
Abstract
Background:
The lumbar multifidus (LMF), as a dynamic stabilizer of the lumbar spine, may play an important role in the prevention of overuse-related back complaints.
Hypothesis:
LMF morphology is associated with trunk stability and differs between symptomatic and asymptomatic skiers.
Study Design:
Cohort study.
Level of Evidence:
Level 3.
Methods:
A total of 85 youth skiers (28 females, mean age, 14.7 ± 0.7 years; 57 males, mean age, 14.9 ± 0.5 years) underwent anthropometric assessments, an estimation of biological maturation, a magnetic resonance imaging- and ultrasound-based examination of LMF morphology, and a biomechanical quantification of deadbug bridging stabilization performance. Athletes were categorized as symptomatic if they had registered at least 1 significant overuse-related back complaint episode in the 12 months before the main examination.
Results:
Male skiers showed a greater LMF size (ie, anatomical cross-sectional area [ACSA]) than female skiers, except for vertebral body L5, where no difference was found (8.8 ± 1.8 cm2 vs 8.3 ± 1.4 cm2, P = 0.18). Conversely, female skiers displayed longer fascicles than male skiers (5.8 ± 0.8 cm vs 5.4 ± 0.8 cm, P = 0.03). Skiers aged under 16 years (U16) skiers had greater values for LMF size and fascicle length than U15 skiers. Maturity offset was associated with L5 LMF size (R2 = 0.060, P = 0.01), fascicle length (R2 = 0.038, P = 0.04), and muscle thickness (R2 = 0.064, P = 0.02). L5 LMF size was associated with trunk stability (R2 = 0.068, P = 0.01). Asymptomatic skiers showed on average a 12.8% greater value for L5 LMF size compared with symptomatic skiers (P = 0.04).
Conclusion:
There are sex- and age-related differences in LMF morphology in youth competitive alpine skiers. Moreover, the ACSA at the level of the lumbar vertebral body L5 undergoes changes during biological maturation, shows a small, but significant association with trunk stability, and differs between symptomatic and asymptomatic skiers with back complaints.
Clinical Relevance:
The observed association of muscle structure (ie, L5 LMF ACSA) with functional aspects (ie, trunk stabilization capacity) and clinical representation (ie, overuse-related back complaints) further highlights the important role of the multifidus muscle for training and injury prevention in youth competitive alpine skiers around the growth spurt.
Competitive alpine skiers suffer from various traumatic and overuse injuries.18,31 Among overuse injuries, the lower back is one of the most affected body regions in youth competitive alpine skiers. 28 While skiing, the lumbar spine is exposed to adverse loading conditions that may favor the occurrence of overuse injuries (such as spine flexion, lateral flexion and rotation in combination with high vibration loads). 30 A previous study showed that U16 skiers presented different overuse-related structural abnormalities in the lumbar spine, some of which were classified as clinically relevant and resulted in sport participation restriction. 25 Furthermore, pain intensity was significantly associated with years of sport participation, number of competitions per season, and number of ski days per season in adolescent competitive alpine skiers. 2 Studies on adult elite skiers showed that overuse-related back complaints occur both in the preparation phase (off- and on-snow training) and during the competition season.11,12
The role of the lumbar multifidus (LMF) in overuse-related back complaints has been studied extensively. 10 LMF size, more specifically anatomical cross-sectional area (ACSA), appears to be a relevant variable in low back pain.17,21,34 For example, in patients with acute unilateral low back pain, the LMF ACSA was found to be smaller on the symptomatic side than on the nonsymptomatic side. 17 Furthermore, patients with chronic low back pain showed a smaller ACSA of the LMF than healthy subjects, specifically at the L5 vertebral level. 34
Given its characteristic morphology (ie, large CSA and a small fiber length-to-muscle length ratio), the LMF is designed to produce high forces and can therefore act as a dynamic stabilizer of the lumbar spine. 35 However, studies that have investigated the relationship between LMF muscle architecture and overuse injuries of the lower back are still limited. In a recently published cross-sectional magnetic resonance imaging (MRI) study examining 108 youth competitive alpine skiers, Peterhans and colleagues 25 showed that a smaller relative LMF ACSA was significantly associated with the more frequent occurrence of overuse-related spinal abnormalities such as disc protrusions and end plate changes. However, to date, no study has investigated a potential relationship between LMF morphology (muscle size and architecture) and overuse-related back complaints in youth competitive alpine skiers.
In another recent study, Ellenberger and colleagues 5 proposed a novel biomechanical approach to quantify the stabilization capacity of athletes’ posterior chain, which plays a central role, especially in alpine skiing, using deadbug bridging (DBB). They demonstrated that DBBdisplacement (ie, the maximum amplitude of the relative vertical displacement between 2 hip markers) was significantly associated with overuse-related back complaints in U16 skiers. As the LMF belongs to the paraspinal muscles, the next step would be to determine whether LMF morphology is associated with DBB performance.
Therefore, the aims of the present study were to (1) provide reference values regarding LMF morphology of female and male youth competitive alpine skiers, (2) investigate the influence of biological maturation on LMF morphology, (3) verify whether LMF morphology is associated with DBB performance, and (4) compare the LMF morphology of symptomatic and asymptomatic skiers and examine the potential clinical relevance of these findings.
Methods
Study Design, Participants, and Ethics
The present study was designed as a cohort study involving anthropometric measurements, noninvasive maturity offset estimates, MRI and ultrasound (US)-based LMF muscle imaging, and a biomechanical quantification of DBB performance. To complement this, skiers were monitored prospectively for overuse-related back complaints in the 12 months before the main examinations. Recruitment was carried out via advertisement and information events within the youth development structure of the Swiss Ski Federation (Swiss-Ski). Female and male skiers affiliated with certified regional performance centers (RLZ/RPC) were eligible to participate. The exclusion criteria were as follows: skiers should not have any systematic pathologies, such as inflammatory arthritis, and should not have undergone rehabilitation before study participation. A total of 85 youth competitive alpine skiers formed the data pool for the analysis of the present study, of which 28 were female (mean age, 14.7 ± 0.7 years) and 57 were male (mean age, 14.9 ± 0.5 years). The underlying study protocol was approved by the local ethics committee of the Canton of Zurich (KEK-ZH-NR: 2017-01395) and was conducted according to the ethical standards of the Declaration of Helsinki and national laws. All participants provided written informed consent.
