
Abstract
Wildfires have become increasingly frequent and severe, releasing large amounts of fine particulate matter (PM2.5) and toxic gases that pose serious threats to respiratory health. This review summarizes current clinical evidence on the respiratory effects of wildfire smoke exposure, focusing on both short-term effects—such as respiratory symptoms, infections, and increased emergency department visits—and long-term consequences, including declines in pulmonary function and elevated mortality. The review highlights vulnerable populations—including pregnant individuals, infants, children, older adults, individuals with asthma or COPD, and firefighters, who experience disproportionate risks. It also compares the toxicity of wildfire-derived PM2.5 to other pollution sources and identifies differences in clinical impact. Evidence-based protective strategies are discussed, including respiratory protection, behavioral interventions, and health care provider preparedness. Finally, the review identifies gaps in the current literature and emphasizes the need for longitudinal studies to evaluate chronic outcomes and improve public health responses to future wildfire events.
Introduction
Wildfires release vast quantities of smoke containing fine particulate matter ≤2.5 µm (PM2.5) and toxic gases, which can travel hundreds or even thousands of miles. Breathing this smoke can irritate the respiratory tract and pose serious health risks, especially as wildfires become more frequent and intense because of climate change (Figs. 1 and 2).1,2 In recent years, epidemiological studies have documented both immediate (short-term) and persistent (long-term) respiratory health effects associated with wildfire smoke exposure.1–65 This literature review summarizes current knowledge on the respiratory impacts of wildfire smoke inhalation, with particular attention to vulnerable populations (including children, the elderly, individuals with preexisting respiratory conditions, pregnant individuals, and firefighters), and outlines public health recommendations and mitigation strategies.

Comparative skyline views of Chicago, IL under normal conditions and during wildfire smoke impact. The left panel shows reduced visibility and haze over downtown Chicago in June 2025 during a Canadian wildfire smoke event. The right figure shows the same view on a clear day in July 2024. Both images were taken from the same location under similar daylight conditions.
Progression of an approaching dust storm over a residential neighborhood, Chicago, Illinois (May 16, 2025). Sequential photographs taken from the same vantage point at (top) 18:43, (middle) 18:45, and (bottom) 18:49 local time illustrate the rapid reduction in horizontal visibility as the dust plume advanced across the area.
Literature Search Strategy and Results
A search of the published English literature was conducted in PubMed until January 24, 2025, using the following key words: (“wildfire smoke”[Title/Abstract] OR (“Smoke”[MeSH] AND “Wildfires”[MeSH])) AND (respiratory[Title/Abstract] OR pulmonary[Title/Abstract] OR lung*[Title/Abstract] OR trachea*[Title/Abstract] OR nose*[Title/Abstract] OR bronch*[Title/Abstract] OR alveol*[Title/Abstract] OR “Respiratory System”[MeSH] OR “Pulmonary Medicine”[MeSH]). The inclusion criteria were limited to clinical retrospective and prospective studies. A total of 187 articles were identified. Of these, 82 were excluded for not addressing the respiratory effects of wildfire smoke exposure. An additional 43 articles were excluded for the following reasons: inappropriate study design (13), animal studies (5), irrelevant outcome (24), and duplicate publication (1). Ultimately, 62 studies were included in the review.1–28,30–57,60–65
Among the included studies, 37 were conducted in the United States (Fig. 3a), with 17 specifically focused on California (Fig. 3b). Regarding study populations, over half examined adults, with 26% focusing on older adults, and approximately one-third addressed pediatric populations (Fig. 4a). Notably, most studies were published within the past decade, with a concentration between 2019 and 2024 (Fig. 4b).
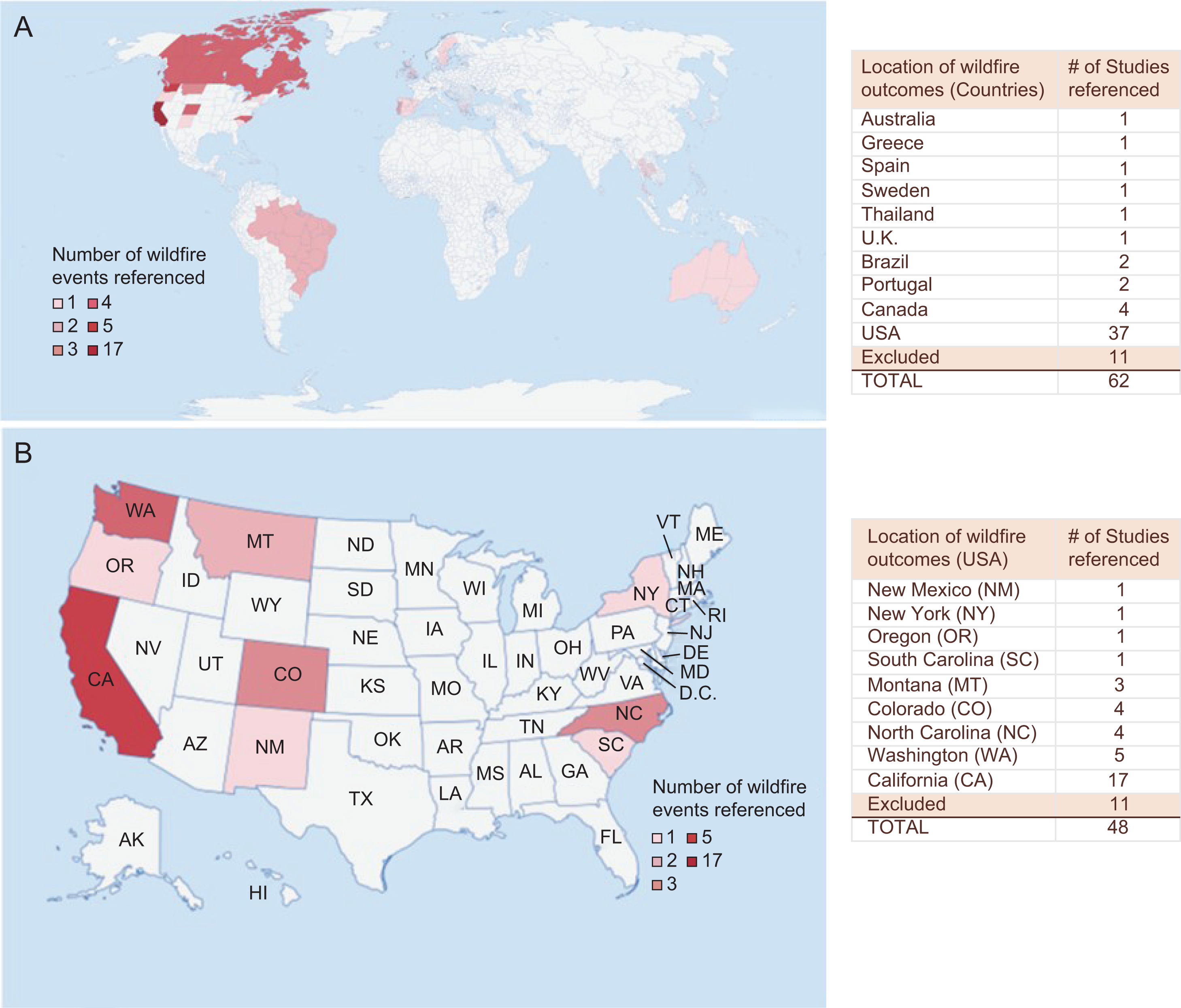
Geographic distribution of wildfire-related health outcome studies (global and United States).
