
Abstract
Context:
Previous research has demonstrated that using a multicomponent approach to ankle injury preventions can significantly reduce ankle injuries; however, these studies lack specific intervention recommendations.
Objective:
To evaluate the exercise components of prevention programs on ankle injuries specifically in high school athletes. Secondary objectives were to assess the overall effectiveness of prevention programs on ankle injuries in this population and how compliance and education may impact success.
Data Sources:
A total of 5 databases were searched through September 26, 2022.
Study Selection:
Study inclusion criteria included randomized control trials (RCTs) investigating exercise interventions in high school athletes aged 13 to 19 years, participation in sports competition, reporting of injury incidence, and specific exercise interventions used.
Study Design:
Systematic review and meta-analysis.
Level of Evidence:
Level 1.
Data Extraction:
Pooled overall ankle injury incidence rate ratio and 95% CIs were calculated using random-effects meta-analysis.
Results:
A total of 10 studies were included, of which 9 used multicomponent exercise interventions and 1 used only balance training. Of the 10 studies, 3 demonstrated statistically significant reduction in ankle injuries. When data from all 10 studies were pooled and analyzed, there was a statistically significant overall reduction (incidence rate ratio, 0.74; 95% CI 0.60-0.91) in ankle injuries when comparing intervention groups with controls.
Conclusion:
The most effective injury prevention programs included multiple components, emphasized strengthening and agility exercises, and promoted high adherence to the intervention. The importance of coach and player education on how and why to perform an injury prevention program as well as the frequency and duration of programs was also important. Exercise-based injury prevention programs may reduce ankle injury incidence in youth athletes by 26% when pooling data from a multitude of sport types/settings.
Current estimates suggest that over 45 million children (5-18 years old) in the United States (US) participate in organized sporting activity; this equates to roughly 75% of US families with age-eligible children. 21 When looking at the benefits this provides for youth, research has shown that structured aerobic activity during adolescence is associated with improvements in body mass index, sleep, self-esteem, mental health, and peer engagement.10,16 While these benefits are remarkable, there is also inherent risk to participation in sporting activity. Two million sports-related injuries occur each year, with 500,000 high school aged persons receiving medical care. 18 In the emergency room, two-thirds of all sports-related visits are children, highlighting the need for more attention to the prevention of youth athlete injuries.21,25
The body parts in youth athletes injured most are the ankle and knee. 2 The most common injury types are contusions and strains. 7 Injury exposure rates in children, adolescents, and adults have been reported at 2.85, 1.94, and 0.74 per 1000 exposure hours, respectively. 9 The mean return-to-play time is 15 ± 19 days; however, severe injuries may take up to 105 days or even longer if surgery is required, and medical costs can be great. 8
One well-supported method to decrease the incidence of injuries is via the implementation of injury prevention programs.1,7,12,13,14,19,20,22,23,27,29 It has been shown that injury prevention programs can reduce injuries by 28% to 80% and that these programs can be successful in youth and young adults when performed for as little as 20 minutes per week.11,30 However, many of these programs focus on the prevention of knee injury or general lower extremity injury and do not report significance for ankle injury prevention. Currently, injury prevention programs focused on the ankle have been shown to be effective at reducing ankle injury rates in nonspecific populations of adult soccer players and in female athletes in general, yet there are no systematic reviews that specifically evaluate the effectiveness or analyze the components of ankle injury prevention programs across a multitude of youth sports.5,15 Two studies have shown that ankle injuries can be reduced in youth athletes; however, these studies were limited to a smaller variety of sports, did not isolate intervention components, or did not isolate this particularly vulnerable age group.13,24
Previous research has demonstrated that using a multicomponent approach to ankle injury prevention can significantly reduce ankle injuries; however, these studies lack specific intervention recommendations. Furthermore, previous systematic reviews for this age group and body region have not provided recommendations for coach education, compliance rates, and overall time required to significantly reduce injury risk. The primary aim of this study was to systematically review the components of injury prevention programs being performed with a variety of high school athletes to determine what coaches and players can best implement in an injury prevention program to reduce risk of ankle injury. Our secondary aim was to determine the overall effectiveness of ankle-specific injury prevention programs across a range of youth sports.
Methods
Search Strategy and Selection Criteria
This systematic review is reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. A systematic literature search was completed in Ovid (Medline), CINAHL, Cochrane Library, PubMed, and Scopus databases from inception until September 26, 2022. The search strategies were completed by a reference librarian and peer reviewed by the other members on the systematic review project team. The search strings were an expanded version of “(injury OR risk) AND (proprioception OR exercise) AND (athletes OR sports) AND (lower extremity OR ankle)” to find relevant literature on the topic. The search strategy in each database included a combination of keyword and subject heading terms, synonymous terms, adjacency searching, and truncated terms. Limiters were applied to the search, if available, to include articles focusing only on the adolescent age group population (age, 13-19 years). The search strings were altered to fit the functionality and subject heading availability of the search interface of each database. The full search strategies for each database can be found in the Appendix (available in the online version of this article).
