
Abstract
Background:
Concern has been raised over the injury risk to school Rugby union (Rugby) players and the potential long-term health consequences. Despite the increase in studies for this cohort, the influence of playing position on injury incidence and presentation is unclear.
Purpose:
To describe the incidence, nature and severity of match injuries for school Rugby in Ireland overall, and as a function of playing position.
Study Design:
Prospective cohort study.
Methods:
Data were collected from 15 male (aged 16-19 years) school Senior Cup teams across 2 seasons. In total, 339 players participated in season 1, whereas 326 players participated in season 2. Injury data were recorded onto a bespoke online platform. Match exposure was also recorded.
Results:
The incidence rate of match injuries (24-hour time loss) was 53.6 per 1000 hours. Across both seasons, 6810 days were lost from play due to injury. Forwards (65.4 per 1000 hours) sustained significantly more (P < 0.05) injuries than backs (40.5 per 1000 hours). The head, shoulder, knee, and ankle were the most common injured body regions; however, forwards sustained significantly more (P < 0.05) head and shoulder injuries than backs. The tackle was responsible for the majority of injuries in both groups. The highest proportion of injuries occurred during the third quarter.
Conclusion:
Clear differences in injury presentation and incidence were evident when comparing forwards versus backs. The high rate of head and shoulder injuries in the forwards suggest the need for more targeted injury-prevention strategies and further research on education and laws around the tackle event. The spike of injuries in the third quarter suggests that fatigue or inadequate half-time warm-up may be a contributing factor warranting further exploration.
Clinical Relevance:
This study demonstrates clear differences in injury presentation according to playing position in school Rugby and highlights the need for a more tailored approach to the design and implementation of injury-prevention strategies.
Level of Evidence:
Level 3
Rugby union, hereafter “Rugby,” has become increasingly popular among children and adolescents in recent years with initiatives such as “Get Into Rugby”’ by World Rugby reaching a worldwide participation of over 2 million children in 2017. 49 Due to the increase in professional practices of school Rugby teams in particular, concern has been raised over the injury risk to these youth players and the potential long-term health consequences.30,34 The high incidence of injury in the professional game 47 may have contributed to these concerns; however, a lack of standardized surveillance methods and challenges associated with implementing injury epidemiology studies in a school setting has resulted in varying injury incidence rates (IRs) for school Rugby of 23.7 to 129.8 per 1000 player hours previously reported. 28 To effectively develop and implement optimal injury reduction protocols, the true incidence of injury must first be established as per the Translating Research Into Injury Prevention Practice (TRIPP) model. 16 In an attempt to address these discrepancies and improve the quality of injury surveillance research in rugby, World Rugby published standardized guidance on injury surveillance and reporting for researchers, including recommendations on the use of a 24-hour time-loss injury definition. 18 This led to the publication of high-quality school Rugby injury surveillance data in England 3 and Northern Ireland 1 with reported injury IRs ranging from 29.06 to 34.00 per 1000 hours for standard school Rugby competitions and 77 per 1000 hours for elite school Rugby teams in England. Although these studies have contributed to the research knowledge on injury trends for school rugby cohorts, the influence of playing position on injury incidence and injury trends is still unknown. Furthermore, in the Republic of Ireland, senior school Rugby (age 16-19 years) represents an elite level of competition, yet the incidence of injury has not been established.
In a game of Rugby, there are 15 players split into forwards (positions No. 1-8) and backs (positions No. 9-15). The primary function of forwards is to contest for and regain possession of the ball by participating in tackles, scrums, lineouts, rucks, and mauls. Backs gain possession of the ball from the forwards, accelerate from rucks, mauls, and scrums, evade opposing players, and carry the ball down the field to create scoring opportunities. 32 Forwards have a higher body mass, muscle mass and strength compared with backs, whereas backs have less body and muscle mass, possess higher levels of aerobic fitness and are faster than forwards.5,27,39 The distinct differences in positional demands and activity of forwards versus backs on the Rugby field suggest that variations in injury incidence and trends are likely. In Rugby league, variations in injury nature, site, and mechanism of injury were evident when analyzing injury data by playing position. 22 Although research into professional Rugby has identified positional differences in the injury incidence and trends,7,24,26,38 injury incidence as a function of playing position has yet to be reported or investigated in school Rugby. In professional Rugby, a significantly higher incidence of tackling shoulder injuries was reported in backs compared with forwards, while front-row forwards and midfield backs sustained markedly higher incidences of shoulder injuries, although differences were not significant. 24 Sankey et al 38 reported that second-row forwards were more likely to sustain ankle injuries than any other position, when analyzing professional Rugby players. In Rugby league, distinct differences in injury nature, site, and mechanism of injury were evident when analyzing injury data by playing position. 22 The reporting of overall injury incidence data for school Rugby teams may not accurately reflect the potential differences in injury rates between forwards and backs. Some rugby-playing countries have already implemented injury-prevention protocols and programmes for youth rugby, with encouraging results10,25; however, these have been team-targeted approaches. To effectively reduce injury incidence and severe injury rates, injury-prevention programs should perhaps be sensitive to positional influences on injury trends; however, it must first be established whether positional trends indeed exist in school Rugby. Therefore, the aim of this study was to describe the incidence, nature and severity of match injuries for schoolboy Rugby in Ireland overall, and as a function of playing position.
Methods
Study Design
This prospective cohort study was conducted over 2 seasons (2018-2020) as part of the wider Irish Rugby Injury Surveillance (IRIS) project. Participating teams were male Senior Cup teams (SCTs) registered with the Irish Rugby Football Union (IRFU) school SCT competitions across 2 provincial regions for the 2018/2019 and 2019/2020 seasons. In Ireland, the SCT division is the most elite rugby competition at school level for male players aged 16 to 19 years.
