
Abstract
Promethazine, a common antiemetic, can cause severe tissue injury with intravenous (IV) injection. Dihydroergotamine (DHE), commonly used for the acute treatment of migraine, can cause arterial vasoconstriction. We report a rare complication of brachial artery vasospasm in a patient receiving IV promethazine and DHE sequentially through the same midline IV catheter. A 40-year-old woman with history of migraine headaches and Raynaud phenomenon was admitted for treatment of status migrainosus with scheduled IV DHE infusions. While receiving the DHE infusions, IV promethazine was added to the patient’s regimen to treat nausea. During an infusion of DHE, the patient developed acute pain near the catheter insertion site due to active extravasation of IV DHE. An arterial Doppler ultrasound demonstrated stenosis in the right brachial artery near the region of infusion. The patient ultimately required balloon angioplasty and intra-arterial injection of nitroglycerin to restore adequate blood flow. We hypothesize that caustic injury to the right brachial vein from IV promethazine predisposed the patient to the extravasation of DHE, which, in turn, caused adjacent brachial artery vasospasm. This case suggests the need for careful consideration, if not strict avoidance, of the use of concurrent IV promethazine and DHE.
Introduction
Intravenous anti-emetic medications are frequently used for the treatment of migraine-related nausea. Promethazine, a first-generation anti-histamine and anti-emetic that is commonly used for this purpose, carries an FDA black box warning for severe tissue injury with intravenous (IV) injection. Dihydroergotamine (DHE), commonly used for the acute treatment of migraine, is known to cause arterial vasoconstriction. We report a rare complication of brachial artery vasospasm in a patient receiving IV promethazine and DHE sequentially through the same intravenous line.
Case Description
A 40-year-old woman with history of migraine and Raynaud phenomenon presented to the emergency department (ED) with a 10-day history of bi-frontal throbbing headache, nausea, vomiting, and photophobia typical of her prior migraine headaches. Initial treatment with IV ketorolac, IV diphenhydramine, IV prochlorperazine, and IV fluids did not improve her headache and she was admitted for treatment of status migrainosus with scheduled IV DHE infusions. A right upper extremity midline catheter (4 French single lumen in right basilic vein) was placed in preparation for her infusions. Her nausea was treated with IV prochlorperazine 12.5 mg every 6 hours as needed.
While increasing the DHE dosage according to established protocol, the nausea persisted and IV promethazine 12.5 mg every 6 hours PRN was added to her regimen as a second-line anti-emetic. She received a total of 6 doses of IV promethazine during days 2 and 3 of her admission. On day 3 of admission, the patient developed acute pain around the midline catheter insertion site during infusion of IV DHE, approximately 5 hours after the most recent promethazine dose. Examination of her right upper extremity revealed active extravasation in the surrounding tissue, a weak brachial pulse, and patchy numbness in her right hand. Grip strength was reduced in the right hand although the examination was limited by pain. The infusion was immediately stopped and her midline catheter was removed.
