
Abstract
A previously healthy 21-year-old Caucasian female G1P0 at 32 weeks gestation presented to the ED for an episode of syncope. She also complained of headaches, neck pain, and blurry vision. Physical examination revealed a healthy pregnant female. Neurological examination demonstrated Grade III papilledema but was otherwise unremarkable. CT brain revealed hydrocephalus and intraventricular hemorrhage of unclear etiology MRI of the head was negative for a mass lesion. MRA/MRV of the head was negative, ruling out cavernous sinus thrombosis. Lumbar puncture was bloody but negative for infection. Infectious workup, including HSV, toxoplasmosis, and neurocysticercosis, was negative. An intraventricular drain was placed for hydrocephalus. While in the hospital, she developed sudden left-sided weakness, prompting an emergency C-section. Further workup with CT angio of the brain and neck revealed an arteriovenous malformation (AVM) involving the anterior spinal artery and adjacent venous plexus. Digital subtraction angiography showed a C2-3 pial AVM with a partially thrombosed nidal aneurysm. She was transferred to an outside hospital for embolization. Embolization obliterated the aneurysm, but residual flow remained in the AVM. Blood products are visible on sagittal MRI after embolization. At hospital discharge, her left-sided weakness had resolved, and her neurological examination was normal. The hydrocephalus had resolved.
Keywords
Case Report
A previously healthy 21-year-old Caucasian female G1P0 at 32 weeks gestation presented to the ED for an episode of syncope. She also complained of headaches, neck pain, and blurry vision. Physical examination revealed a healthy pregnant female. Neurological examination demonstrated Grade III papilledema but was otherwise unremarkable. CT brain revealed hydrocephalus and intraventricular hemorrhage of unclear etiology (Figure 1A). MRI of the head was negative for a mass lesion. MRA/MRV of the head was negative, ruling out cavernous sinus thrombosis. Lumbar puncture was bloody but negative for infection. Infectious workup, including HSV, toxoplasmosis, and neurocysticercosis, was negative. An intraventricular drain was placed for hydrocephalus (Figure 1B). CT head of hemorrhagic hydrocephalus with blood in the right lateral ventricle (arrow) (A). CT head without contrast two days post embolization showing persistent hemorrhagic hydrocephalus (B). A right external ventricular drain is present.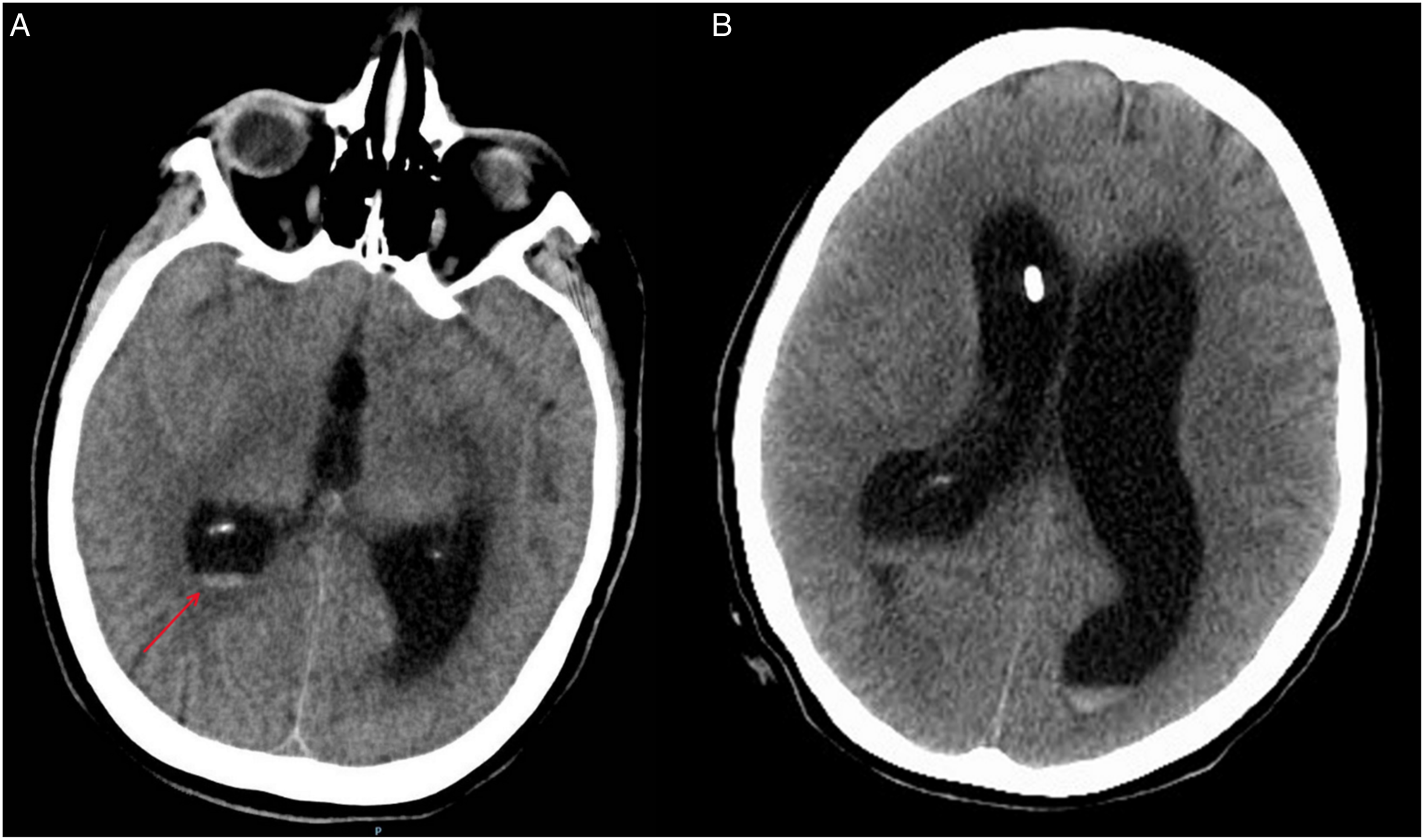