Recruitment
Before each season (September 2018 and September 2019), recruitment packs were sent out to schools participating in the provincial SCT competition. In total, 15 male teams were available for recruitment across the 2 provinces.
To be included in the analysis, match injury reports had to be completed for 100% of scheduled school matches; teams that did not meet these criteria were excluded. The principal researcher (T.L.) performed audits on the injury data each week to ensure accuracy, and injury recorders were contacted to clarify missing or incomplete data. Across both seasons, 473 individual Senior Cup players aged 16 to 19 years participated in the study. Before the commencement of the study, written informed consent was obtained from players and parents (where players were under 18 years). Ethical approval was granted by the University of Limerick’s research Ethics Committee 2016_06_19_EHS in agreement with the Declaration of Helsinki.
Injury Surveillance
This study adhered to the World Rugby injury surveillance consensus and the International Olympic Committee consensus statement on injury surveillance practices.2,18 All injury definitions were aligned with the 2007 Rugby consensus statement. 18 A 24-hour time-loss injury definition was used per the consensus statement, where an injury was defined as “Any physical complaint, which was caused by a transfer of energy that exceeded the body’s ability to maintain its structural and/or functional integrity that was sustained by a player during a Rugby match or Rugby training, irrespective of the need for medical attention or time-loss from Rugby activities” (p.193). For the purposes of this study, only match injuries and match exposure were recorded, as training injury data were dependent upon the availability of qualified personnel available at training sessions. Any injury that resulted in greater than 24-hour absence from match or training activities was classed as a time-loss injury, and categorized according to injury severity. Only time-loss injuries were included in injury IR calculations. Injuries that did not require time loss from Rugby activities were classified as medical attention injuries.
Per the consensus statement, a “recurrent injury” was defined as one of the same site and same type as the original injury that occurred within 2 months of the player returning to match play following the original injury. 18 Injury severity was calculated as the number of days elapsed since the date of injury to the date of the player’s return to full participation in training and availability for match selection. Injury severity was classified as minimal (1-3 days), mild (4-7 days), moderate (8-28 days), and severe (>28 days). Injury burden was calculated using the formula IR × severity, and expressed as days lost per 1000 hours. A dual injury was defined as one of multiple diagnoses resulting from 1 injury event. Dual injuries were analyzed as 1 injury event for the purposes of calculating overall incidence and injury severity. However, when analyzing injury location and nature, dual injuries were separated per international best practice. 2
A bespoke online injury surveillance platform 51 was modified to ensure it was suitable for use by nonmedical (teachers/coaches) injury recorders and appropriate for the school rugby setting in Ireland. 29 An injury recorder was nominated by each team who was subsequently trained on the use of the online platform, injury documenting practices, injury classification, and injury definitions by the primary researcher (T.L.). Injury recorders were primarily coaches (n = 13), physiotherapists (n = 6), or school nurses (n = 2). Injury recorders were instructed to document all Rugby match injuries on the online system classifying injury-specific data including location, nature, mechanism, occurrence, provisional diagnosis, confirmed diagnoses by the treating healthcare professional, and days absent from rugby activities.
Match schedules were also collected each month, so that match exposure could be calculated. SCT matches are 70 minutes in duration, with 15 players a side (per IRFU under-19 rules).
Data Analysis
The 2-season analysis consisted of 220 team matches for the school SCTs. The 220 matches consisted of 3861 player hours: 2059 hours for forward positions, and 1802 hours for back positions. Overall player hours were calculated as follows: 220 matches × 1.17 hours (duration of a SCT match) × 15 players.
IR of injury is reported per 1000 player hours of match exposure with 95% CIs, per the consensus statement 18 :
Player hours for forwards were calculated by: 220 matches × 1.17 hours × 8 players (number of forward positions), while player hours for backs were calculated by: 220 matches × 1.17 hours × 7 players (number of back positions). Injury IR for forward and back positions was calculated using the adjusted exposure for each positional group.
Poisson regression models were used to compare the injury IR between backs and forwards. Risk ratios were reported with associated 95% CIs. A chi-square test of independence was used to examine differences in the profile of mechanism of injury between backs and forwards.
Injury severity is reported as the mean days’ absence from play. Injury burden (days absent per 1000 hours) was calculated to present the overall burden of injuries in terms of days lost from play (mean severity × IR per 1000 hours). The level of significance was set at P < 0.05 for all analyses using SPSS Version 26.0 (IBM).
Results
Twelve teams (339 players) were recruited in season 1, whereas 11 of these teams (326 players) participated in season 2. One team from each season was excluded from analysis due to incomplete match injury reporting, resulting in a compliance rate greater than 90%.
Match Injury Results
Across the 2 seasons, 207 match injuries were recorded, totaling 6810 days absence from rugby activities. Each SCT competed in an average of 9 ± 2.3 matches in season 1 and an average of 13 ± 2.5 matches in season 2. The overall match injury IR requiring >24 hours’ absence across the 2 seasons was 53.6 per 1000 player hours (Table 1). Forwards sustained significantly more injuries (65%) than backs (35%), rate ratio = 1.61 (95% CI 1.21-2.14; P = 0.00). The forward lock positions (No. 4 and 5) sustained the most injuries (15%, IR 8.0 per 1000 hours) followed by the blindside flanker (No. 6) (13%, IR 6.7 per 1000 hours). Of all match injuries recorded, 26% of registered players sustained at least 1 match injury across the 2 seasons, whereas 7% of registered players sustained more than 2 match injuries across both seasons.
