
Abstract
Background:
Approximately 1 in 4 athletes returning to sports will sustain a second anterior cruciate ligament (ACL) injury. Psychological factors related to kinesiophobia, confidence, and psychological readiness are associated with second ACL injury; however, the evidence is conflicting.
Hypothesis:
Athletes who sustain a second ACL injury (ie, graft rupture or contralateral ACL rupture) within 2 years of ACL reconstruction (ACLR) would have greater kinesiophobia, less confidence, and lower psychological readiness prior to return to sport (RTS) compared with athletes who do not sustain a second ACL injury.
Study Design:
Secondary analysis of a prospective randomized trial.
Level of Evidence:
Level 3.
Methods:
A total of 39 female Level I/II athletes completed the following measures after postoperative rehabilitation and a 10-session RTS and second ACL injury prevention program: ACL Return to Sport after Injury (ACL-RSI) scale, the 11-item Tampa Scale of Kinesiophobia (TSK-11), and question 3 on the Knee injury and Osteoarthritis Outcome Score (KOOS) quality of life (QoL) subscale. Athletes were dichotomized based on whether they sustained a second ACL injury within 2 years of ACLR or not. Independent t tests determined group differences in TSK-11, KOOS-QoL, ACL-RSI, and the 3 individual components of the ACL-RSI (ie, emotions, confidence, risk appraisal).
Results:
Nine athletes sustained a second ACL injury (4 graft ruptures and 5 contralateral ACL ruptures). The group that sustained a second ACL injury had higher scores on the ACL-RSI (P = 0.03), higher on the risk appraisal questions of the ACL-RSI (P < 0.01), and met RTS criteria sooner than athletes who did not (P = 0.04). All second ACL injuries occurred in athletes who underwent primary ACLR with hamstring tendon autografts.
Conclusion:
Athletes who sustained a second ACL within 2 years of ACLR had a more positive psychological outlook, higher scores on the specific questions related to the risk appraisal construct of the ACL-RSI, and met RTS criteria sooner than athletes who did not sustain a second ACL injury.
Clinical Relevance:
Counseling athletes about delaying RTS to reduce the risk of second ACL injury may be especially important in athletes who display high psychological readiness and meet RTS criteria sooner.
The prevalence of second anterior cruciate ligament (ACL) injuries remains high in athletes returning to high level sports involving cutting, jumping, and pivoting.4,5 Factors associated with second ACL injury include time from surgery to return to sport (RTS), quadriceps strength deficits, poor functional performance, graft type, age, sex, and activity level.4,5,11,17,21,22,30,34 In addition, psychological factors such as psychological readiness to RTS, knee confidence, and fear of reinjury have been identified recently as potential factors associated with second ACL injury.19,20,23,24,26 However, the association among second ACL injury, psychological factors, and level of psychological readiness for safe RTS is still unclear as studies report conflicting evidence.
Paterno et al 24 developed a preliminary clinical prediction model to identify athletes at high risk of sustaining a second ACL injury. The authors found high knee confidence at the time of RTS, as measured by the Knee injury and Osteoarthritis Outcome Score (KOOS), quality of life (QoL) subscale question 3, was a factor included in 1 of the 2 identified high-risk models. Paterno et al 24 also found that patients who went on to sustain an ipsilateral graft tear within 2 years of RTS clearance had higher scores on the 11-item Tampa Scale of Kinesiophobia (TSK-11), indicating more fear of movement. 23 In 2 published studies, McPherson et al19,20 examined the association between psychological readiness to RTS (preoperatively, and 12 months after ACL reconstruction (ACLR)) and second ACL injury. Their first study found that younger patients (≤20 years) with lower psychological readiness scores were at higher risk of second ACL injury. 19 The second study found that among younger patients (≤20 years), a smaller improvement in psychological readiness from before surgery to 12 months after ACLR was associated with second ACL injury. 20 These conflicting findings make the relationship between second ACL injury and psychological readiness ripe for further inquiry.
The limited studies examining psychological factors and second ACL injury used different self-reported measures that examine various psychological constructs (ie, kinesiophobia, knee confidence, psychological readiness). None have examined the relationship between multiple psychological constructs and second ACL injury. A better understanding of the relationship among specific psychological constructs and second ACL injury is needed to develop targeted interventions to reduce reinjury after ACLR.