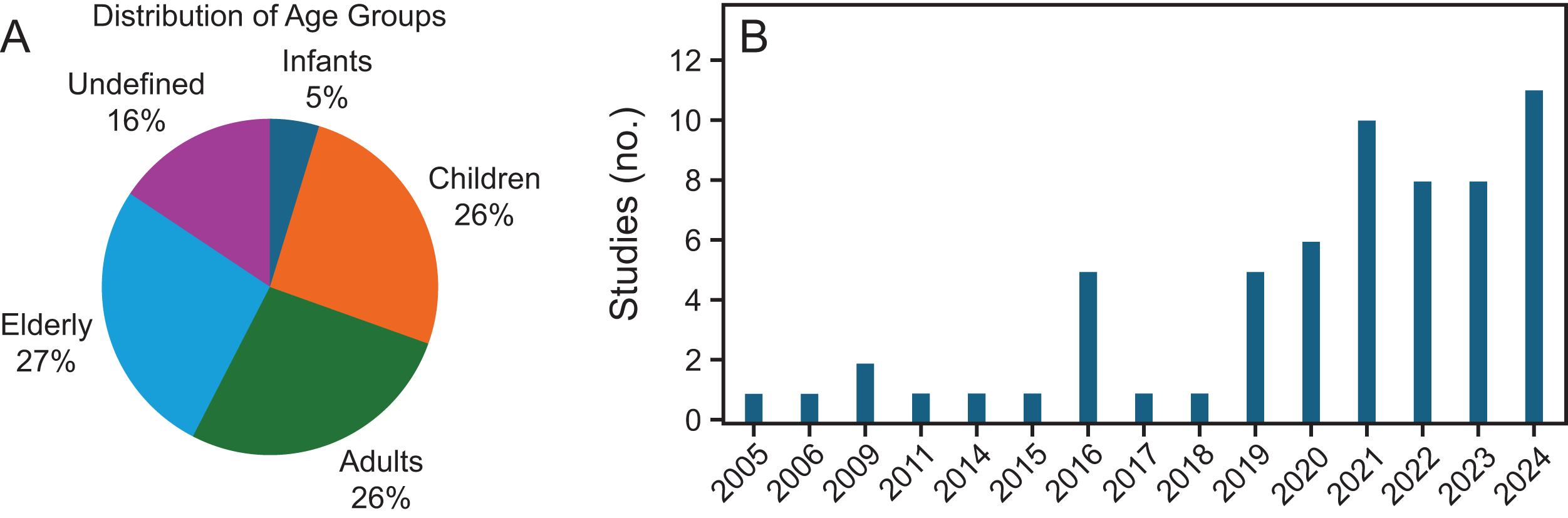
Characteristics of included studies by population age group and publication year.
Short-Term/Immediate Respiratory Effects
Respiratory symptoms: coughing and wheezing
Wildfire smoke, rich in fine particulate matter (PM2.5), can penetrate deep into the lungs, often triggering acute respiratory symptoms such as coughing and wheezing (Fig. 5). In a study following the 2003 Southern California wildfire, Künzli et al assessed respiratory symptoms in children using parent-reported questionnaires. They found increased reports of wheezing, dry and wet cough, bronchitis, and asthma attacks—especially among children exposed for 6 or more days. Notably, nonasthmatic children exhibited similar or stronger associations with wheezing compared to their asthmatic peers, 3 possibly because of higher baseline symptoms and more frequent medication use among children with asthma, which may attenuate symptom reporting. This finding underscores that wildfire smoke can induce significant respiratory symptoms even in healthy children without preexisting respiratory conditions. One limitation of this study is the high background rates of symptoms, which may have reduced the observed effect estimates among children with asthma.
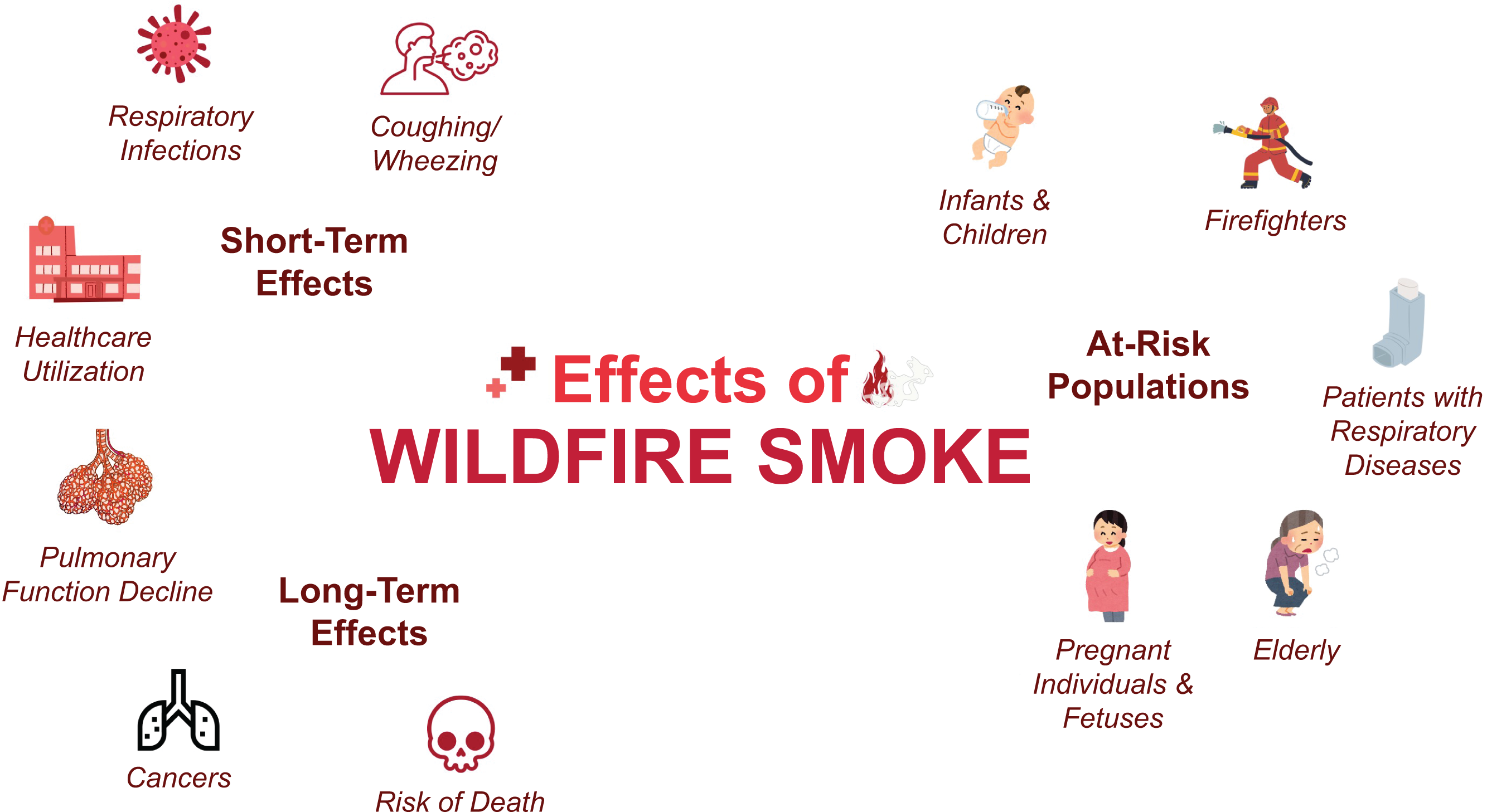
Overview of the health effects of wildfire smoke. This conceptual figure summarizes the health impacts of wildfire smoke, including short-term effects, long-term effects, and highlights populations at increased risk.