Match injury rates as a function of injury definition and player position
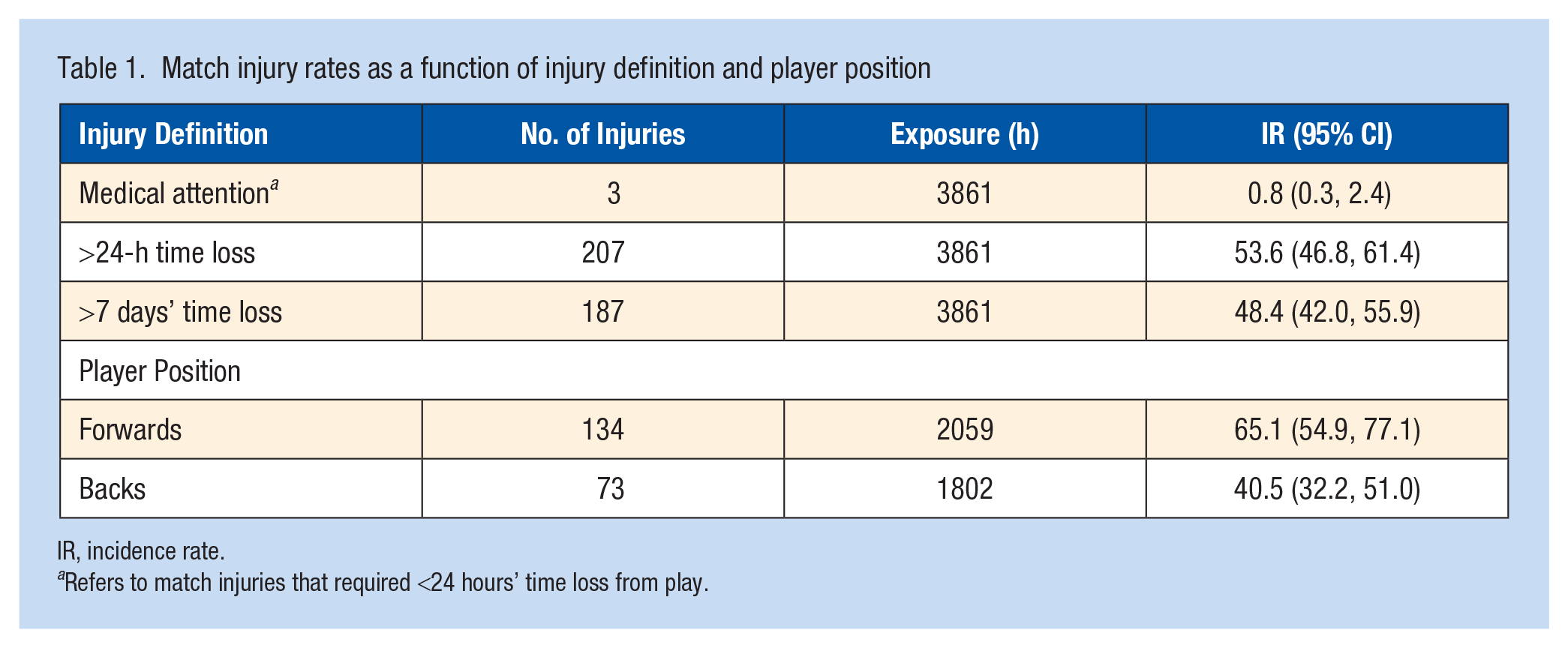
IR, incidence rate.
Refers to match injuries that required <24 hours’ time loss from play.
Location of Match Injuries
The shoulder, followed by the head and ankle, were the most injured body locations for all match injuries accounting for an IR of 12.2 per 1000 hours, 9.1 per 1000 hours, and 7.3 per 1000 hours, respectively. Overall, lower limb injuries were most common (41%) followed by upper limb (35%), head/neck (21%), and trunk (3%) injuries. In total, 50% of injuries sustained by the backs involved the lower limb, whereas lower limb injuries in forwards represented 35%. Forwards were significantly (P < 0.05) more likely to sustain shoulder and head injuries in comparison with backs (Table 2). Figures 1 and 2 illustrate the distribution of injury location by position.