Anthropometric Measures and Maturity Offset Estimations
The anthropometric measures involved the assessment of body mass with a body scale, and body height and sitting height with a tape measure. The noninvasive method of Mirwald and colleagues, 23 which has already been validated in youth alpine skiers, 24 was used for the estimation of biological maturation. The formula determines the maturity offset based on the anthropometric data and the chronological age of the skiers. The maturity offset reflects the difference between the assessment date and the time when the skier is expected to reach, or have reached, the maximum growth rate. In study participants with negative values, the time of maximum growth rate is therefore still to be reached, while in study participants with positive values, this time has already passed.
Muscle Imaging
All muscle imaging procedures were carried out at the Swiss Centre for Musculoskeletal Imaging (SCMI). While MRI represents the gold standard for obtaining the 2-dimensional (2-D) area of a given muscle (ie, ACSA), 13 US imaging offers the possibility to investigate the muscle architecture variables fascicle length (Lf), pennation angle (PA), and muscle thickness (MT). 9 Accordingly, MRI scans and US measurements were conducted.
The MRI measurements were performed with a 3-T MRI scanner (Magnetom Prisma, Siemens). The ACSA analysis of the LMF was obtained from axial T2-weighted MRI images by an experienced rater (L.P.) using image processing software (ImageJ, National Institutes of Health). For the lumbar vertebral bodies (L1-L5), the centers and the cranial and caudal adjacent sections were identified in the sagittal plane (Figure 1A), and the ACSA of the LMF was measured in the associated transversal plane (Figure 1B). Thus, 3 sections per vertebral body and side were analyzed. For statistical analysis, the average of the 2 sides for each lumbar vertebral body was calculated (ie, L1-L5 ACSAavg). The intrarater reliability of a similar procedure using the same image processing software has been shown to be high in a previous study. 6
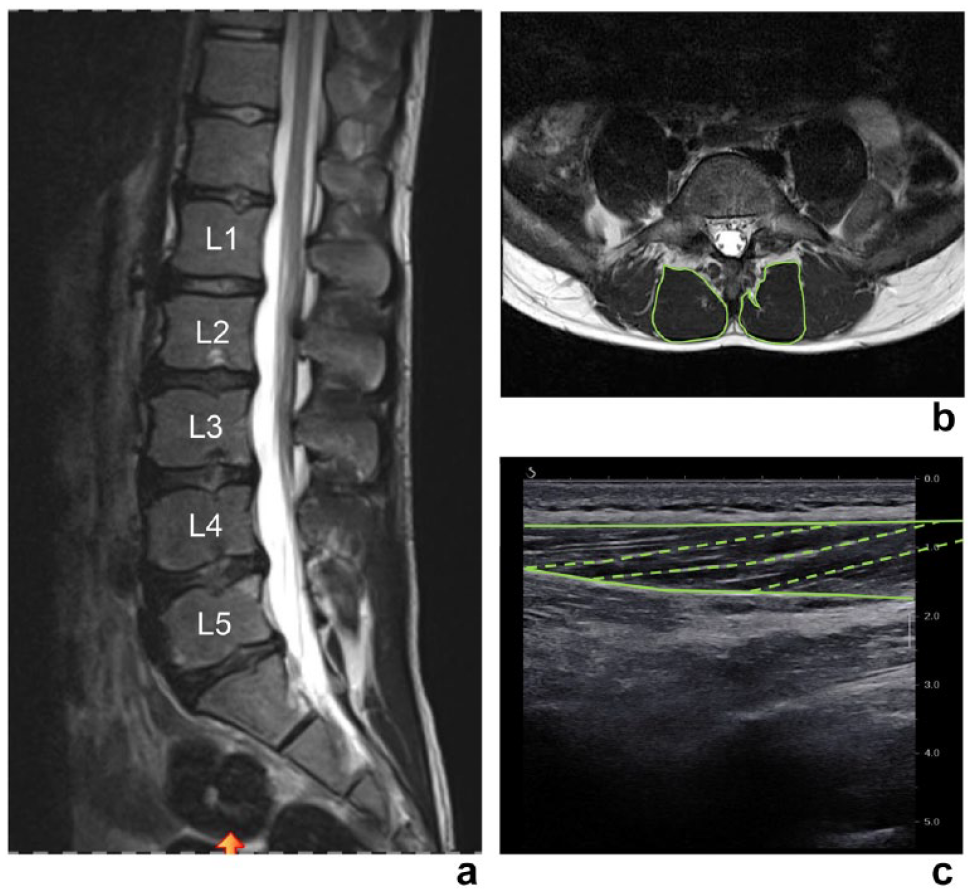
Exemplary MRI and US scans. (A) Sagittal MRI scan and marked lumbar vertebral bodies; (B) transversal MRI scan with segmented ACSAs of the LMF; (C) static longitudinal US scan with traced aponeuroses and fascicles. ACSA, anatomic cross-sectional area; LMF, lumbar multifidus; MRI, magnetic resonance imaging; US, ultrasound.