However, findings vary across studies. For instance, Vicedo-Cabrera et al examined children in Valencia, Spain, during the 2012 wildfires and found no significant association between wildfire smoke exposure and coughing. However, sore throat emerged as a significant symptom among children with asthma, though not in those without asthma, 4 potentially reflecting upper airway irritation. Since sore throat often co-occurs with coughing, it may serve as a more sensitive early indicator of early exposure. The study’s reliance on survey data also introduces the possibility of recall bias and symptom overreporting.
Respiratory infections
Exposure to wildfire smoke has been associated with increased risk of respiratory infections, particularly bronchitis and pneumonia. For instance, Rappold et al reported significant increases in emergency department (ED) visits for both acute bronchitis and pneumonia during wildfires in North Carolina. 5 Similarly, Mahsin et al found a relative risk (RR) of 2.11 (95% CI 1.86–2.40) for acute respiratory infections in Calgary, Canada, in the month following a 2015 wildfire. 6
Increase in health care utilization
Wildfire smoke exposure is strongly associated with an increase in health care utilization for respiratory conditions, particularly ED visits and hospitalizations (Tables 1 and 2).
Summary of wildfire events and associated health care utilization outcomes in the general population
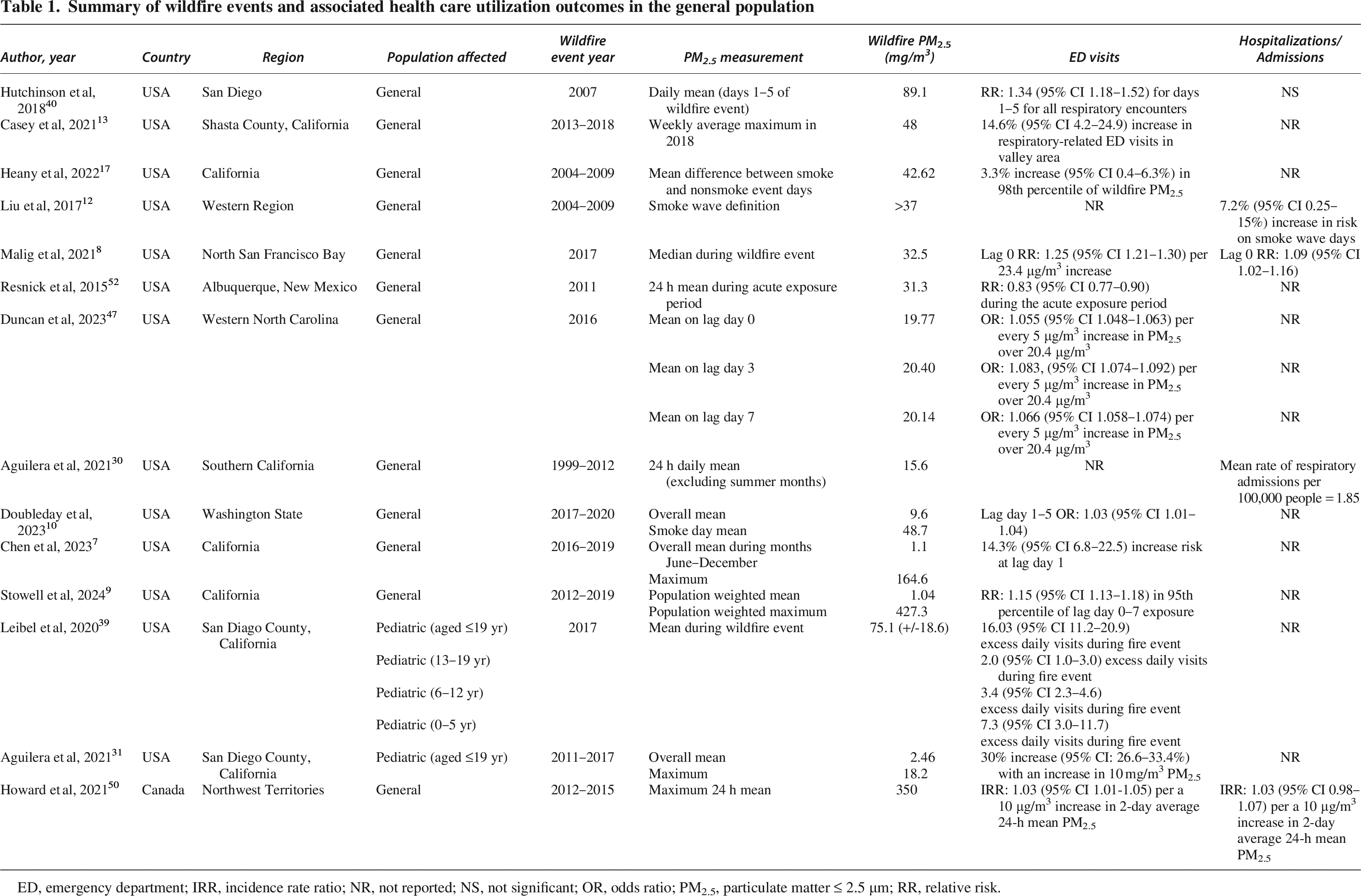
ED, emergency department; IRR, incidence rate ratio; NR, not reported; NS, not significant; OR, odds ratio; PM2.5, particulate matter ≤ 2.5 µm; RR, relative risk.