Inclusion criteria included randomized controlled trials (RCTs) of exercise interventions on high school athletes between 13 and 19 years old that reported ankle injury incidence data, participation in ≥1 sporting competition or practice yearly, specific exercise components, and were published during or after 2005. Exclusion criteria included studies that involved collegiate, amateur league, or professional level competition. Only full-text articles published in English were included in this review. Targeted searching of reference lists was also performed to identify any articles not found using the database search strategy.
Study Selection, Data Extraction, and Quality Assessment
Two reviewers independently screened all titles and abstracts of the received search results. A full-text review of possibly relevant articles was performed and compared against selection criteria to determine the final list of included articles. These reviews were also hand searched for additional research included in article references.
The reviewers independently extracted data from included articles. Data extracted for the primary aim included number of participants (total and per study group), participant age, sport team or population, and details of the intervention. For the primary aim, the number of injuries were extracted for reported “overall injuries” and injuries specific to the ankle joint (injury per 1000 exposure hours).
Two reviewers independently extracted data for the secondary aim related to frequency of the interventions and componentry of each intervention, which was categorized into 1 of 6 components (agility, balance, mobility, plyometrics, strength, and running). In addition to the training components, delivery of coach and player education along with compliance data to the injury prevention program were extracted. Each study was classified as including a component if it described ≥1 activity that fit the description for that component. If studies had unclear reporting of the intervention, referenced work of the intervention was examined where available.
Two reviewers independently assessed the methodological quality of included studies using the Physiotherapy Evidence Database (PEDro) scale. A third reviewer was consulted to resolve any discrepancies in scoring. For each included study, based on PEDro clinimetric properties, each study was then rated as overall poor, fair, good, or excellent. Cohen’s kappa was calculated to assess the extent of agreement between reviewers for the 7 domains, where a kappa of 0.61 to 0.80 was deemed good agreement and ≥0.80 as very good. 7 Any discrepancies for study selection, data extraction, and quality assessment were initially resolved through discussion and mutual consensus, with a third reviewer consulted if consensus could not be reached.
Quantitative Synthesis
Data were pooled from all 10 studies for the meta-analysis. To examine the effects of the ankle injury prevention programs on overall injury rates, the pooled overall injury incidence rate ratio (IRR) and 95% CIs were calculated using random-effects meta-analysis. Comprehensive meta-analysis was used to calculate the pooled estimates. A forest plot was generated to allow visual representation of each study included in the meta-analysis and the pooled estimate. Between-study statistical heterogeneity was evaluated for our outcome using the standard I 2 statistic (ie, the percentage of variability in prevalence estimates that is due to heterogeneity rather than chance, 0%, no inconsistency; 100%, maximal inconsistency) and Cochran’s Q with a significance threshold of P < 0.05. 17
Results
Search Results
The search strategy originally retrieved 5042 articles, which was then narrowed down to 10 articles based on meeting the study selection criteria (Figure 1). During the full-text review, 2656 duplicate studies were removed, 2386 studies were screened for title and abstract, and 89 studies were selected for the full-text review. A total of 79 studies did not meet the inclusion criteria due to lack of intervention specifics, wrong study design, or wrong age range. The remaining 10 studies were included in the quantitative analysis.
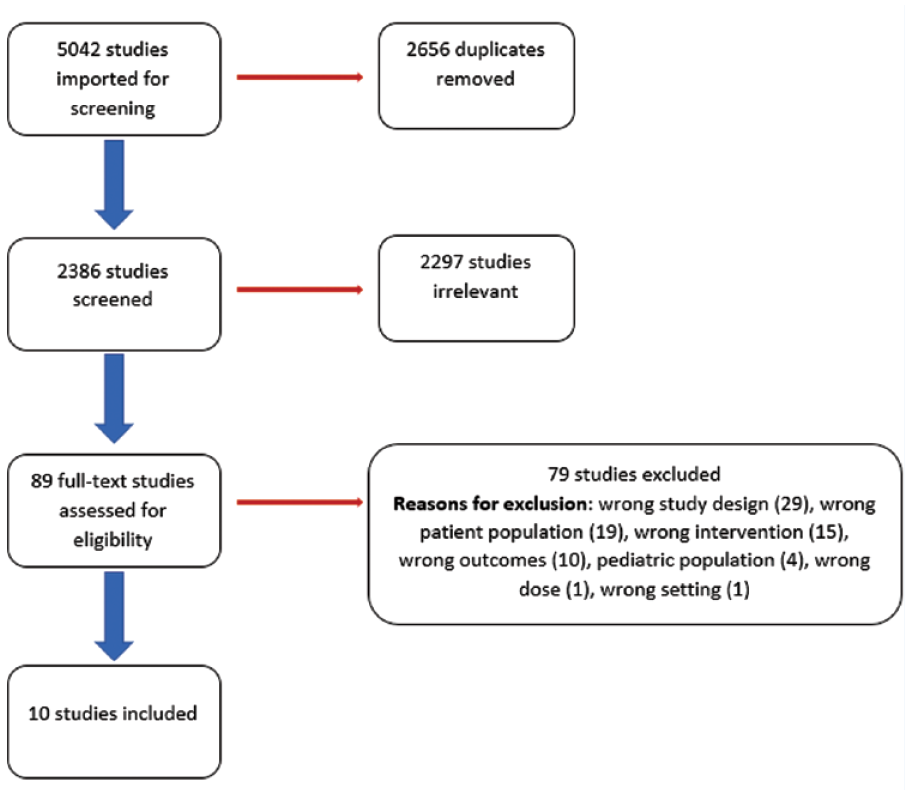
Flowchart of study inclusion and exclusion.
