
Abstract
Background:
While concussions are common pediatric injuries, a lack of agreement on a standard definition of recovery creates multiple challenges for clinicians and researchers alike.
Hypothesis:
The percentage of concussed youth deemed recovered as part of a prospective cohort study will differ depending on the recovery definition.
Study Design:
Descriptive epidemiologic study of a prospectively enrolled observational cohort
Level of Evidence:
Level 3.
Methods:
Participants aged 11 to 18 years were enrolled from the concussion program of a tertiary care academic center. Data were collected from initial and follow-up clinical visits ≤12 weeks from injury. A total of 10 recovery definitions were assessed: (1) cleared to full return to sports; (2) return to full school; (3) self-reported return to normal; (4) self-reported full return to school; (5) self-reported full return to exercise; (6) symptom return to preinjury state; (7) complete symptom resolution; (8) symptoms below standardized threshold; (9) no abnormal visio-vestibular examination (VVE) elements; and (10) ≤1 abnormal VVE assessments.
Results:
In total, 174 participants were enrolled. By week 4, 63.8% met at least 1 recovery definition versus 78.2% by week 8 versus 88.5% by week 12. For individual measures of recovery at week 4, percent recovered ranged from 5% by self-reported full return to exercise to 45% for ≤1 VVE abnormality (similar trends at 8 and 12 weeks).
Conclusion:
There is wide variability in the proportion of youth considered recovered at various points following concussion depending on the definition of recovery, with higher proportions using physiologic examination-based measures and lower proportions using patient-reported measures.
Clinical Relevance:
These results further emphasize the need for a multimodal assessment of recovery by clinicians as a single and standardized definition of recovery that captures the broad impact of concussion on a given patient continues to be elusive.
Keywords
Concussion is a common pediatric injury evaluated across clinical practice settings, yet much remains unknown regarding optimal diagnostic techniques, prognostication strategies, and treatment to accelerate recovery.15,30,34 These knowledge gaps provide exciting opportunities to rapidly advance the field. In the past decade alone, interventional trials have been published guiding clinicians on the benefits (or lack thereof) of strict rest3,42; the value of targeted rehabilitation programs, including aerobic exercise and visio-vestibular rehabilitation26,27,28; and the utility of pharmacologic treatments. 2 In addition, large, observational cohorts of children and adolescents have been evaluated to elucidate factors associated with prolonged recovery and assist providers in risk stratification.35,36,44 However, all of these studies have a common significant limitation: a lack of agreement on a standard definition of “recovery.”
Multiple systematic reviews have noted the large variety of clinical outcomes utilized across concussion studies, including symptoms, neurocognitive testing results, return to activity, and physician clearance.14,21 There is even variability within these categories: while symptom-based recovery definitions are common, studies differ on whether they utilize complete symptom resolution as the definition of recovery,3,42 or compare with a return to preinjury baseline (with disagreement on the ideal definition for how close to preinjury baseline a patient must return before being considered recovered).16,44 Further complicating the issue is the potential inability to collect the varied clinical outcomes across all health care settings and disparate loss-to-follow-up rates depending on the outcome definition chosen. 5 The lack of agreement on a standard definition of recovery has significant implications for clinicians and researchers alike. As multiple between-group differences (based on age, sex, comorbidities, and concussion history) in recovery trajectories emerge, 21 the definition of recovery, with the potential influence of these between-group differences, is critical. 11
In light of these challenges, systematic reviews have provided an overview of the various recovery definitions available14,21; however, a rigorous comparison of how these definitions affect the ultimate determination of recovery outcomes in a single population has yet to be undertaken. The objectives of this study were to use an observational, prospective cohort of concussed youth to (1) describe various commonly used definitions of concussion recovery, including definitions based on symptoms, physiologic examination-based abnormalities, physician-assessed clearance, and self-assessment; (2) compare the differences in the proportion of concussed youth who would be considered recovered by each of these definitions up to 12 weeks after injury; and (3) determine the degree to which data are not available, either due to lack of documentation/measurement or due to the participant not returning for clinical care, for each definition of recovery in prospectively collected clinical data of concussed adolescents. We hypothesized that there would be significant variability in the proportion of youth recovered among the various definitions of recovery.
Methods
Study Population
As part of a larger prospective, observational study of clinical and device-based measures of concussion among concussed youth, we enrolled participants seeking treatment for a concussion from a concussion program that evaluates acute concussion in a large tertiary care pediatric center; results from this prospective cohort study have been reported in other manuscripts.7,10,41 We included participants aged 11 to 18 years in the current study. Enrollment criteria required that the participant (1) be diagnosed with concussion by a trained sports medicine pediatrician in accordance with the 5th Consensus Statement on Concussion in Sport 34 ; (2) sustained a concussion from a sports- or recreation-related injury; and (3) presented to the referral clinical setting within 28 days of injury. Participants had their initial clinical visit during the period August 25, 2017 through December 13, 2019 and were asked to return for follow-up care per clinical guidelines. Data were collected at the initial and follow-up clinical visits. No additional visits were conducted for research purposes only. In-person follow-up clinical care was paused on March 13, 2020, due to the novel coronavirus pandemic; therefore, the end date of enrollment was chosen to allow for up to 90 days of in-person clinical follow-up for all participants. If a participant sustained >1 concussion during the enrollment time period, data related to the first concussion only were included. Informed consent from a parent or guardian and child assent was obtained for those under 18 years of age at enrollment; informed consent was obtained for those aged 18. This study was approved by the Institutional Review Board of Children’s Hospital of Philadelphia.