Injury severity and burden for the top 3 most common body locations injured for forwards versus backs
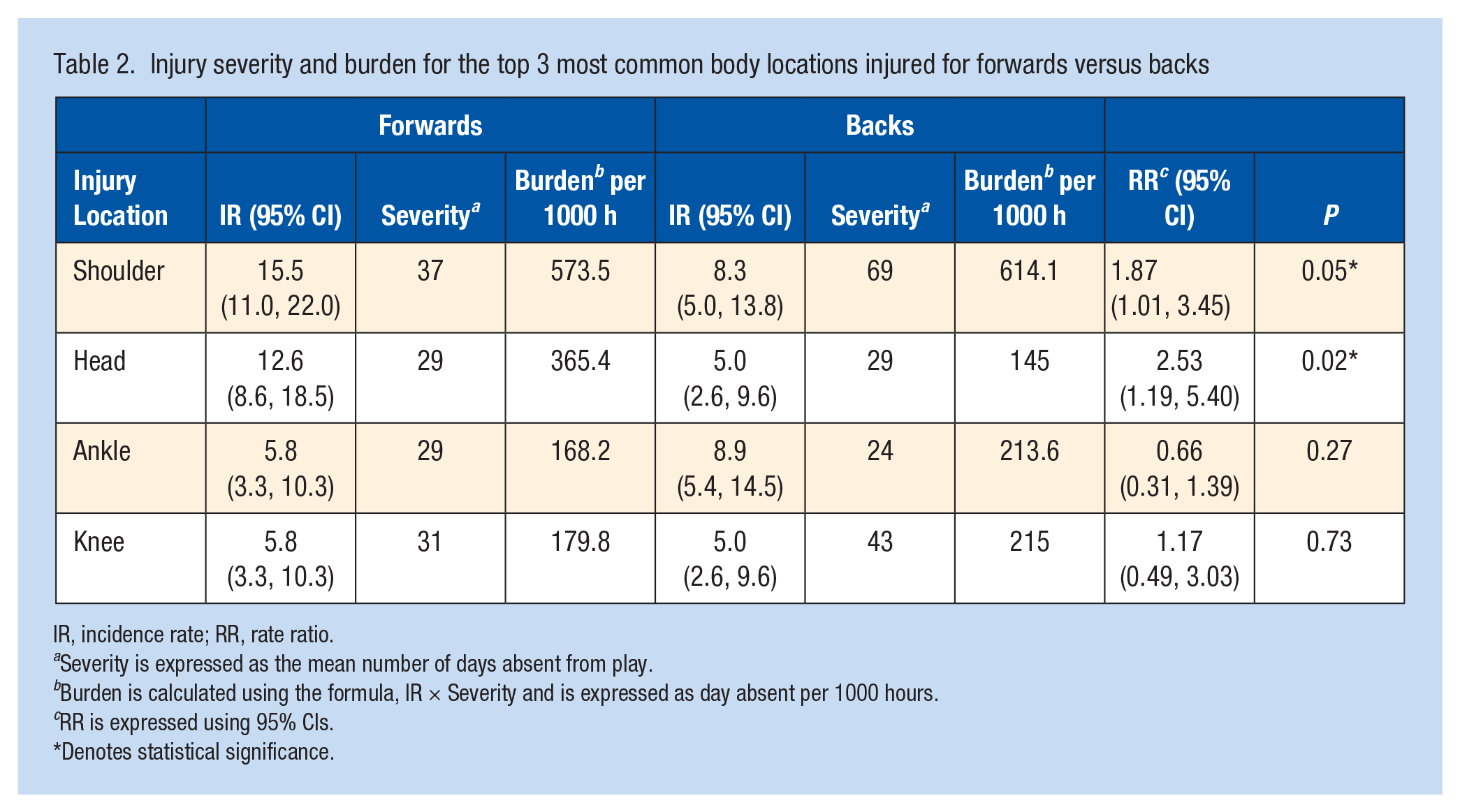
IR, incidence rate; RR, rate ratio.
Severity is expressed as the mean number of days absent from play.
Burden is calculated using the formula, IR × Severity and is expressed as day absent per 1000 hours.
RR is expressed using 95% CIs.
Denotes statistical significance.
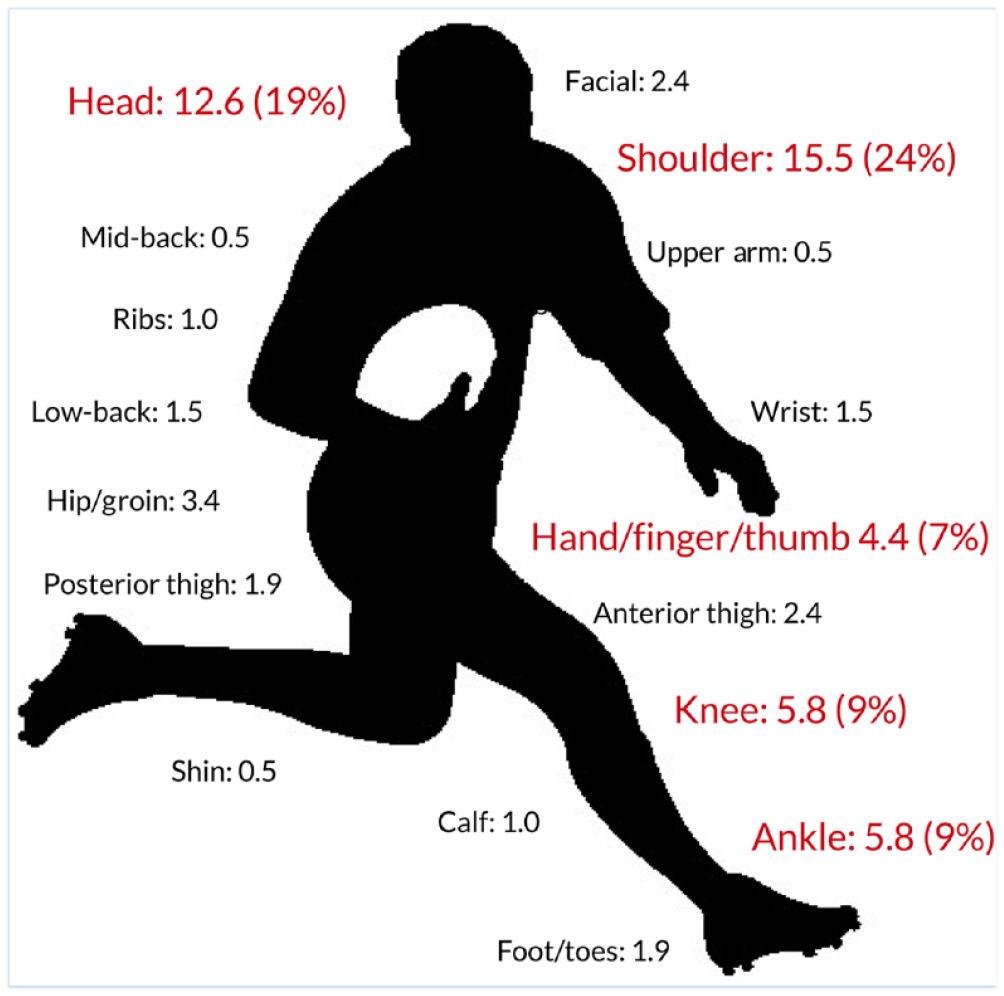
Location of match injuries for forwards IR (%).
