
Abstract
Context:
Male amateur marathon runners represent a unique subset of the population who may be at increased risk of cardiovascular disease (CVD) due to their underlying risk factors and their involvement in vigorous exercise such as marathon running.
Objective:
To assess the modifiable risk factors (MRFs) of CVD in experienced male amateur marathon runners and health interventions on CVD risk factors.
Data Sources:
CINAHL, Cochrane Library, Embase, Medline, and SPORTDiscus.
Study Selection:
Studies selected according to the inclusion criteria.
Study Design:
Systematic review.
Level of Evidence:
Level 3.
Data Extraction:
The publication dates included were from June 1, 2008 to February 29, 2020.
Published primary epidemiological, observational, randomized controlled trial (RCT) and/or non-RCT studies assessing the MRFs of CVD and health interventions on CVD risk factors in male amateur marathon runners aged ≥18 years and written in the English language were included in the review.
Results:
Five studies met the inclusion criteria for analysis. These included male amateur marathon runners (n = 862), aged 42 to 77 years. Hypertension, hyperlipidemia, smoking, and alcohol use were MRFs positively associated with an increased risk of coronary atherosclerosis found in a subset of male marathon runners. No studies examined health interventions on CVD risk factors in any of the included studies. All 5 studies were of good quality from the National Heart, Lung, and Blood Institute quality assessment tools used. The risk of bias was low to moderate.
Conclusion:
There is a paucity of observational studies evaluating the CVD MRFs. Negative lifestyle behaviors exist within this population despite their engagement in physical exercise through marathon running. Marathon running does not negate the long-term effects caused by past negative lifestyle behaviors. This systematic review identifies that this population may not be aware of their possible risk of atherosclerosis and, consequently, CVD.
Cardiovascular (CV) disease (CVD) is the leading cause of premature death globally.49,62,63 CVD accounts for 3.9 million deaths in Europe annually. 62 Coronary artery disease (CAD) is the main cause of CVD morbidity and mortality in the western world. 59 More than 90% of CVD is attributed to preventable modifiable risk factors (MRFs), namely unhealthy diet, physical inactivity, tobacco use, excessive alcohol use, unhealthy body weight, high blood pressure (BP), hypercholesterolemia, and diabetes mellitus (DM).26,37,42,58
Physical inactivity is the fourth leading cause of mortality, contributing to approximately 6% of deaths globally.42,58,64,65 With 1 in 4 adults deemed insufficiently physically active, there is concern about the development or exacerbation of noncommunicable diseases such as CVD. 17 However, there is a debate on the dose-response relationship between physical activity and health outcomes.40,68 There are significant evidence-based pleiotropic CV protective benefits of physical activity, where modest physical activity has been shown to result in positive health outcomes as opposed to a sedentary lifestyle.42,58,65,68 Conversely, research has also found that excessive vigorous exercise may produce harmful CV effects in certain persons that may contribute to coronary atherosclerosis and atrial fibrillation.12,24
Health promotion campaigns for physical activity encourage people to exercise regularly where evidence-based research has shown it to reduce CVD morbidity and mortality.52,58 However, participants need to be cognisant of the potential liabilities of vigorous exercise and consider what is too much, too soon, and too fast before the risk becomes harmful to health. 52 Running is one of the most popular forms of physical activity and a growing trend in recessionary times. 52 The global participation rates in male amateur marathon running grew by 46.91% from 2008 to 2018. 50 According to a report on recreational marathon runners, a greater proportion of men (65.18%) than women (34.82%) participate in marathon running, with 41.90% of runners residing in Europe. 51 Evidence-based research has questioned the dose-response relationship between exercise and CVD outcomes, including the development of adverse CV outcomes such as CAD.11,25 Consequently, amateur athletes represent a unique subset of the population who may be at increased risk of CVD due to their underlying risk factors and their involvement in vigorous exercise. 10 Full marathons predispose participants to a greater health risk than half marathons.21,46 Age, level of fitness, physical demands, and CV health status all have an impact on the health of amateur athletes. 31 Neurohormonal activation, precipitating plaque rupture, hypercoagulability, and endothelial erosion have been linked to cardiac events during sports where these subclinical events can often go unnoticed as some participants may be asymptomatic.45,55,56
Men tend to experience greater negative health outcomes when compared with women as men do not access healthcare services as frequently as women.28,60,61,66 Consequently, they may present at a later stage for healthcare with medical issues that could have been prevented.42,58,60 This gender-based health disparity remains a challenging issue for healthcare professionals.42,58 Evidence from Denmark has found that the underutilization of primary care services by men has resulted in a financial strain on acute healthcare services. 6 Some sporting organisations are a useful medium by engaging with their participants and audience through the delivery of health education. 16 The male population who start to run in middle age may present with pre-existing MRFs and consequently be susceptible to undiagnosed CVD.12,21,67 Therefore, excessive vigorous marathon running may be a precipitating factor contributing to exercise-induced CV events.12,21
Current research has found that men are at a higher risk of experiencing sudden cardiac arrest and sudden cardiac death (SCD) while running a marathon and directly afterward when compared with women - a possible explanation for this difference being the earlier onset of atherosclerosis in men.21,30,42,44,47,58
Recent evidence has demonstrated that SCD in young athletes <35 years is caused by electrical and structural disorders of the heart such as cardiomyopathies, ion channel disorders, coronary anomalies, and acquired cardiac conditions.12,14 However, older recreational athletes ≥35 years have different CV risk factors and underlying medical conditions, mainly atherosclerotic CAD, which can consequently lead to CV events.12,48 Physiological parameters regarding CV strain and cardiac responses are amplified due to marathon participation, but the clinical implications for this population remain uncertain. 2
Worldwide, preparticipation CV screening is recommended for elite athletes but not routinely for amateur athletes. 34 However, undiagnosed atherosclerotic CAD is the predominant cause of exercise-related cardiac events in the older athlete (≥35 years). 34 There is ongoing debate surrounding routine preparticipation screening, with doubts expressed about its capacity to produce accurate results. 8 Established bodies such as the European Society of Cardiology (ESC) and the American College of Cardiology/American Heart Association (ACC/AHA) provide recommendations on CVD prevention within the world of sport.4,13,27,29,39,40 However, differences exist, due largely to the cultural, social, and legal backgrounds within Europe and America. 41 Preparticipation CV screening is recommended mainly for elite athletes <35 years or for athletes with a known diagnosis of CVD but not for middle-aged or older amateur athletes in Europe. 14
Previous research has predominantly examined the health effects of marathon running on professional male runners. 3 However, it is crucial to evaluate the uncertain relationship between marathon running and health outcomes specifically for male amateur marathon runners.15,24,43 This is of particular concern given that, in 2018, out of all marathon participants worldwide, an average of 68.08% were men compared with 31.92% women. 50 Although cardiac arrests are rare in marathon running, they still occur in approximately 1.01 per 100,000 runners. 21
The systematic review aimed to assess the MRFs of CVD in experienced male amateur marathon runners and health interventions on CVD risk factors. The objectives included identifying and providing a comprehensive synthesis of the running profile of male amateur marathon runners, the prevalence of MRFs, the screening or assessment approaches used for MRFs, the associations between marathon running profile and CVD, and the associations between MRFs and CVD.