The US measurements were conducted by an experienced operator (M.V.F.) using an US device (Aixplorer Ultimate, SuperSonic Imagine). Study participants were instructed to lie prone on the massage bed with their ankles on the edge of the bed so that their feet could be kept in a neutral position and the hip and knee joints were extended. In addition, a pillow was placed under the abdomen of the study participants to ensure a neutral spinal position. The lumbar vertebral bodies (L1-L5) were first identified by a longitudinal US scan and marked. A 5 cm linear transducer (SuperLinear SL18-5, SuperSonic Imagine) was then used to acquire a static longitudinal image for the right and left sides to analyze the muscle architecture. Image analysis was performed by an experienced rater (D.P.F.) using image processing software (ImageJ, National Institutes of Health). Figure 1C shows an example of a static longitudinal US scan with traced aponeuroses and fascicles. For each image, the superficial and intermediate aponeurosis and 4 fascicles were drawn. The respective 4 values for Lf, PA, and MT were averaged. For statistical analysis, the average value of the 2 sides for each muscle architecture variable was calculated (ie, Lfavg, PAavg, MTavg).
Because studies on the reliability of LMF muscle architecture (ie, Lf, PA and MT) analysis are lacking to date, we reanalyzed the muscle architecture variables in 10 randomly selected participants. The spreadsheet for consecutive pairwise analysis by Hopkins 19 was used to determine intrarater reliability. The spreadsheet was used to calculate intraclass correlation coefficients (ICC)(3,1), with “3” indicating the ICC type with subjects as random effect and trials as fixed effect, and “1” referring to the reliability of single repeated measurements and standardized typical errors (STEs). 19 ICC values were classified based on the definitions of Koo and Li 22 : <0.5 indicates weak reliability, 0.5 to 0.75 indicates moderate reliability, 0.75 to 0.9 indicates good reliability, and >0.9 indicates excellent reliability. STEs were interpreted based on commonly used thresholds 29 : 0.2 (small), 0.6 (moderate), 1.2 (large), 2.0 (very large), and 4.0 (extremely large).
DBB Performance Assessment
The protocol for the assessment of DBB performance has been described in detail previously by Ellenberger and colleagues. 5 Briefly, 2 reflective markers were placed on the right and left iliac bones and on the lateral and medial malleolus. DBB execution was recorded using a 200 Hz 3-dimensional (3-D) optoelectronic motion capture system (Vicon, Oxford Metrics). For the starting position, study participants were instructed to lie supine, abduct the arms 90° (palms up), and abduct the legs until the distance between the heels was equal to that of the elbows. The study participants were then instructed to raise the hips without changing the position of the shoulders and heels. From this position, the task was to lift 1 heel off the ground, flex the hip and knee to a joint angle of 90°, and hold this position for 3 seconds. Afterwards, the leg was brought back to the starting position in a controlled manner, with the aim of keeping the hip as stable as possible. Three repetitions were performed per side while keeping the hips off the ground. The marker trajectories were then identified using motion capture software (Vicon Nexus v.2.7, Oxford Metrics) and exported to the programming and numeric computing platform (MATLAB R2016b, The MathWorks, Inc.) for calculations. For the variable DBBdisplacement, the maximum amplitude (in millimeters) of the vertical displacement between the hip marker on the stabilizing side (reference marker) and the hip marker on the side where the leg was lifted was calculated.
Overuse-Related Back Complaints Surveillance
Surveillance of overuse-related back complaints was conducted over a period of 12 months before muscle imaging using the Oslo Sports Trauma Research Centre (OSTRC) health problems questionnaire. 3 Data collection and management were carried out in a secure and web-based software platform (REDCap). The participants received an individualized link to the questionnaire every second week. If the participants did not complete the questionnaire within 2 days, they were reminded via email. If the questionnaire was still not completed after 3 days, the participants and their parents were contacted by manual text message. The time window to complete the questionnaire was a maximum of 7 days from the time of the first message. At the end of the 12-month prospective OSTRC-based health problem survey, the data collected were reviewed retrospectively for accuracy and completeness via interviews and physical examinations by an experienced sports physician (S.F.). In a subsequent data analysis, all overuse-related back complaints were classified as “substantial” or “not substantial” based on the OSTRC severity score. Problems that resulted in “moderate or severe reductions in training volume,” “moderate or severe reductions in sports performance,” or “complete inability to participate in sports” were considered “substantial.” This was the case if the skiers had selected option 3, 4, or 5 in question 2 or 3 of the OSTRC questionnaire. 3 The classification was used to distinguish symptomatic and asymptomatic skiers.
Differentiation From Previously Published Studies
Regarding DBB performance assessment and the OSTRC-based registration of overuse-related back complaints, it must be noted that the results of an overlapping, but not identical, part of the underlying dataset have already been published in a previous study. 5 In the present study, these data have now been reanalyzed for the purpose of relating the novel LMF muscle imaging data with trunk stability and back complaints.
Statistical Analyses
Statistical analysis was performed using statistical software (SPSS Statistics 26, IBM). Normal distribution of the data was tested using the Kolmogorov-Smirnov test, graphical techniques (ie, histograms and quantile-quantile plots) and shape parameters (ie, skewness and kurtosis coefficients). 26 In the case of a normal distribution of the data, parametric tests were applied. If the Kolmogorov-Smirnov test was significant but the skewness and kurtosis values were below the defined normality reference limits of <2.0 and <7.0, respectively, 37 the parametric tests were supported by bias corrected accelerated (BCa) bootstrapping with 10,000 samples. Beyond these reference limits, nonparametric tests were applied.
Anthropometric measures, maturity offset estimations, and LMF morphology variables are presented as the means and standard deviations and were analyzed for sex- and age-specific differences using independent samples t tests. Linear regression analyses were performed to investigate the associations between maturity offset and LMF morphology. The associations between LMF morphology and DBB performance (ie, DBBdisplacement) were tested using multiple linear regression analyses (backward method). Finally, the differences in LMF morphology of symptomatic and asymptomatic skiers were analyzed using independent samples t tests.
Results
Intrarater Reliability of US-Based LMF Morphology Assessments
Intrarater reliability for the Lfavg variable was classified as good (ICC(3,1), 0.85; 95% CI, 0.49-0.96), and STE was classified as moderate (STE, 0.44; 95% CI, 0.30-0.81). Good intrarater reliability (ICC(3,1), 0.76; 95% CI, 0.29-0.93) and moderate STE (STE, 0.54; 95% CI, 0.37-0.98) were also revealed for the variable PAavg. For the variable MTavg, excellent intrarater reliability (ICC(3,1), 0.98; 95% CI, 0.94-1.00) and a small STE (STE, 0.14, 95% CI, 0.10-0.26) were found.
