
Abstract
Background and Purpose
Status epilepticus (SE) is a life-threatening emergency associated with high morbidity and mortality. Limited guidance exists on optimal therapy for refractory SE (RSE), which may include administration of repeat second-line IV-antiseizure medications (IV-ASMs) or escalation to IV-anesthesia (IVA). This study examined real-world treatment dynamics and outcomes of hospitalized patients with RSE in the United States.
Methods
A retrospective, cross-sectional analysis of hospitalized patients with SE between 2018-2022 was performed using PINC AI™ Healthcare Database. Patient encounters for RSE were categorized into RSE-no IVA (≥2 IV-ASMs without IVA) and RSE-IVA (≥1 IV-ASMs with IVA and concomitant mechanical ventilation). RSE-no IVA episodes were further stratified by exposure to 2 IV-ASMs and ≥3 IV-ASMs.
Results
Across 140 538 SE episodes in 113 229 unique patients, 44% were RSE. IV-ASM and IVA exposure, as well as time to escalation varied widely across SE episodes. Compared to RSE-no IVA episodes (59%), RSE-IVA episodes (41%) were associated with increased ICU length of stay (LOS; 5 vs 3 days), hospital LOS (9 vs 6 days), and in-hospital mortality (25% vs 12%). Compared to patients with RSE-no IVA administered 2 IV-ASMs, those administered ≥3 IV-ASMs had increased ICU admission (73% vs 62%), longer ICU LOS (4 vs 2 days), and hospital LOS (9 vs 5 days).
Conclusions
Heterogeneity in RSE treatments management is prominent, with variation in IV-ASM treatment sequencing and escalation timing. Both increased IV-ASM utilization and IVA exposure were associated with similarly worse outcomes and healthcare utilization. Rapidly effective anti-SE treatments remain an urgent unmet need in this patient population.
Introduction
Status epilepticus (SE) is a common life-threatening neurological emergency associated with high morbidity, mortality, and healthcare resource utilization.1-4 The incidence of SE reported in the United States (US) ranges from 3.5 to 41 episodes per 100 000 patients per year and may be higher with increased utilization of electroencephalograms (EEGs) allowing for increased detection of non-convulsive SE.5-9 Prolonged uncontrolled seizure activity in SE increases the risk of neurologic injury, including alterations of neuronal networks and neuronal death.10,11 To minimize negative consequences, management of SE centers around rapid and sustained seizure control.12,13
Current guidelines recommend administration of a benzodiazepine (ie, lorazepam, diazepam, or midazolam) as first-line therapy for SE.10,14 Approximately one third of patients do not respond to first-line therapy and are considered to have established SE (ESE), requiring administration of second-line intravenous (IV) antiseizure medications (ASMs).14-16 SE cessation is achieved in approximately 50% of patients after second-line IV-ASM administration, with the remaining 50% progressing to refractory SE (RSE), necessitating additional treatment with IV-ASMs or escalation to IV-anesthesia (IVA).3,10,17-20 If SE continues for ≥24 hours after initiation of IVA or recurs after withdrawal or reduction of IVA, it is considered super-refractory (SRSE).21,22
While first-line therapy for convulsive SE is well established, treatment approaches in RSE are less understood, limited by absence of randomized controlled trials confirming efficacy or superiority of any single therapy in optimizing patient outcomes.14,20 Optimal treatment selection for patients who do not respond to initial therapies, including whether to escalate to IVA or trial alternative IV-ASMs, remains unknown. The objective of this study was to examine the real-world treatment of patients with RSE reflective of the current standard of care in the hospital setting in the US, including baseline profiles, treatment characteristics, and clinical outcomes.
Methods
A retrospective, claims-based, cross-sectional analysis of PINC AI™ Healthcare Database was conducted in patients with SE from 2018 to 2022. PINC AI™ Healthcare Database is a deidentified, hospital-based, service-level, all-payer database capturing hospital and patient-level data from over 347 million adult and pediatric patients and 170 million visits, representing ∼25% of all-cause annual US inpatient admissions.