Methods
This systematic review was conducted in harmony with the Preferred Reporting Items for Systematic Review and Meta-Analyses Protocols (PRISMA-P) 2015 guidelines.38,54
Literature Search
The search strategy of the MEDLINE, CINAHL, Embase, SPORTDiscus, and Cochrane databases was performed in June 2018. It was updated in March 2020 and included studies published between June 1, 2008 and February 29, 2020. The electronic search was restricted to published English language studies, including primary epidemiological, observational, randomized controlled trials (RCTs) and/or non-RCTs studies: published between June 1, 2008 and February 29, 2020. The search strings for all the electronic databases are included in Appendix 1 (available in the online version of this article). The search terms used for each database can be seen in Appendix 2 (available online). The reference lists of all included articles were scanned for additional relevant studies.
Inclusion and Exclusion Criteria
Studies were included if they reported data relating to (1) male amateur marathon runners aged ≥18 years with a known or unknown diagnosis of CVD that had participated in ≥1 marathon (42.195 km) in the previous year; (2) mixed “men and women OR amateur and elite marathon runners studies” where data specific to male amateur marathon runners could be extracted; (3) reported data on any MRFs for CVD such as smoking, diet, physical activity, body weight, BP, lipids, and diabetes as per the 2021 ESC Guidelines on CVD prevention in clinical practice42,58; (4) health interventions on CVD risk factors; (5) related studies if they meet the inclusion criteria; (6) if available, a comparative male group relating to the general male population; (7) published primary epidemiological, observational, RCTs and/or non-RCTs; (8) were published in the English language; and (9) were published between June 1, 2008 and February 29, 2020.
We excluded studies that (1) sampled sportsmen aged <18 years, elite/professional sportsmen; or sportswomen or sportsmen age ≥18 years with known congenital heart disease as defined by the ESC (2020) 1 ; (2) were based on first-time marathon race participants; (3) reported data on sportsmen who took part in any other running races other than marathon races (42.195 km); (4) related study papers if they did not meet the inclusion criteria; (5) were specifically based on diagnostic screening; (6) were not reported in the English language, or were case reports, gray literature, qualitative studies, quasi-experimental, or pilot studies.
Selection Process
Two authors conducted the literature search and screened all titles and abstracts of articles retrieved from the search. The online software product Covidence was used as a primary screening and data extraction tool. 9 The full-text articles were then read by both authors if deemed potentially eligible for inclusion. A secondary search was carried out by screening the reference lists of the included studies, where 1 further eligible study was found. When required, any discrepancies in the selection process were resolved through consensus with both authors and a third author if needed.
Data Extraction
Data were extracted from the included studies by 1 author and cross-checked by 2 authors. These data included author, year of publication, and country; marathon setting, sample size, age of study participants (mean ± SD), running profile, CV health; study design, methods of data collection, measures of screening for MRFs and diagnostic imaging for CVD, approaches, guidelines for MFRs; health interventions on CVD risk factors; and prevalence (means) of MRFs, associations with CVD and other variables. The years of publication ranged from 2008 to 2020. The studies that met the inclusion criteria are listed in Table 1, which also describe the details of each study.
Study characteristics and results of included articles
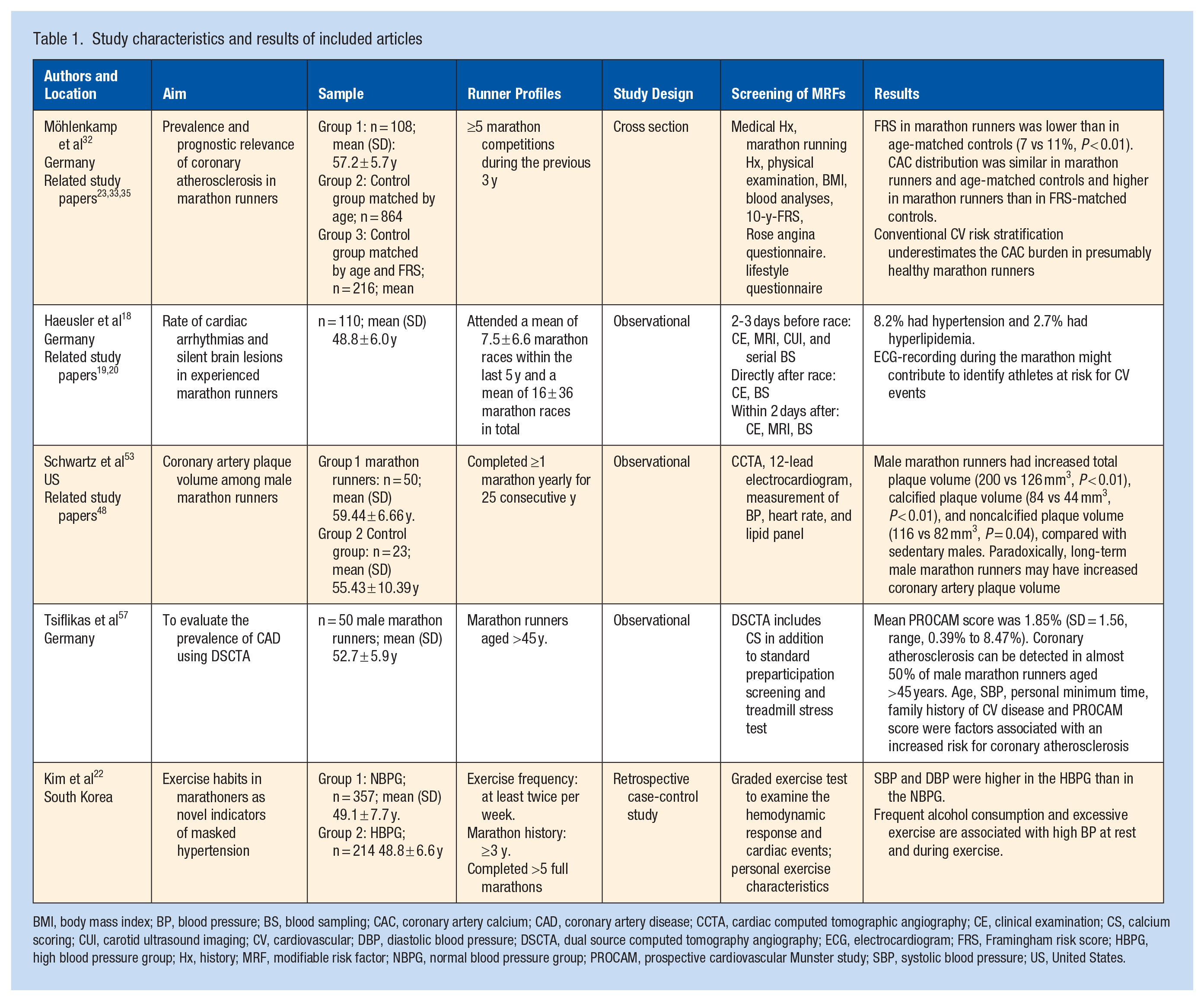
BMI, body mass index; BP, blood pressure; BS, blood sampling; CAC, coronary artery calcium; CAD, coronary artery disease; CCTA, cardiac computed tomographic angiography; CE, clinical examination; CS, calcium scoring; CUI, carotid ultrasound imaging; CV, cardiovascular; DBP, diastolic blood pressure; DSCTA, dual source computed tomography angiography; ECG, electrocardiogram; FRS, Framingham risk score; HBPG, high blood pressure group; Hx, history; MRF, modifiable risk factor; NBPG, normal blood pressure group; PROCAM, prospective cardiovascular Munster study; SBP, systolic blood pressure; US, United States.