Overview of the Anthropometric Measures and Maturity Offset Estimations
An overview of the anthropometric measurements and maturity offset estimations is shown in Table 1. Female and male skiers did not differ significantly in age (P = 0.19), but there was a significant age difference between the group means of U16 skiers and U15 skiers (P < 0.001). Female skiers demonstrated a significantly higher value for maturity offset than males (P < 0.001). The maturity offset value of the U16 skiers was also significantly higher than that of the U15 skiers (P = 0.003). Male skiers were significantly taller than females (P = 0.02). Similarly, U16 skiers were significantly taller than U15 skiers (P = 0.005). Body mass was not significantly different between the 2 sexes (P = 0.87). However, the U16 skiers were significantly heavier than the U15 skiers (P = 0.003). For body mass index, there was a significant difference both in sex, where female skiers had a higher value than male skiers (P = 0.04), and in age groups, where U16 skiers had a higher value than U15 skiers (P = 0.04).
Overview of the anthropometric measures and maturity offset estimations a
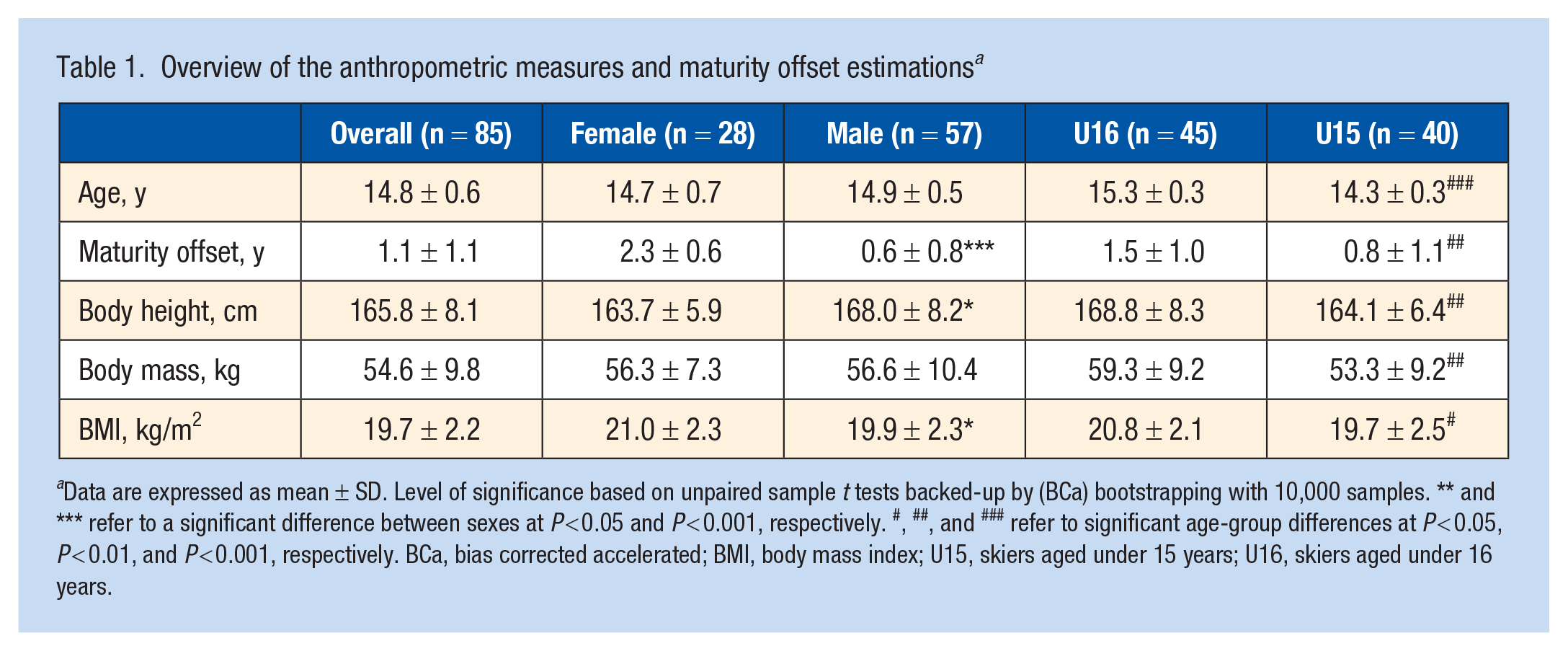
Data are expressed as mean ± SD. Level of significance based on unpaired sample t tests backed-up by (BCa) bootstrapping with 10,000 samples. ** and *** refer to a significant difference between sexes at P < 0.05 and P < 0.001, respectively. #, ##, and ### refer to significant age-group differences at P < 0.05, P < 0.01, and P < 0.001, respectively. BCa, bias corrected accelerated; BMI, body mass index; U15, skiers aged under 15 years; U16, skiers aged under 16 years.
Overview of LMF Morphology in Youth Competitive Alpine Skiers
An overview of the LMF morphology in youth competitive alpine skiers is presented in Table 2. Male skiers showed significantly higher values of ACSAavg at the level of vertebral bodies L1 (P = 0.001), L2 (P = 0.005), L3 (P = 0.03), and L4 (P = 0.02) than female skiers. At vertebral body L5, no significant difference between female and male skiers was found (P = 0.18). The Lfavg value was greater for female skiers than for male skiers (P = 0.03). For PAavg and MTavg, there were no significant differences between sexes (P = 0.25 and P = 0.21, respectively). U16 skiers demonstrated significantly larger ACSAavg than U15 skiers at any vertebral body level (L1, P = 0.001; L2, P = 0.002; L3, P = 0.02; L4, P = 0.03; L5, P = 0.04). For Lfavg, U15 skiers showed a significantly higher value than U16 skiers (P = 0.04). No significant differences between age groups were found for PAavg and MTavg (P = 0.06 and P = 0.94, respectively).