Study Characteristics
The sample size of included studies ranged from 279 to 3611 participants (Appendix 2, online). A total of 4 studies were conducted in Europe, 4 in the US, 1 in Africa, and 1 in Canada; 4 studies involved club soccer, 4 involved multiple high school sports, and 2 studies were conducted with handball athletes. Of the 10 studies, 4 included female athletes only, 2 included only male athletes, and 4 included both sexes.1,11,14,19,20,22,23,26,27,29 Intervention adherence data and information on educational resources provided to the teams for each study are reported in Appendix 3, online.
Quality Assessment
The PEDro risk of bias scores are presented in Table 1, which includes individual numerical rating as well as risk of bias scores based on validated research. 6 Of the 10 studies included, 8 received a score of “great,” 1 received a score of “excellent,” and 1 received a score of “fair” overall, indicating that risk of bias was not high among the included studies. 7 Cohen’s kappa was 0.83, which indicates a near perfect strength of agreement between reviewers.
PEDro analysis
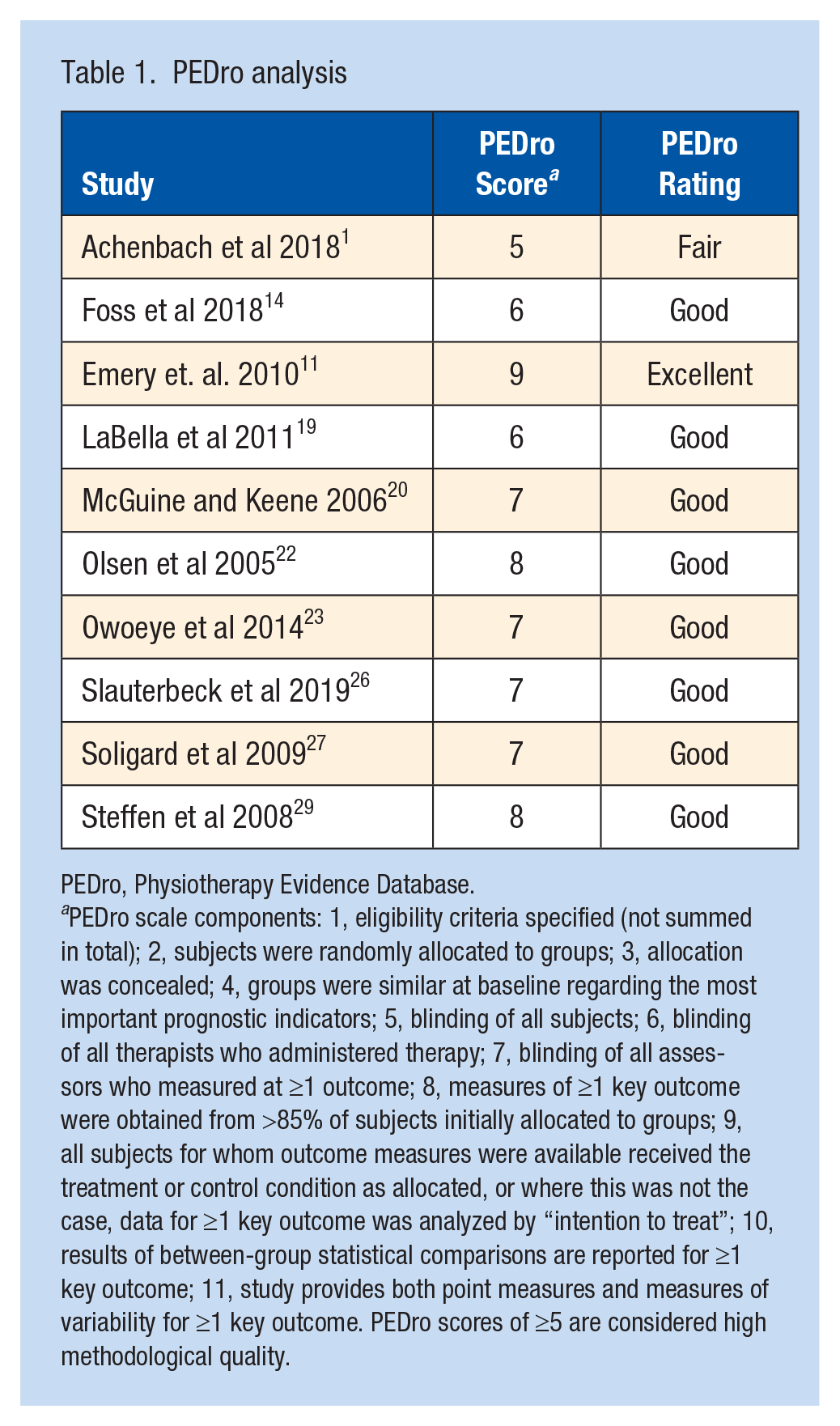
PEDro, Physiotherapy Evidence Database.