Data Analysis and Quality Assessment
Data analysis was presented by reporting variables derived from the data extraction process. Since the review did not identify any studies on interventions to address MRFs, a meta-analysis to determine intervention effects was not possible. The National Institutes of Health (NIH) Quality Assessment Tools for both Observational Cohort and Cross-sectional studies and Case-Control studies were used to assess the quality of the studies. 36 The quality appraisal of the studies ranked the studies as good, fair, or poor. All articles were independently assessed by 1 researcher and cross-checked by a second researcher. Any discrepancies that arose were then discussed and resolved by 2 researchers or in consultation with a third researcher.
Results
Search and Study Selection Results
The primary search yielded 4606 articles. After the review of titles, 334 duplicates were removed using the primary screening and data extraction tool Covidence. 9 A total of 4272 titles and abstracts were screened, and 4154 studies were excluded from the title and abstract screening. After the review of 118 full-text articles, 108 were excluded. One full-text study was found after screening references 48 ; 4 primary studies met the inclusion criteria. Data from 3 studies were used in subsequently published articles. Therefore, data from 11 papers based on 5 studies contributed to the findings reported in Table 1 of this systematic review. Möhlenkamp et al 32 reported initial findings in 2008 and then 3 other studies later provided further analysis concerning the MRFs.23,33,35 Similarly, Haeusler et al19,20 later reported findings in 2 related papers that provided information in relation to the aims of the study and follow-up data. Finally, Schwartz et al 53 provided subsequent analysis in a related paper on the MRFs of marathon runners. 48 The search and output processes are described in Figure 1 using the PRISMA format.38,54
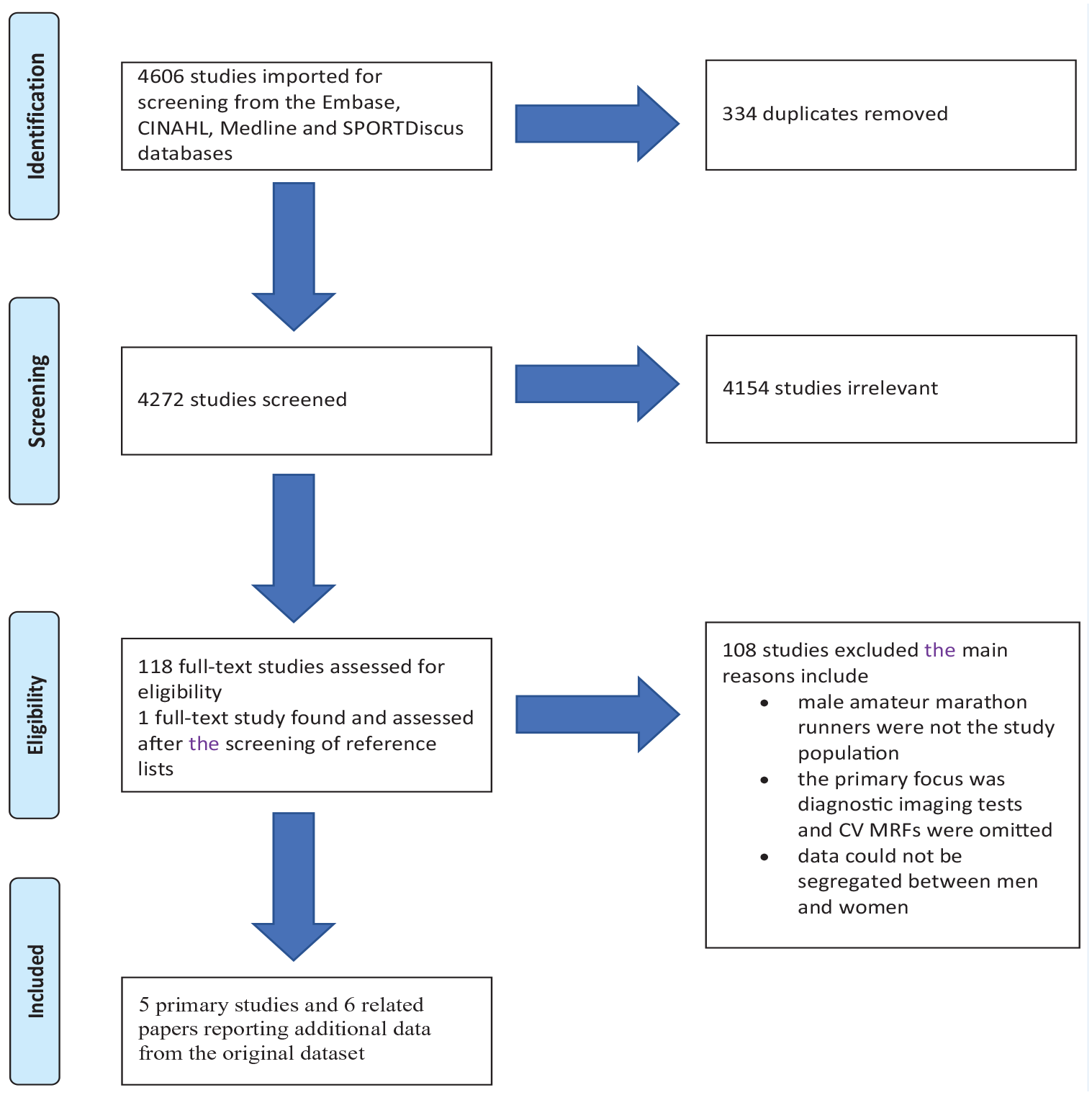
PRISMA flow diagram illustrating the epidemiological search and study selection strategy. 55 CV, cardiovascular; MRFs, modifiable risk factors; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
Table 1 shows the characteristics of the 5 studies included.18,22,32,53,57 Our review includes 4 observational studies,18,32,53,57 and 1 case-control study that presents cohort data. 22 Three studies were conducted in Germany,18,32,57 1 originated in South Korea, 22 and 1 in the United States (US). 53 There were no studies on health interventions on CVD risk factors in any of the included studies; therefore, we cannot report on this objective of the review.