ED visits
Multiple studies have reported increases in respiratory-related ED visits during wildfire periods,7–9 with effects persisting up to 4 days postexposure. 10 Several investigators have also explored the dose-response relationship between wildfire-specific PM2.5 levels and ED visits, though findings remain mixed. For instance, Delfino et al’s study during the 2003 Southern California wildfires reported a 10.1% (95% CI 3.0–17.8%) rise in respiratory ED admissions per 10 µg/m³ increase in PM2.5 among adults aged 65–99. 11 In contrast, Liu et al found no significant association between “smoke wave” days (defined as PM2.5 > 37 µg/m³) and cardiopulmonary ED visits across the western United States from 2004 to 2009, though they did observe a 7.2% increase in respiratory visits (95% CI 0.25–15%). 12 This discrepancy may stem from differing exposure metrics—for example, cumulative smoke wave thresholds versus incremental PM2.5 increases—and regional variation in pollutant sources. Likewise, Casey et al found no correlation between wildfire PM2.5 and countywide ED visits in Shasta County, California. Yet, a subregional analysis focusing on the lower-elevation valley area revealed a 14.6% increase in respiratory-related ED visits (95% CI 4.2–24.9) during the week with high-PM2.5 exposure. 13 These inconsistencies may reflect variations in geographic resolution, population density, baseline air quality, or the duration and intensity of exposure—factors that broader, regionwide studies may not fully capture.
Hospitalizations
Although ED visits represent the immediate health burden of wildfire smoke exposure, hospitalizations indicate more severe or prolonged respiratory compromise. Evidence increasingly supports a robust association between wildfire-specific PM2.5 and respiratory hospital admissions, with emerging insights into dose–response relationships, temporal patterns, and socioeconomic disparities. Large-scale epidemiologic studies further confirm the dose-dependent nature of this relationship. In a comprehensive Medicare-based analysis, Deflorio-Barker et al examined over 1 million respiratory-related hospitalizations across 692 United States counties affected by 123 wildfires between 2008 and 2010. They found that hospital admissions for asthma, bronchitis, and wheezing rose significantly when wildfire PM2.5 concentrations exceeded 5 µg/m³. 14 Similarly, Stowell et al reported that each 1 µg/m³ increase in wildfire-related PM2.5 was associated with an elevated risk of asthma hospitalizations (OR: 1.081, 95% CI 1.058–1.105). 15 Timing of exposure also plays a role: Many studies found that respiratory hospitalizations peak on the days of exposure or in the days following.8,16,17 Although another study reported the strongest associations between PM2.5 and respiratory diseases at 3 days post fire. 18 The longest lag days where associations were reported were up to 7–13 days after the fire.19,20 These findings highlight the need for extended surveillance and public health messaging that extends beyond the active fire period. However, one possible limitation in these studies is the inability to isolate wildfire-specific PM2.5 from other concurrent pollution sources during the fire period, which could bias estimates of exposure–response relationships.
Socioeconomic factors further compound the burden of wildfire smoke exposure. Reid et al found that ZIP Codes with lower median household incomes experienced higher rates of respiratory ED visits and hospitalizations for COPD and pneumonia during the 2008 California wildfires, with significant associations between PM2.5 and respiratory hospitalizations in these communities (P < .001).21,22 These disparities likely reflect limited access to clean air, health care, and adaptive resources.
In summary, hospitalization data reinforce the substantial and inequitable impacts of wildfire smoke exposure, particularly during sustained or high-concentration PM2.5 events. These findings underscore the need for real-time air quality monitoring, enhanced hospital preparedness, and targeted public health interventions during and after wildfire episodes.
Long-Term Effects
Declines in pulmonary function
Long-term exposure to wildfire smoke, particularly increased PM2.5 levels, has been associated with measurable declines in pulmonary function. Blando et al observed a significant reduction in peak expiratory flow (PEF) among 842 asthma-related patient visits at an allergy clinic 1 year after the 2008 and 2011 wildfire events. 23 Likewise, Orr et al reported significant declines in the FEV1 and the ratio of FEV1 to FVC, with FEV1 values falling below the lower limit of normal at both 1- and 2-year follow-ups, suggesting potential progression toward obstructive lung disease. Interestingly, PEF did not significantly change in the Orr study, likely because of differences in the populations studied. 24 Blando et al’s cohort consists of subjects with preexisting respiratory conditions, whereas Orr et al studied the general community population. Despite these differences, both studies suggest that wildfire smoke exposure may contribute to long-term declines in pulmonary function. Another aspect to consider is the development of restrictive lung diseases as studied by Kronzer et al. They found that each 1 µg/m3 increase in PM2.5 was associated with nearly double the odds of developing rheumatoid arthritis–associated interstitial lung disease (adjusted OR: 1.98 [95% CI 1.08–3.62]). However, this study was limited to a veteran population, which may reduce generalizability because of overrepresentation of men and higher smoking prevalence. 25
Recognizing the limitations of existing data, several initiatives have aimed to address the need for robust longitudinal research. One example is the ongoing L.A. Fire HEALTH Study, 66 a large, multi-institutional collaboration designed to investigate the long-term cardiopulmonary and systemic health effects of wildfire smoke exposure among Los Angeles residents. This study may provide more definitive evidence regarding chronic outcomes.
Increased risk of death
The health impacts of wildfire smoke extend beyond morbidity to include mortality. During the 2020 Washington wildfires, Liu et al reported that elevated PM2.5 levels were associated with increases in weekly all-cause mortality (87.6 cases, 95% CI 70.9–103.1), cardiovascular-related deaths (19.1 cases, 95% CI 10.0–28.2), and respiratory-related deaths (9.4 cases, 95% CI 5.1–13.5). 26 The authors conducted a model analysis and reported that a mean of 3.5 ± 1.4 µg/m3 rise in annual PM2.5 levels was associated with a 1.8% (95% CI 1.2–2.6) increase in all-cause mortality and a 4.3% (95% CI 3.1–5.4) increase in cardiorespiratory deaths. 27 Furthermore, Doubleday et al examined the wildfire smoke exposure in Washington from 2006 to 2017 and revealed a 1.3% (95% CI 0.2–2.4%) increase in mortality the day after wildfire smoke exposure, with same-day respiratory mortality increasing by 9.0% (95% CI 0.0–18.0%) and COPD-specific deaths by 14.0% (95% CI 2.0–26.0%). 28 However, a major limitation across these studies is the reliance on generalized or modeled PM2.5 data, rather than direct measurement of wildfire-specific PM constituents. This introduces potential exposure misclassification and may dilute observed associations. Collectively, these studies affirm that wildfire smoke—especially PM2.5—contributes to elevated mortality from both acute and chronic causes.
