted using a SmartLung Adult test lung (IMT Analytics, Buchs, Switzerland). Home-care ventilators were configured to operate in volume control mode with the following settings: tidal volumes of 300 and 500 mL, a respiratory rate of 12 breaths/min, and an inspiratory time of 1.0 s. The ventilators delivered a decelerating wave inspiratory flow, and the rate was automatically calculated by the device based on the set volume and inspiratory time. The inspiratory trigger was turned off. For all ventilators, the circuit compliance compensation feature was activated, and alarm settings were either turned off or set to their widest limits to prevent interference with measurements. However, the prismaVENT50-C, which lacks a volume control mode, was set to a pressure-controlled ventilation mode that targets a specific tidal volume, with the maximum inspiratory pressure adjusted to its upper limit.
To assess how the ventilators’ tidal volume delivery responds to deteriorating respiratory mechanics, a change in compliance from 30 mL/cm H2O to 10 mL/cm H2O and a change in airway resistance from 5 to 20 cm H2O/L/s were simulated using the available settings on the test lung. The compliance value of 10 mL/cm H2O was intentionally chosen to create a challenging, worst-case scenario, to stress-test the stability of each ventilator’s volume delivery algorithm. These settings resulted in three combinations of respiratory mechanics that were tested: C30R5 (compliance 30 mL/cm H2O, resistance 5 cm H2O/L/s), C30R20, and C10R5.
All measurements were performed using a PF-301 flow analyzer (IMT Analytics) positioned in the respiratory circuit to accurately measure the actual inspiratory tidal volumes. All tidal volumes were measured to BTPS (body temperature, ambient pressure, saturated with water vapor). For each test condition, data were collected for 10 min; the measured tidal volume represents the mean value of all breaths recorded during this period. Breath-to-breath stability is reported as the standard deviation of these breaths. The entire experiment was conducted in a temperature- and humidity-controlled environment.
Statistical analysis
Statistical analyses were performed using R version 4.2.2. All data are presented as mean ± standard deviation. To compare the performance of the six ventilators under each specific test condition, a one-way ANOVA was performed. When a significant difference was detected, the Tukey–Kramer test was used for post hoc pairwise comparisons. To evaluate the influence of changing respiratory mechanics for each individual ventilator, the measured tidal volumes across the three conditions (C30R5, C30R20, and C10R5) were compared using a one-way ANOVA followed by the Tukey–Kramer test. A two-tailed P value < .05 was considered statistically significant for all analyses. It should be noted that all statistical comparisons of performance were made between the mean measured tidal volumes themselves, not between the calculated discrepancy values from the setpoint.