Profile of Marathon Runners
Table 1 shows the characteristics of all 5 studies.18,22,32,53,57 The total sample size from the 5 studies was 862 male amateur marathon runners where all studies used convenience sampling methods. The age of the male amateur runners across the studies ranged from 41.7 to 77 years. Data on MRFs were obtained from self-reported information, BP recordings and anthropometric measurements. One study reported on the follow-up of participants. 32 Möhlenkamp et al 32 reported that no deaths were recorded during the 21-month (interquartile range [IQR], 18.6-24.0 months) follow-up period; however, 4 runners experienced a coronary event. No marathon runner experienced a CV event 1 year after the marathon.18,20 Both studies found that the body mass index (BMI) and systolic BP (SBP) were lower and that high-density lipoprotein (HDL) was higher in the marathon running groups compared with controls.32,53
Quality Assessment
The included studies were assessed according to the Quality Assessment Tools for both Observational Cohort and Cross-sectional studies, and Case-control Studies. 36 The quality assessment results can be viewed in Tables 2 and 3. Overall, the studies indicated good quality and achieved more than half of the recommendations required to contribute to the internal validity.18,22,32,53,57 However, it could not be determined whether the outcome measures were clearly defined, valid, reliable, and implemented consistently across all study participants in 4 studies.18,32,53,57 Furthermore, 2 studies demonstrated a lower quality as they failed to address whether the outcome assessors were blinded to the exposure status of participants.53,57 Therefore, the quality appraisal indicates a risk of bias within these studies.18,22,32,53,57
Results of the quality assessment tool for observational cohort and cross-sectional studies
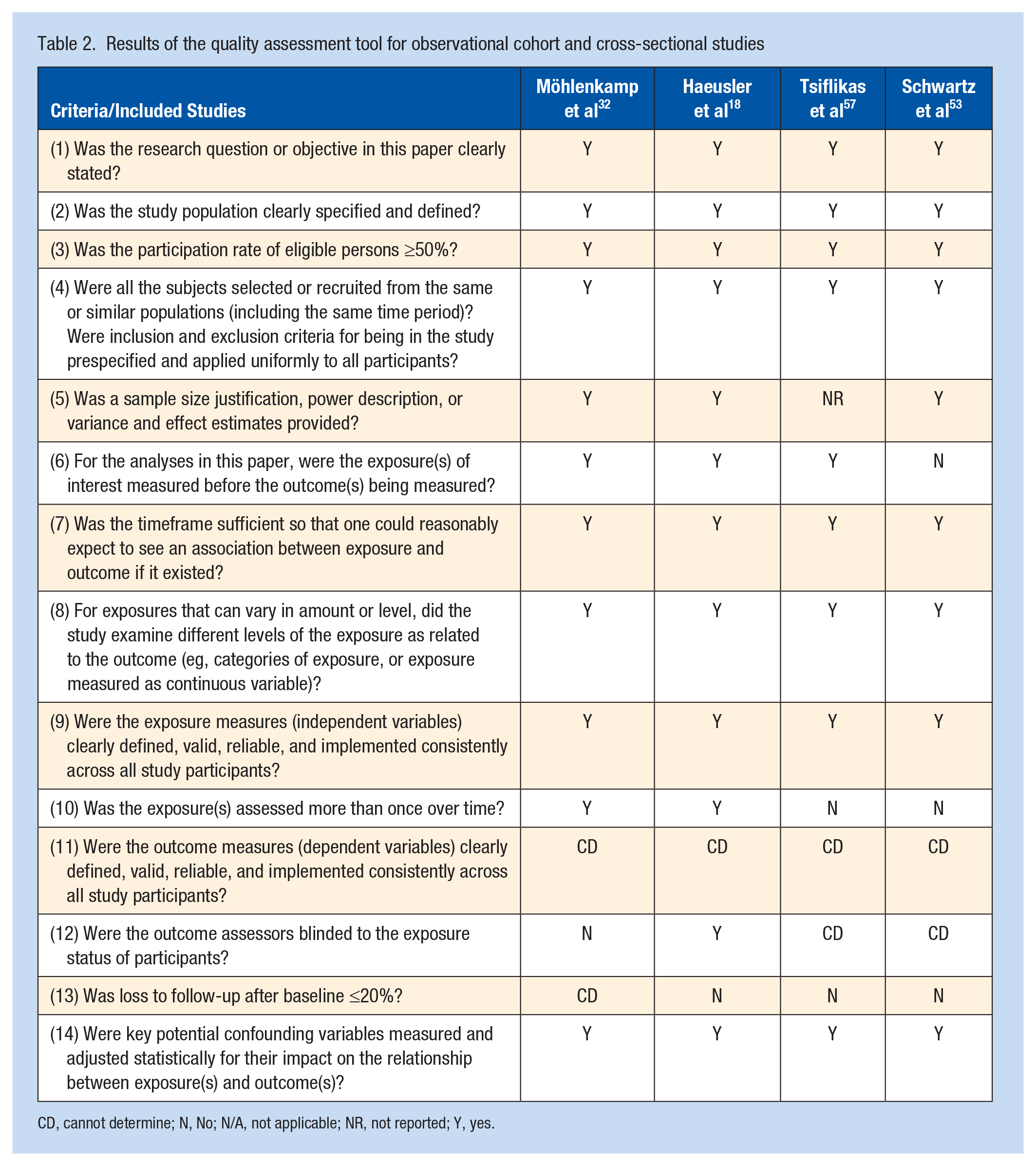
CD, cannot determine; N, No; N/A, not applicable; NR, not reported; Y, yes.