A right upper extremity venous Doppler ultrasound revealed a superficial occlusive thrombus in the proximal right basilic vein. She was started on therapeutic dosing of intramuscular enoxaparin. An arterial Doppler ultrasound showed arterial wall thickening and evidence of moderate to severe stenosis in the proximal right brachial artery in the region of DHE infiltration (Figure 1). There was no evidence of vasospasm or stenosis in other arteries of both upper extremities. The medical toxicology and vascular surgery services were consulted and she initially received conservative management with topical nitroglycerin paste along the extravasation site. However, her symptoms persisted and she was transferred to the surgical intensive care unit for treatment with intravenous nitroprusside drip and subcutaneous phentolamine along the course of the right brachial artery. Showing no demonstrable improvement, she underwent an angiogram confirming vasospasm (Figure 2), leading to balloon angioplasty and direct intra-arterial injection of nitroglycerin into the right brachial artery with improvement of blood flow on day 5. Following the procedure, the patient had near complete resolution of her sensory symptoms. An arterial Doppler ultrasound performed 3 weeks after discharge demonstrated nearly full resolution of right brachial artery stenosis and no other areas of vasospasm or stenosis. Ultrasound of the proximal right brachial artery demonstrating wall thickening and stenosis (arrow). Catheter angiography demonstrating severe stenosis (arrow) of the proximal right brachial artery prior to balloon angioplasty.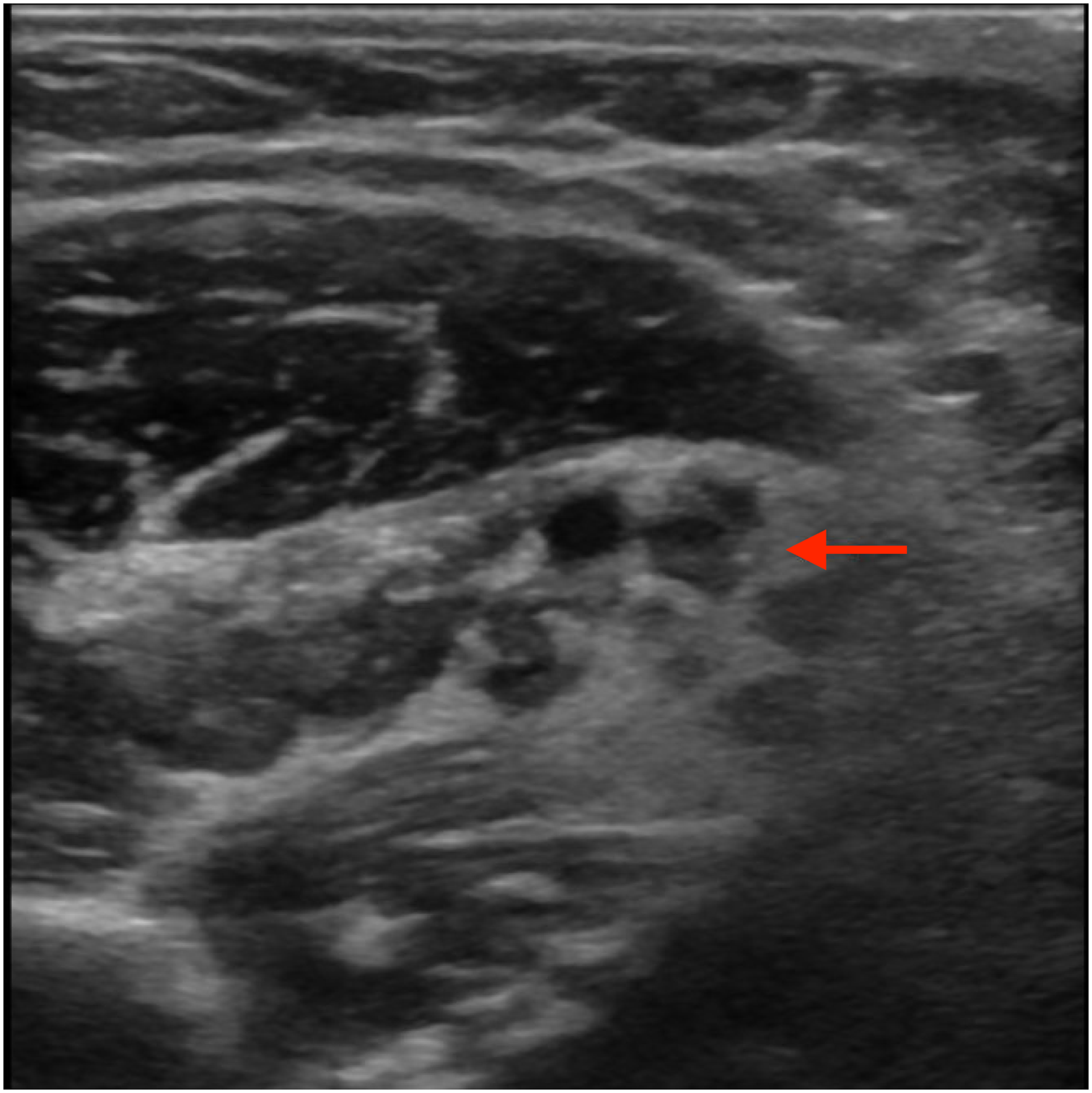

Discussion
Dihydroergotamine is a derivative of ergotamine, an ergot alkaloid. One proposed mechanism of action of this drug is vasoconstriction of the intracranial extracerebral blood vessels mediated by serotonergic 5-HT1B receptors. 1 Current guidelines in the United States and France list DHE and triptans as first line treatment for moderate to severe migraine attacks. 2 Although DHE is generally well tolerated, there are rare reports of both cerebral and limb ischemia with the use of this medication at high concentrations; to our knowledge, there are no reports of local DHE extravasation as the sole mechanism of injury.3,4,5 In addition, vascular complications such as deep venous thrombosis appear to be higher in midline and peripherally inserted central catheter (PICC) administration as compared to peripheral IV catheter infusion. 6 Promethazine, on the other hand, is highly caustic to the intima of blood vessels due to its acidic profile. In fact, due to the frequency of serious injuries after infiltration or inadvertent intra-arterial injection, the Institute for Safe Medication Practices (ISMP) recommended the FDA re-examine the product labeling and consider eliminating the IV route of administration. 7
