
Abstract

A 74-year-old female with known primary hyperparathyroidism presented with acute headache and altered level of consciousness. On examination she was normotensive with altered sensorium and repetitive episodes of left arm clonic movement concerning for epilepsia partialis continua. Laboratory evaluation revealed elevated serum calcium-total of 3.49 mmol/L (2.20-2.55 mmol/L) with intact parathyroid level 119.72 pmol/L (1.6-6.9 pmol/L) and creatinine 241 mmol/L (55-100 mmol/L). Magnetic resonance imaging (MRI) of the head revealed T2-weighted fluid-attenuated inversion recovery (FLAIR) hyperintensities involving bilateral occipital cortical-subcortical regions, right posterior limb of the internal capsule and thalami, and frontoparietal cortices (Figure 1A-C). Corresponding patchy restricted diffusion was also seen (Figure 1D-F). Intracranial MR angiogram findings were normal. Radiographic abnormalities resolved completely on repeat imaging 1 month later (Figure 1G-I). A diagnosis of Posterior Reversible Encephalopathy Syndrome (PRES) secondary to hypercalcemia was made and parathyroidectomy was performed. Her serum calcium normalized but residual deficits included left visuospatial neglect and left hemiparesis.
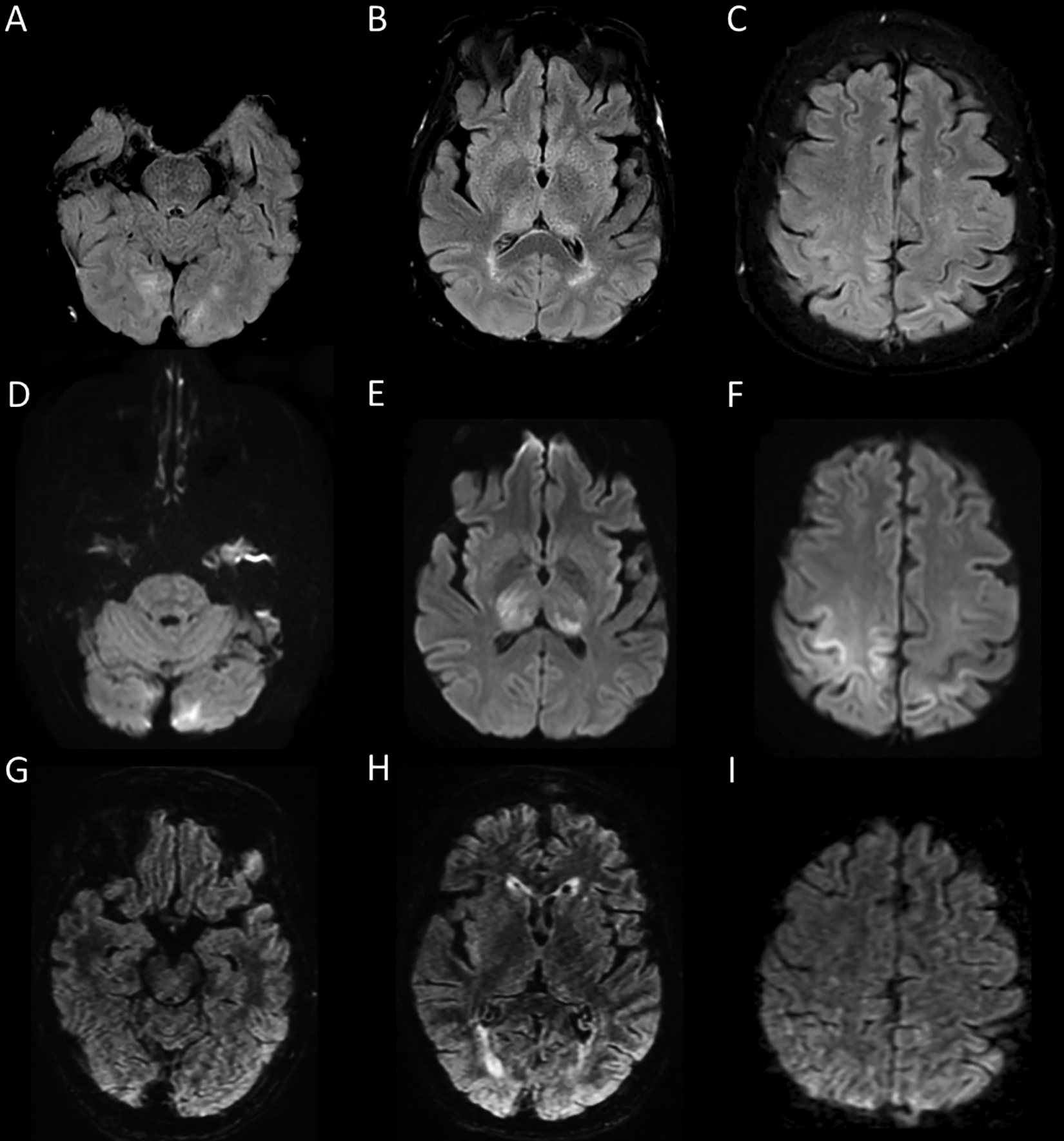
Brain MRI findings in hypercalcemia-associated PRES. Axial T2-weighted FLAIR imaging shows hyperintensities involving bilateral occipital cortical-subcortical regions (A), right posterior limb of the internal capsule and thalami (B), and frontoparietal cortices (C). Axial diffusion-weighted imaging shows corresponding hyperintensities (D-F), with associated apparent diffusion coefficient map hypointensities indicating true restricted diffusion (not shown). Axial T2-weighted FLAIR imaging performed 1 month later shows resolution of previously seen signal abnormalities (G-I).
A minority of patients with PRES will present with status epilepticus and focal neurological deficits. 1 Hypercalcemia is rarely associated with PRES and may occur alongside other risk factors such as hypertension and renal failure. 2 The pathophysiology may be due to varying degrees of calcium-induced vasospasm and endothelial injury 2,3 however there were no vessel abnormalities to suggest the former in our case. A predominantly parieto-occipital pattern of abnormalities on neuroimaging is classic of PRES 3 while restricted diffusion is associated with incomplete clinical recovery. 4
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.