The purpose of this study was to examine the relationship between second ACL injury and multiple self-reported psychological domains (ie, kinesiophobia, knee confidence, psychological readiness) in a group of female athletes at high-risk of second ACL injury enrolled in the Anterior Cruciate Ligament–Specialized Post-Operative Return to Sports (ACL SPORTS) clinical trial. While the literature is conflicting, we hypothesized that greater kinesiophobia, less knee confidence, and lower psychological readiness would be associated with second ACL injury.
Methods
This study is a secondary analysis of a prospective clinical trial and was approved by our Institutional Review Board. Participants were recruited between December 2011 and January 2017, and provided written informed consent, with additional consent/assent obtained from parents or guardians and minors. All rights of participants were protected.
A total of 39 female athletes were included from the ACL-SPORTS trial. 3 A full description of the recruitment methods were reported by White et al. 33 Only female athletes from the ACL-SPORTS cohort were included for analysis of reinjury since only 1 of 40 male athletes enrolled in the trial experienced a second ACL injury in the 2 follow-up years. Participants were dichotomized into 2 groups: athletes who sustained a second ACL injury (either graft rupture or contralateral ACL rupture) within 2 years of surgery, and those who did not.
Participants were Level I or II athletes (ie, cutting, jumping pivoting sports) who sustained an isolated primary ACL injury and underwent subsequent ACLR. 8 Participants were between 3 and 9 months after unilateral ACLR, had achieved ≥80% quadriceps strength limb symmetry index (QI), had minimal to no knee joint effusion, 29 full knee range of motion (defined as being equivalent to the uninvolved knee), could hop on each leg without pain, and had successfully initiated a running progression in postoperative rehabilitation. 33 Participants were excluded if they had a concomitant grade III ligamentous injury, >1 cm2 full thickness chondral defect assessed via magnetic resonance imaging (MRI) or arthroscopy, or any history of previous lower extremity surgery or serious injury.
The ACL-SPORTS randomized control trial methods have been published previously. 33 In brief, participants underwent 10 physical therapy sessions of either strengthening, agility, plyometric, and secondary prevention exercises with the addition of perturbation training, or strengthening, plyometric, and secondary prevention exercises alone. 9 As no analyses of the ACL-SPORTS have found differences between groups in knee function, patient-reported outcome measures, second ACL injury, and gait biomechanics at any time point, participants were collapsed across both groups for the purposes of this study.3,6,7,12 For the purposes of this study, data collected postoperatively after 10 training sessions (post-training) were analyzed. All athletes also completed a battery of physical performance tests at post-training. Before returning to sport, all athletes had to achieve ≥90% limb symmetry index on a battery of functional performance tests (ie, isometric quadriceps strength test and 4 single-legged hop tests). All but 1 of the female athletes in this study passed all tests before RTS. This 1 athlete did not achieve ≥90% on isometric quadriceps strength test, but did achieve >90% on all 4 single-legged hop tests. This athlete did not sustain a second ACL injury and had returned to sport by 1 year post-ACLR.
Three patient-reported outcome measures examining psychological factors were collected post-training, including the ACL Return to Sport after Injury (ACL-RSI) scale, TSK-11, and the KOOS QoL subscale. The ACL-RSI is a valid and reliable questionnaire that assesses an athlete’s psychological readiness to RTS, and includes 12 questions about confidence, emotions, and risk appraisal.16,31 Five items within the ACL-RSI measure emotions, 5 items measure confidence in performance, and 2 items measure risk appraisal. The ACL-RSI is scored from 0 to 100, with 0 suggesting a negative psychological response to injury. The TSK-11 assesses kinesiophobia or the fear of movement or reinjury. This measure consists of 11 questions with lower scores indicating less kinesiophobia. Only question 3, “How much are you troubled with lack of confidence in your knee?” from the KOOS QoL subscale was used in this study as previous studies have used this question to measure knee confidence.24,26
All statistical analyses were performed using SPSS Version 24.0 (IBM Corp). Independent t tests and chi-square tests were used to determine group (second injury vs no second injury) differences in demographics and all self-reported measures at the post-training time point. In addition, independent t tests were also used to determine group differences in each category of the ACL-RSI (ie, emotions, confidence, and risk appraisal). A P value ≤0.05 was determined a priori to denote statistically significant differences between groups.
Results
Of 39 female athletes (average age, 18.8 years), 9 (23%) sustained a second ACL injury within 2 years of surgery. There were no significant group differences in age, body mass index (BMI), and weeks from surgery to testing between those who were injured and those who were not (P ≥ 0.17, Table 1). There was a significant difference in the number of graft types between groups (P < 0.01, Table 1). The 4 athletes who sustained an ACL graft rupture had undergone ACLR with a hamstring (HS) tendon autograft. The 5 athletes who sustained a contralateral ACL rupture also had HS grafts in the index knee. There was also a significant group difference in the time from ACLR to achieving RTS criteria, with the second ACL injury group achieving RTS criteria on average 9.1 weeks sooner (P = 0.04, Table 1).