Overview of LMF morphology in youth competitive alpine skiers a
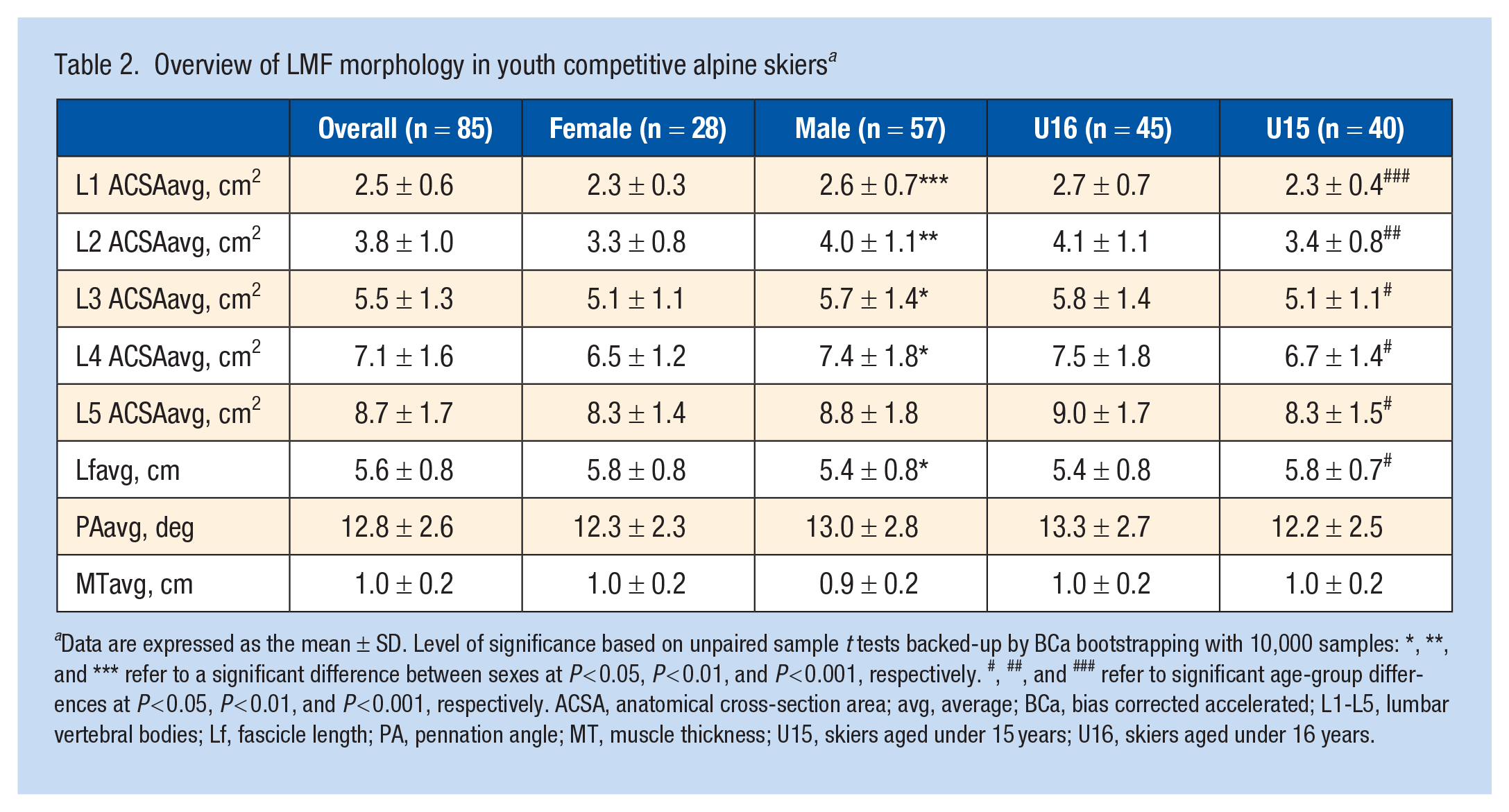
Data are expressed as the mean ± SD. Level of significance based on unpaired sample t tests backed-up by BCa bootstrapping with 10,000 samples: *, **, and *** refer to a significant difference between sexes at P < 0.05, P < 0.01, and P < 0.001, respectively. #, ##, and ### refer to significant age-group differences at P < 0.05, P < 0.01, and P < 0.001, respectively. ACSA, anatomical cross-section area; avg, average; BCa, bias corrected accelerated; L1-L5, lumbar vertebral bodies; Lf, fascicle length; PA, pennation angle; MT, muscle thickness; U15, skiers aged under 15 years; U16, skiers aged under 16 years.
Associations of Maturity Offset With LMF Morphology
Appendix Table A1 (available in the online version of this article) shows the results of the linear regression analyses regarding the associations between the predictor maturity offset and the LMF morphology. The maturity offset was significantly associated with the L5 ACSAavg (P = 0.01). The maturity offset explained 6% of the variance in L5 ACSAavg (R2 = 0.060). No significant associations were found between maturity offset and ACSAavg for the other vertebral body levels (L1, P = 0.07; L2, P = 0.13; L3, P = 0.11; L4, P = 0.22). The maturity offset was significantly associated with Lfavg (P = 0.04) and MTavg (P = 0.02). For Lfavg, the maturity offset explained 3.8%, and for MTavg, it explained 6.4% of the variance (R2 = 0.038 and R2 = 0.064, respectively). For PAavg, there was no significant association with maturity offset (P = 0.93).
Association of LMF Morphology With DBB Performance
Figure 2 shows the result of the multiple regression analysis (backward method) regarding the association of LMF morphology and DBB performance (ie, DBBdisplacement). The L5 ACSAavg had a significant influence on DBBdisplacement (P = 0.01). L5 ACSAavg explained 6.8% of the variance in DBBdisplacement (R2 = 0.068). L1 ACSAavg, L2 ACSAavg, L3 ACSAavg, L4 ACSAavg, Lfavg, PAavg, MTavg, and the potential confounder maturity offset were removed from the model by the backward method.