PEDro scale components: 1, eligibility criteria specified (not summed in total); 2, subjects were randomly allocated to groups; 3, allocation was concealed; 4, groups were similar at baseline regarding the most important prognostic indicators; 5, blinding of all subjects; 6, blinding of all therapists who administered therapy; 7, blinding of all assessors who measured at ≥1 outcome; 8, measures of ≥1 key outcome were obtained from >85% of subjects initially allocated to groups; 9, all subjects for whom outcome measures were available received the treatment or control condition as allocated, or where this was not the case, data for ≥1 key outcome was analyzed by “intention to treat”; 10, results of between-group statistical comparisons are reported for ≥1 key outcome; 11, study provides both point measures and measures of variability for ≥1 key outcome. PEDro scores of ≥5 are considered high methodological quality.
Effects of Prevention Programs on Ankle Injuries
Table 2 reports key differences in ankle injury rates between control and intervention groups. This table includes data on the number of participants analyzed, total player exposure hours, overall injuries, ankle injuries, and ankle injuries per 1000 exposure hours. Three of the studies reported data in athlete exposure (AE), which we adjusted by assuming that 1 AE equaled 2 exposure hours as was done in previous literature.7,14,19,20,22,23,26 Figure 2 shows that there was a statistically significant reduction of 26% in the rate of ankle injuries per 1000 exposure hours in favor of injury prevention programs compared with control conditions (IRR 0.74, 95% CI 0.60-0.91). There was moderate between-study statistical heterogeneity (I 2 , 39%; Q, 0.09).
Ankle injury rates
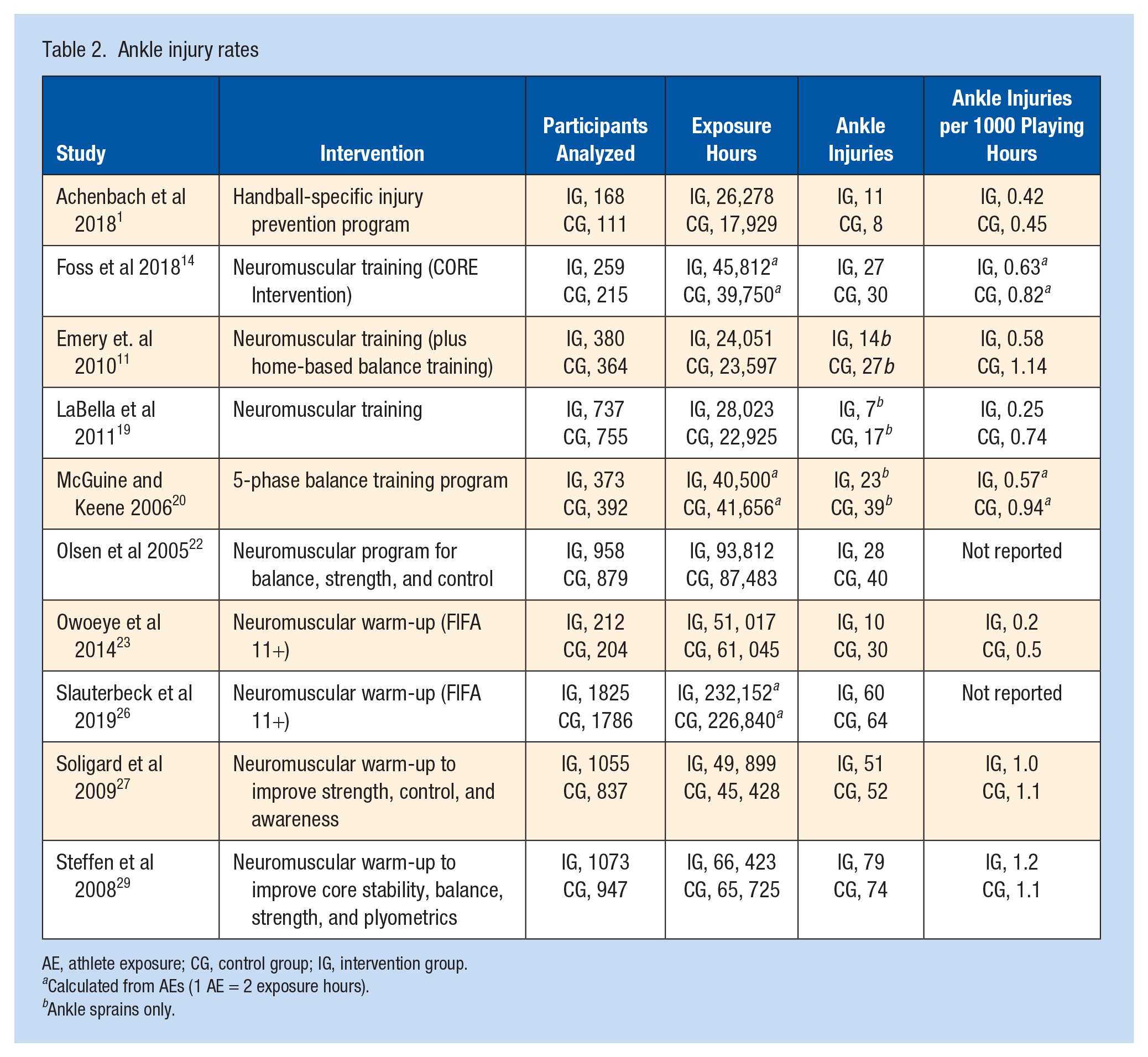
AE, athlete exposure; CG, control group; IG, intervention group.