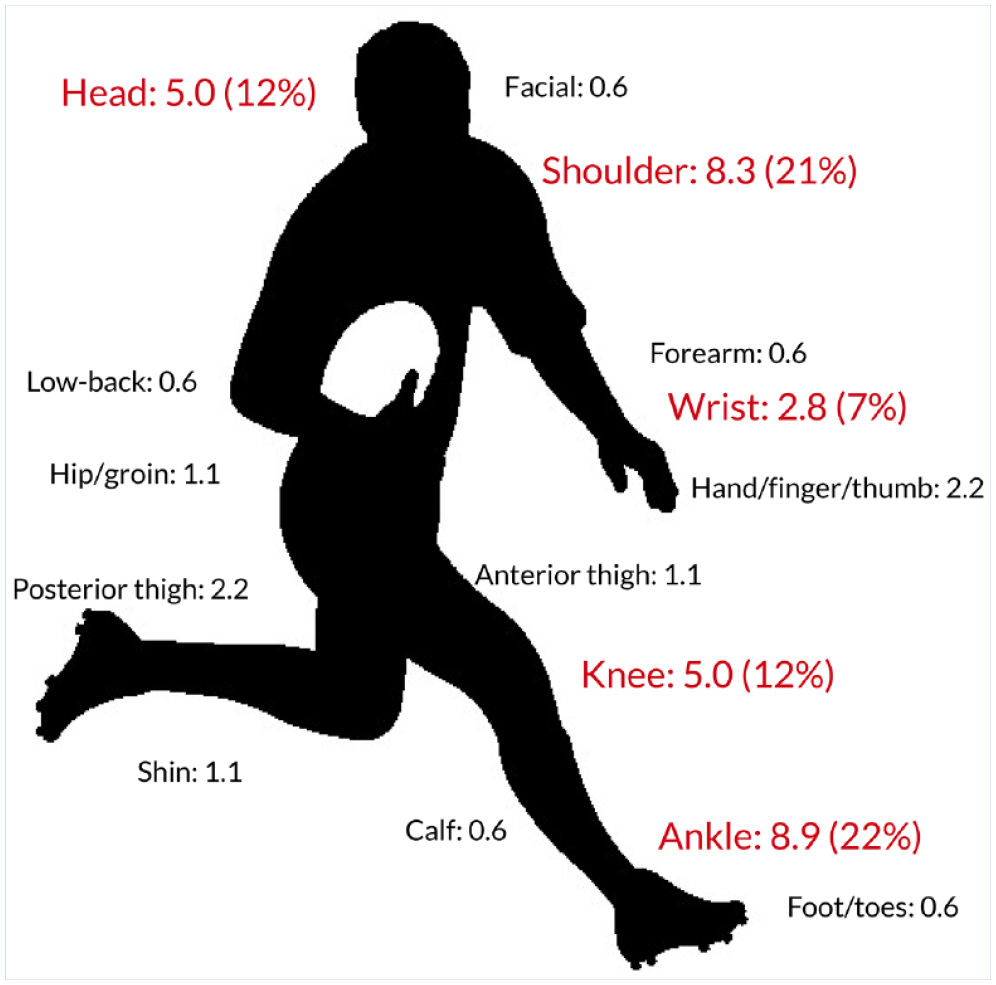
Location of match injuries for backs IR (%).
Nature of Match Injuries
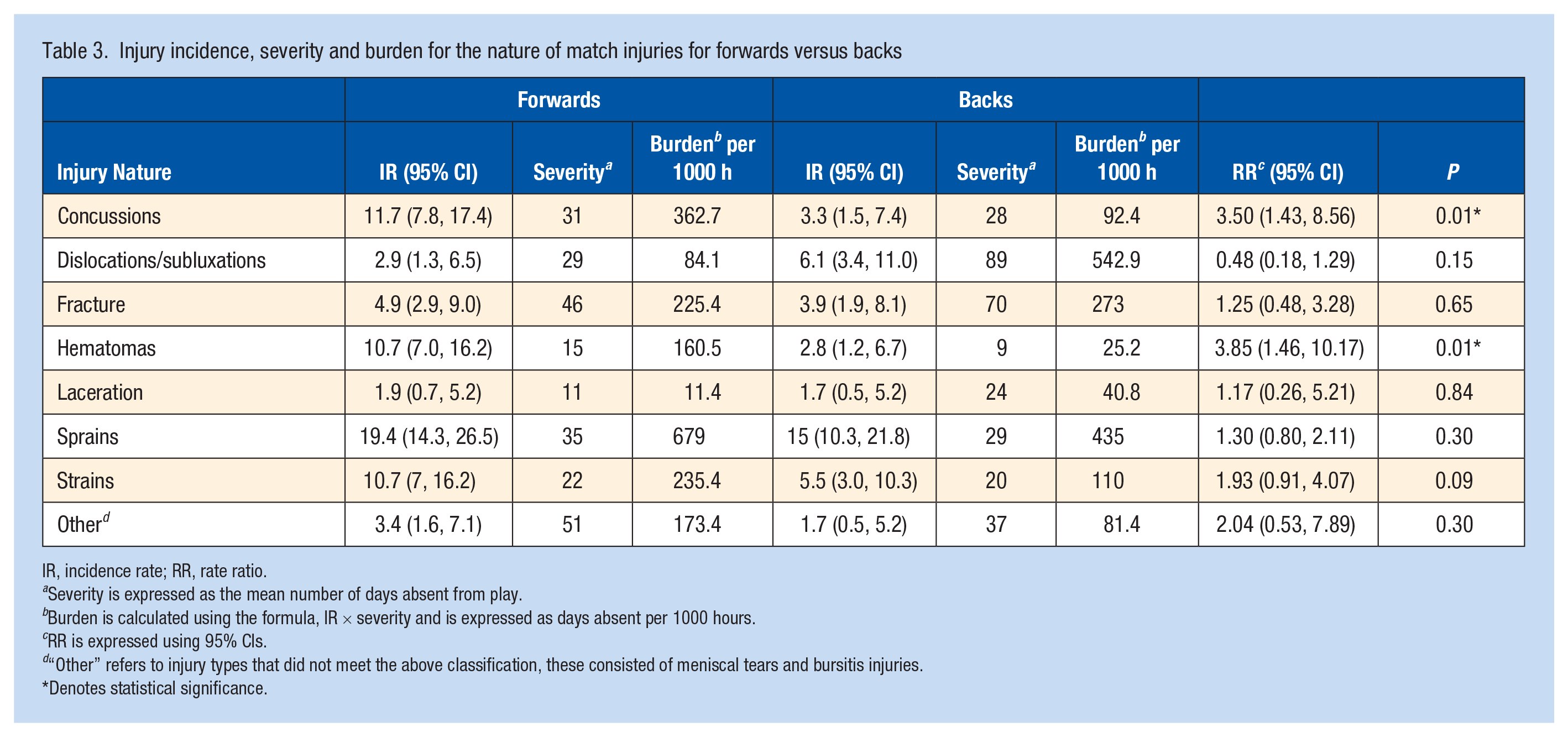
Sprains (33%) followed by strains (15%) were the most common injury type representing an overall match injury IR of 17.6 per 1000 hours and 8.3 per 1000 hours, respectively. When analyzing injury type by position, sprains remained the most common injury type for both backs and forwards; however, forwards were significantly (P < 0.05) more likely to sustain concussions and hematomas than the backs. Sprains represented the most burdensome injury for forwards, whereas dislocations/subluxations represented the most burdensome injury for backs in terms of days absent from play per 1000 hours. Table 3 illustrates incidence, severity and burden for the nature of match injuries for forwards versus backs.
Injury incidence, severity and burden for the nature of match injuries for forwards versus backs
IR, incidence rate; RR, rate ratio.
Severity is expressed as the mean number of days absent from play.