Differences in Respiratory Health Impact Between Wildfire and Nonwildfire Smoke
A growing body of literature suggests that wildfire-derived PM2.5 may exert greater toxicity than ambient PM2.5 from nonwildfire sources. This distinction is increasingly supported by both epidemiologic data and toxicological studies, which highlight the unique chemical composition and biological reactivity of wildfire emissions. In addition to fine particulate matter, wildfire smoke contains a complex mixture of volatile organic compounds, polycyclic aromatic hydrocarbons, and combustion byproducts, many of which possess high oxidative potential and pro-inflammatory properties. 29
Epidemiologic evidence supports this distinction. Aguilera et al demonstrated that wildfire-specific PM2.5 was more strongly associated with respiratory-related hospital admissions than nonwildfire PM2.5, implicating the distinct composition of wildfire emissions as a critical factor in health risk. 30 Similarly, in a pediatric-focused study, the proportion of asthma-related ED visits rose sharply when exposure was attributable to wildfire smoke, rising from 3.7% with nonsmoke PM2.5 to 30.0% with wildfire-specific PM2.5. 31 However, a key limitation of this study is the lack of individual-level data, which precluded a sensitivity analysis to account for possible repeated visits by the same patients. Additional findings from Stowell et al indicate that wildfire-derived PM2.5 had a stronger association with acute respiratory outcomes—including ED visits—compared with PM2.5 from other ambient sources. 15
The long-term health risks also appear to differ. In a study conducted in Brazil, Yu et al observed that wildfire-related PM2.5 exposure was significantly associated with higher cancer-related mortality compared with nonwildfire PM2.5 (P = .003), with increased deaths from cancers of the nasopharynx, esophagus, stomach, colon/rectum, larynx, skin, breast, prostate, and testis. Interestingly, no significant association with lung cancer was observed. 32 Although not accounting for gaseous pollutants, these findings raise concern about the potential for long-term systemic toxicity from wildfire-specific pollutants. Collectively, these findings reinforce the heightened toxicity of wildfire smoke and emphasize the need for differentiated risk assessments and public health responses based on pollution sources.
Vulnerable populations
Although wildfire smoke exposure can adversely affect individuals across all demographics, certain groups experience disproportionate risk because of developmental, physiological, or environmental vulnerabilities. This section synthesizes evidence on differential susceptibility across life stages, health conditions, and occupational settings.
Pregnant individuals and fetuses
Respiratory development begins early in gestation and continues into early adulthood, making each developmental stage uniquely vulnerable to wildfire smoke. Exposure during early pregnancy may impair placental function, whereas exposure later in gestation may interfere with fetal lung maturation.33–35
In Brazil, Requia et al found that second-trimester wildfire smoke exposure was associated with increased odds of cleft lip/palate (OR: 1.007, 95% CI 1.001–1.013) and congenital respiratory abnormalities (OR: 1.013, 95% CI 1.002–1.023). First trimester exposure was linked to congenital nervous system abnormalities (OR: 1.002, 95% CI 1.001–1.003), particularly in certain geographic regions. 35 However, this study may underestimate the true effects because of live-birth bias, as they excluded miscarriages and stillbirths potentially linked to wildfire smoke exposure. Lan et al reported that every 10 µg/m³ increase in PM2.5 during gestation heightened the risk of early-life health issues. Specifically, exposure during weeks 19–28 (when the eustachian tube develops) increased odds of otitis media (OR: 1.31, 95% CI 1.22–1.41), whereas exposure during weeks 18–27 (critical for lower respiratory tract development) raised the risk of lower respiratory infections (OR: 1.21, 95% CI 1.15–1.28). 36 One important limitation of this study is the absence of adjustments for environmental tobacco smoke exposure and maternal stress, both of which could confound the observed associations.
Studies using medication usage as a proxy for long-term respiratory outcomes further support this risk. In a 3-year cohort study of 35,065 full-term individuals, Jardel et al found that exposure during the first 12 postnatal weeks was associated with increased use of lower respiratory tract medications (OR: 1.21, 95% CI 1.05–1.40, respectively). 33 Similarly, Dhingra et al observed that although prenatal exposure to wildfire smoke delayed the initial use of respiratory medications, postnatal exposure during the first 12 weeks of life accelerated it—especially for upper respiratory medication, with a hazard ratio of 1.094 (95% CI 1.005–1.191) for weeks 0–12 and 1.108 (95% CI 1.016–1.209) for weeks 13–24. 34 However, these studies are limited by potential medication noncompliance and dataset constraints—particularly in Dhingra’s study, which used nonrural, private insurance claims, limiting generalizability.
Supplementing this finding, Haikerwal et al found that individuals born extremely preterm (<28 weeks) or with extremely low birthweight (<1,000 g) were more vulnerable to lower respiratory infections and adverse respiratory health outcomes in early adulthood following wildfire smoke exposure. Still, these findings are based on a small sample size (n = 73) who completed the health survey, limiting statistical power. 37 The existing evidence supports protecting pregnant individuals from wildfire smoke exposure throughout gestation, especially during periods of critical organ development. Further research that includes comprehensive gestational outcomes and adjusts for key confounders is needed to clarify the full scope of risk.
Infants and children
Young children remain highly susceptible to the adverse respiratory effects of wildfire smoke because of their developing lungs, higher ventilation rates, and smaller airways. 38 PM2.5 deposit in children’s lungs rates up to 35% higher than in adults, 39 increasing the risk of lung injury through mechanisms such as oxidative stress and inflammation.
In Southern California, Delfino et al reported an 8.3% increase in asthma-related hospital admissions among children aged 0–4 years during the 2003 wildfires, though no such association was observed for children aged 5–18 years in the postfire period. 11 However, the statistical power for age-stratified outcomes may have been limited, potentially masking effects in older children. Similarly, Hutchinson et al found a 70% increase in ED visits for respiratory diagnoses among children aged 0–4 years, including a 243% spike in asthma diagnoses in infants under 1 during the 2007 wildfires. 40 However, the use of Medi-Cal data may limit generalizability, as it predominantly represents low-income populations, though it may also highlight some of the most at-risk groups. Similarly, Leibel et al observed that during the 2017 Lilac Fire, in San Diego County, California, children aged 0–5 years had the highest daily excess asthma-related ED visits (7.3 visits, 95% CI 3.0–11.7), whereas those aged 6–12 years had the greatest overall increase in visit numbers (3.4 visits, 95% CI 2.3–4.6). 39 Unlike the other 2 studies, this analysis focused on a single wildfire event, limiting its generalizability across broader exposure scenarios.