Results
Home-care ventilator performance at different tidal volume settings
Discrepancies between the set values and measured tidal volumes were observed across all home-care ventilators (Fig. 1). At the baseline 500 mL setting (C30R5), the Trilogy Evo and EO-150 had actual measured volumes that were substantially higher than the set values, with mean deviations of +41.6 mL (+8.3%) and +35.9 mL (+7.2%), respectively. In contrast, other ventilators, such as the Vivo45LS and ASTRAL150, under-delivered by −16.2 mL (−3.2%) and −14.1 mL (−2.8%), respectively.
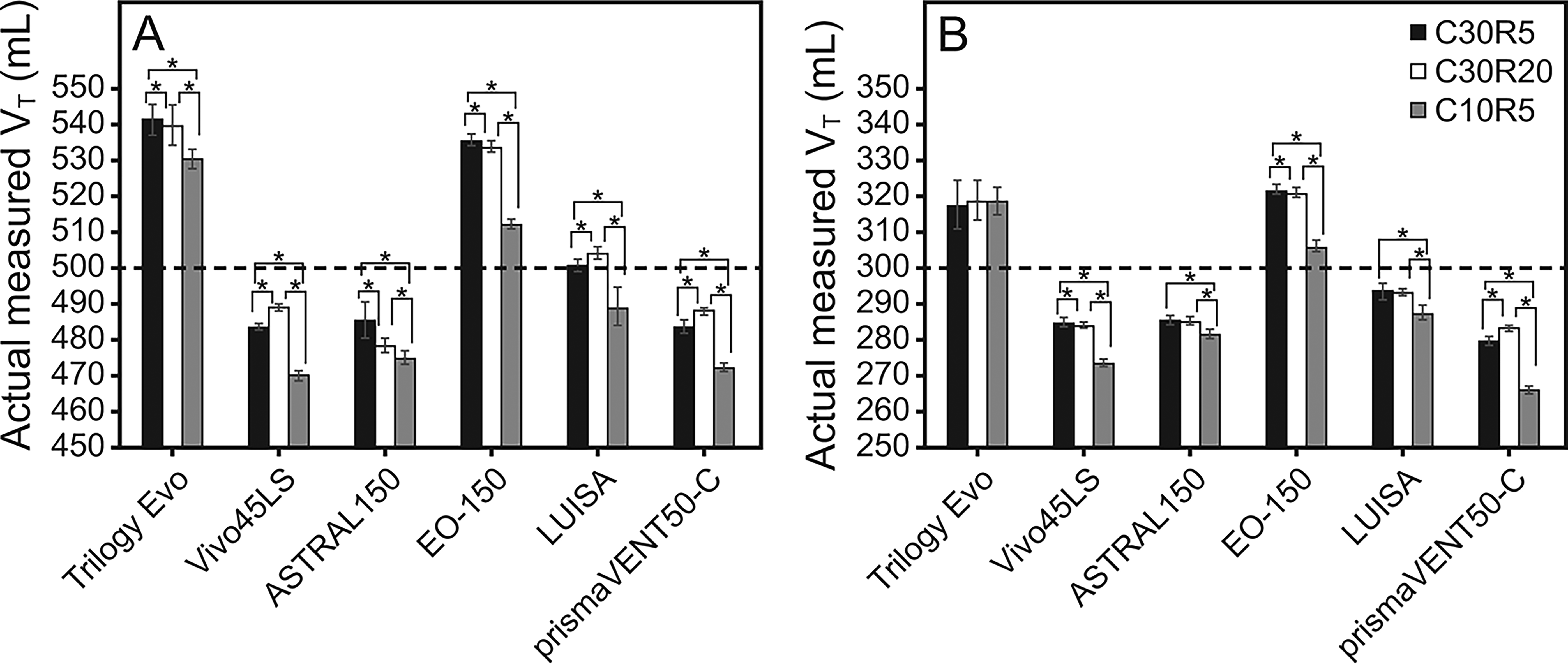
Comparison of actual measured tidal volumes across 6 home-care ventilators at set tidal volumes of
A similar pattern of over- and under-delivery was observed at the 300 mL setting (C30R5), where the Trilogy Evo and EO-150 over-delivered by +18.0 mL (+6.0%) and +22.2 mL (+7.4%), respectively, while the prismaVENT50-C under-delivered by −19.6 mL (−6.5%).
Breath-to-breath stability also varied, with standard deviations under C30R5 ranging from 0.9 mL (Vivo45LS) to 4.8 mL (ASTRAL150) at the 500 mL setting. One-way ANOVA identified significant differences between the home-care ventilator models at both tidal volume settings (P < .05).
Effects of compliance and airway resistance on actual measured tidal volumes
Changes in compliance had a more substantial impact on the delivered tidal volume than the changes in airway resistance (Fig. 2). For example, when compliance was reduced (C10R5 condition) at the 300 mL setting, under-delivery worsened for several ventilators, most notably for the prismaVENT50-C, where the discrepancy increased to −33.3 mL (−11.1% of set VT). In contrast, increasing airway resistance (C30R20 condition) produced more modest effects, although the ASTRAL150’s delivered volume decreased by 7.4 mL at the 500 mL setting when resistance was increased.
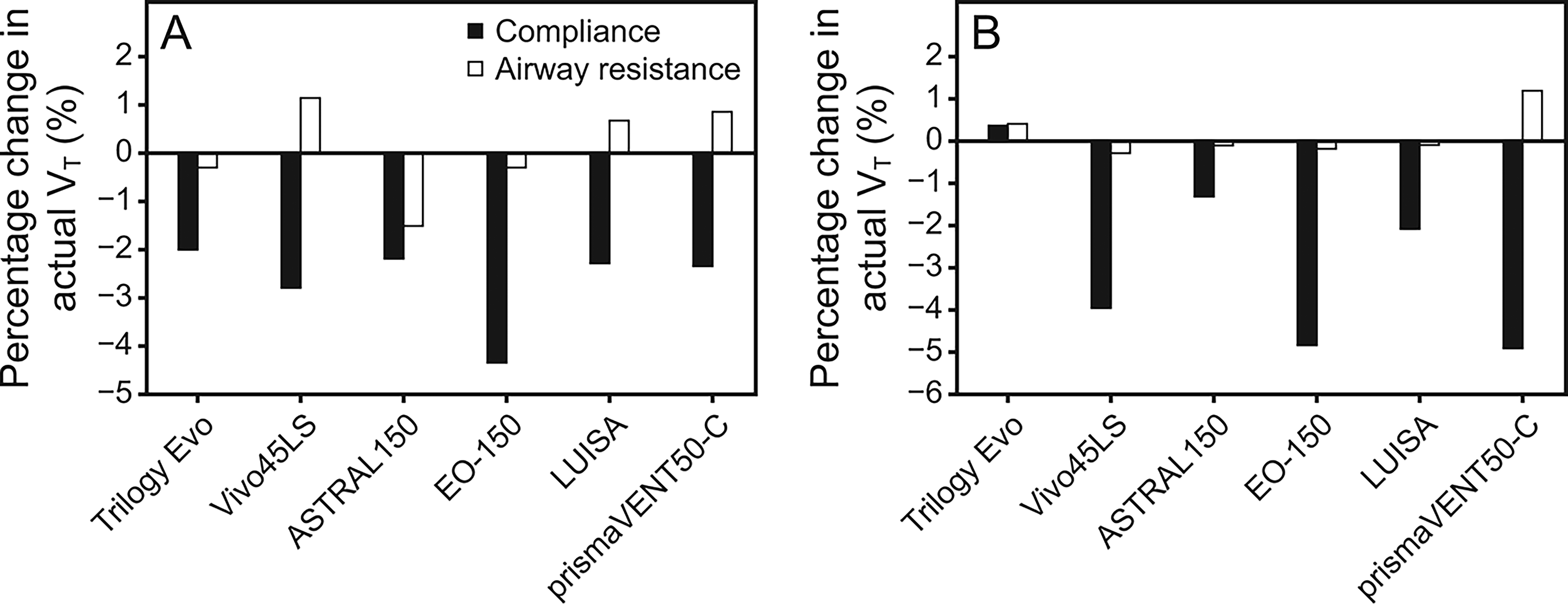
Effect of compliance reduction and increase in airway resistance on actual measured tidal volumes at a set tidal volume of
Discussion
This study revealed two significant findings. First, consistent, model-specific discrepancies exist between the set and actual measured tidal volumes, with some ventilators consistently delivering higher volumes while others delivered lower volumes. Second, changes in compliance had a greater impact on the actual measured tidal volumes than did changes in airway resistance.
The first main finding revealed discrepancies between set and measured tidal volumes across all ventilators. This finding aligns with research by Martínez-Castro et al 1 and suggests the observed patterns arise from differing manufacturer algorithms. Although the breath-to-breath variability was small, Chen et al demonstrated that even minor variations can impact gas exchange in patients with limited respiratory reserve, 7 a crucial consideration in unmonitored home-care settings. These findings highlight the importance of matching home-care ventilators to the respiratory needs of individual patients.