Burden is calculated using the formula, IR × severity and is expressed as days absent per 1000 hours.
RR is expressed using 95% CIs.
“Other” refers to injury types that did not meet the above classification, these consisted of meniscal tears and bursitis injuries.
Denotes statistical significance.
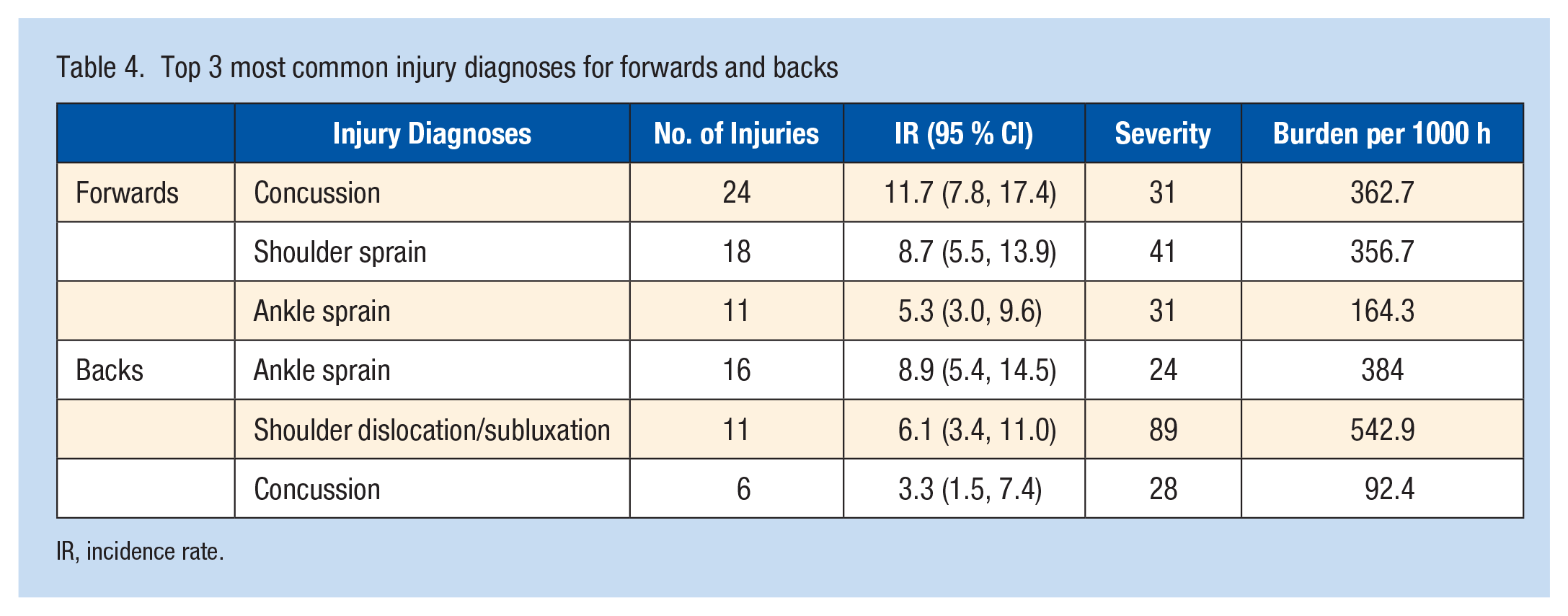
Match Injury Diagnoses
Table 4 illustrates match-injury diagnoses for 24-hour time-loss injuries for forwards versus backs for the top 3 diagnoses in each group. Concussions carried the highest injury burden for forwards (356.7 per 1000 hours), whereas shoulder dislocations/subluxations carried the highest injury burden for backs (542.9 per 1000 hours) in terms of days absent from play. The forward lock positions (No. 4 and 5) sustained the highest proportion of concussions (27%), the wing positions (No. 11 and 14) sustained the highest proportion of shoulder dislocations/subluxations (33%), the inside center sustained the most ankle sprains (26%), whereas shoulder sprains were more evenly distributed among the lock (20%), loose-head prop (20%), and blindside flanker (20%) positions.