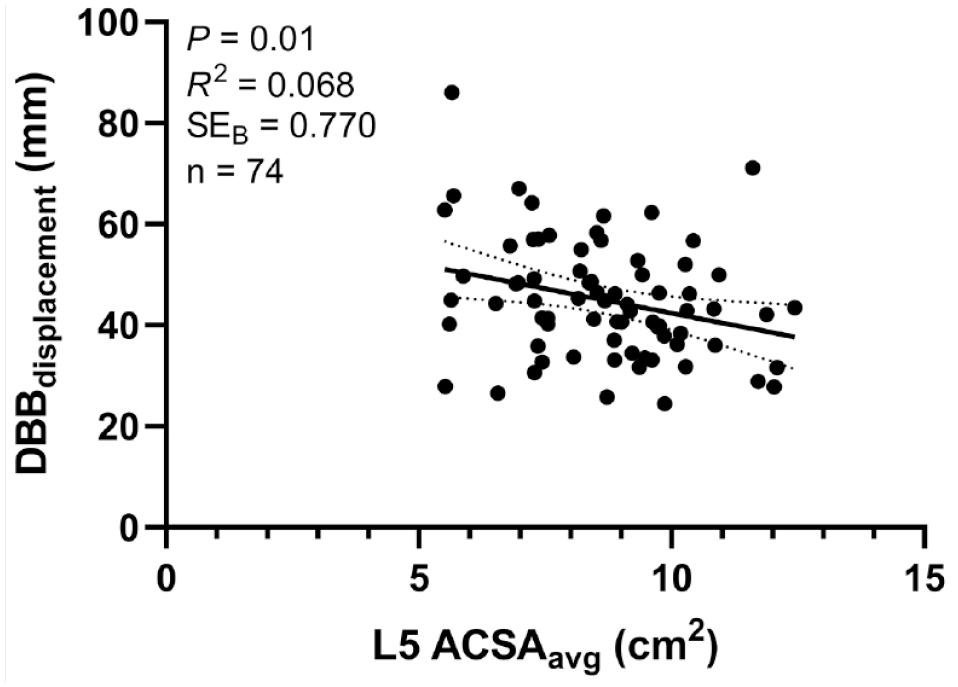
Linear regression analysis assessing the association of LMF morphology with DBB performance (ie, DBBdisplacement). The predictors L1 ACSAavg (cm2), L2 ACSAavg (cm2), L3 ACSAavg (cm2), L4 ACSAavg (cm2), Lfavg (cm), PAavg (deg), MTavg (cm), and the potential confounder maturity offset were removed from the model by the backward method. ACSA, anatomical cross-sectional area; avg, average; DBB, deadbug bridging; L1-L5, lumbar vertebral bodies; Lf, fascicle length; LMF, lumbar multifidus; PA, pennation angle; MT, muscle thickness.
Differences in LMF Morphology Between Symptomatic and Asymptomatic Youth Competitive Alpine Skiers
The differences in LMF morphology between symptomatic and asymptomatic skiers are shown in Table 3. Asymptomatic skiers showed on average a 12.8% greater value at the L5 ACSAavg compared with symptomatic skiers (P = 0.04). For lumbar vertebral body levels L1-L4, no statistically significant differences were found in ACSAavg (L1, P = 0.079; L2, P = 0.23; L3, P = 0.06; L4, P = 0.06). Similarly, no statistically significant differences were found in muscle architecture variables between symptomatic and asymptomatic skiers (Lf, P = 0.87; PA, P = 0.54; MT, P = 0.86).
LMF morphology in symptomatic and asymptomatic youth competitive alpine skiers a
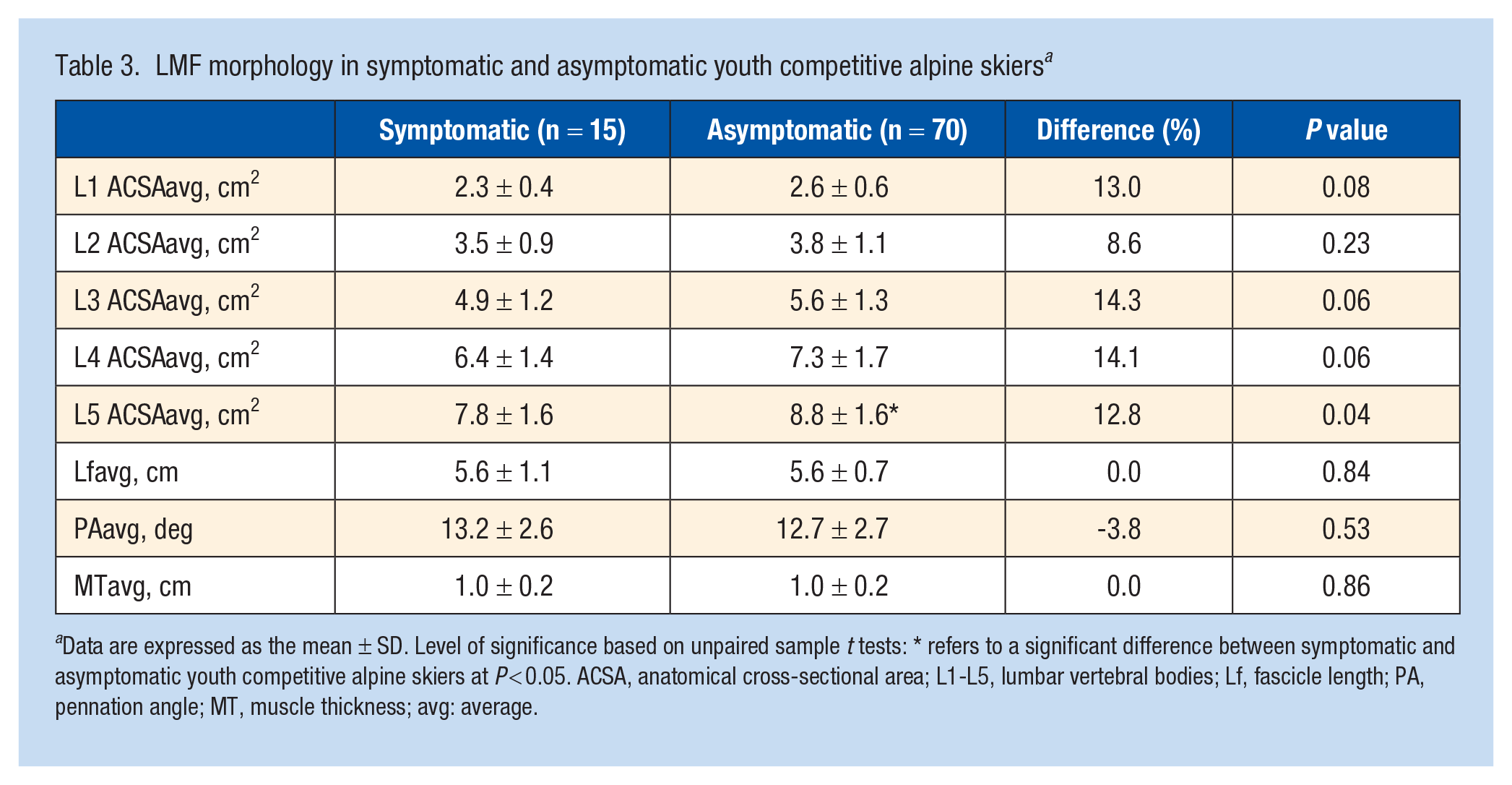
Data are expressed as the mean ± SD. Level of significance based on unpaired sample t tests: * refers to a significant difference between symptomatic and asymptomatic youth competitive alpine skiers at P < 0.05. ACSA, anatomical cross-sectional area; L1-L5, lumbar vertebral bodies; Lf, fascicle length; PA, pennation angle; MT, muscle thickness; avg: average.
Discussion
The major findings of this study were as follows: (1) male skiers showed greater ACSAavg values than females, except at vertebral body L5, where no significant difference between sexes was found; (2) the value for Lfavg, on the other hand, was greater for female skiers than for male skiers; (3) U16 skiers had greater ACSAavg and Lfavg values than U15 skiers; (4) maturity offset was associated significantly with L5 ACSAavg, LFavg, and MTavg; (5) L5 ACSAavg was associated significantly with DBBdisplacement; and (6) asymptomatic skiers showed significantly greater L5 ACSAavg than symptomatic skiers.
LMF Morphology in Youth Competitive Alpine Skiers
At lumbar vertebral levels L1-L4, ACSAavg was larger in male skiers than in female skiers. In contrast, this sex-specific difference was not found at the L5 level. Regarding spine levels L2-L4, previous studies also showed larger values for male than for female study participants.14,34 For L5, some studies found larger values for the male sex,32,36 but there is also a study that found no sex-specific differences at the L5 level in an asymptomatic population. 14 Because female skiers were more developed than males in terms of biological maturation at the time of measurement (maturity offset: 2.3 ± 0.6 vs 0.6 ± 0.8) and a significant association between maturity offset and ACSAavg was found exclusively for the L5 vertebral body level, it is plausible that a sex-specific difference will manifest at this level as well. Regarding muscle architecture variables, there was a significant difference in Lf between the sexes. The Lf was greater in female skiers than in male skiers. Due to the different maturity offset values and the fact that a significant association was found between maturity offset and Lf, it would also be conceivable here that this sex-specific difference is still changing. Although to different degrees, studies of lower extremity muscles show that Lf increases with the progression of biological maturation. 33