23
Hospitalized patients were included if encounter billing listed an International Classification of Disease 10th Edition code of “with status epilepticus” during the hospital visit (including direct inpatient, emergency department (ED) to inpatient and ED-only) in the primary or secondary diagnostic position within the study period (eTable 1). Metrics that required complete visibility into patient encounters were evaluated using a subset of episodes (referred to as “Completed Episodes”, eTable2) in which patients were not identified as having transferred between centers during their care based on claims data (eTable 3). Patient encounters were segmented according to benzodiazepine, IV-ASM, and IVA treatment exposures (Figure 1) into cohorts based on previously published definitions.
2
Patient encounters for RSE were categorized into RSE-no IVA (≥2 IV-ASMs without IVA) and RSE-IVA (≥1 IV-ASMs with IVA and concomitant mechanical ventilation (MV)). RSE-no IVA episodes were further stratified by exposure to 2 IV-ASMs and ≥3 IV-ASMs. RSE-IVA was subcategorized into SRSE for episodes with 2 or more consecutive days of IVA and concomitant MV. Since benzodiazepine administration by patient caregivers, emergency medical personnel, or other outpatient providers was not captured within the PINC AI™ Healthcare Database, RSE segmentation was not reliant on documentation of benzodiazepine administration. IVAs administered in the operating room setting were excluded for RSE segment evaluation, as these were likely administered for indications other than acute treatment of SE (eg, for elective surgery). Comorbid acute etiologic factors of interest were identified using ICD-10 codes (eTable4). SE Episode Segmentation. Abbreviations: IV, intravenous; IVA, intravenous anesthesia; IV ASMs, intravenous antiseizure medications; RSE, refractory status epilepticus; SE, status epilepticus; SRSE, super-refractory status epilepticus. Note. IV ASMs exposures included IV formulations of the following ASMs: levetiracetam, fosphenytoin, phenytoin, lacosamide, brivaracetam, phenobarbital, valproic acid. Benzodiazepine exposures included non-oral formulations [IV, intramuscular, intraosseous, para rectal, or intranasal routes] of the following benzodiazepines: lorazepam, diazepam, midazolam. IVA exposure included exposure to IV formulations of the following anesthetic: propofol, ketamine, pentobarbital, midazolam. Midazolam was categorized as an anesthetic if administered intravenously in the intensive care unit concomitantly with mechanical ventilation
Clinical outcome measure evaluated included ICU and hospital length of stay (LOS), discharge status, inpatient mortality, and 30-day readmission rates between cohorts. Further, treatment characteristics, including provider and treatment distribution, were investigated. As this study utilized a de-identified claims database, and all data were analyzed in accordance with ethical guidelines for use of secondary data, institutional board review was not required based on the policy of the Office of Human Subjects Research Protections, National Institutes of Health, under the revised Common Rule.
Data Analysis
Baseline characteristics across RSE cohorts were evaluated using t-tests or χ2 test as appropriate. Association of RSE cohort with discharge disposition was evaluated using ordinal logistic regression between groups, ordered from lowest to highest starting from home, followed by long-term care/rehab/intermediate care facility/other, hospice, and death. Ordinal regression analysis was used to assess the relationship between the groups of interest and discharge outcomes with adjustment for age and acute etiologic factors of interest. Outcome variables related to hospital and ICU LOS were examined between groups using negative binomial multivariate regression with age and presence of acute comorbid etiologic factors as covariates. Findings were considered significant at P < 0.05.
Results
Baseline Characteristics

Abbreviations: ICF, intermediate care facility; IQR, interquartile range; IVA, intravenous anesthesia; IV ASMs, intravenous antiseizure medications; RSE, refractory status epilepticus; SNF, skilled nursing facility. Complete Episode Sample refers to episodes in which patients were not transferred to another center during their care. Adjusted Episode Sample refers to episodes that were consecutive within a 2-day span and were likely the same continuous episodes that were stitched together with full visibility. Refer to eTable 3 for more detail.
