
Abstract
Background:
Children with cardiac disease liberated from mechanical ventilation often receive noninvasive respiratory support (NRS) postextubation via high-flow nasal cannula, CPAP, or noninvasive ventilation. Predicting the type and duration of postextubation NRS can be challenging due to a lack of objective tools to guide decision-making. The dead space to tidal volume ratio (VD/VT) is a potential tool to guide this decision. We hypothesized that an elevated VD/VT would be associated with longer duration and higher level of NRS following extubation in children with cardiac disease.
Methods:
We conducted a retrospective cohort study of mechanically ventilated patients admitted to our pediatric cardiac intensive care unit between March 2019 and July 2021 with at least one VD/VT recorded before extubation. Subjects were dichotomized a priori into two groups VD/VT < 0.30 and VD/VT ≥ 0.30. We recorded the type of NRS at 24 hours, 48 hours, 72 hours, 7 days, and 14 days after extubation.
Results:
We included 226 subjects. Median (IQR) weight was 4.1 (3.3–6.6) kg, 47% were female, 47% had cyanotic heart disease, and 90% were mechanically ventilated for respiratory failure or cardiac surgery. Subjects with VD/VT ≥ 0.30 experienced longer postextubation NRS (4 [1.9–9.1] vs 3 [1.2–5.3] days, P = .001) and were more likely to receive high-flow nasal cannula (67% vs 45%, P = .02) 24 hours following extubation. NRS modality immediately postextubation and reintubtion rates were similar between groups. Subjects with VD/VT ≥ 0.30 were younger (1.2 [0.1–3.6] vs 4.8 [1.2–30] months, P < .001) and more likely to have cyanotic congenital heart disease (59% vs 26%, P < .001). After adjusting for demographic and clinical characteristics, VD/VT was not associated with NRS use.
Conclusions:
VD/VT was not associated with the length of NRS after extubation or re-intubation after controlling for demographic and clinical differences.
This is a visual representation of the abstract.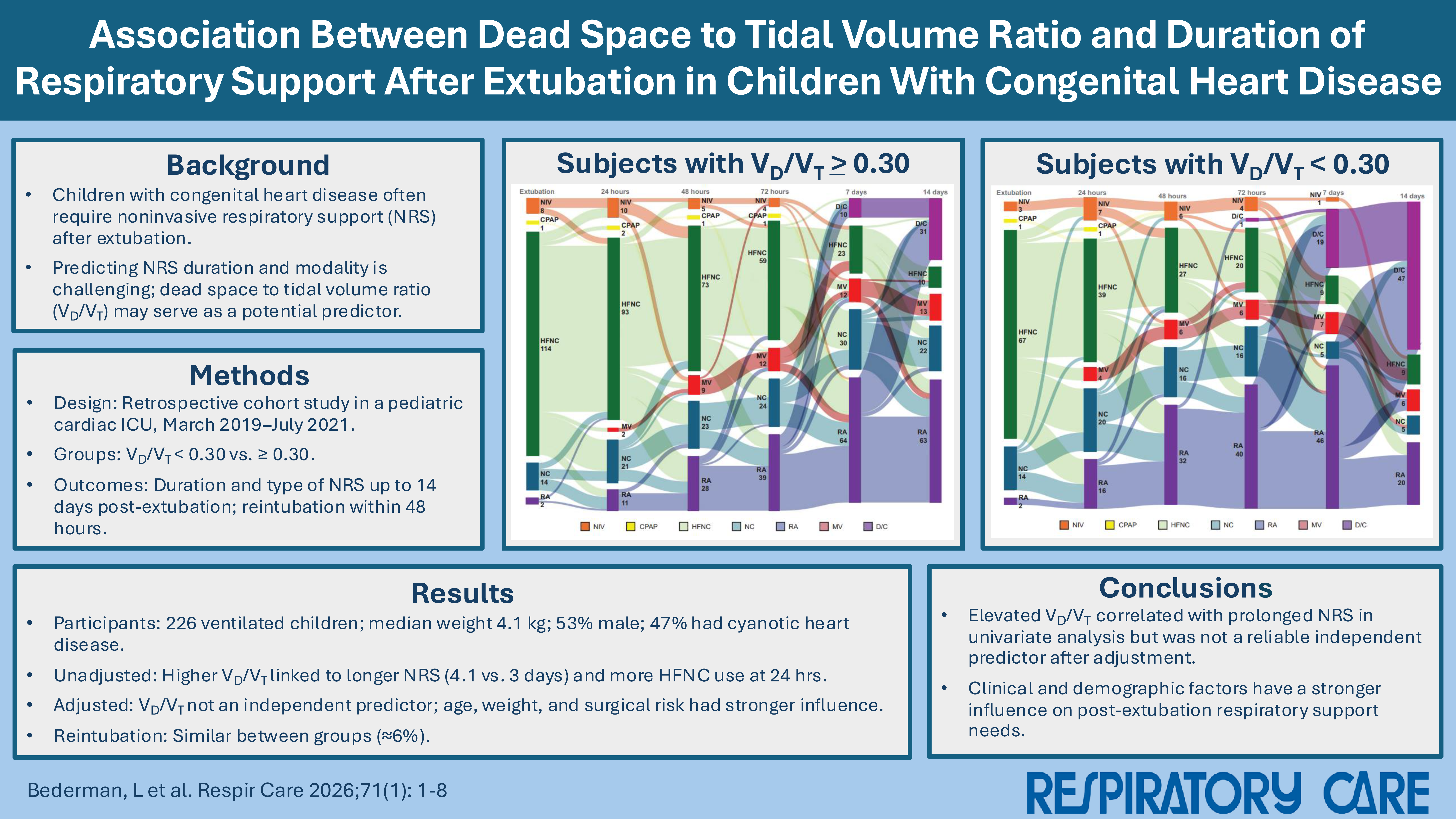
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.