Calculated from AEs (1 AE = 2 exposure hours).
Ankle sprains only.
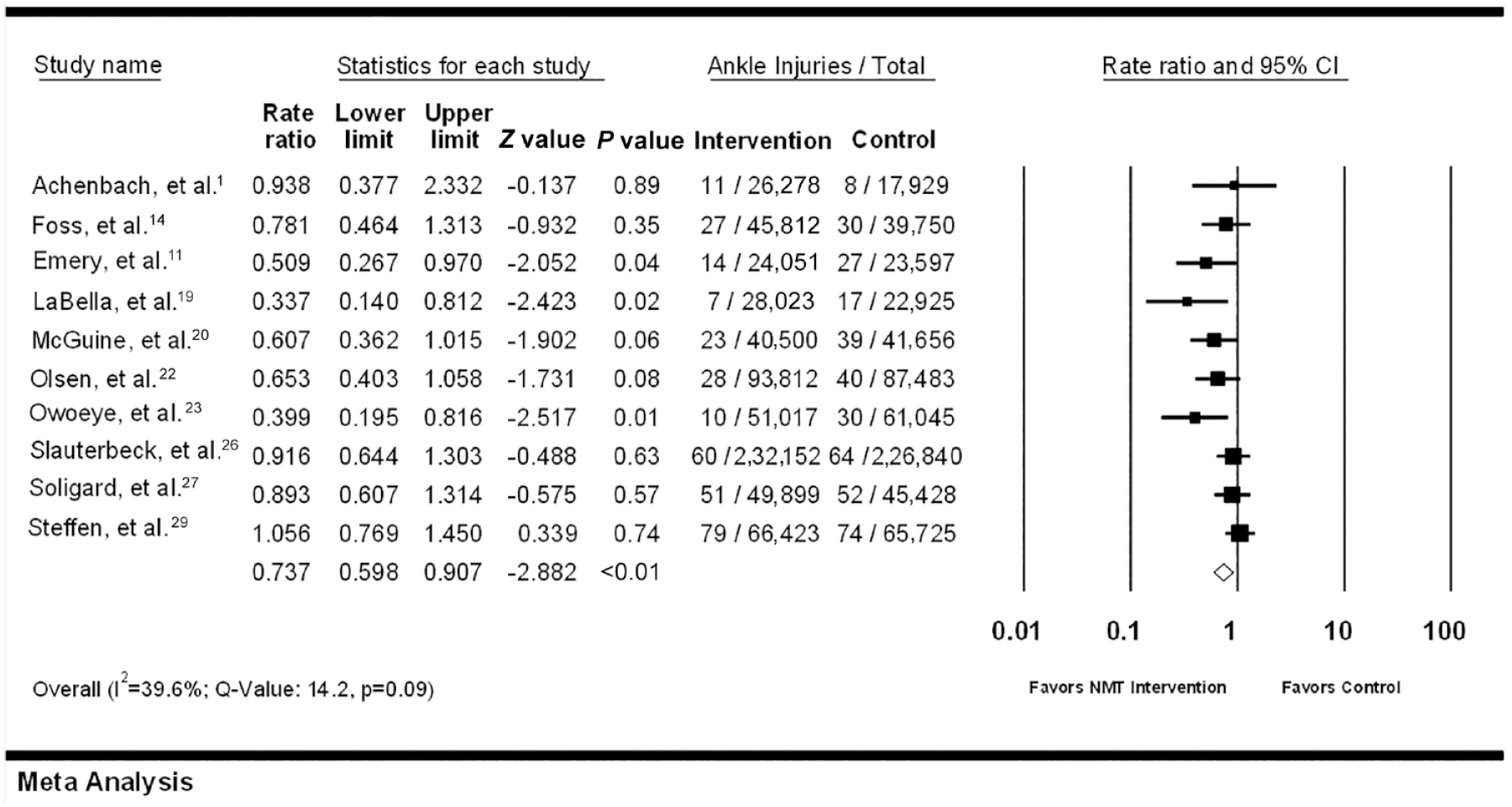
Meta-analysis describing the injury prevention effect reported by each study. Horizontal lines through the boxes demonstrate data within the 95% CI. The diamond describes the combination of all raw pooled data for injury risk reduction ratio, with its boundaries representing the 95% CI.