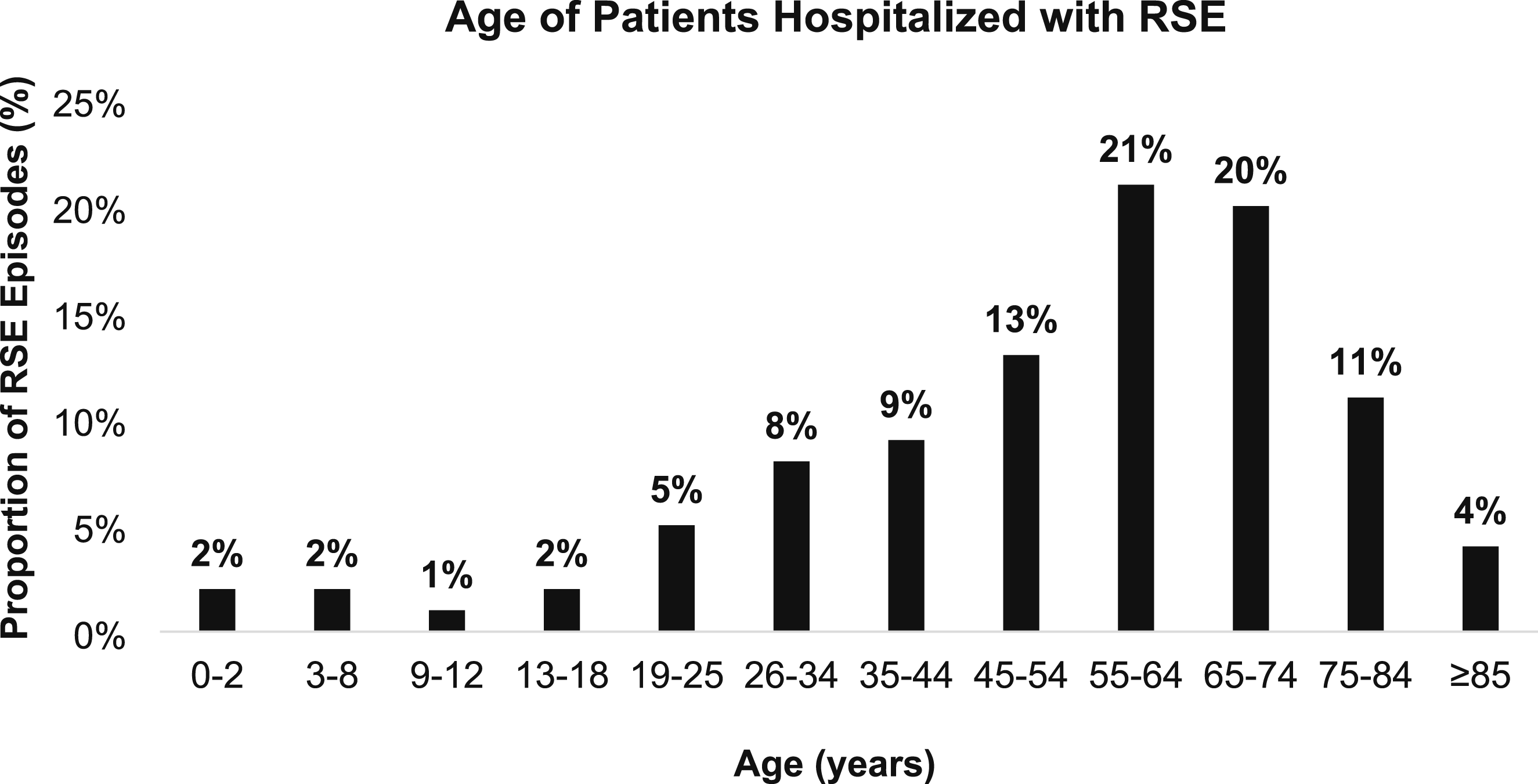
Age distribution of hospitalized patients with refractory status epilepticus
Treatment Characteristics

Abbreviations: IV ASM, intravenous antiseizure medication; IVA, intravenous anesthesia; IQR, interquartile range; NA, not applicable.
aUtilized the adjusted complete episode sample (n = 92 055).