Results for the quality assessment tool of case-control studies
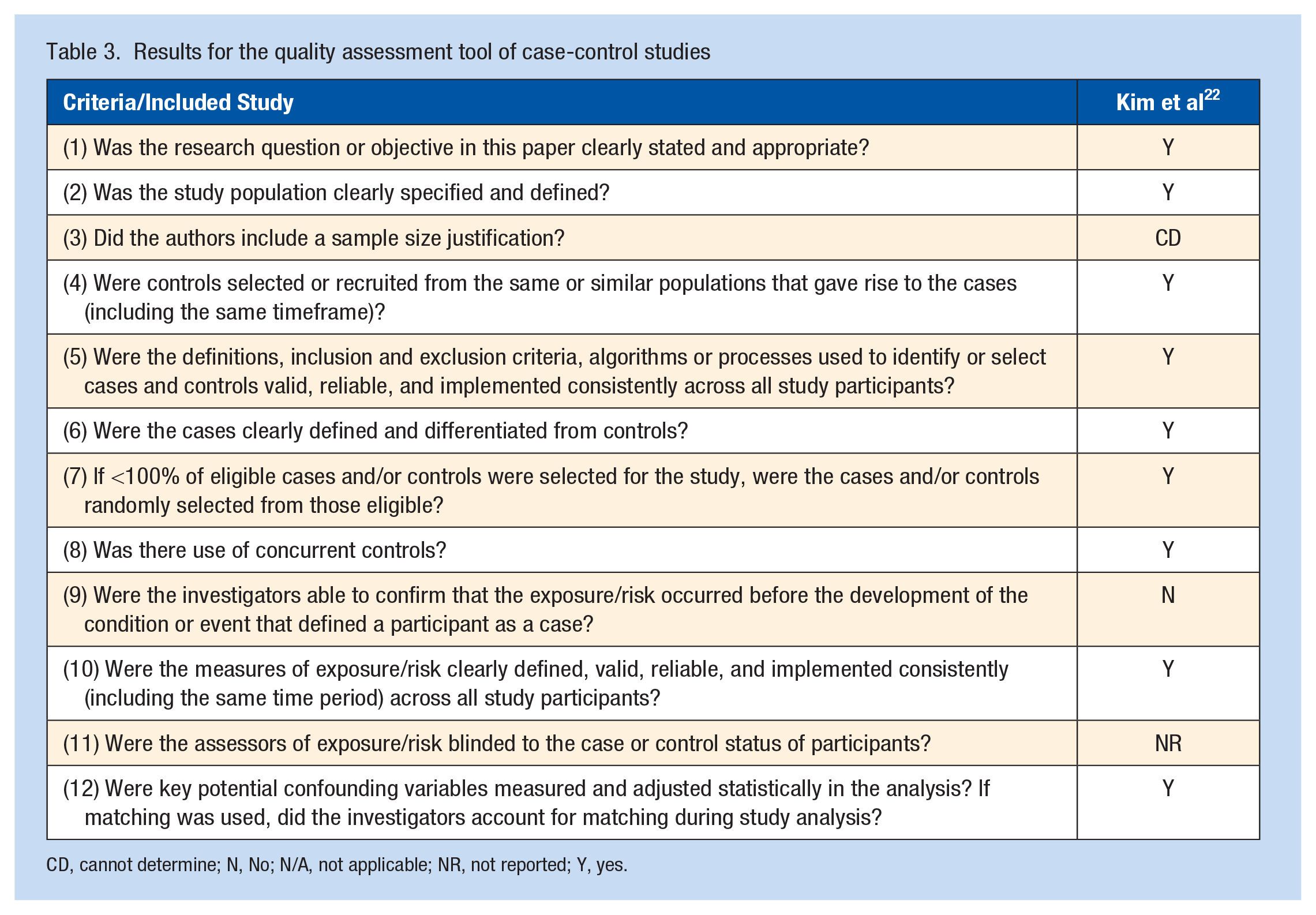
CD, cannot determine; N, No; N/A, not applicable; NR, not reported; Y, yes.
Assessment for MRFs
The assessment for MRFs varied across the 5 studies.18,22,32,53,57 Most of the studies used a combination of the following: medical history18,22,32,53,57; marathon race history18,22,32,53,57; physical examination18,22,32,53,57; blood analyses18,22,32,53,57; sociodemographic history18,19,20; Framingham risk score (FRS)23,32,33,35; Rose angina questionnaire23,32,33,35; nonvalidated questionnaires,23,32,33,35 for example on lifestyle,48,53 health, nutrition, exercise, and psychosocial and socioeconomic risk factors; interviews23,32,33,35; Prospective Cardiovascular Münster (PROCAM) cardiovascular study CV risk score 57 ; BORG rating of perceived exertion scale 22 ; and an exercise treadmill stress test (GXT). 22 It was difficult to compare these data as not all studies followed specific criteria that can be noted in their measurement of BP and recall data, which could influence bias.18-20,22,23,32,33,35,48,53,57
Modifiable Risk Factors
Smoking
All studies reported that smoking was evident in a number of their participants.18,22,32,53,57 From the included studies, the rate of current smoking ranged from 4.6% to 8.7%,22,32 and the rate of former smoking ranged from 34% to 52%.53,57 Möhlenkamp et al 32 reported that there was a 19% lower rate of ever-smoked in marathon runners compared with the control group matched by age. Notably, more than half of the marathon runners were former smokers and 5% were current smokers, which may explain the presence of coronary atherosclerosis. 32 Haeusler et al 18 reported that 7.2% of the participants were smokers, which may be a contributing cause of the 10.8% who were hypertensive. Schwartz et al 53 found that current or previous tobacco use was higher in participants with coronary artery calcium (CAC) than in those without CAC. Tsiflikas et al 57 found that participants who had a history of smoking had no impact on the presence or absence of CAD. Kim et al 22 found smoking status to be higher in the normal blood pressure group (NBPG); however, there was a larger number of participants in the NBPG compared with the high blood pressure group (HBPG). The percentage of marathon runners found to be ‘current smokers’ was low, with 3 studies reporting ≤10.5%.18,22,32
Alcohol
Two studies reported on alcohol use.18,22 Haeusler et al 18 studied 83 participants and found no alcohol use among participants. Kim et al 22 studied 571 participants, of whom 357 met the HBPG criteria and 214 met the NBPG. The level of exercise intensity was higher in the HBPG (13.3 ± 1.6) than that in the NBPG (12.9 ± 1.5; P < 0.01). 22 Kim et al 22 reported that marathon runners in the HBPG (1.8 ± 1.9) (mean ± SD) had a significantly higher alcohol daily consumption rate weekly compared with the NBPG (1.3 ± 1.4; P < 0.01) (mean ± SD). However, this study was unable to determine the exact volume of alcohol consumed within this population. 22
Diet
None of the 5 studies reported on the dietary behaviors of the marathon runners.18,22,32,53,57
Physical Activity