Clinical Visits
Data from initial clinical and subsequent follow-up visits within 90 days of injury listed below were included in the analysis. Demographic data, including sex, age at concussion, and race/ethnicity, were abstracted from the electronic health record (EHR).
At each visit, participants completed self-reported questionnaires and a battery of clinical measures were used to evaluate their injury. Measures obtained from the questionnaires included symptoms pre- (at initial visit) and postinjury (at initial and follow-up visits) using the postconcussion symptom inventory (PCSI) scale for (adolescent PCSI for ages 13-18 years and child PCSI [cPSCI] for ages 11-12 years). 38 School and exercise behavior were also obtained from the questionnaires. At the initial visit, participants also completed a self-administered baseline survey to report characteristics of the concussion, including date of injury, and past medical history, including previous concussion(s).
Clinical measures included the Sport Concussion Assessment Tool, 5th edition (SCAT-5) and the 9 elements of the visio-vestibular examination (VVE). In addition to orientation, memory, and attention testing, the SCAT-5 includes a question related to self-assessed recovery (“If 100% is feeling perfectly normal, what percent of normal do you [currently] feel?”). 4 The VVE is a battery of 9 maneuvers designed to evaluate visual function, vestibular function, and gait. The examination has been implemented across multiple specialties, including sports medicine, emergency medicine, and primary care,1,8 and has been shown to be reliable in these settings. 6 Its elements include (1) smooth pursuit, evaluating the participant’s ability to track in a horizontal plane for 5 repetitions, with a deficit defined as symptom provocation (eye fatigue, pain, dizziness, headache, or nausea), jerky or jumpy eye movements, or nystagmus 10 ; (2) horizontal and vertical saccades, with the participant’s eyes moving rapidly between 2 fixed objects, in both the horizontal and vertical plane, with a deficit defined as symptom provocation (eye fatigue, pain, dizziness, headache, or nausea) with 20 or fewer repetitions 41 ; (3) horizontal and vertical gaze stability, or angular vestibulo-ocular reflex, where the participant’s eyes are fixed and his or her head moves in the horizontal or vertical plane, with a deficit defined as symptom provocation (eye fatigue, pain, dizziness, headache, or nausea) with 20 or fewer repetitions 41 ; (4) nearpoint of convergence (NPC), assessing for break (double vision) using a standard Astron accommodative rule (Gulden Ophthalmics) with a single column 20/30 card, with a receded NPC defined as break at >6 cm 39 ; (5) right and left monocular accommodation, assessing clear to blur distance with 1 eye open using a standard Astron accommodative rule, with a deficit defined based on age-related distance using Hofstetter’s formula 37 ; and (6) complex tandem gait, where the participant is evaluated walking in tandem for 5 steps forward and backward, eyes open and closed; a point is given for each step off the line, as well as the presence of sway on each of the 4 conditions, with a deficit defined as a composite score of at least 5 (on a scale of 0-24). 10
Recovery Definitions and Methods
A total of 10 different definitions of recovery were created, plus a composite measure, and assessed at each clinical visit for each patient, as listed below.
Clinician Assessments
The first set of recovery definitions involved assessments by the sports medicine specialty clinician regarding clearance to return to athletic activities and school - a multifactorial decision based on patient symptoms, injury history and comorbidities, and physical examination findings. If the sports medicine clinician documented in the EHR that the participant was fully cleared to return to athletic activity with no restrictions, the participant was recovered as defined by cleared for full return to sports (1). If the clinician documented in the EHR that the participant was able to return to school full-time without any academic accommodations, the participant was recovered as defined by return to full school without accommodations (2).
Self-Reported Recovery
The next set of recovery definitions relied on participant self-report, as obtained from the SCAT-5 as well as the questionnaires. Participants who responded with 100% in response to the SCAT-5 regarding “what percent of normal” the participant felt were considered recovered as defined by self-reported return to normal (3). The participant also answered questions regarding their current behavior regarding school and exercise on the separate questionnaires. If the participant reported returning to school at “100% of preinjury workload,” they were considered recovered as defined by self-reported full return to school (4). If the participant reported returning to “100% of preinjury exercise/sports participation,” they were considered recovered as defined by self-reported full return to exercise (5).
Symptom-Based Recovery
The third set of recovery definitions was based on self-reported symptoms using the PCSI/cPCSI. For those participants who provided both an assessment of self-reported PCSI/cPCSI symptoms for the preinjury period and at a postinjury clinical visit, those who reported that <3 symptoms were worse at current state compared with preinjury state were considered recovered as defined by symptom return to preinjury state (6). 44 Further, we used postinjury PCSI/cPCSI symptom assessments to determine that those who reported no symptoms postinjury were (7) recovered as defined by complete symptom resolution. Finally, we compared the total PCSI/cPCSI symptom score to predetermined thresholds normalized for age and sex based on data for uninjured youth (PCSI <9 for women, PCSI <6 for men, and cPCSI <10 for both sexes). 10 These participants were categorized as recovered as defined by symptoms below standardized threshold (8).