SE as a secondary diagnosis to a primary illness generally increased with escalating exposure to additional IV ASMs and IVA. RSE episodes presented to academic (61%) or community (39%) hospitals of varying sizes. Most RSE episodes in academic hospitals were treated at large centers with ≥500 beds (63%), while admissions to a community center were equally distributed across institution sizes (Table 1). The emergency room was the most common entry point (89%), with most cases (92%) originating from home. The hospital admitting specialty during RSE episodes was heterogenous, encompassing neurologists, hospitalists, and pulmonologists, among others.
Association of IVA on Clinical Outcomes in RSE
Clinical Outcomes of RSE by IVA and IV ASM Exposure
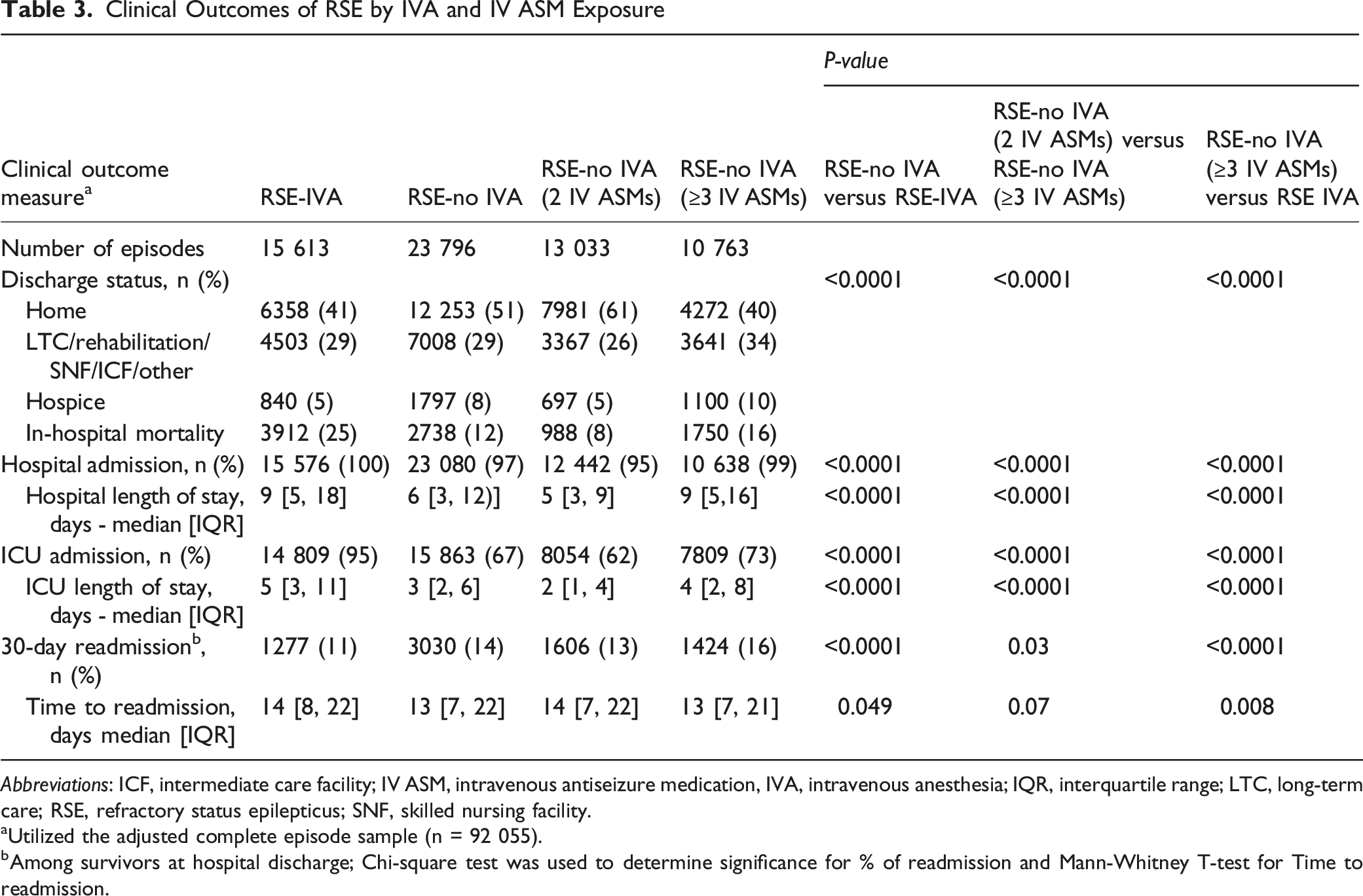
Abbreviations: ICF, intermediate care facility; IV ASM, intravenous antiseizure medication, IVA, intravenous anesthesia; IQR, interquartile range; LTC, long-term care; RSE, refractory status epilepticus; SNF, skilled nursing facility.
aUtilized the adjusted complete episode sample (n = 92 055).
bAmong survivors at hospital discharge; Chi-square test was used to determine significance for % of readmission and Mann-Whitney T-test for Time to readmission.
Association of Repeat IV-ASMs on Clinical Outcomes in RSE
The RSE-no IVA with ≥3 IV-ASMs episodes compared with 2 IV-ASMs saw increased ICU admission, ICU LOS (median 4 [IQR 2, 8] vs 2 [1, 4] days), and hospital LOS (9 [5, 16] vs 5 [3, 9] days), in-hospital mortality (16% vs 8%) or discharge to hospice (10% vs 5%) or care services (34% vs 26%), and decreased discharge to home (40% vs 61%), Table 3. When adjusted for age and comorbid acute etiologic factors, the RSE-no IVA with ≥3 IV-ASMs episodes saw 