Physical Components of the Interventions
Table 3 indicates which components of injury prevention were included in each intervention. Overall, 9 of 10 programs included balance, 7 of 10 programs included an aerobic component, and 5 of 10 programs included an agility component.1,11,14,19,20,22,23,26,27,29 Of the 10 programs, 7 demonstrated sufficient parameters (defined in Table 3) for power/plyometrics, and 6 of 10 programs showed proper parameters for strength. The 3 programs that demonstrated statistically significant improvement in ankle injury reduction all incorporated a strengthening and an agility component. Two additional studies were near the cut-off (P = 0.06, P = 0.08) for statistical significance in injury reduction; 1 of these included a program of only balance interventions whereas the other program included all 5 domains.20,22
Intervention characteristics a
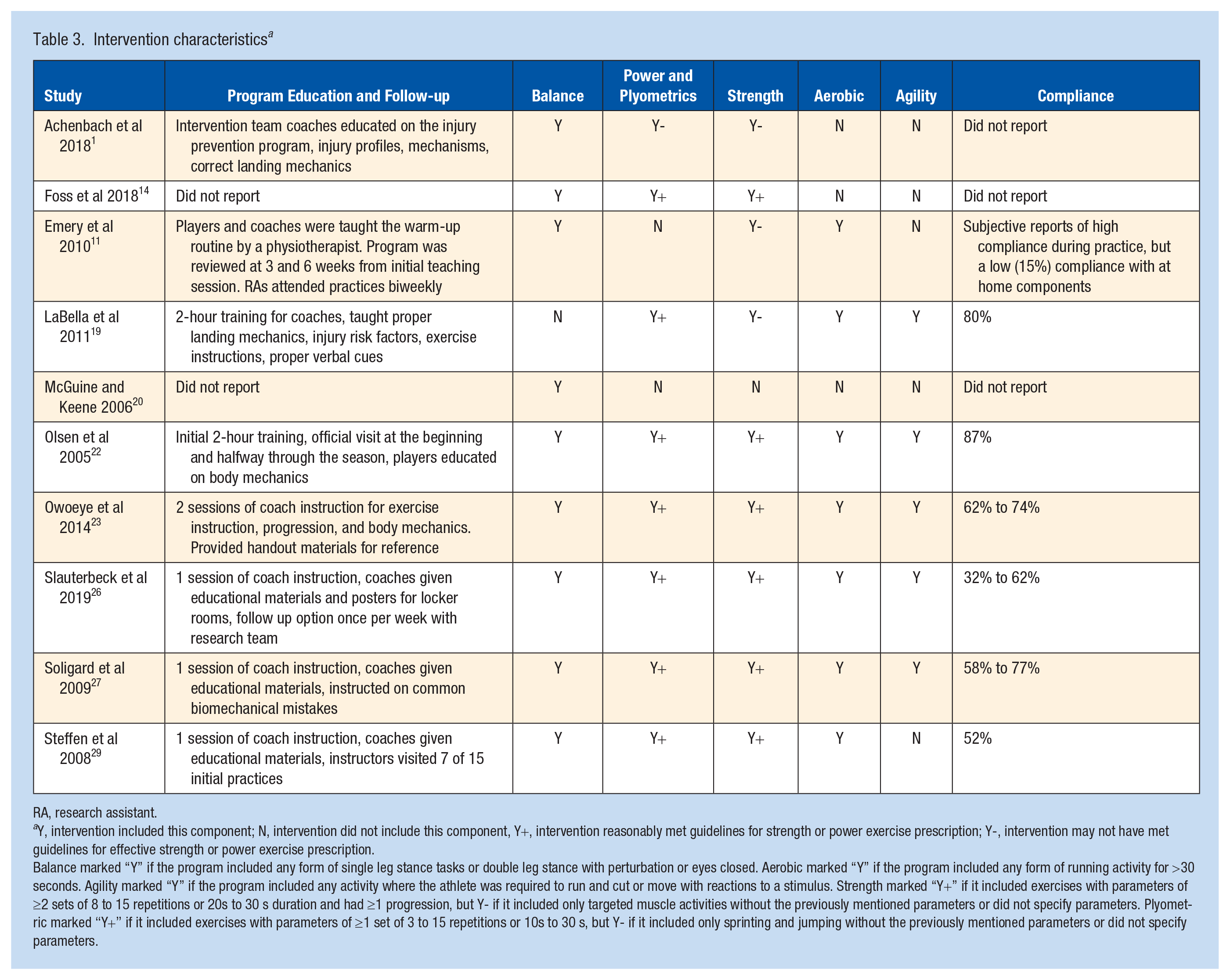
RA, research assistant.
Y, intervention included this component; N, intervention did not include this component, Y+, intervention reasonably met guidelines for strength or power exercise prescription; Y-, intervention may not have met guidelines for effective strength or power exercise prescription.
Balance marked “Y” if the program included any form of single leg stance tasks or double leg stance with perturbation or eyes closed. Aerobic marked “Y” if the program included any form of running activity for >30 seconds. Agility marked “Y” if the program included any activity where the athlete was required to run and cut or move with reactions to a stimulus. Strength marked “Y+” if it included exercises with parameters of ≥2 sets of 8 to 15 repetitions or 20s to 30 s duration and had ≥1 progression, but Y- if it included only targeted muscle activities without the previously mentioned parameters or did not specify parameters. Plyometric marked “Y+” if it included exercises with parameters of ≥1 set of 3 to 15 repetitions or 10s to 30 s, but Y- if it included only sprinting and jumping without the previously mentioned parameters or did not specify parameters.