VVE-Based Recovery
The final set of recovery definitions was derived from the VVE. Participants who had normal assessments on all 9 elements were considered recovered as defined by 0 abnormal VVE assessments (9). Since nonconcussed youth can present with deficits in some of these elements,9,10 an additional VVE recovery definition was used; participants who had ≤1 abnormal assessment were considered recovered as defined by ≤1 abnormal VVE assessments (10).
Recovery by Any Definition
Finally, we included a composite recovery measure, whereby the patient was determined to be recovered if they met criteria for any of the 10 definitions described above.
Time to Recovery
For each participant, we determined whether they were recovered or not recovered, based on available data for each of the recovery definitions at each clinical visit. For each recovery definition, we calculated the time to recovery as the number of days from the date of injury to the date of the earliest clinical visit at which the recovery definition was met. We then categorized time to recovery into weekly intervals through 12 weeks of follow-up such that the 1st week began with the date of injury (day 0) through day 6, the 2nd week included days 7 through 13, through the 12th week, which included days 77 through 83. Further, data were collapsed in 4-week increments (recovered by week 4, the accepted definition of prolonged post-concussion symptoms [PPCS]19,44 recovered by week 8, and recovered by week 12).
Data Analysis
We described the distribution of demographic characteristics, past medical history, and the timing of follow-up visits among participants. For each recovery definition, we categorized each participant’s recovery status at the end of the 4-, 8-, and 12-week follow-up periods (through day 27, 55, and 83 postinjury, respectively) as (1) recovered, such that the participant met documented criteria for the specified recovery definition during ≥1 clinical visit in the follow-up period; (2) not recovered, such that the participant did not meet criteria for the specified recovery definition at any clinical visit during the follow-up period (specifically, the provider documenting that the participant had not reached said criteria); (3) not documented, such that data were not available due to the measure not being documented (or measured) at the clinic visit; and (4) no return to clinic, such that data were not available as the participant did not return for clinical care.
Results
A total of 174 concussed youth were enrolled. Slightly over half (54.6%) of participants were female and 82.8% identified as non-Hispanic White (Table 1). The median age at injury was 15 years (interquartile range [IQR] 14, 16). Almost half (45.4%) reported experiencing a previous concussion before enrollment into this study.
Demographic and clinical characteristics of concussed adolescents (n = 174)
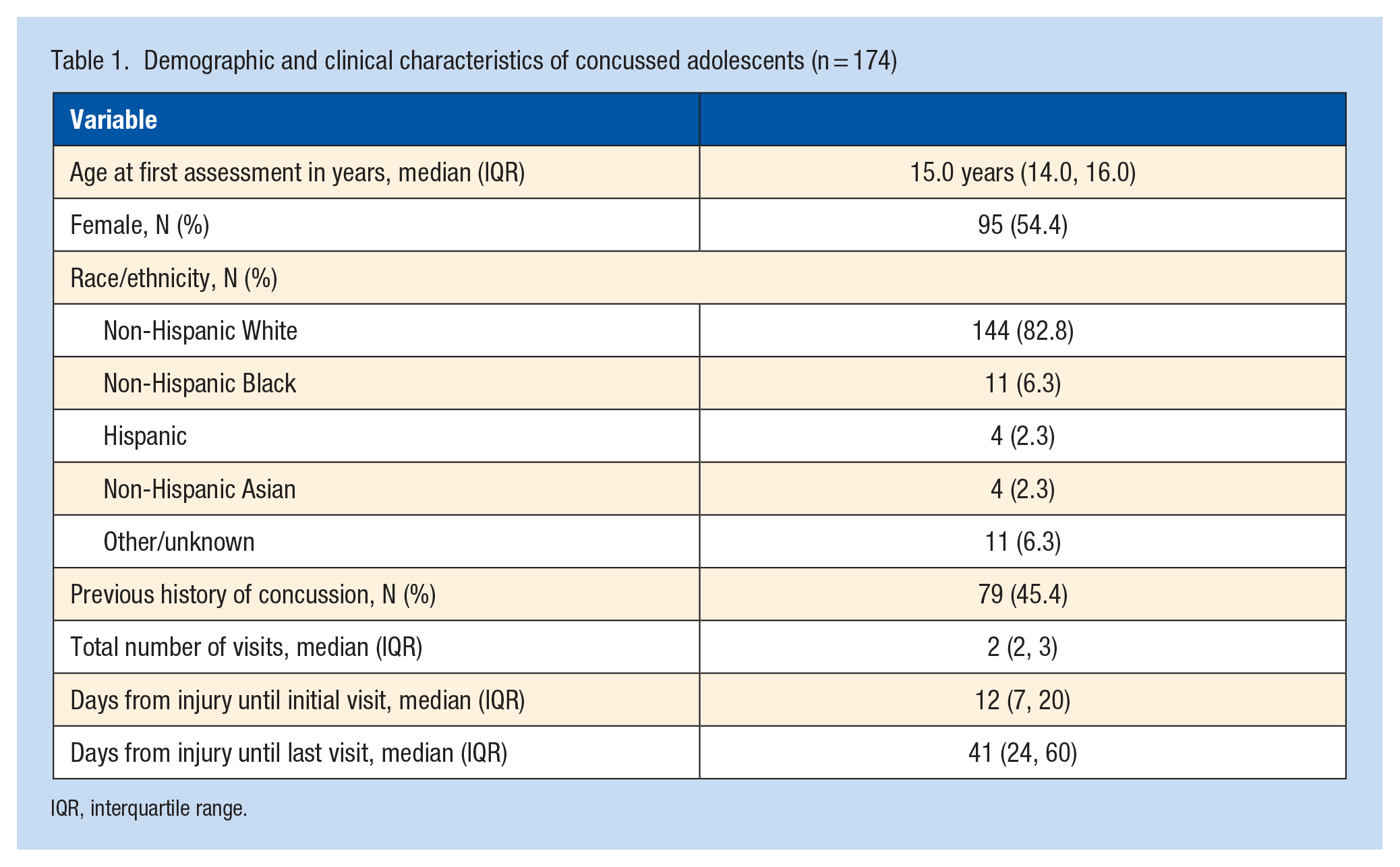
IQR, interquartile range.