1.6-fold increased odds in ICU LOS (95% CI 0.43, 0.48; P < 0.0001) and 1.6-fold increased odds in hospital LOS (95% CI 0.46, 0.51; P < 0.0001) compared to 2 IV-ASMs. Additionally, RSE-no IVA (≥3 IV-ASMs) episodes were associated with 1.9-fold increased odds in in-hospital mortality (95% CI 0.55, 0.72; P < 0.0001) and 1.9-fold decreased odds of discharge to home (95% CI 0.59, 0.69; P < 0.0001) compared to 2 IV-ASMs after adjustment for age and comorbid acute etiologic factors. Thirty-day readmission rates were higher amongst survivors to hospital discharge in RSE-no IVA (≥3 IV-ASMs) episodes vs RSE-no IVA (2 IV-ASMs) episodes.
Association of RSE Episodes Treated With IVA vs ≥3 IV-ASMs Only
RSE-IVA episodes compared with the RSE-no IVA (≥3 IV-ASMs) episodes were associated with only marginally increased ICU admission, ICU and hospital LOS, and in-hospital mortality but decreased discharge from hospital to other care services (29% vs 34%) (Table 3). When adjusted for age and comorbid acute etiologic factors, RSE-IVA episodes were associated with 1.3-fold increased odds in ICU LOS (95% CI 0.25, 0.30; P < 0.0001), and 1.1-fold increased odds in hospital LOS (95% CI 0.10, 0.14; P < 0.0001) compared to the RSE-no IVA (≥3 IV ASMs) episodes. Furthermore, RSE-IVA episodes were associated with 1.8-fold increased odds in in-hospital mortality (95% CI 0.50, 0.63; P < 0.0001) and 1.3-fold decreased odds of discharge to home (95% CI 0.18, 0.27; P < 0.0001) compared to the RSE-no IVA (≥3 IV-ASMs) episodes after adjustment for age and comorbid acute etiologic factors. Thirty-day readmission rates were marginally higher amongst survivors to hospital discharge among RSE-no IVA (≥3 IV-ASMs) episodes vs RSE-IVA episodes (16% vs 11%, P < 0.0001).