Demographics, graft type, and timing between groups (means and SD)
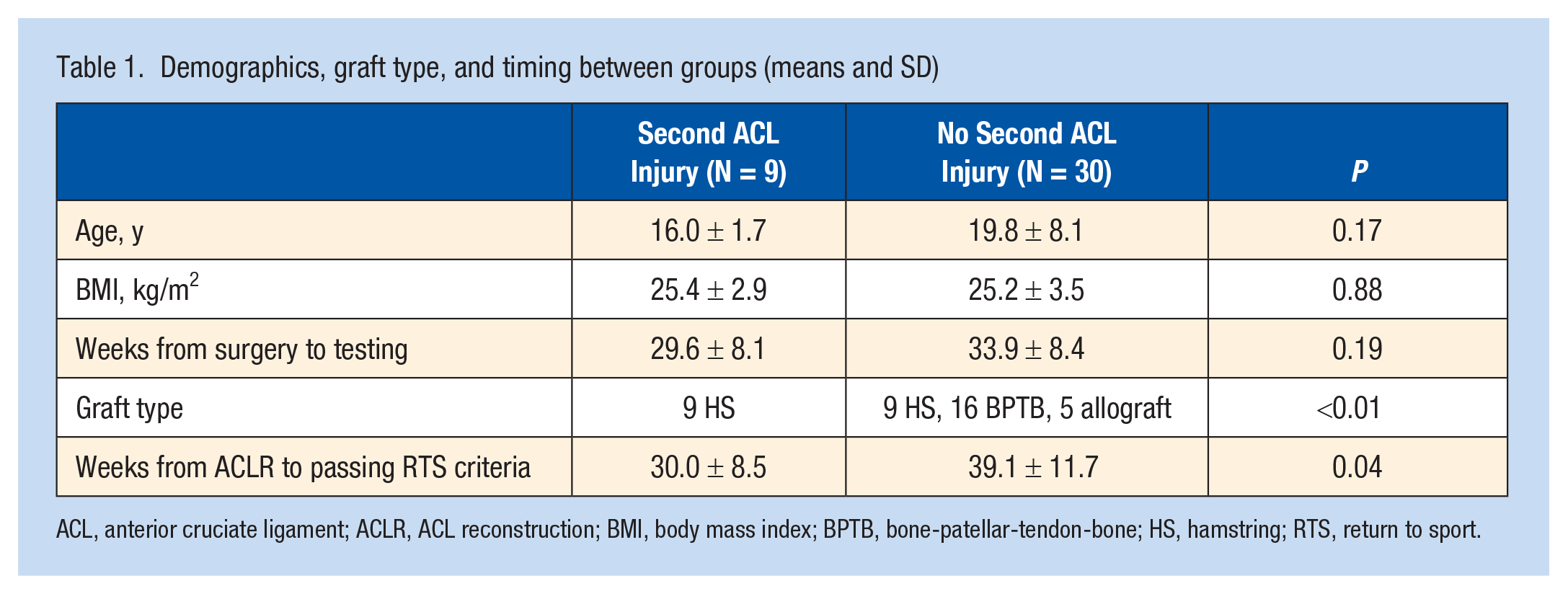
ACL, anterior cruciate ligament; ACLR, ACL reconstruction; BMI, body mass index; BPTB, bone-patellar-tendon-bone; HS, hamstring; RTS, return to sport.
There was a significant group difference in ACL-RSI scores (P = 0.03, Table 2). The second ACL injury group scored 11.9 points higher compared with the no second ACL injury group. Analysis of the individual constructs measured by the ACL-RSI revealed a significant group difference with the risk appraisal questions (P < 0.01, Table 2). The second ACL injury group scored about 20 points higher on the risk appraisal questions compared with the no second ACL injury group. There were no significant group differences in the ACL-RSI questions related to emotions (P = 0.06) or confidence (P = 0.21). There were no group differences in TSK-11 scores (P = 0.51) or the KOOS QoL section, question 3 (P = 0.53).