Tactical Components of the Interventions
All 3 of the statistically successful interventions were performed with soccer players, both male and female. These 3 studies reported 62% to 80% or subjectively “high compliance.”11,19,23 The highest compliance reported across all 10 studies was 87% in a study that produced successful reduction in ankle injury rates, but with limited statistical significance (P = 0.06). 22 Of these 3 programs, 1 demonstrated significantly improved injury ankle rates with the FIFA 11+ in youth soccer; however, another study showed that the FIFA 11+ does not guarantee ankle injury rate reduction when implemented across a multitude of sports via school athletic trainers.23,26
Discussion
Among youth team sports, we found an overall statistically significant protective effect for using injury prevention programs to reduce ankle injury rates. Out of 10 studies included in this review, 9 incorporated multiple exercise-based components; 1 study included only balance exercises as a part of the intervention. Out of 10 programs in this review, 3 had a statistically significant reduction in ankle-related sports injuries.11,19,23 All 3 of these studies included interventions incorporating multiple exercise-based components. Two other studies demonstrated trends toward improving ankle injury incidence but did not meet statistical significance.20,22
Effects of Injury Prevention Programs
Our report supports that implementation of injury prevention programs may reduce the rate of ankle injuries across a variety of youth sports by 26% when compared with no injury reduction program. Previous literature has shown that exercise interventions can be effective at reducing injury rates for general lower extremity injuries, ankle injuries (including Achilles tendonitis), and knee injuries (including patellar tendonitis). Our findings demonstrate confidence that these programs may also be effective specifically for preventing youth ankle injuries.5,7,12,13,15 While the 3 strongest studies included were conducted with soccer athletes, combined data from all articles included suggest that these ankle injury prevention programs may still be effective across a spectrum of youth sport athletes and may provide a financial benefit of up to an 8.2-fold return on investment. 3
Components of Successful Programs
Of the studies that presented positive trends toward reducing ankle injury, there was a wide variety in the number of included components, with only 2 programs including all 5 domains.11,19,20,22,23 In the 3 programs that demonstrated statistical significance in favor of the intervention, the only common elements were the inclusion of strengthening exercises, agility exercises, and utilizing a multicomponent approach.11,19,23 Similarly, Brunner et al 4 also found that strengthening is a key component of ankle injury prevention programs. Across all analyzed programs included in this review, there were no specific exercises or parameters of duration or intensity that were identified to be more beneficial in improving ankle injury reduction. Previous reviews have supported that multicomponent interventions are the most successful; whereas this is in agreement with the findings in this current study, there does not appear to be a specific combination of intervention components that provide the best results for reducing injury.5,7,20 One particular injury prevention program that is frequently cited in the literature is the FIFA 11+, which includes all of the 5 components we analyzed and was included in studies analyzed in this review. This program has been shown previously to make a significant impact on general lower extremity injuries in youth soccer. 23 When applied across a variety of high school sports, the FIFA 11+ had limited effect and did not demonstrate statistical significance in ankle-specific injury reduction 26 ; however, it is worth noting that the program was impmlemented by school athletic trainers who may have been constrained by time to ensure proper teaching and compliance. Overall, it provides a great framework for coaches and players to build their own injury prevention program with the other guidelines set in this review.
Duration of Injury Prevention Programs
Programs were most likely to be successful when implemented in both 15-minute and 20-minute blocks and utilized at least twice per week.11,19,23 Previous literature focused on generalized lower extremity or knee injury prevention has also reported success with intervention dosage of 20 to 30 minutes across 2 or more exercise sessions per week.5,12,30 There was no difference in success when programs were initiated during the preseason or in-season; however, utilizing a program for 3 to 6 months showed the best results.11,19,23 Other systematic reviews analyzing injury prevention programs have demonstrated timelines of >6 weeks to be more beneficial, but durations >6 months in length did not produce more favorable outcomes.13,30
Demographics
Both male and female athletes participating in soccer showed significant success with ankle injury reduction programs, regardless of implementation in a school or club setting, and there is a positive trend toward injury reduction in indoor sports such as basketball and handball players.11,19,20,22,23 Through all 10 studies, athletes age 16 to 18 years presented with the most successful reduction in ankle injuries by following prevention programs.11,19,20,22,23
Compliance
Rate of compliance was an important consideration for successful versus nonsuccessful programs. The programs that demonstrated higher success also reflected higher compliance when compared overall with programs that did not have success with injury reduction.11,19,22,23,26,27,29 This finding is also supported by Caldemeyer et al, 5 who reported that compliance is one of the key elements of a successful injury prevention intervention. Although no conclusions can be drawn about the minimum compliance required for injury reduction, studies analyzed by Caldemeyer et al 5 and in this review support that compliance rates of >62% have a higher likelihood of success. These compliance rates appear to be independent of the frequency or duration of the program; there has been high compliance reported in 2 times per week programs as well as in programs that perform prevention programs every practice.19,23
Coach and Player Education
Although there was no association between the success of injury prevention and how coaches/players were educated in our 10 included studies, it is worth mentioning that other authors have reported the importance of coach education. Steffen et al 28 found that formal coach education did improve compliance with injury prevention programs. In addition, Emery et al 12 recently reported a slight increase in compliance for teams that received a once-per-week visit from researchers to observe the intervention. This trend was also identified in the 10 articles included in this study, with several programs showing higher compliance when they reported more frequent communication between teams and researchers that specialized in the given injury prevention program.11,19,22 Based on these findings, it appears that it may be beneficial for coaches to receive a 2- to 3-hour in-person workshop to help implement these programs and identify errors in their players. Furthermore, if resources are available, it may benefit teams to have a specialist (trained physical therapist, athletic trainer, or strength and conditioning coach) who is well versed in injury prevention to visit teams once per week and be available to be contacted by coaches or players that have questions.