Outcomes of RSE Episodes With IVA that Progressed to SRSE
In patients with RSE who received IVA, 26% progressed to SRSE with SRSE episodes having incrementally worse outcomes, higher healthcare utilization, and increased in-hospital mortality (eTable 5).
Discussion
Despite advances in critical care, patients suffering from RSE continue to encounter substantial risks of morbidity and mortality. Care pathways and their association on outcomes in RSE remain largely unexplored due to the heterogeneity of SE coupled with a complex, evolving treatment landscape influenced by multiple guidelines. Thus, our retrospective, cross-sectional analysis examined the real-world treatment of patients with RSE in the hospital setting in the US. Overall, we found that heterogeneity in treatment exists in the current standard of care management of RSE, with variability in treatment selection and care pathways that may impact patient outcomes and recovery.
SE onset may be abrupt, presenting as an exacerbation of an underlying epilepsy disorder, new seizure disorder, or complication of an acute medical or neurologic illness. 10 In our study, RSE episodes presented equally at both academic and community medical centers across patients of all ages in the emergency medicine or inpatient setting, cared for by a variety of specialties and/or generalist providers. As duration of SE is an independent predictor of treatment-refractoriness and poor outcomes, rapid SE control is the cornerstone of treatment goals.12,13 Coupled with the heterogenous demographics of patients with RSE, universal recognition of SE symptomology and comfort with varying treatment strategies are necessary to optimize patient outcomes.24,25 Structured curriculums such as Emergency Neurologic Life Support certification and SE simulations to support education of a broad range of neurology, critical care and emergency medicine healthcare practitioners are examples of tools that have been successfully implemented to heighten awareness and support patients.26-28 Despite the need for control of ongoing seizures in SE, there is no clear evidence to guide selection of RSE therapy and current guidelines recommend either repeat IV ASM or escalation to IVA.10,14,29 Our study found repeat IV-ASM was administered in the majority of RSE episodes, though administration of IVA ultimately occurred in ∼40% of total RSE episodes. Furthermore, the treatment selection for first-line and second-line IV-ASM therapy, as well as IVA of choice, was diverse.
While the time to treatment and median total number of therapies was largely similar among RSE episodes regardless of IVA treatment, there were observed gaps in duration between treatments. This finding contrasts with current guideline recommendations on administration of first-line, second-line, and third-line therapy within 0-5, 5-10, and 20-60 minutes of SE onset, respectively.10,14 Incongruence between guidelines and clinical practice may be attributed to seizure activity, acute SE treatments not being readily available, a lack of access to continuous EEG monitoring and personnel with expertise of EEG technology, and the inability to sustain seizure control leading to SE reoccurrence. While it cannot be concluded from this study that the prolonged treatment times directly led to the poor outcomes and the need for IVA, minimizing times between treatment is imperative for rapid and sustained seizure control and for limiting the pathophysiological changes associated with ongoing SE.12,13,30
In patients with RSE, exposure to IVA was associated with worse outcomes, including increased in-hospital mortality, ICU and hospital LOS, and healthcare resource utilization. While episodes exposed to IVA saw more comorbid acute etiologic factors, which are associated with poor outcomes in RSE, our findings were adjusted for this confounding variable.31,32 The mortality rates in our study are generally consistent with previous literature that has demonstrated that patients with RSE who require IVA with MV have increased risk of complications, longer hospital and ICU LOS, and increased mortality.33,34 This increased risk of mortality appears to not only be related to the severity of SE, underlying etiologies, and prolonged immobility of patients with RSE but also due to IVA treatment itself.33,35,36 Patients with SE who require prolonged use of IVA with MV have previously been reported to have 3-fold higher mortality than patients not requiring MV, exceeding 30% across studies.35,37 Overall, our results further support established literature that treatment with IVA is a driver of poor outcomes and high mortality in patients with RSE. Therapeutic coma with intravenous anesthetics, particularly when prolonged and in severely ill patients, has been associated with hypotension requiring vasopressor support (with potential risk of organ hypoperfusion), frequent need for mechanical ventilation and invasive vascular access (which may increase risk of hospital-acquired infections), and delayed participation in early rehabilitation; however, these risks are influenced by depth and duration of sedation, underlying disease severity, and the clinical indication for coma induction.2,38 While exposure to IVA in our study was associated with decreased readmission rates, this decrease in readmission could be due to a number of factors including, increased clinical stability on hospital discharge following prolonged hospital and ICU length of stay, transfer to other services (eg, skilled nursing facilities, long-term care facilities, etc.) capable of providing a higher level of care for routine ailments than home caregivers, or other unmeasured confounders that warrant further consideration. Additionally, because patients with RSE who did not receive reported decreased mortality, it is possible that survivors to discharge may have represented a sicker population potentially more vulnerable to subsequent hospital readmissions.