Psychological measures between groups (means and SD)
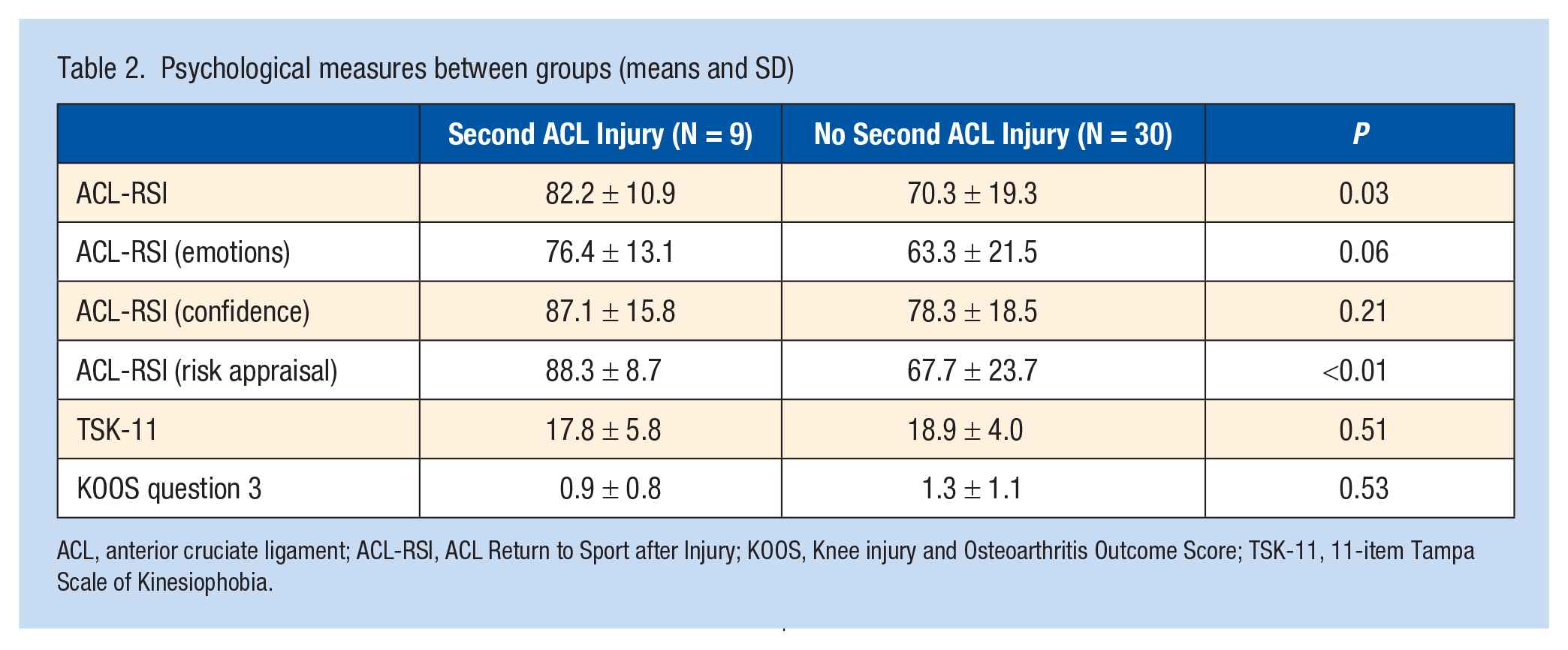
ACL, anterior cruciate ligament; ACL-RSI, ACL Return to Sport after Injury; KOOS, Knee injury and Osteoarthritis Outcome Score; TSK-11, 11-item Tampa Scale of Kinesiophobia.
Discussion
Female athletes who sustained a second ACL injury within 2 years of ACLR had higher psychological readiness scores for RTS assessed after extended postoperative rehabilitation and RTS training before returning to sport. More specifically, the group of athletes who sustained a second ACL injury had significantly higher scores on the ACL-RSI questions related to risk appraisal. Our hypotheses were not supported as we expected the athletes with poorer scores would go on to sustain a second ACL injury. In addition, the group of athletes who sustained a second injury passed RTS criteria 9.1 weeks earlier than athletes who did not sustain a second ACL injury.
Importantly, all ACL graft ruptures in this cohort occurred in athletes who underwent ACLR with HS tendon autograft. Previously published data from the full ACL-SPORTS trial indicated that athletes with HS grafts met clinical milestones and RTS criteria sooner than those with bone-patellar-tendon-bone (BPTB) grafts. 28 As all second ACL injuries in the current study occurred in HS autografts, perhaps a more positive psychological outlook is a surrogate for meeting RTS criteria sooner. Athletes who met RTS criteria sooner likely returned to sports faster, putting them at increased risk for a second ACL injury.