Outside the United States, similar patterns have been observed. In Calgary, Canada, Mahsin et al reported a 55% increase in pediatric respiratory morbidity (95% CI 42–69%) per 10 µg/m3 rise in PM2.5 during the month following the 2015 wildfires. Children aged 0–9 years were particularly affected, showing increased RR for asthma-related physician visits. 6 Taken together, the evidence underscores the substantial and consistent respiratory burden wildfire smoke imposes on children, with potential for both acute and long-term effects.
Individuals with asthma
Asthma is among the most consistently impacted conditions in wildfire smoke research and may serve as a sentinel indicator of respiratory stress in affected populations. Exposure to PM2.5, carbon monoxide (CO), and nitrogen dioxide (NO2) can trigger airway inflammation and bronchospasm, often leading to asthma exacerbations. In patients aged 12–21, FEV1 decreased after 1 day of smoke exposure as wildfire PM2.5 increased by 10 µg/m³. 41
Multiple studies across the United States have demonstrated increased asthma-related ED visits and hospitalizations during wildfire events (Table 2).5,15,42,43 Rappold et al, in a study of the 2008 North Carolina wildfire, found that asthma exacerbations accounted for 44% of wildfire-related respiratory ED visits, with a cumulative RR of 1.65 (95% CI 1.25–2.17) during a high-exposure period. 5 Gan et al reported that a 10 µg/m³ increase in PM2.5 was associated with an 8.9% increase in the odds of asthma-related ED admissions (OR: 1.089, 95% CI 1.043–1.136) during Oregon’s 2013 wildfire season. 42 Similarly, Stowell et al estimated that each 1 µg/m³ increase in PM2.5 was associated with an 8.1% increase in asthma-related ED/hospitalizations (OR: 1.081, 95% CI 1.058–1.105). 15
Summary of wildfire events and associated health care utilization outcomes in patients with chronic lung disease
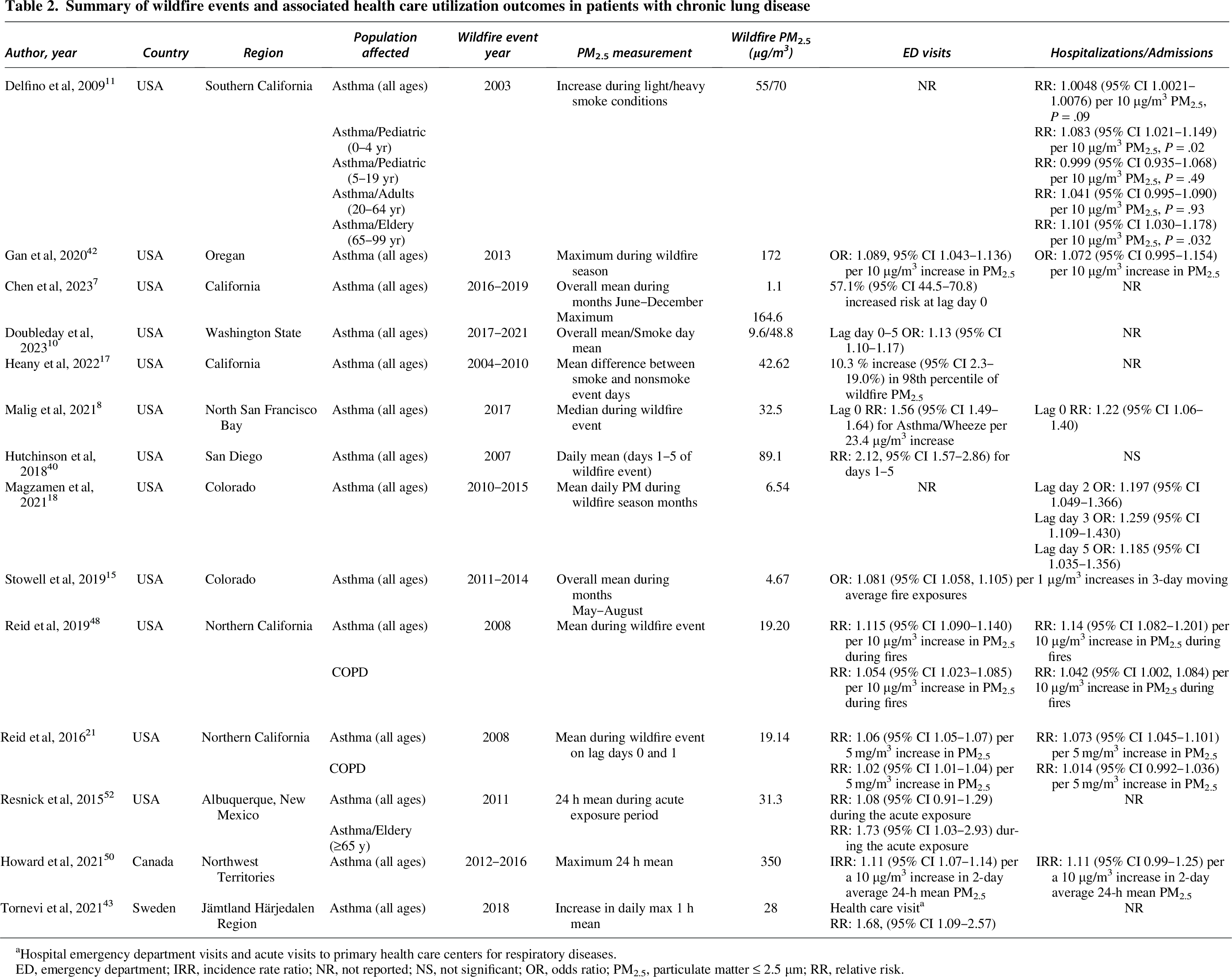
Hospital emergency department visits and acute visits to primary health care centers for respiratory diseases.
ED, emergency department; IRR, incidence rate ratio; NR, not reported; NS, not significant; OR, odds ratio; PM2.5, particulate matter ≤ 2.5 µm; RR, relative risk.
These results were also reinforced in international studies. In Sweden, Tornevi et al observed elevated risks of asthma diagnoses (RR: 1.68, 95% CI 1.09–2.57) and lower airway conditions (RR: 1.4, 95% CI 1.01–1.92) during the 2018 wildfire event, with health care visits doubling in municipalities experiencing sustained PM2.5 concentrations ≥20 µg/m³. 43 However, one study showed contrasting results where asthma control improved in subjects aged 18–26 years with a decrease in air quality, potentially because of increased vigilance and better symptom management. 44 Depending on the study location, especially sparsely populated areas, data analysis was affected by misclassification of exposures and medical ICD codes. These findings underscore the critical need for asthma-specific action plans during wildfire seasons, including medication access, clean air shelters, and early-warning systems.