The second main finding highlighted that compliance changes had a more substantial impact on actual measured tidal volumes than did airway resistance changes. In this study, the reduction in compliance from 30 to 10 mL/cm H2O caused decreases in actual measured tidal volumes ranging from −2.0% to −4.9% across different home-care ventilators, with EO-150 and prismaVENT50-C demonstrating the greatest sensitivity to compliance changes. In contrast, changes in airway resistance produced modest effects (ranging from −1.5% to +1.2%). This observation is consistent with prior research showing that ventilator performance varies with respiratory mechanics. 3 Interestingly, Delgado et al demonstrated similar differential responses among ventilators when exposed to changing lung mechanics, suggesting that these variations reflect fundamental differences in ventilator design and algorithms. 8 The practical implications of this finding are significant for home-care patients with variable lung compliance, such as those with neuromuscular disorders, obesity hypoventilation syndrome, or pulmonary fibrosis, who might experience clinically important changes in ventilation based on their underlying condition and the specific home-care ventilator model used.
These findings underscore that clinicians should consider both patient respiratory mechanics and specific home-care ventilator performance characteristics when selecting them for patients. For instance, in patients with changing lung compliance, the Trilogy Evo demonstrated the most consistent ventilation across varying compliance levels. For patients requiring precise ventilatory control, the Vivo45LS demonstrated the most stable breath-to-breath performance. Such device-specific characteristics are crucial for personalizing ventilator selection as the population requiring home-care ventilation increases.
This study has some limitations. First, it tested only a single unit of each home-care ventilator model, which precluded an assessment of inter-unit variability in performance. Second, this bench study utilized a passive lung model and did not simulate patient inspiratory effort. Future studies using dynamic lung models are warranted to investigate performance during simulated patient–ventilator interactions. Third, the study examined only volume-controlled ventilation in a simulated environment, which may not fully represent the complex and dynamic conditions encountered in actual patients. Finally, only a limited range of compliance and resistance combinations were tested, while real-world patients may present more varied and extreme respiratory mechanics. Despite these limitations, this study provides valuable evidence on ventilator performance under standardized conditions to inform selection.
Author Disclosure of Interest
The author has no relationships to disclose.
Footnotes
Funding Information
No financial support was provided for this study.