Participants had a total of 419 clinical visits. The median time from date of injury to date of initial visit was 12 days (IQR: 7, 20). Most participants returned for ≥1 follow-up clinical visit after their initial visit, as only 17 (9.8%) participants had just 1 clinical visit. The median time from date of injury to date of last visit was 41 days (IQR: 24, 62). The distribution of patients continuing to seek care at each week after injury is shown in Figure 1. At 4 weeks postinjury, 146 (83.9%) continued to have clinical follow-up. In addition, 73 (42.0%) were still following up clinically 8 weeks after injury, and 17 (9.8%) were still following up at 12 weeks after injury.
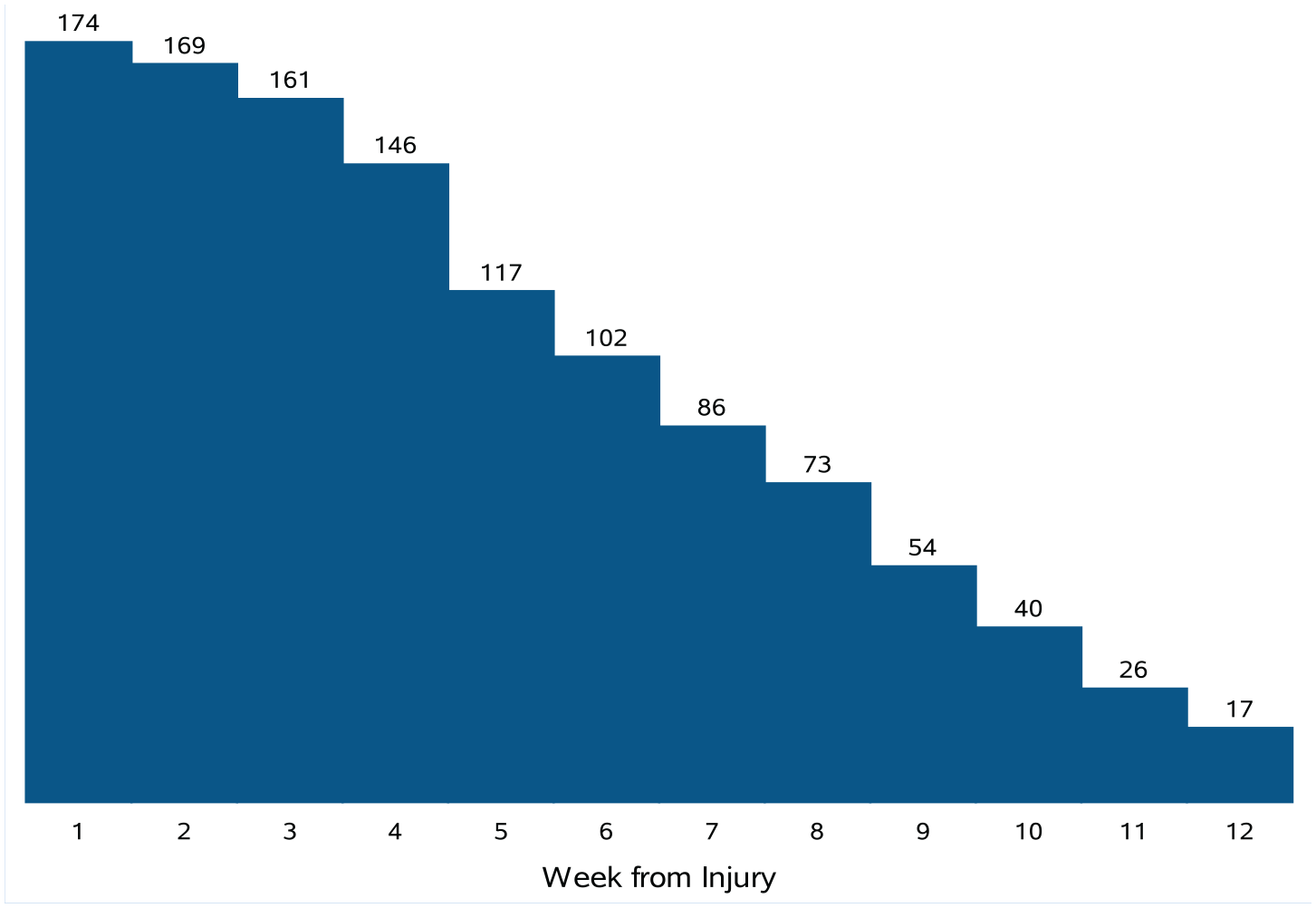
Number of concussed participants remaining for follow-up by week.