Individuals with COPD
COPD is another major respiratory condition exacerbated by wildfire smoke, particularly among older adults and those with preexisting comorbidities.45,46 Multiple studies have found an increase in COPD-related ED visits during wildfire events.47–49 During the 2008 wildfire in North Carolina, a cumulative RR of 1.73 (95% CI 1.06–2.83) was reported for COPD-related ED visits. 5 Delfino et al showed that COPD hospitalizations rose by 3.1% among older adults during the 2003 Southern California wildfires. 11 Sutherland et al found that symptom severity in COPD subjects increased significantly on high-pollution days, particularly when PM2.5, PM10, and CO levels were elevated. 49 However, regional differences persist. Howard et al found no significant association between PM2.5 and COPD-related ED visits in subarctic Indigenous communities, possibly reflecting differences in baseline health, access to care, or housing conditions. 50 Although COPD may be less sensitive than asthma to wildfire smoke on a population level, it remains a clinically important outcome—especially for older adults—and warrants targeted surveillance and mitigation strategies.
Older adults
Older adults face heightened susceptibility to wildfire smoke because of age-related declines in pulmonary function and immune response and the high prevalence of chronic respiratory diseases such as asthma, COPD, and cardiovascular disease. During the 2017 California wildfires, Cleland et al observed that patients over age 65 accounted for more than half of asthma- and respiratory-related hospital admissions, despite comprising only 14% of the entire population. 51 Resnick et al found that adults over 65 had a significantly increased risk of asthma ED visits (RR: 1.73, 95% CI 1.03–2.93). 52 Zheng et al reported that older adults with asthma exposed to wildfire smoke experienced persistent symptoms that interfered with sleep and mental health, suggesting prolonged effects beyond acute episodes. 53 Notably, none of these analyses adjusted for potential socioeconomic or behavioral confounders, which could influence access to health care, protective behaviors, or overall resilience to wildfire smoke.
Findings related to COPD in older adults further support this pattern. As discussed earlier, Delfino et al observed a notable increase in COPD hospitalizations among seniors during wildfire events. 11 However, some studies offer contrasting results. For example, Stowell et al found no significant association between PM2.5 exposure and respiratory hospitalizations in adults over 65, suggesting that factors such as protective behaviors, medication use, or baseline health status may modulate risk. 15 Taken together, these findings highlight the intersection of aging and chronic disease as a critical axis of vulnerability.
Occupational risk: firefighters
Occupational groups, especially wildland firefighters, face repeated and intense exposures to wildfire smoke, placing them at elevated risk for adverse respiratory outcomes. During wildfires, levels of PM2.5, NO2, and sulfur dioxide were found to surpass legislated occupational exposure thresholds. 54
Small cohort studies have demonstrated measurable physiologic changes following wildfire exposure. In a study involving 53 firefighters, Ramos et al reported that wildfire exposure for more than 48 h was significantly associated with the development of restrictive lung patterns—particularly in firefighters who lacked adequate respiratory protection. 55 Similarly, Moitra et al studying Canadian firefighters within 90 days post-occupational exposure to wildfire smoke, identified significant declines in residual volume (RV) and RV/total lung capacity ratios. 56 In Chiang Mai, Thailand, Panumasvivat et al followed 54 wildland firefighters over a fire season and reported significant declines in FVC, FVC% predicted, FEV1, and FEV1% predicted during the peak season. However, no significant pre- versus postseason lung function changes or DNA damages were detected, 57 possibly because of the relatively lower PM2.5 concentrations (highest: 95.82 ± 18.89 µg/m³), which were below those reported in studies that observed significant epigenetic changes.58,59 Likewise, Wu et al evaluated 12 healthy young wildland firefighters (mean age 33) from U.S. Forest Service and found only mild pulmonary responses following wildfire exposure—specifically, a marginal increase in the oxidative stress biomarker 8-isoprostane. These limited effects were likely attributable to exposure levels and durations that were over 40% lower than those reported in other studies. 60 Supporting the biological plausibility of these findings, Mylonaki et al found that the wildfire smoke had 1.5 times the oxidative potential of dust, implying increased respiratory health risks. 61
Although these small-sample studies report only mild declines in pulmonary function,54,56,57 these may underestimate true risk because of small-sample sizes and the “healthy worker effect”—in which those with better baseline fitness may both tolerate and remain in the profession, masking exposure-related impairments, especially early physiologic changes. This effect limits generalizability, particularly for longer serving or medically vulnerable personnel.
Beyond respiratory effects, evidence suggests that chronic wildfire smoke exposure has systemic consequences. Navarro et al reported increased RRs of lung cancer (1.08–1.43) and cardiovascular disease (1.16–1.30) among wildland firefighters, with risk rising in proportion to years of service. 62 The risk assessment did not account for previous fire exposures prior to their firefighting careers. Collectively, these findings highlight the substantial occupational risks firefighters face because of chronic and repeated wildfire smoke exposure. They underscore the urgent need for stronger protective measures, improved respiratory protection protocols, and longitudinal surveillance to assess long-term respiratory and systemic health effects in high-risk occupational groups.
Protective Strategies
Personal protective measures are critical for mitigating the respiratory health impacts of wildfire smoke, with mask use being one of the most effective strategies. However, the level of protection varies depending on the mask type. Cloth masks provide minimal filtration of PM2.5 because of the small size of smoke particulates. Surgical masks offer moderate protection, particularly against larger particles, but are insufficient against fine particulate matter. In contrast, respirator masks (eg, N95, P2) provide the highest level of filtration and are the most effective at reducing inhalation of PM2.5. 63 (Fig. 6).