The construct of risk appraisal was included in the ACL-RSI (Webster 2008, PT Sport) because it was determined by Johnston and Carroll 13 to be an essential appraisal for athletes returning to sport. As athletes’ eagerness to return to play grows near the end of rehabilitation, poor risk appraisal can lead to athletes overestimating their abilities and underestimating the severity of their injuries as they return to sports. There are 2 items pertaining to risk appraisal in the ACL-RSI questionnaire. Item 2 asks “Do you think you are likely to reinjure your knee by participating in your sport?” and item 10 asks “Do thoughts of having to go through surgery and rehabilitation prevent you from playing your sport?” During the original development of the ACL-RSI, feedback from athletes suggested that having to go through surgery and rehabilitation a second time was something important to consider in determining readiness to RTS. 31 Athletes who perceive their risk of second injury to be low and have no concerns about having to go through surgery and rehabilitation again may be overconfident in their abilities. Having high confidence scores in these questions may contribute to athletes returning to sport before they are ready, thus increasing their risk of second ACL injury. Others have described the mismatch between patient expectations for RTS without reinjury and the actual risk. 10 Counseling athletes regarding reinjury risk and slowing RTS may be especially critical in athletes with higher scores on the 2 risk appraisal questions.
Several studies have evaluated the association between ACL-RSI scores and RTS rates; however, few studies have looked at the relationship between ACL-RSI scores and second injury rates.1,2,32 McPherson et al 20 evaluated the change in ACL-RSI scores from before surgery to 12 months after ACLR using the modified ACL-RSI and tracked second ACL injuries 2 to 4 years after surgery. Counter to the findings of the current study, the authors reported athletes who experienced a second ACL injury had significantly smaller improvements in ACL-RSI scores over time compared with athletes who did not reinjure, and athletes who sustained a second injury reported significantly lower 12-month ACL-RSI scores, suggesting a poorer psychological response. In a larger study by McPherson et al, 19 younger athletes (≤20 years) who experienced a second ACL injury reported lower psychological readiness scores. King et al14,15 evaluated variables in male patients after ACLR between those who experienced a second ACL injury within 2 years of surgery compared with those with no second ACL injury. Again, counter to the findings of this study, the authors reported lower mean ACL-RSI scores 9 months after surgery in the second injury group, suggesting less confidence, in those who experienced a second ACL injury of the ipsilateral knee, though not statistically significant (P = 0.09), 14 and no difference in scores for those who experienced a contralateral ACL injury compared with no second ACL injury. 15
Psychological constructs of kinesiophobia, measured with the TSK-11, and knee-related confidence, measured by the KOOS QoL subscale question 3, have been assessed in patients who experience a second ACL injury. Paterno et al, 23 utilizing the TSK-11, reported individuals with worse TSK-11 scores at the time of medical clearance to RTS were 13 times more likely to experience an ipsilateral ACL injury within 2 years of returning to athletic activities. In a separate study, Paterno et al 24 identified knee-related confidence to be an essential component of a high-risk profile that was able to predict second ACL injury. The authors defined knee-related confidence using question 3 from the KOOS QoL subscale, which asks, “How much are you troubled with lack of confidence in your knee?”. In the current study, there was no statistically significant difference in scores for the KOOS QoL question or TSK-11 between the second ACL injury group and the no second ACL injury group. In a follow-up study by Paterno et al, 26 at the time of medical release for sports participation, 62.2% of participants were classified as lacking confidence, using this metric, and performed significantly worse on functional, strength, and patient-reported RTS measures. Those participants who were confident at the time of medical clearance were 2 times more likely to experience a second ACL injury. These findings are similar to the results of the current study.