Given safety concerns associated with the use of IVA, clinicians may opt to trial additional non-anesthetizing IV ASMs. In our study, we found that avoidance of IVA may not be associated with improved outcomes as even in the absence of IVA, the use of ≥3 IV-ASMs was associated with similarly poor outcomes, including increased in-hospital mortality, ICU and hospital LOS, and healthcare resource utilization that was maintained after adjustment for underlying comorbid conditions. While the use of IVA may be avoided in patients who may not tolerate it or are at heightened risk of complications, our study found that the cycling of IV-ASMs may not offer an advantage.33,34 To our knowledge, current literature predominately categorizes RSE cohorts on the use or lack of IVA. Our study provides unique insights into patient outcomes related to cycling IV ASMs beyond the initial 2 IV ASM treatments.2,39,40 While some guidelines recommend escalation to IVA in patients with a benzodiazepine who fail one IV ASMs, others provide no preference on whether repeat IV ASMs therapy or IVA should be used as third-line therapy.10,14 Thus, while optimal treatment sequencing with IV ASMs and/or IVA remains to be determined and often based on patient and provider-specific factors, it remains critical that early treatment success is critical for patient outcomes.
SRSE in literature is generally defined as SE that continues for ≥24 hours after initiation of IVA or in which SE recurs after the withdrawal or reduction of IVA and is associated with significantly worse outcomes.21,22 Patients with prolonged exposure to IVA with MV ≥2 days (ie, SRSE) in our cohort reported highest mortality and healthcare resource utilization. Surprisingly, patients with SE requiring increased IV-ASM therapy also showed incrementally worse outcomes compared to those with an initial treatment response, similar to patients with RSE who needed extended durations of IVA. Overall, the refractoriness to standard of care, whether to repeat IV-ASMs or IVA, and their association with poor outcomes in SE represents a patient population with high unmet needs. Collectively, these results indicate that increased treatment intensity leads to poor outcomes and filling knowledge gaps in the literature may help guide optimal treatment selection for patients with RSE.