Möhlenkamp et al 32 reported that the 108 participants completed an average of 20 marathons (a median value, ranging from Q1-Q3: 14-42), ran their first marathon 9 years ago (a median value ranging from Q1-Q3: 7-16 years), and ran 55 km (a median value ranging from Q1-Q3: 45-65 km) on 5 days a week during the year. Haeusler et al. 18 reported that 83 participants completed a mean (SD) of 18.0 (40.8) marathons per year and ran the average mean (SD) of 43.2 (14.1) km per week; no data were available on when they ran their first marathon. Tsiflikas et al 57 reported that 50 male participants ran a mean (SD) of 13.8 (16.2) marathons ranging from 1 to 72. These participants ran a mean (SD) of 5 (1.8) hours per week ranging from 2 to 12 hours and had been actively running for a mean (SD) of 16.3 (9.8) years, ranging from 3 to 50 years. 57 When these participants were divided into no-CAD versus CAD, there was no statistically significant difference in their physical activity. 57 Kim et al 22 divided their participants into 2 groups: NBPG and HBPG. The NBPG completed (44.4 ± 45.3) marathons (mean ± SD), whereas the HBPG completed (43.4 ± 37.8) marathons (mean ± SD). 22 The NBPG trained 93.7 ± 37.0 minutes per day and the HBPG trained 101.3 ± 38.9 minutes per day. 22 Roberts et al 48 divided the participants into 2 groups: CAC absent and CAC present. Participants completed (mean ± SD)(78.63 ± 11.46 vs 66.24 ± 6.18 marathons for CAC absent and CAC present participants, respectively (P = 0.30). The mean (± SD) age (years) at which they ran their first marathon was 28.00 ± 1.55 years vs 33.50 ± 1.10 years (P < 0.01). 48 There were no data on their weekly exercise participation. 48 They were then divided into 4 different groups depending on the level of their CAC; Zero CAC (0), Low CAC (1-100), Moderate CAC (101-400), and Extensive CAC (>400). 48 When comparing participants who had no CAC with those with moderate and extensive CAC, the participants with CAC were older, began running at an older age, ran their first marathon at an older age, and had more risk factors for CAC. 48 In summary, these data on physical activity suggest that long-term training and marathon running may not protect these marathon runners from the progression of CAC and coronary events, which, paradoxically, may be associated with accelerated coronary artery plaque formation despite the positive effects from other MRFs.32,48,53 As concluded from studies by Möhlenkamp et al 32 and Schwartz et al,40,53 this also suggests that prolonged strenuous exercise and marathon running may reduce or eliminate the positive benefits of physical activity witnessed by practicing moderate physical activity.
Body Weight
Waist circumference, an important measure of CVD risk, was not recorded in any of the studies, nor was any measure of skinfold thickness.18,22,32,42,53,57,58 Two studies found that there was a lower BMI (kg/m2) in marathon runners than in nonrunners.32,53 There was a higher BMI noted in participants who had CAD than in those who did not have CAD mean (SD), [range] 24.0 (2.7) [20.4-33.1] vs 23.1 (2.5) [18.7-26.6]. 57 No other study compared no-CAD, CAD, and BMI. The study by Möhlenkamp et al 32 found that runners had a lower BMI when compared with nonrunners. A 15% lower BMI was reported in marathon runners in Group 1 (G1) when compared with the control group matched by age in Group 2 (G2); mean (SD): 24.0 ± 2.3 versus 28.1 ± 4.0 (G1) versus (G2) (P ≤ 0.01). 32 Haeusler et al 18 also reported a normal BMI in the male participants, with a mean (SD) of 23.5 (2.0). Tsiflikas et al 57 compared BMI in those with and without CAD; no-CAD (n = 26) vs CAD (n = 24); mean (SD), [range], 23.1 (2.5) [18.7-26.6] vs 24.0 (2.7) [20.4-33.1] and found the BMI to be lower in the no-CAD group, which had a slightly higher number of participants. However, the difference was not statistically significant. Kim et al 22 noted a higher BMI in the NBPG (n = 357) compared with the HBPG (n = 214); mean ± SD, 23.5 ± 1.9 versus 23.3 ± 2.2. This data was also not statistically significant. 22 Schwartz et al 53 found marathon runners (n = 50) had a lower BMI when compared with sedentary male controls (n = 23), mean ± SD, 24.16 ± 2.88 versus 30.29 ± 5.16 (P < 0.01).
