
Abstract
Clinical Problem
Identification, work-up and treatment approach of isolated cortical venous thrombosis (ICVT) in the absence of traditional risk factors.
Case Presentation
A 66-year-old previously well male presenting with two episodes of left-sided spreading sensory symptoms, found to be secondary to ICVT from extrinsic compression by an arachnoid cyst.
Key Teaching Points
Early identification of structural abnormalities causing extrinsic venous compression and ICVT or cerebral venous sinus thrombosis (CVST) is important for alternative treatment options and to avoid unnecessary testing.
A 66-year-old previously well male presented with two episodes of leftsided spreading positive sensory disturbance. Figure 1A Axial and Figure 1B coronal multiphase CT angiogram demonstrated isolated cortical vein thrombosis (ICVT) overlying the right parietal lobe, Figure 1C with adjacent subarachnoid hemorrhage seen on the noncontrast CT scan. Figure 1D Cerebral angiography demonstrated severe stenosis of the right vein of Trolard at the insertion to the superior sagittal sinus, and right hemisphere venous dilation. Figure 1E Sagittal and Figure 1F axial brain MRI T2 sequence scans revealed a hyperintense right parasagittal vertex arachnoid cyst causing extrinsic compression at the cortical vein insertion.
He was initiated on apixaban. Valproic acid was started for suspected focal seizures. Future cyst fenestration was discussed if the ICVT progressed despite anticoagulation.
Although hemorrhagic infarction and focal seizures are more common in ICVT than cortical vein thrombosis associated with cerebral venous sinus thrombosis (CVST), most clinicians treat ICVT with anticoagulation.
1
External compression, leading to stenosis and stasis, is a known contributing factor for CVST,
2
but not yet reported for ICVT. Early identification of structural abnormalities causing extrinsic venous compression and ICVT or CVST is important for alternative treatment options and to avoid unnecessary testing. (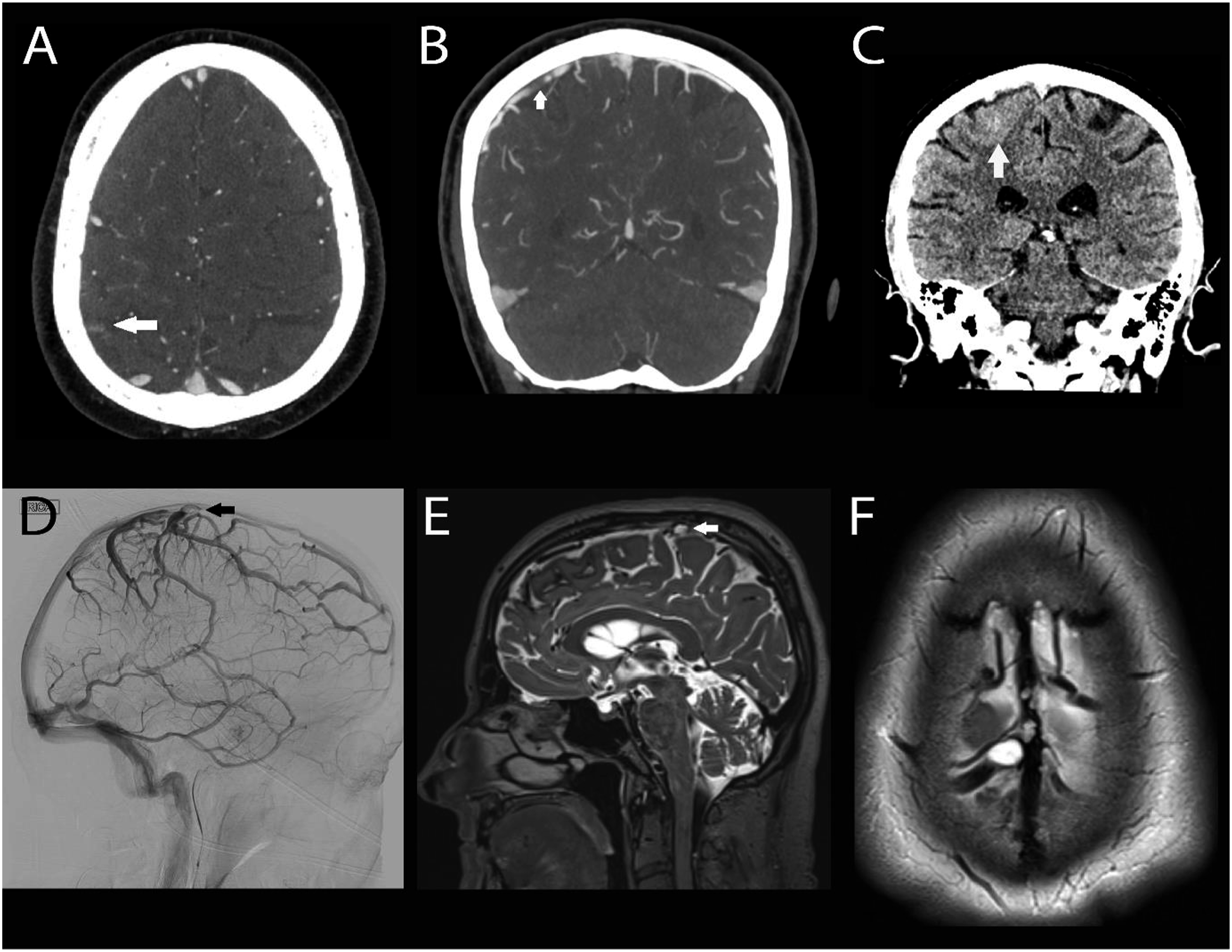
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AAJ is supported by Canadian Institutes of Health Research (award FRN 190708), the University of British Columbia Clinician Investigator Program, and the Ludmila & Henry Zeldowicz Endowment.