Comparison of the age groups showed that older skiers had greater ACSAavg at all vertebral body levels than younger skiers. In a cohort of healthy asymptomatic participants and patients with chronic low back pain, age was not associated with any of the vertebral levels studied (ie, L2-L5), although the majority of the former were younger. 14 Similarly, another study found no significant effect of age on LMF size at vertebral body levels L4 and L5. 32 Accordingly, chronological age seems to influence LMF size, especially during the growth spurt, whereas in adults, differences cannot be attributed to age. Thus, adolescence appears to be a “window of opportunity” to increase the ACSA of the LMF, while it remains rather constant in adulthood. Among the muscle architecture variables, only Lf resulted in a significant difference between the age groups. Interestingly, the U16 skiers had shorter fascicles than the U15 skiers. This is noteworthy because Lf, especially in lower extremity muscles, generally increases during growth. 33 Conversely, although not to a statistically significant degree, PA was greater in U16 skiers than in U15 skiers. Thus, there must have been loading conditions that favored radial muscle fiber hypertrophy (ie, PA increase) over longitudinal conditions (ie, Lf increase). However, from an injury prevention point of view, an adaptation of both dimensions would theoretically be beneficial. Due to the nature of the sport, the spine is often in flexion, lateral flexion, and rotation. 30 Resistance training strategies for longitudinal muscle fiber hypertrophy would include lengthening muscle actions and/or isometric muscle actions at long muscle-tendon unit lengths.1,7
Associations of Maturity Offset With LMF Morphology
The linear regression analyses revealed that maturity offset was associated significantly with ACSAavg of the L5 vertebral body level, while no significant associations were found for the other lumbar vertebral body levels. This differs fundamentally from a chronological age-specific analysis, in which U16 skiers showed greater ACSAavg than U15 skiers at all lumbar vertebral bodies. Accordingly, LMF ACSAavg, particularly at the level of the lumbar vertebral body L5, can have multiple influencing factors. Among the muscle architecture variables, significant associations resulted between the maturity offset and Lfavg as well as between the maturity offset and MTavg, whereas no significant association resulted for PA. Regarding Lf, it is well described in the literature that, with the progression of biological maturation, Lf adapts due to the growth of segments in terms of greater length. 33 The association between maturity offset and MTavg is reasonable due to the placement of the transducer in the region between L3 and L5, as it has already been shown that MT correlates with ACSA. 8 In summary, although small in magnitude, biological maturation was found to be significantly associated with variables that increase with radial (ie, increase in ACSA and MT) and variables that increase with longitudinal muscle fiber hypertrophy (ie, increase in Lf), primarily in the region of the lumbar vertebral body L5.