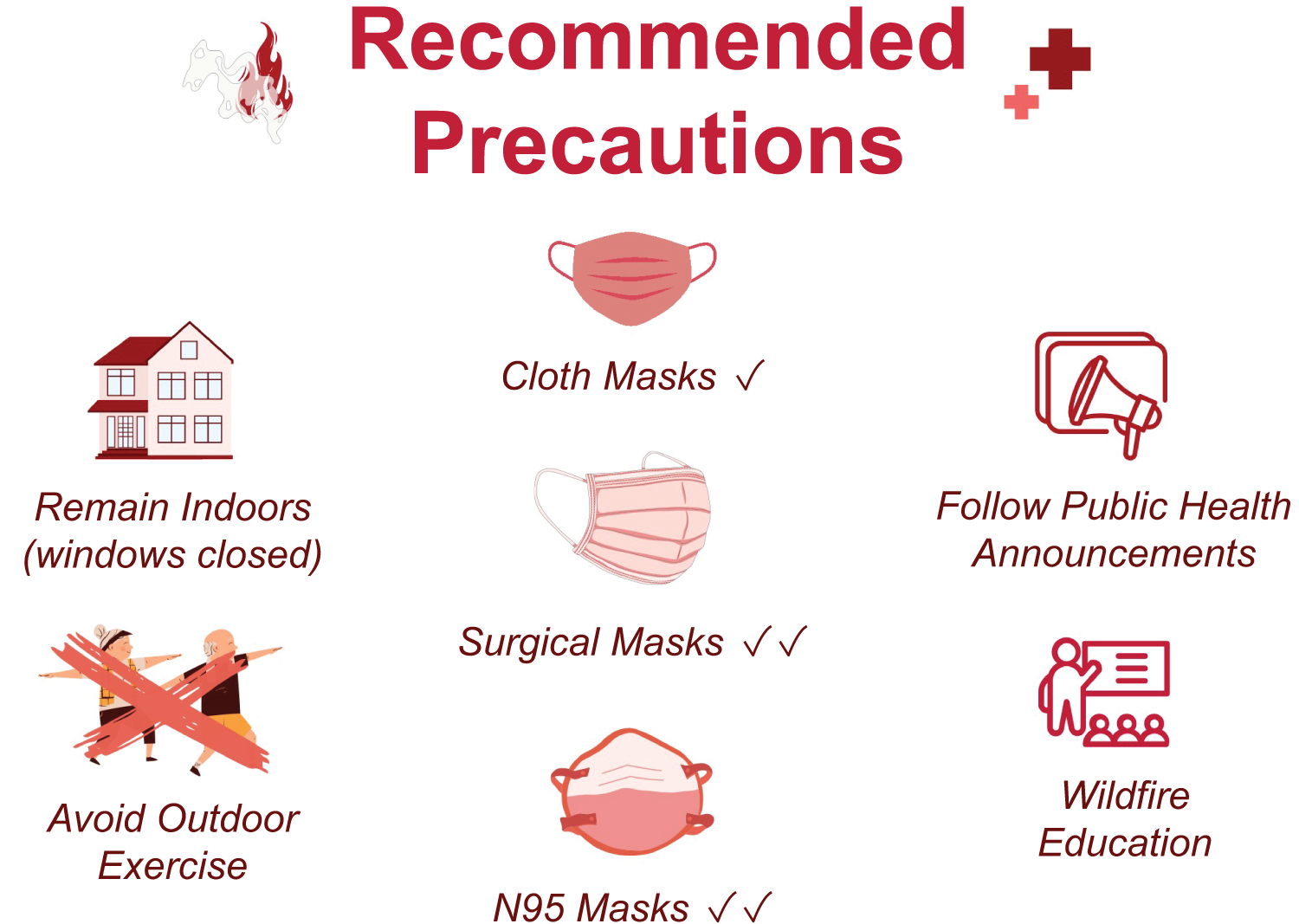
Recommended precautions during wildfire smoke exposure. This figure outlines key public health recommendations to reduce exposure to wildfire smoke. Strategies include remaining indoors with windows closed, avoiding outdoor physical activity, wearing appropriate respiratory protection (with increasing filtration efficacy from cloth masks to surgical masks to N95 respirators), following public health announcements, and engaging in wildfire education initiatives.
Despite their effectiveness, mask usage remains inconsistent in wildfire-affected populations. A survey by Seale et al found that few individuals wore masks specifically to protect against wildfire smoke. Among those who did, many repurposed masks originally intended for other uses (eg, COVID-19 protection, gardening) rather than obtaining purpose-built wildfire respirators. Encouragingly, a majority expressed willingness to adopt appropriate mask use in future wildfire events, highlighting an opportunity for improved public education and preparedness. 64
Firefighters, who experience the most intense and prolonged smoke exposure, require especially robust protective strategies. In a study by Ramos et al, 77% of firefighters who used fabric masks equipped with FFP2 filters showed no evidence of restrictive ventilatory patterns. In contrast, 61% of those who did not use respiratory protection exhibited such patterns, underscoring the importance of proper respiratory equipment in preventing long-term pulmonary damage in high-risk occupational groups. 55
Behavioral strategies also play a vital role. Staying indoors and improving indoor air quality—such as sealing windows and using high-efficiency particulate air filters—can significantly reduce exposure. Although these measures are widely recommended, adherence varies. For example, a survey conducted in Yellowknife, Canada found that although 76% of residents were aware of air quality alerts, only 48% reported following the advice to remain indoors during wildfire events. 67 This gap highlights a need for more effective risk communication and practical support for implementing avoidance strategies.
Additionally, health care providers play a pivotal role in guiding patients, but knowledge gaps may hinder effective counseling. A study by Crocker et al involving 21 pediatric pulmonologists found that only 25% knew where to access reliable guidance for managing wildfire smoke exposure, and just 36% felt confident educating patients on protective measures. 65 These findings suggest an urgent need for enhanced provider training and accessible clinical resources. Together, these results support prioritizing effective mask use, clearer public guidance on indoor avoidance, and improved provider education to reduce the health burden of wildfire smoke.
Summary
Wildfire smoke exposure poses significant respiratory health risks across the lifespan, beginning as early as gestation. Elevated levels of PM2.5 have been consistently associated with increased respiratory symptoms, more medication use, higher rates of ED visits, and long-term declines in pulmonary function. Firefighters and others with repeated and prolonged exposure exhibit early signs of pulmonary impairment, underscoring the occupational hazards of wildfire response work. To mitigate these risks, individuals in affected regions—particularly those in vulnerable groups—must adopt and adhere to protective strategies, including the use of high-efficiency masks and indoor air quality improvements, and avoidance behaviors during smoke events. Future research should prioritize longitudinal studies to better characterize the chronic effects of wildfire smoke exposure, evaluate the efficacy of protective measures, and inform public health education aimed at improving community-level preparedness and resilience.
Footnotes
Acknowledgment
The authors would like to thank Lorena Juarez from the Library of Rush University for her help in the literature search and screening. ChatGPT was used to assist in revising the manuscript for improved readability. The authors retain full responsibility for the content of this publication.
Author Disclosure Statement
Dr. Li discloses research funding from COPD Foundation, the American Association for Respiratory Care, MEKICS Co. Ltd., and Vincent Ltd., and speaker fees from the American Association for Respiratory Care, Aerogen Ltd., Heyer Ltd., Vincent Ltd., and Fisher & Paykel Healthcare Ltd. Dr. Li is also a section editor of R
Funding Information
No funding was received for this article.