Blood Pressure
All 5 studies recorded both SBP and diastolic BP (DBP); however, the methods of BP measurement did not state whether there was a standardized method utilized as recommended by the ESC.22,32,42,53,57,58 Hypertension (HTN) was evident in some of the participants, but the studies did not state how HTN was defined.18,22,32,53,57 None of the studies reported an optimal recording of conventionally measured seated office BP of <120/80mmHg as recommended by ESC guidelines.18,22,32,42,53,57,58 All 5 studies reported baseline BP recordings only, and several participants had a history of HTN.18,22,32,53,57 In studies that compared marathon runners with nonmarathon runners they found that the marathon runners had a lower BP.32,53 A higher BP recording was observed in the CAD group when compared with the no-CAD group, mean (SD), [range]: SBP: 137 (15) [105-165] and DBP: 85 (8) [70-100] versus SBP: 125 (13) [105-150] and DBP: 81 (7) [65-90]. This was also the case for marathon history, mean (SD), [range]: 15.6 (18.9) [1-72] versus 12.0 (13.3) [1-55]. 57 The BORG rating of perceived exertion (RPE) scale is the main instrument used to measure exercise intensity.22,40,58 Findings that reported excessive exercise intensity and longer exercise durations were associated with an increase in BP at rest and during exercise irrespective of marathon history. Möhlenkamp et al 32 was the only study to compare 2 control groups. They found SBP and history of HTN were lower in marathon runners when compared with both control groups. 32 Marathon runners had a 12% lower SBP when compared with the control group matched by age and a lower heart rate when compared with both control groups. 32 Kim et al 22 reported that, of 571 participants, 214 runners had a BP >140/90mmHg. However, Kim et al 22 recorded SBP and DBP before and after a GXT on a treadmill (Medtrack ST 55, Quinton Instrument Co) showing an increase in SBP and a decrease in DBP after exercise (SBPrest mmHg: 134.2 ± 15.5 vs SBPmax mmHg: 214.0 ± 27.4, DBPrest mmHg: 85.1 ± 10.6 vs DBPmax mmHg: 73.8 ± 13.3. Schwartz et al 53 reported SBP and DBP to be lower in the marathon group than the sedentary group. Kim et al 22 found that excessive exercise intensity and longer exercise durations were suggestive of an association of an increase in BP at rest and during exercise irrespective of the marathon history. This can be witnessed from the following exercise characteristics of the participants in their study: Marathon history (month) (mean ± SD), NBPG: 96.4 ± 60.9 versus HBPG: 80.7 ± 44.7, total: 90.6 ± 55.8 (P < 0.01). Marathon completion durations (minutes) (mean ± SD), NBPG: 217.4 ± 29.6 versus HBPG: 211.2 ± 28.1, total: 214.6 ± 29.2 (P = 0.03). Exercise intensity (Borg RPE scale), (mean ± SD), NBPG: 12.9 ± 1.5 versus 13.3 ± 1.6, total: 13.0 ± 1.6 (P < 0.01). Exercise duration (minutes/day), (mean ± SD), NBPG: 93.7 ± 37.0 versus 101.3 ± 38.9, total: 96.6 ± 37.9 (P = 0.02).
Lipids
Four studies reported on blood lipids.18,22,32,57 Blood lipids were analyzed into their 4 components, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), HDL cholesterol (HDL-C), and triglycerides in 3 of the studies.32,53,57 Möhlenkamp et al 32 found that TC and LDL-C were lower and that HDL-C was higher in marathon runners when compared with both control groups; triglyceride levels were not reported. Accordingly, when the marathon runners were compared with controls matched by age, a 42% higher HDL-C and an 18% lower LDL-C were reported in marathon runners. 32 HDL cholesterol (mg/dl), (mean ± SD), marathon runners: 73.8 ± 17.3 versus age-matched controls: 51.9 ± 14.7 versus controls matched for age and risk factors: 60.6 ± 14.7 (P value; marathon runners vs age-matched controls: <0.01), (P value; marathon runners vs controls matched for age and risk factors: <0.01). LDL cholesterol (mg/dl), (mean ± SD), marathon runners: 121 ± 29 versus age-matched controls: 147 ± 36 versus controls matched for age and risk factors: 131 ± 31, (P value; marathon runners vs age-matched controls: <0.01), (P value; marathon runners vs controls matched for age and risk factors: <0.05). Haeusler et al 18 reported hyperlipidemia was noted in participants with a mean (SD) of 3.6 (3). Roberts et al 48 noted similar results to those of Möhlenkamp et al 32 as marathon runners with CAC absent had lower TC, triglycerides, and LDL-C but higher HDL when compared with runners with CAC. Roberts et al 48 found that an increasing CAC score was positively associated with having started running at an older age and the age they ran their first marathon and LDL-C. A possible cause of this was that the marathon runners had more CVD MRFs and reported greater pack-years of smoking, which all consequently resulted in a higher LDL-C. 48 These results imply that marathon running cannot overcome past negative lifestyle choices practiced by some marathon runners. 48 Tsiflikas et al 57 reported that, for the runners in the no-CAD group compared with the CAD group, TC and HDL-C were lower, triglycerides were higher, and there was no difference for LDL-C in the CAD group. Kim et al 22 did not report on lipids.
Diabetes Mellitus
Four studies reported on diabetes and found no marathon runner to have diabetes.18,32,53,57 Möhlenkamp et al 32 reported 8.6% of the aged-matched control group has diabetes versus 0% in the marathon runners. 32 In another comparison group involving marathon runners and sedentary male controls, the percentage of diabetes was 0% versus 17.4%. 53
CAD in Marathon Runners
Möhlenkamp et al 32 found that 36% of marathon runners had a CAC score ≥100, indicating the prevalence of myocardial damage within this cohort and a major risk factor for all-cause mortality and CV events. Haeusler et al 18 found no participant to have CAD but associated data from Herm et al 20 found some marathon runners to experience exercise-induced transient ST-T segment deviations associated with elevated high-sensitive troponin T (hsTnT) directly after the marathon. Schwartz et al 53 found marathon runners to have increased coronary artery plaque volume when compared with the sedentary group, thereby concluding that excessive training and marathon running may be associated with coronary artery plaque formation. 53 The study by Tsiflikas et al 57 demonstrated that almost 50% of the participants had coronary atherosclerosis detected by cardiac computed tomography (CT) despite a positive CV risk factor profile. The treadmill exercise testing was unable to detect these results. 57 Kim et al 22 did not state if CVD was found in their study participants; however, they did highlight that vigorous exercise and excessive alcohol consumption resulted in high BP during exercise and at rest in the HBPG of marathon runners.
Discussion
This systematic review is the first to investigate the current literature on the MRFs of CVD in experienced male amateur marathon runners. There were 5 studies, and additional data were reported in 6 related papers that described MRFs and CVD.18-20,22,23,32,33,35,48,53,57 The most compelling finding was that excessive training and marathon running may cause a reduction in the benefits received from exercise, whereas moderate training appears to have a more profound positive effect on health.18,22,32,53,57
The next most striking finding was that, although marathon running can exert many positive health benefits, it does not override the negative effects of long-term exposure to an unhealthy lifestyle.18,22,32,53,57
There was no evidence of a standardized method or criteria followed to assess the MRFs or the running history of the male amateur marathon runners, rendering comparison between studies difficult.18,22,32,53,57 CV risk assessment tools such as the ESC high-risk Systemic Coronary Risk Estimation (SCORE) chart may be useful in this population group who may deem themselves healthy but may not be if they do not meet the recommended ESC guidelines on CVD in clinical practice.42,58 No study reported on preventive health interventions for CVD risk factors. Despite CVD being the world’s most prevalent cause of death,5,7,26,42,49,58 there was no evidence concerning participants’ knowledge levels about their CV MRFs or whether they had attended a healthcare provider for a health assessment before participating in vigorous training and marathon running.