Clinical Implications
These findings support that clinicians should utilize or educate others on the use of injury prevention programs to prevent ankle injuries in youth sports. Programs should include a strengthening and agility component and must emphasize the importance of compliance. Clinicians should inform athletes and coaches that these programs work best to prevent injury when they are performed ≥30 minutes per week and for >6 weeks, but that an increase in frequency and duration may not be beneficial. Still, a more detailed understanding of the best approaches to implementing injury prevention programs in this population is needed - and would begin to address existing gaps in this literature.
Limitations
This current study has limitations due to inconsistent definitions, method of reporting of injury, use of AEs and exposure hours, and lack of clear control group guidelines. The strict inclusion and exclusion criteria used for this study may been another limitation as studies that did not specifically outline the intervention, were quasi-experimental, or had a large age range of the subjects that included adult participants were excluded. In addition, our search string included only English language studies. Large CIs may indicate uncertainty in the results of the included studies. This may be due to the nature of reporting and how injury types were classified. It is also important to note that the pooled effect of the meta-analysis was influenced significantly by a few studies with large sample sizes; only 3 of the 10 studies reported significant ankle injury reduction with the implementation of an injury prevention program.19,24
The definition of ankle injuries is unclear and could refer to only ankle sprains or include other injury types such as fractures and tendinopathies.1,14,23,26,27,29 Intervention crossover may also have occurred into the control groups as many of the included RCTs did not have specific guidelines for the control groups.1,19,20,22,23,26,27,29 Coaches and athletes may have been exposed to additional interventions or injury prevention techniques and used them as a part of their normal warm-up. The lack of separation between match and training injuries and the use of AEs can influence the overall IRR reported. With the conversion of AEs into 2 playing hours, it is difficult to control for players who attended matches but did not get the full on-field playing time for that match. This could lead to the under-reporting of injury incidence as each AE was likely <2 hours. Using a shorter duration for each AE (60 or 90 minutes) in the studies that reported using AEs would have resulted in higher injury incidence. 7 Finally, when grading the quality of the RCTs using the PEDro scale, there are inherent limitations in evaluation of injury prevention programs because of the inability to blind participants.
Strengths
This review included comprehensive searches of 5 major databases conducted by a reference librarian. Also, this topic is relevant to the health and safety of adolescent athletes who are particularly vulnerable to ankle injury.
Conclusion
This study is the first of its kind to analyze the impact of ankle-specific injury prevention programs across a wide range of youth sports and provide recommendations for generalizable implementation of these programs. There is high-quality evidence that demonstrates targeted injury prevention programs may reduce ankle injuries in youth sports. Currently, the best methods for reducing ankle injury are utilizing exercise programs that emphasize agility, strengthening, and compliance.1,11,14,19,20,22,23,26,27,29 Injury prevention programs may have an added benefit when coaches and players are formally educated on the injury prevention programs and are monitored throughout the season by external professionals.12,28 Reducing injuries can help prevent costly medical bills for teams and players, and it may promote the continuation of healthy aerobic activity for youth. Implementing preventive programs requires a sacrifice of time for the coaches and players, but proper programing and coach education will optimize player performance and participation by best protecting players from injury. Preventative programing can substitute for a team’s traditional warm-up and reduce injury sufficiently with as little as 30 minutes of their time per week.
Future research needs to be conducted to determine the most efficient type of coach education, the methods that can improve compliance in youth athletics, the effects of supervised and unsupervised injury prevention programs, and assessment of the most important injury prevention components specific to individual sports.
Supplemental Material
sj-pdf-1-sph-10.1177_19417381241231588 – Supplemental material for Ankle Injury Prevention Programs for Youth Sports: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-sph-10.1177_19417381241231588 for Ankle Injury Prevention Programs for Youth Sports: A Systematic Review and Meta-analysis by Ryan Berkey, Afsar Sunesara, Lindsay Allen, Ryan Pontiff, Alison DeVries and Steve R. Fisher in Sports Health
Supplemental Material
sj-pdf-2-sph-10.1177_19417381241231588 – Supplemental material for Ankle Injury Prevention Programs for Youth Sports: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-2-sph-10.1177_19417381241231588 for Ankle Injury Prevention Programs for Youth Sports: A Systematic Review and Meta-analysis by Ryan Berkey, Afsar Sunesara, Lindsay Allen, Ryan Pontiff, Alison DeVries and Steve R. Fisher in Sports Health
Supplemental Material
sj-pdf-3-sph-10.1177_19417381241231588 – Supplemental material for Ankle Injury Prevention Programs for Youth Sports: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-3-sph-10.1177_19417381241231588 for Ankle Injury Prevention Programs for Youth Sports: A Systematic Review and Meta-analysis by Ryan Berkey, Afsar Sunesara, Lindsay Allen, Ryan Pontiff, Alison DeVries and Steve R. Fisher in Sports Health
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.