The differences in characteristics of the participants in the current study compared with those of McPherson et al19,20 and King et al14,15 may account for some of the stark differences in findings. The participants in the current study are all female, while the participants in McPherson’s studies were 34% and 44% female, and King’s studies were all male. Sex differences in psychological outcomes after ACLR may be contributing to differences in psychological findings. The participants in the current study were tested approximately 7.4 months and 8.5 months after surgery, while the participants in McPherson’s and King’s studies were tested at 12 months and 9 months, respectively. Psychological perceptions of readiness to RTS have been reported to change over time and may be contributing to study differences.27,35 The participants in the current study who were reinjured were almost 4 years younger (16.0 years), compared with those who were not (19.8 years). The age of participants in McPherson’s studies was not described based on reinjury. The participants in King’s study were matched to uninjured ACLR participants by age and other variables and reported an overall older cohort, even based on injured limb (contralateral injury, 21.3 years; no injury, 21.9 years). Age is associated with an increased risk of second ACL injury and may be a factor in psychological assessment as well.19,34
Paterno et al23,26 had similar findings to the current study and also had similar patient demographics. Although not all female, Paterno reports a higher percentage of female participants, 70.4% (n = 112). The participants in Paterno’s studies were younger, with mean ages of 16.2 years and 17.2 years.23,26 The age of participants in the current study who experienced a second ACL injury is similar to the second ACL injury group by Paterno (current study, 16.0 years; Paterno et al, 26 16.1 years). Paterno’s studies reported similar numbers of graft ruptures and contralateral ACL ruptures in their studies (8 vs 7; 16 vs 19, respectively).23,26 The rates of reinjury are similar between the current study and those of Paterno, at 23% (9/39) and 22% (35/159), respectively. The participants in Paterno’s study were tested at a similar time frame regardless of second injury status (no injury, 8.4 months; second ACL injury, 8.5 months), but similar time frames to the no second injury group in the current study. The similarities in characteristics between Paterno’s studies and the current study may explain similarities in psychological findings.
Limitations
There are several limitations to the current study. First, a major limitation is the small number of study participants, especially the limited number of ACL graft injuries and contralateral ruptures. Second, time from surgery to RTS was not collected. Evidence suggests that athletes who RTS sooner after surgery are at greater risk of second ACL injury and knee reinjury.5,11,25 While we do not know when the athletes in the current study returned to sport, we do know that the second ACL injury group met RTS criteria sooner than the “no second ACL injury” group. Third, as mentioned previously, all participants who experienced a second ACL injury in the current study received an HS tendon autograft. A recent systematic review and meta-analysis of graft failure rates in younger athletes reported a pooled failure rate of 16.6% for HS and 8.5% for BPTB. Laboute et al 18 reported similar graft failure rates for HS and BPTB, at 6.5% and 2.1%, respectively. In our cohort, 4 participants sustained graft ruptures while 5 participants sustained contralateral ACL ruptures. Thus, graft type alone cannot explain our findings. Future research should attempt to further determine the relationships between psychological readiness, graft type, and time to RTS. Fourth, the participants included in this study were all female. Although female athletes are at a higher risk for second ACL injury after ACLR, there is some debate about sex differences in psychological outcomes after surgery. Finally, we extrapolated only a single question from the KOOS QoL to determine knee confidence. To our knowledge, question 3 from the KOOS QoL has not been validated as a stand-alone question.
Conclusion
Young female athletes who experienced a second ACL injury within 2 years after surgery reported higher psychological readiness scores after ACLR, including higher risk appraisal scores. Limited research has been published evaluating second ACL injury rates and associations with psychological constructs. This subgroup of athletes after ACLR may overestimate their abilities, and underestimate the risk of reinjury, putting them at higher risk of reinjury upon RTS. Future research is needed to identify and understand the relationships between psychological factors and second ACL injuries after ACLR, but higher scores are not always better.
Clinical Recommendations
Assessing psychological readiness should be incorporated into RTS decision-making. Previous research indicates that lower psychological readiness is associated with asymmetrical lower extremity kinematics during gait. 36 Perhaps, there is a psychological readiness “sweet spot” for athletes recovering from ACLR. Athletes with high psychological readiness may require a slower RTS progression to mitigate the risk of sustaining a second ACL injury. Athletes with low psychological readiness may require targeted interventions to address altered movement patterns.
Footnotes
The following authors declared potential conflicts of interest: R.Z. received a grant from the National Institutes of Health (NIH) for his PhD and received salary support via grant NCT04504344. E.A. received a grant from the NIH for salary support, and a grant from the Foundation for Physical Therapy Research PODS Level II Scholarship in support of her doctoral thesis. J.J.C. received a grant from the NIH, a grant from ACL-SPORTS randomized controlled trial, a Career Development Award from the Academy of Orthopaedic Physical Therapy, a grant from Veterans Health Administration Eastern Colorado Geriatric Research, Education, and a grant from the Clinical Center Advanced Geriatrics Fellowship. L.S.-M. consulted on an NIH research grant from the University of Kentucky, an NIH research grant from the University of Michigan, and the Brigham & Women’s Orthopedics Sports’ new research and performance center, and is also on the National Football League Scientific Advisory.