We hypothesize that the use of IV promethazine resulted in direct caustic injury to the brachial vein in our patient. This predisposed her to the extravasation of DHE through the midline catheter, which in turn caused adjacent brachial artery vasospasm. In a separate case, IV DHE was reported to cause peripheral artery vasospasm in a patient that also had Raynaud phenomenon and received IV promethazine, though no extravasation was noted and multiple arteries were affected, suggesting a more systemic reaction to the DHE. 8 In contrast, in our patient the presence of focal arterial vasospasm only in the area immediately adjacent to the DHE extravasation suggests local effect of the extravasated DHE rather than a systemic process. Though it is unknown if Raynaud phenomenon could predispose to this as well, it is not likely that the Raynaud contributed to the initial extravasation. Finally, although IV promethazine has an long elimination half-life of up to 19 hours, it is not likely that promethazine itself caused the vasospasm because there was no sign of extravasation during the last promethazine infusion, and symptoms and signs of extravasation and vasospasm began during DHE infusion approximately 5 hours after the last promethazine injection. Regardless, given the known risk of arterial vasospasm with DHE, we recommend avoiding the concurrent and sequential administration of IV promethazine due to the risk of vessel injury and subsequent arterial vasospasm. It is also worth noting that recent reviews of inpatient headache treatment experiences do not report promethazine use in any formulation, suggesting that it is already not used in standard practice at some institutions.9,10 Alternative antiemetics and administration routes can be considered, including intramuscular (IM) promethazine, IV or IM prochlorperazine, and IV or IM ondansetron, as well as oral formulations if tolerated. If IV promethazine must be used concurrently with DHE then it is recommended to administer it through a separate IV line.
Supplemental Material
Supplemental Material - Brachial Artery Vasospasm From Sequential Use of Intravenous Promethazine and Dihydroergotamine for Treatment of Status Migrainosus: A Case Report
Supplemental Material for Brachial Artery Vasospasm From Sequential Use of Intravenous Promethazine and Dihydroergotamine for Treatment of Status Migrainosus: A Case Report by Christopher Johns, Rumyar Ardakani, Rohit R. Das, Deborah I. Friedman, and Alexander Frolov in The Neurohospitalist.
Footnotes
Acknowledgements
The authors thank Dr Vincent Parenti, MD for his help in reviewing the figures for this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Friedman serves on a speakers bureau and advisory boards for Impel Pharmaceuticals and has no other relevant conflicts of interest to report.
Informed Consent
An informed consent for publication of a case report was obtained from the patient described in this report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.