Top 3 most common injury diagnoses for forwards and backs
IR, incidence rate.
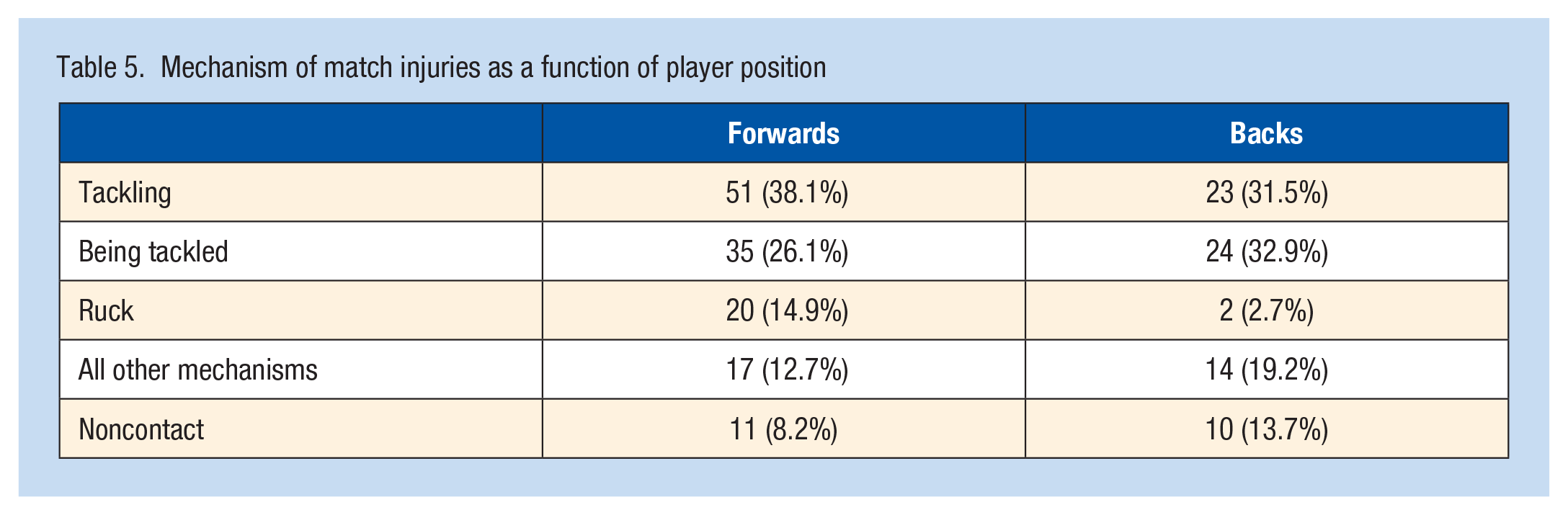
Mechanism
The majority of match-related injuries occurred during the tackle (64%). In the analysis, chi-square X2 (4, N = 207) = 10.66; P = 0.03 suggests that the mechanism of injury differs between backs and forwards, with 79.1% of injuries in forwards involving a tackle or ruck. Table 5 illustrates the mechanisms of match injuries as a function of player position.
Mechanism of match injuries as a function of player position
Timing of Injury
The majority of match injuries (40%) occurred during the third quarter. A significant relationship was not found between player position and time of injury. The highest proportion of tackle injuries occurred during the third quarter for both the forwards (43%) and the backs (37%). Figure 3 illustrates the occurrence of match injuries as a function of position.