Figure 2a-c demonstrates the distribution of those deemed recovered, not recovered, and with data unavailable either due to a lack of documentation or a participant not returning for clinical care at 4, 8, and 12 weeks postinjury, respectively, for each of the 10 recovery definitions, as well as the composite definition. For the individual definitions, the percent recovered by week 4 of follow-up ranged from 4.6% using the definition of self-reported full return to exercise to 45.4% for ≤1 abnormal VVE components (ranks for each of the 10 definitions are provided in Figure 2). Using the composite definition of recovery, 63.8% of the participants met ≥1 of these 10 recovery definitions by 4 weeks. Similar trends were seen at 8 weeks (with a range of 7.5% for self-reported full return to exercise to 64.4% for ≤1 abnormal VVE components) and 12 weeks (range of 9.8% for self-reported full return to exercise to 79.3% for ≤1 abnormal VVE components). Through 12 weeks of clinical follow-up, 88.5% of all participants met ≤1 of the recovery definitions.
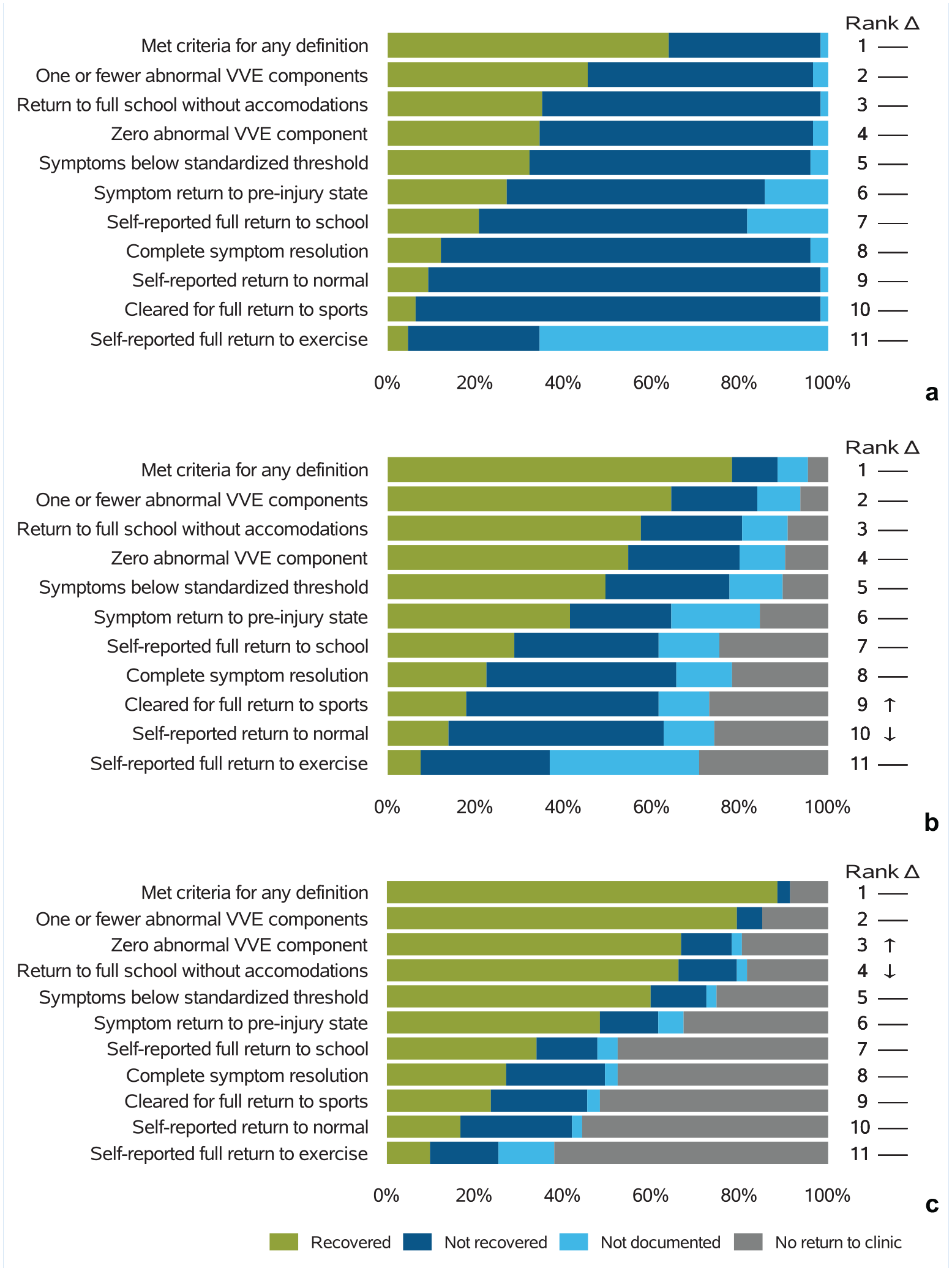
Proportion recovered by each definition, including those with unavailable data either due to measure not being documented or participant not returning for clinical care at 4 (a), 8 (b), and 12 (c) weeks. Rank corresponds to the order in definitions from highest (1) to lowest (11) of the proportion recovered. Δ refers to the trend related to rank changes from 4 to 8 weeks and 8 to 12 weeks. VVE, visio-vestibular examination.