Limitations
There are several limitations of this study that should be considered. Data captured within the PINC AI™ Healthcare Database were reliant on accurate ICD-10 coding by providers; thus, we were unable to differentiate between SE subtypes (eg, convulsive vs non-convulsive SE, focal vs generalized SE), or offer definitive assessment of etiologic factors. Additionally, pre-existing conditions or treatments not reported on a medical claim for emergency department or inpatient care was not available to be captured, including baseline epilepsy disorders. Exact timing, dose, and clinical or electrographic responses to medication used to treat SE was not available. Episodes isolated to the outpatient setting or those transferred in or between centers during care were excluded due to an inability to track patients across facilities within the database. Comorbid conditions beyond the select etiologies have not been included in the outcomes assessment given the extensive heterogeneity and prevalence of conditions across diverse age groups and warrant further study. Furthermore, in addition to age that was adjusted for in our analyses, prognostic scores predominately rely on level of consciousness, seizure characteristics and duration were unable to be captured within the hospital database system. Anoxic brain injury was an acute comorbid etiologic factor in a subset of SE episodes included in this analysis, a condition characterized by high mortality and may have confounded the outcomes despite adjustment for the presence of etiologic factors of interest. However, the proportion of patients with anoxic brain injury was similar between patients with RSE no IVA (2 IV ASMs) and RSE no IVA (≥3 IV ASMs) and increased treatment exposure remained associated with worse outcomes including in-hospital mortality, hospital and ICU length of stay, and 30-day readmission. Additionally, patients with no etiologic factors of interest present still reported a 1.8 – 2.3x increased odds of death between RSE cohort comparison groupings. While the objective of this study was to examine overall SE episodes irrespective of underlying condition, future studies should examine the impact of varying treatment intensity within defined subpopulations presenting with similar acute conditions. Lastly, although our definitions of SE refractoriness were based off previously established research methods, we were unable to confirm the clinical context for which medications were started during SE episodes.2,41 Despite these limitations, this research provides important insights into the heterogeneity in RSE treatment and outcomes within a national cohort.
Conclusions
In this real-world, claims-based analysis, our findings demonstrated heterogeneity in RSE treatment, with variation in IV ASM treatment sequencing and prolonged time between treatment escalation. RSE episodes that required IVA were associated with increased ICU admission rates, longer ICU and hospital LOS, and high mortality. Even in the absence of IVA treatment, RSE episodes that were treated with ≥3 IV-ASMs had worse outcomes and longer LOS compared to those treated with 2 IV-ASMs. Overall, rapidly effective and durable treatments for SE remain an urgent unmet need in this patient population where treatment refractoriness and exposure to IVA may be modifiable risk factors for poor outcomes.
Supplemental Material
Supplemental Material - Evaluating Treatment Dynamics in Refractory Status Epilepticus: A Retrospective Observational Cohort Study
Supplemental Material for Evaluating Treatment Dynamics in Refractory Status Epilepticus: A Retrospective Observational Cohort Study by Megan Barra, Henrikas Vaitkevicius, Salia Farrokh, Sri Saikumar, Saloni Shah, Dushyant Katariya, Eva Rybak in The Neurohospitalist
Footnotes
Acknowledgements
The authors acknowledge Adrienne Lovink for her support on data interpretation, Harjeet Singh for support with data analytics, Dalia Murra for assistance with data analysis and medical writing support, and Jared D. Hoffman for medical editorial assistance under the guidance of the authors. This work was performed by Marinus Pharmaceuticals, Inc (now an indirect wholly owned subsidiary of Immedica Pharma, AB as of 2025).
Ethical Considerations
As this study utilized a de-identified claims database, and all data were analyzed in accordance with ethical guidelines for use of secondary data, ethic board review was not required based on the policy of the Office of Human Subjects Research Protections, National Institutes of Health, under the revised Common Rule.
Author Contributions
M.Barra, H.Vaitkevicius, S. Saikumar, S. Shah, and E. Rybak lead conceptualization of this project. S.Saikumar, S. Shah, and D. Katariya provided data analytics and statistical analysis support. M.Barra, H. Vaitkevicius, S. Farrokh, E.Rybak contributed interpretation and clinical translation of the data. M.Barra, S. Saikumar, and E.Rybak contributed to the drafting of the manuscript. All authors were involved in methodology development, critically reviewing the manuscript for intellectual content and final approval of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Marinus Pharmaceuticals, Inc.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs. Barra, Vaitkevicius, and Rybak report employment with and stock or stock options at Marinus Pharmaceuticals. Sri Saikumar reports equity in Trinity Life Sciences. All other authors have no conflicts of interest to disclose.
Data Availability Statement
All data supporting the findings of this study are available within the paper and its Supplementary Information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.