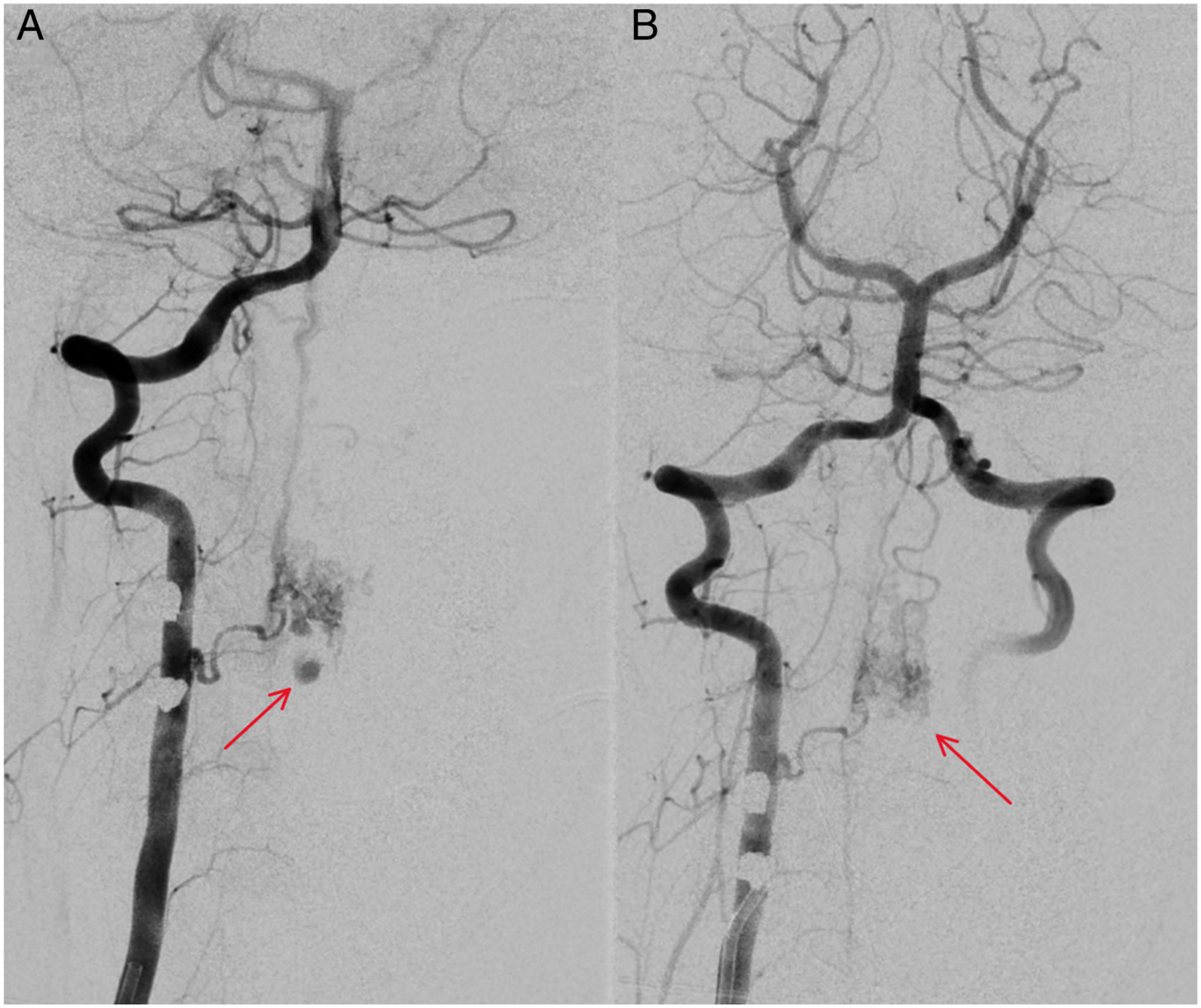
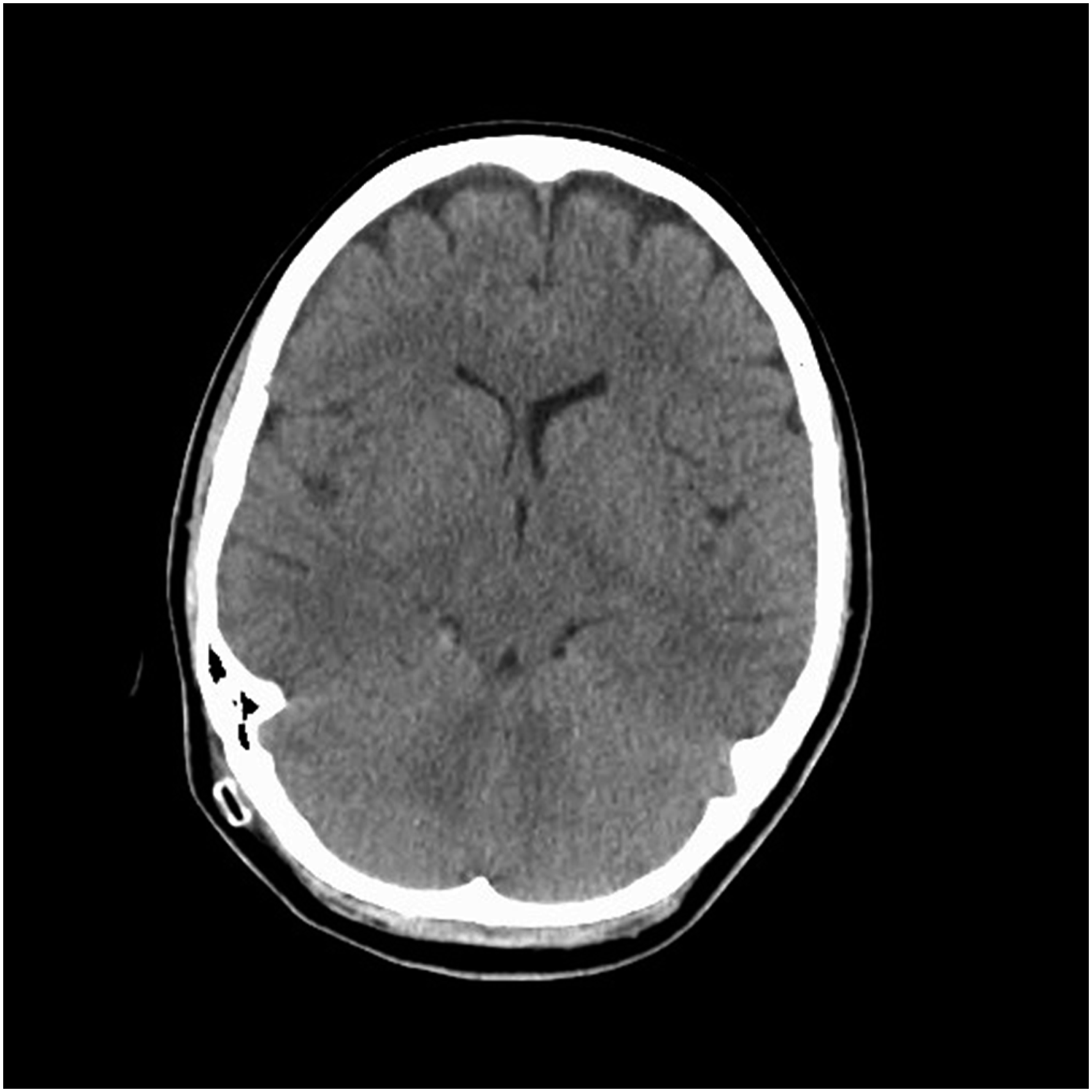
While in the hospital, she developed sudden left-sided weakness, prompting an emergency C-section. Further workup with CT angio of the brain and neck revealed an arteriovenous malformation (AVM) involving the anterior spinal artery and adjacent venous plexus with an associated aneurysm (Figure 2). She was transferred to an outside hospital for embolization. Embolization obliterated the aneurysm, but residual flow remained in the AVM (Figure 3). Blood products are visible on sagittal MRI after embolization (Figure 4). At hospital discharge, her left-sided weakness had resolved, and her neurological examination was normal. Her hydrocephalus has since resolved (Figure 5). CT angio of the brain and neck revealing an arteriovenous malformation (AVM) involving the anterior spinal artery and adjacent venous plexus (arrow) (A) with an associated aneurysm measuring 7 × 8 mm (arrow) (B). Digital subtraction angiography showing partially thrombosed intranidal