Although the review revealed that some marathon runners exhibited a high prevalence of CV MRFs, these results may be higher as 4 out of 5 studies excluded subjects with a known medical history of CVD.18,22,32,53,57 Therefore, CVD may be more prevalent in those excluded who may be unaware of their risk.18,22,32,57 As all 5 studies recruited participants through convenience sampling methods, participants who are concerned about their health may have been more receptive to the study as opposed to other marathon runners.18,22,32,53,57 Möhlenkamp et al 32 and Schwartz et al 53 were the only studies to use control groups. Möhlenkamp et al 32 compared marathon runners with matched controls from the unselected general population of the Heinz Nixdorf Recall Study and Schwartz et al 53 compared marathon runners with sedentary male controls.32,53 When marathon runners with no CAC were compared with those with CAC, the CAC group was found to be older, began running at an older age, ran their first marathon at an older age, had a history of both tobacco use and hyperlipidemia and more MRFs.48,57 Tsiflikas et al 57 studied 50 male marathon runners and found CAD to be present in 24 marathon runners detected using coronary dual-source CT angiography (DSCTA). 57 The results of these studies demonstrate that some marathon runners may be asymptomatic of CVD and should be made aware of the potential negative cardiac effects of extremely vigorous exercise on their cardiac health.48,57 Preparticipation screening may be required for marathon runners with a high risk of CVD or a known medical history of CVD before marathon training and marathon races. 40 It was found that age, SBP, family history of CVD, and a faster personal minimum time were all associated with an increased risk of developing coronary atherosclerosis. 57 Kim et al 22 compared NBPG vs HBPG within their study population. The HBPG exhibited a greater alcohol consumption and exercise-induced HTN, which markedly increased BP at rest and during exercise in this group compared with the NBPG. 22 This finding suggests that middle-aged marathon runners who partake in vigorous marathon running and frequent alcohol consumption weekly, may be at risk of high BP both at rest and during exercise. 22 Therefore this population should be observed for the risk of masked HTN. 22
Strengths and Limitations of the Review
A strength of this systematic review is the comprehensive search strategy across 5 databases, which was undertaken by following the PRISMA guidelines.38,54 However, the findings of this systematic review should be interpreted with caution. The search was limited to English language studies only. Case reports, gray literature, qualitative studies, quasi-experimental, and pilot studies were excluded owing to the risk of introducing bias. Although the literature search included any available papers from June 1, 2008 to February 29, 2020, only 5 studies met the inclusion criteria.18,22,32,53,57
Recruitment bias cannot be ruled out as this systematic review was limited to male marathon runners only; therefore, the data are not generalized to all marathon runners. All studies used self-reported measurements of marathon running profile,18,22,32,53,57 and 1 study used nonvalidated lifestyle questionnaires, which may introduce recall bias. 32 All studies were of good methodological quality based on the quality appraisal assessment tools used.18,22,32,53,57 All 5 studies reported BP measurement at 1 timepoint, which may introduce bias.18,22,32,53,57 A 24-hour ambulatory BP recording would be more accurate in detecting HTN and masked HTN within this population.42,58 The studies reported used nonstandardized measures, therefore making it difficult to compare the studies as they lacked homogeneity.
Clinical Recommendations and Further Research
From this review, a clinical recommendation should be advised for novice marathon runners ≥35 years with a high risk of CVD to undertake a preparticipation health assessment to identify any underlying unknown CV health issues that could cause adverse effects or ill health, whereby partaking in vigorous training and a marathon could be detrimental to the marathon runner. 40 This systematic review demonstrates that the CV MRFs are not accurate as a primary method in detecting whether someone has CVD or not, which can be shown only in diagnostic imaging tests. Training and marathon running should be tailored to each cardiorespiratory fitness and CV risk factor profile as a result of their health assessment. 40 This systematic review found no studies that reported on health interventions on CVD risk factors; therefore, future studies should play a pivotal role in addressing this research gap. An example may be the prevention and early detection of CVD, thereby raising awareness of the CV MRFs in male amateur marathon runners. Furthermore, as diet was not discussed in any of the papers, it may be pertinent for marathon runners to be educated on the importance of a healthy nutrient-dense diet as no amount of marathon running can revoke an unhealthy Western diet. Moreover, additional research is required to investigate whether a preparticipation assessment should be made mandatory for this population to ensure safe participation. The question arises as to whether runners should monitor their cardiovascular health before participating in a marathon.
Conclusion
There is a paucity of available research and heterogeneous data on the reporting of the CV MRFs of experienced male amateur marathon runners. Research has shown that CAD is the main cause of marathon-related sudden cardiac arrest in men ≥35 years.21,47 There is an increasing number of older men participating in marathons later in life, which may be leading to an increase in exercise-related cardiac conditions.21,47 Despite the evidence-based research demonstrating physical activity has many positive health outcomes, it should be recognized that excess physical activity is not beneficial, particularly in marathon runners as defined as those who participate in ≥1 marathon (42.195 km) in the previous year who may have an unknown diagnosis of CVD. ESC guidelines offer little guidance for this population, which is remarkable given the prevalence of marathon running worldwide.40,42,58 There is a need for consensus guidelines on this topic.
Supplemental Material
sj-docx-2-sph-10.1177_19417381231176534 – Supplemental material for Cardiovascular Disease Risk Factor Profile of Experienced Male Amateur Marathon Runners: A Systematic Review
Supplemental material, sj-docx-2-sph-10.1177_19417381231176534 for Cardiovascular Disease Risk Factor Profile of Experienced Male Amateur Marathon Runners: A Systematic Review by Catherine O’Riordan, Eileen Savage, Micheál Newell, Gerard Flaherty and Irene Hartigan MSc in Sports Health
Supplemental Material
sj-pdf-1-sph-10.1177_19417381231176534 – Supplemental material for Cardiovascular Disease Risk Factor Profile of Experienced Male Amateur Marathon Runners: A Systematic Review
Supplemental material, sj-pdf-1-sph-10.1177_19417381231176534 for Cardiovascular Disease Risk Factor Profile of Experienced Male Amateur Marathon Runners: A Systematic Review by Catherine O’Riordan, Eileen Savage, Micheál Newell, Gerard Flaherty and Irene Hartigan MSc in Sports Health
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
The authors report funding received from the European Society of Cardiology in the form of an ESC Nursing Training Grant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.