In addition to differences in the proportion recovered by each definition, we also observed differences in unavailable data for each of the definitions. The proportion with unavailable data due to a lack of documentation by week 12 ranged from 0% for ≤1 abnormal VVE components to 12.6% for self-report full return to exercise, and the proportion with unavailable data due to the participant not returning for clinical follow-up by week 12 ranged from 14.9% for ≤1 abnormal VVE components to 62.1% for self-report full return to exercise. The distributions at weeks 4, 8, and 12, when those with unavailable data were removed, are shown in Figure 3. Excluding those with unavailable data, at weeks 4, 8, and 12, the percentage of youth meeting ≥1 recovery definition was 64.9%, 88.3%, and 96.9%, respectively. For the individual measures, we found a similar rank order of definitions within the individual elements excluding those with unavailable data (Figure 3) compared with our overall rank order in Figure 2. Specifically, at week 12, 38.6% of the subjects met recovery criteria by self-reported full return to exercise when excluding those with unavailable data, whereas 93.2% were considered recovered with ≤1 abnormal VVE components (Figure 3c).
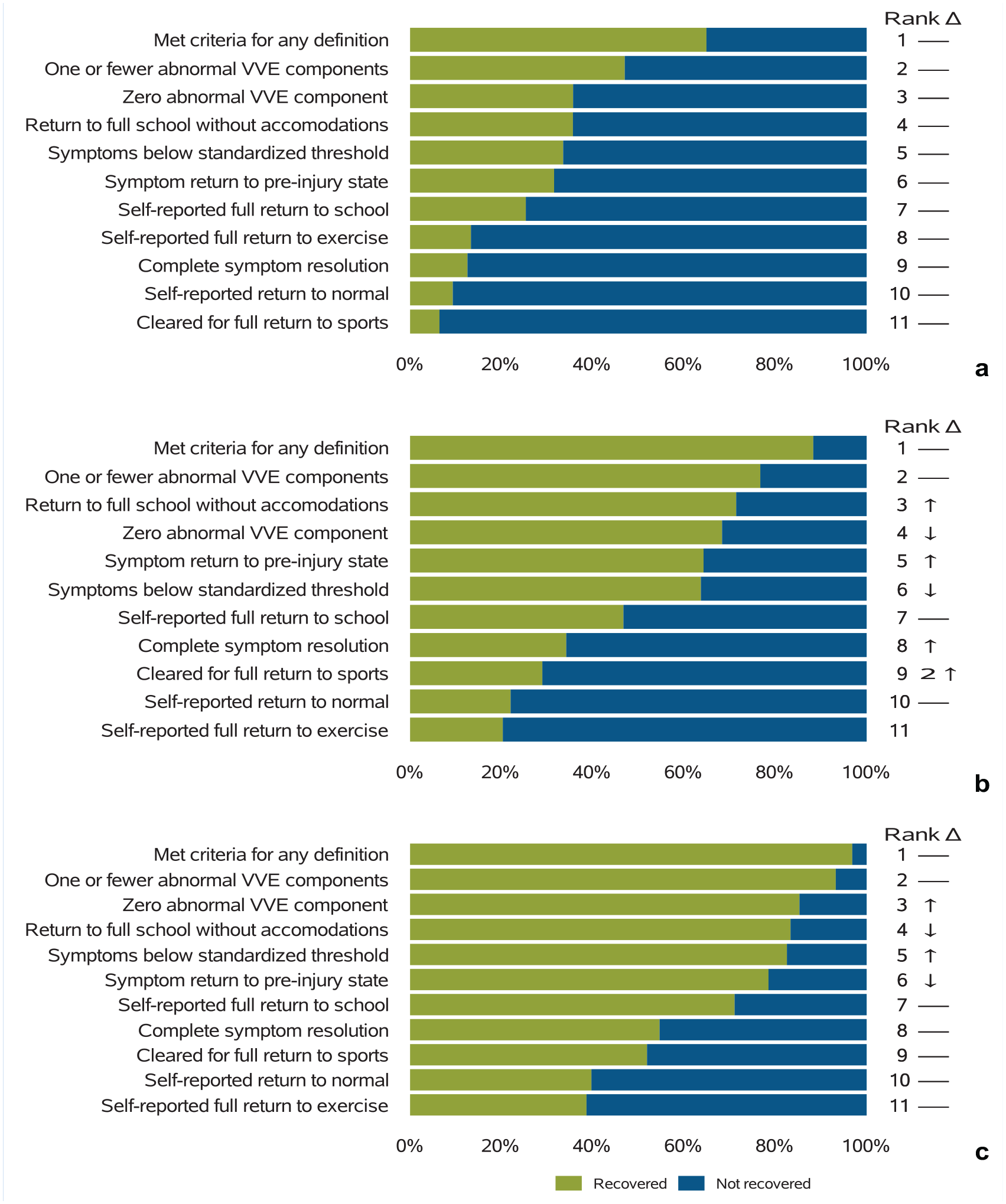
Proportion recovered for each definition, excluding those with unavailable data, at 4 (a), 8 (b), and 12 (c) weeks postinjury. Rank corresponds to the order in definitions from highest (1) to lowest (11) of the proportion recovered. Δ refers to the trend related to rank changes from 4 to 8 weeks and 8 to 12 weeks. VVE, visio-vestibular examination.