aneurysm at the C2-C3 level (arrow) (A) pre and (B) post-embolization. There is no opacification of the aneurysm post embolization, but filling of the AVM remains (arrow). One day post embolization. Sagittal STIR MRI of cervical spine without contrast showing epidural blood products anterior to aneurysm (arrow) spanning C3-C6. CT head without contrast six weeks post embolization showing resolution of intraventricular hemorrhage and hydrocephalus.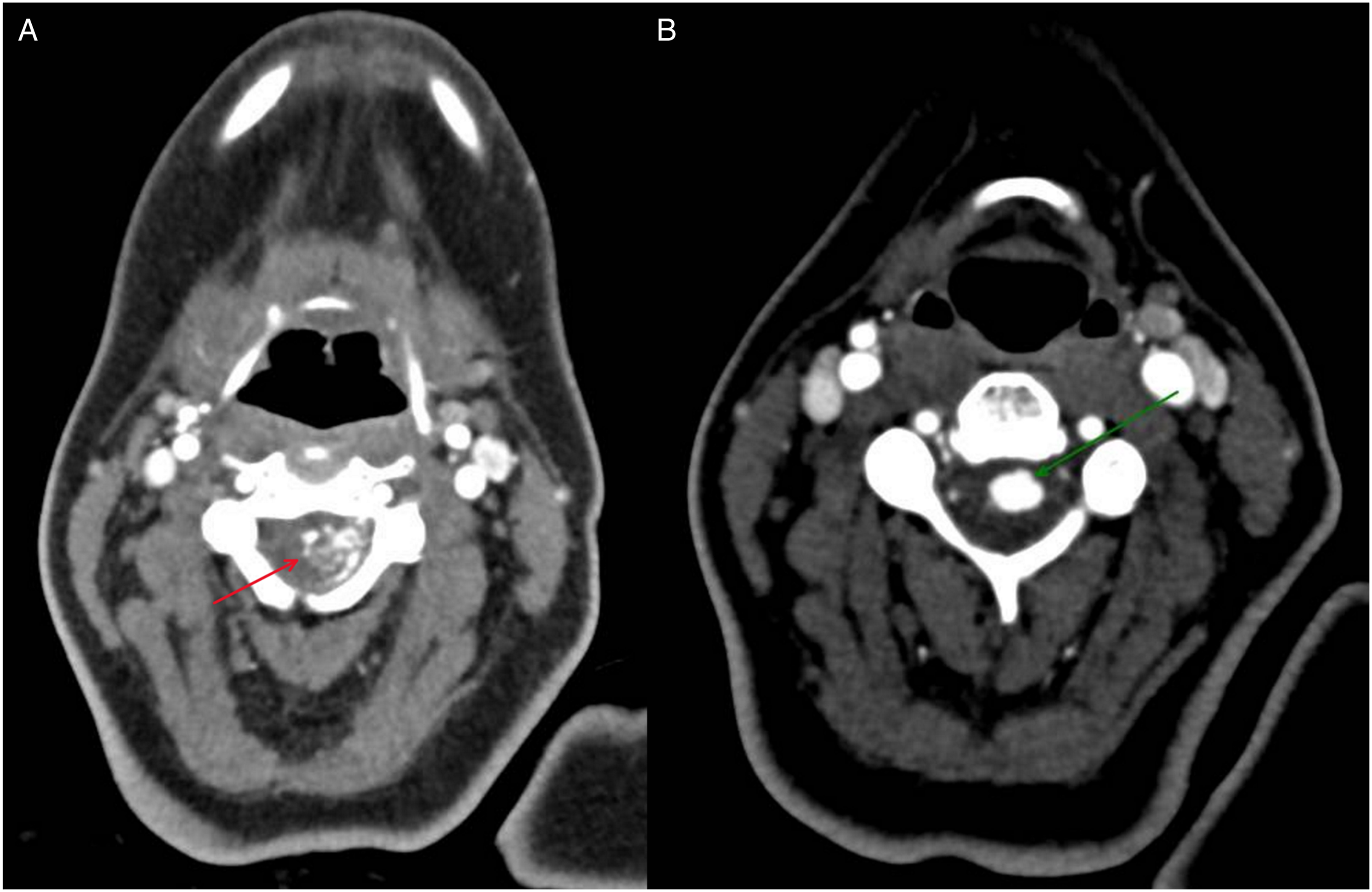

Discussion
Spinal arteriovenous malformations (AVMs) are rare and may precipitate neurologic deficits secondary to mass effect, ischemia, or hemorrhage due to venous hypertension from abnormal capillary beds. 1 Spinal AVMs comprise 3-4% of intradural lesions occupying the spinal cord. 2 Although similar in their pathology to intracranial AVMs, which can present with nonspecific symptoms and may be confused with more common etiologies of headache during pregnancy, 3 spinal AVMs often present with worse clinical symptoms. 4 Spinal AVMs often cause myelopathic symptoms, such as lower extremity weakness, loss of pain and temperature sensation, and bladder and bowel incontinence. Early diagnosis and treatment are necessary for improved long-term neurologic outcome. 4 The diversity, complex architecture, and lack of established treatment protocols of spinal AVMs constitute a therapeutic challenge. 2 Treatment options include endovascular embolization, open microsurgery, and stereotactic radiosurgery. 2
Only four other patients with cervical pial AVMs with a spinal aneurysm have been reported, one of whom was pregnant. Patients presented with unilateral upper extremity weakness, sudden hemiplegia, and tetraparesis. 5 Of these cases, the three that underwent treatment had symptom improvement without recurrence, while one patient died prior to treatment. 5
Although obstructive hydrocephalus from a hemorrhagic brain AVM in not unusual, 6 only one case of a hemorrhagic spinal AVM associated with obstructive hydrocephalus has been reported, but the patient was not pregnant. 7 To our knowledge, this is the first reported case of a cervical spinal AVM with an associated aneurysm resulting in hemorrhagic hydrocephalus in a pregnant woman. It is unclear whether the patient’s pregnancy increased the risk of hemorrhage. 3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.