Association of LMF Morphology With DBB Performance
Multiple regression analysis (backward method) showed a significant association between the predictor L5 ACSAavg and DBBdisplacement, whereas the remaining predictors and the possible confounder maturity offset were removed from the model. In this context, L5 ACSAavg explained 6.8% of DBBdisplacement. This may not appear to be a strong association at first consideration, given that different muscles of the posterior chain are involved in the execution of the exercise. It is nevertheless remarkable that a significant association was found between a single muscle region and DBBdisplacement. In a similar context, it has previously been shown that DBBdisplacement was associated significantly with overuse-related back complaints in U16 skiers, 5 and the present study now has shown that DBBdisplacement can be explained, at least in part, by the LMF ACSA at the level of the lumbar vertebral body L5. Accordingly, it may be argued that, as part of a more holistic injury prevention screening protocol that assesses functional and structural predictors of overuse-related back complaints in youth skiers, both DBBdisplacement and L5 ACSAavg should be assessed.
Differences in LMF Morphology Between Symptomatic and Asymptomatic Youth Competitive Alpine Skiers
The results of the independent samples t tests showed a significant difference between symptomatic and asymptomatic (regarding overuse-related back complaints) skiers only for the variable L5 ACSAavg. On average, asymptomatic skiers had a 12.8% greater L5 ACSAavg than symptomatic skiers. Differences in LMF ACSA between symptomatic and asymptomatic low back pain patients have been shown in several studies using different imaging techniques, including US,14,34 MRI,20,21 or computed tomography. 4 Moreover, LMF ACSA has been reported to be smaller in patients with chronic low back pain than in healthy subjects.10,27 Interestingly, this difference manifests mainly at the lumbar vertebral level L5.14,34 This is also shown by studies that have investigated the effect of loading and unloading on LMF ACSA.15,16 While a 12-week stabilization program in young cricket players with low back pain resulted in an increase in the L5 ASCA of the LMF, 16 the ACSA of the lumbar vertebral levels L3-L5 decreased significantly after several months of microgravity exposure (ie, 6-month stay aboard the International Space Station), with the L5 ACSA experiencing the greatest absolute decrease of all lumbar vertebral levels. 15 Thus, it appears that the LMF in the region of lumbar vertebral body L5 can be associated with low back pain and seems to respond to loading and unloading.
Methodological Considerations
The present study has significant limitations. First, the maturity offset values collected in the present study tend to be slightly outside the recommended range of -1 to +1 for female ski racers. Although the maturity offset around the growth spurt can be estimated with proven validity using the Mirwald formula, 23 the accuracy of estimation decreases with increasing deviation from zero (in both positive and negative directions). Second, the quality of the data collected with the OSTRC health questionnaire depends completely on the answers of the skiers. Therefore, to ensure sufficient data quality, skiers were assisted by their parents in answering the questionnaires and were interviewed by an experienced sports physician after the 12 months of surveillance. Third, the MRI- and US-based analyses used to examine LMF morphology were performed manually, meaning that they are rater dependent. However, a previous MRI study on the reliability of the measurement of LMF ACSA and the intrarater reliability of the US-based analysis in the present study suggest that both methods are reliable. 6 Fourth, it is important to emphasize that the observation of a significant difference in L5 ACSAavg between symptomatic and asymptomatic skiers does not allow conclusions to be drawn about cause and effect. To obtain an adequate prevalence representation of overuse-related back complaints, symptomatic and asymptomatic skiers were classified based on a prospective observation over a full year but before muscle imaging. Further controlled longitudinal studies starting with asymptomatic skiers would be needed to conclusively resolve the question of whether a lower L5 ACSAavg in symptomatic skiers is actually a cause, or an effect of overuse-related back complaints.
Conclusion
There are sex- and age-related differences in LMF morphology in youth competitive alpine skiers. For sports practical/clinical implementation, most importantly, the LMF ACSA at the level of the lumbar vertebral body L5 appears to undergo changes during biological maturation, shows an association with trunk stability, and differs between symptomatic and asymptomatic skiers with back complaints. These findings further highlight the important role of the LMF for training and injury prevention in youth competitive alpine skiers around the growth spurt.
Supplemental Material
sj-docx-1-sph-10.1177_19417381221136129 – Supplemental material for Lumbar Multifidus Morphology in Youth Competitive Alpine Skiers and Associated Sex, Age, Biological Maturation, Trunk Stability, and Back Complaints
Supplemental material, sj-docx-1-sph-10.1177_19417381221136129 for Lumbar Multifidus Morphology in Youth Competitive Alpine Skiers and Associated Sex, Age, Biological Maturation, Trunk Stability, and Back Complaints by Daniel P. Fitze, Martino V. Franchi, Lynn Ellenberger, Loris Peterhans, Stefan Fröhlich, Walter O. Frey and Jörg Spörri in Sports Health: A Multidisciplinary Approach
Footnotes
Acknowledgements
The authors thank all participants, parents, and coaches involved. Special thanks go to the Swiss Centre for Musculoskeletal Imaging (SCMI) where the study was conducted. They also thank Guiseppe Marcolin for his advice on statistical issues.
The authors report no potential conflicts of interest in the development and publication of this article.
This study was generously supported by the Balgrist Foundation, Swiss-Ski, the “Stiftung Passion Schneesport,” and the “Stiftung zur Förderung des alpinen Skisportes in der Schweiz.”
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.