Discussion
This study assessed how recovery outcomes after adolescent concussion in a single prospective cohort varied depending on the definition of recovery. Overall, we found high variability between symptom-based definitions, physiologic examination-based abnormalities, physician-assessed clearance, and self-assessment, with a higher proportion of youth deemed recovered at each interval using physical examination abnormalities and a lower proportion using self-assessment definitions. In addition, in this sample of clinically collected data, there was wide variability in unavailable data, either due to a lack of documentation or the participant not returning for clinical care, among the various recovery definitions, indicating that regular queries of an EHR for these types of data may not result in robust assessment.
Symptoms have traditionally been considered the gold standard in both concussion diagnosis and assessment of recovery. 15 In a recent systematic review by Haider et al 14 evaluating studies that utilized ≥2 measures to define recovery from pediatric concussion, 100% of the 43 included studies had ≥1 symptom-based recovery definition. Likewise, the most impactful interventional trials of concussion management have heavily utilized symptom-based recovery definitions,27,42 and the largest clinical model for predicting prolonged symptoms relied exclusively on symptom changes to define recovery. 44 However, our data showed wide variability between the definitions of symptom-based recovery: at 4 weeks after injury (a cut-off used to determine PPCS in previous work),19,44 only 12.1% of the sample reported complete symptom resolution, compared with 27.0% reporting a return to preinjury baseline and 32.2% below a predetermined threshold of symptom burden, differences that extended out over the 12 weeks of follow-up. The most stringent symptom-based definition within our data, complete symptom resolution, may be an unattainable (and unrealistic) goal, as previous work has shown the majority of nonconcussed teenagers report ≥1 concussion-like symptom on standardized symptom scales even without having sustained a concussion. 22 To account for this, many, including Zemek et al, 44 have advocated for a comparison with a self-reported preinjury baseline in creating the largest predictive model to date for PPCS. Specifically, the definition utilized in their study (recovery = <3 symptoms worse than baseline) was evaluated as one of the recovery definitions in our study. Hearps et al 16 compared several different approaches to define “return to baseline.” However, all of these approaches (including our own) are limited by the reliance on retrospectively assessing a baseline symptom score.
In light of the variability and subjectivity of symptom reporting, many have advocated for the inclusion of physiologic, examination-based markers of recovery. 34 We therefore included in our analysis an assessment of 2 different definitions of recovery using the 9 elements of the VVE. Interestingly, at each time point, these definitions provided the highest proportion of recovered participants (more than via the 3 symptom-based definitions). The vestibular/oculomotor screening tool (VOMS), like the VVE, evaluates visio-vestibular function with a few key differences, as the VOMS does not include monocular accommodation or balance testing, and includes fewer repetitions for gaze stability and saccadic testing. The VOMS has been found to show a similar recovery trajectory to concussion-like symptoms, with a slightly longer duration until resolution. 17 Multiple studies have found that objective physiologic markers of function, including those assessed by functional magnetic resonance imaging (MRI), diffusion tensor imaging, and cerebral blood flow, have abnormalities that outlast the duration of symptoms.24,25 The difference between previous work and our current study may be related to specific differences in the VVE compared with other physiologic measures such as functional MRI or cerebral blood flow. Alternatively, and perhaps more likely, this difference may be a result of documentation. At each 4-week interval, some of the smallest proportions of unavailable data for the recovery definitions were the 2 definitions utilizing VVE elements, likely related to the standardized performance and documentation of the VVE for all patients in the concussion program. Regardless of the etiology, the differences between recovery assessment via symptom-based and examination-based definitions are pertinent for clinicians and researchers alike.
Of the 10 measures assessed, the 3 that showed lower proportions of recovery at each time point included self-assessment measures, specifically the patient reporting feeling 100% back to normal, self-reported return to school, and self-reported return to exercise. These self-assessed measures are important, as the impact of pediatric concussion may go beyond quantifiable symptom scales or physiologic testing. Recently, a multimodal assessment of quality of life (health-related quality of life [HRQOL]) has been recommended as part of an outcome assessment for pediatric injury, 32 with evaluation of concussion patients finding impairment of HRQOL, as a patient-reported outcome, for extended times after pediatric injury. 13 While there does appear to be correlation between symptom burden and HRQOL in children, 18 these results suggest the importance of a comprehensive, holistic evaluation when assessing recovery beyond a simple assessment of subjective symptoms. Future research to further understand how to assess HRQOL outcomes and incorporating them into care is warranted.
In addition to this variability in the proportion determined to be recovered among our outcome measures, there was variability in the degree of unavailable data in this sample of clinically collected data, either due to a lack of documentation or to the participant not returning for clinical care. Assessments timed with clinical visits are likely the easiest to capture, particularly for large, observational studies; however, they rely on both treating clinician and patient availability, and their schedule is nonstandardized across patients as it is influenced by numerous noninjury factors. In addition, it is possible (and likely) that several recovery definitions are “attained” by a patient before attending the inperson visit, adding an extra degree of complexity to determining recovery status. Recently, remote patient monitoring techniques have emerged as a way to capture more granular information more systematically regarding symptoms and activity in concussed youth and has shown to be successful in remotely obtaining information regarding symptom levels, physical activity, cognitive activity, and sleep on a daily basis.20,43 Moving forward, more routine application of remote monitoring techniques may reduce the missingness and both standardize and increase the frequency of assessment timepoints of clinically collected data used for quantifying concussion outcomes.
The underlying etiology of the variability described in this study is likely multifactorial. Part of this variability likely stems from the heterogeneous nature of concussion and these definitions measuring different components of the underlying pathophysiology of the injury. As noted above, the timing of in-person visits adds a layer of complexity to the variability, given our inability to measure the exact timepoint at which these measures reach the definition of recovered. Finally, it is important to note the subjectivity of several of these commonly used measures and the appeal of more objective measures of injury, including biofluid-based biomarkers (such as blood and saliva) and device-based measures of injury (such as the pupillary light reflex and eye tracking.12,23,31,33 Moving forward, these objective markers have the potential to remove subjectivity not just from concussion diagnosis but also the determination of recovery.
The variability in recovery definitions found in this study has implications for clinicians caring for concussed youth, as well as researchers evaluating risk factors for prolonged recovery time and indications for potential novel interventions. Between-group differences in recovery have been demonstrated, to various degrees, in previous studies among sex, age, and concussion history. 21 However, it is very possible these differences are reliant on the definition of recovery chosen, thus making comparisons among studies difficult. As an example, over the past several years, multiple studies have identified sex as an important biologic variable that can influence recovery time; multiple observational studies have found female children and adolescents exhibit a longer duration of postinjury symptom reporting when compared with male counterparts.21,35,44 Choosing the definition of recovery, however, impacts this between-sex comparison. In their study, Desai et al 11 found that time to return to activity for concussed female youth, when controlling for time to presentation to a concussion specialist, was not different from that for concussed men, yet time to resolution of visio-vestibular deficits was prolonged for women regardless of time until initial presentation. Yet another study showed that while complete symptom resolution was different between men and women 4 weeks after injury, there was no significant difference in visio-vestibular deficits. 5 Future work to more fully assess the impact of various definitions of recovery based on observed group differences (eg, sex, age, concussion history, and comorbidities) is needed.
There are several limitations to our study. As we included only participants from a single institution’s concussion program, our data may not be generalizable to a broader population; specifically, as a referral population seen on average 12 days from injury, our group may include more severely injured participants, or those at higher risk for prolonged recovery compared with the general population (eg, the percentage of our participants with a previous concussion, a known risk factor for PPCS, is higher than other studies). 44 However, our institution has several geographic locations that pull from diverse patient populations and also sees concussion patients soon after injury, directly accessed by patients and their families without requiring an initial emergency or primary care visit for referral. In addition, by assessing recovery variability among those with sports- and recreation-related injury, we reduce some inherent variability to recovery that can occur via other injury mechanisms.29,40 Lastly, our data are limited by missingness within our recovery definitions, due either to the patient being lost to follow-up before reaching the specified definition or to inconsistent documentation in the EHR. However, the extent of missingness, as discussed above, is valuable information to consider for those planning data collection for future studies timed with clinical visits, particularly in light of the rigor with which our data were collected.
In conclusion, these data show wide variability in the proportion of youth considered recovered from a concussion at various points after injury depending on the definition of recovery chosen, with higher proportions using physiologic exam-based measures and lower proportions using patient-reported measures. These results further emphasize the need for a multimodal assessment of recovery by clinicians, and multiple measures of recovery by researchers, as a single and standardized definition of recovery that captures the broad impact of concussion on a given patient continues to be elusive.
Footnotes
The following authors declared potential conflicts of interest: K.B.M., C.C.M., M.R.P., K.B.A., and C.L.M. received a grant from Pennsylvania Department of Health (DOH). K.B.A. and C.L.M. received grant R01NS097549 from the National Institute of Neurological Disorders and Stroke.