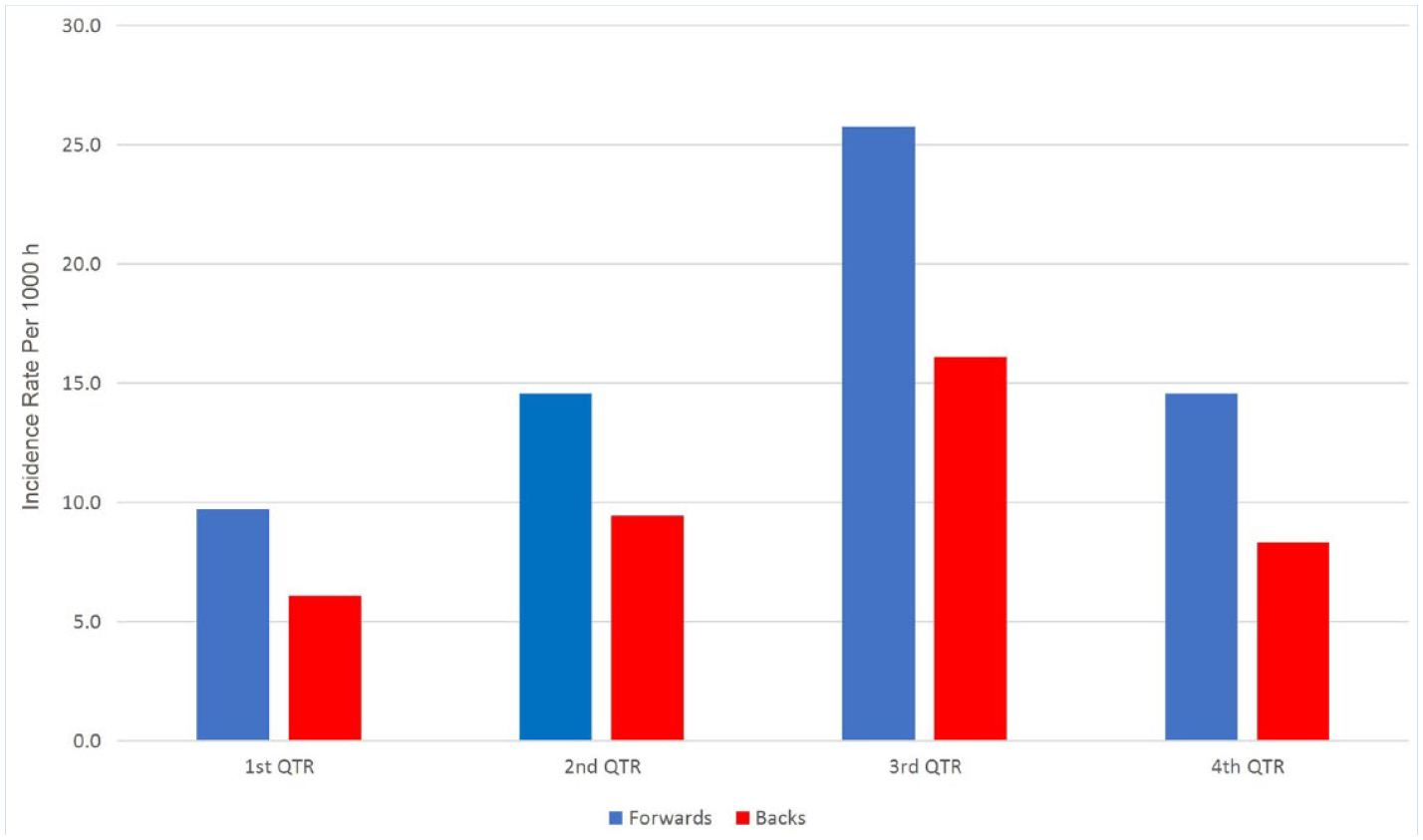
Match injuries as a function of playing position.
Discussion
Summary of Main Findings
This study has established that significant differences in injury incidence and presentation exist between forwards and backs in senior schoolboy Rugby. Forwards sustain more injuries than backs and are at a significantly higher risk of sustaining concussions. Injury presentation differed across both positional groups; ankle sprains were the most common diagnoses for backs, whereas concussions were the most common diagnoses for forwards. Injury severity data suggested that on average, a senior school Rugby team can expect to lose 324 days from play due to injury each season.
Comparison With Existing Literature
The IR of match injuries reported in this study is lower than previously reported for elite schoolboy Rugby in England (77 per 1000 hours), 3 although it is higher than IRs reported by other studies of schoolboy Rugby (28.3-35.0 per 1000 hours) 28 for a 24-hour time-loss definition. The overall match injury IR in this study (53.6 per 1000 hours) is more comparable with the IR of injury in professional under-20 international competitions (57.2 per 1000 hours), 19 and the academy teams of professional Rugby clubs in England (47 per 1000 hours). 33 SCT Rugby is representative of the most elite level of school Rugby in Ireland; therefore, injury risk appears higher than in lower levels of play for similar age cohorts.3,28,33
Forwards were significantly more likely to sustain injuries compared with backs (P = 0.00). Although positional injury data in comparable school cohorts are lacking, the IR of injuries to the forwards (65.1 per 1000 hours) is more than double the IR reported (30.6 per 1000 hours) by the Youth Rugby Injury Surveillance Project (YRISP) 23 for a cumulative group of under-13, under-15 and under-18 school Rugby teams. However, IR was calculated based on overall team exposure, and statistical difference between forwards and backs was not reported. Data from the male adult game for positional differences in injury profiles are conflicting. In English community Rugby (mid-lower levels), a significant interaction (P = 0.01) demonstrated higher IR for forwards compared with backs 37 ; however, a longitudinal analysis carried out over 16 seasons in the professional game found no statistical difference in the IR of injury between forwards and backs. 44 Although a clear statistical difference in IR and injury presentation was observed between forwards and backs in the current study, it is not clear if this is true for school Rugby worldwide. It is vital that future research further evaluates the relationship between playing position and injury risk across youth Rugby. This has important implications for Rugby governing bodies and has the potential to inform future law changes and injury-prevention policies.
Injury Location and Diagnoses
Shoulder, head, knee, and ankle injuries were the most prevalent, which is consistent with injury profiles in the elite,20,47 amateur,37,52 and school game.1,3,28 Although some data exist for positional trends in match-injury occurrence in the professional game,9,45 comparable data are lacking in youth Rugby. Forwards by their nature are generally bigger and stronger than backs, as their primary function is to compete for the ball in scrums and lineouts, whereas backs are usually lighter and faster than forwards, as they require skill for kicking, passing, and reading the game.9,35 The data from the current study clearly demonstrate differences in injury risk and presentation between both positional groups, which has important implications for targeted injury-reduction strategies.
Forwards were significantly more likely to sustain shoulder and head injuries compared with backs, with the majority of these occurring when tackling the ball carrier. The high incidence and burden of shoulder injuries in this cohort is concerning, given the associated high risk of recurrence and the inherent instability of the shoulder joint itself. 21 This, coupled with the skeletal immaturity of the shoulder joint in school-age players, may predispose this group to a higher shoulder-injury risk compared with their adult counterparts.31,43 The increased exposure to tackles for the forwards may lead to accumulative microtrauma to the shoulder joint, which may negatively affect rotator-cuff strength and proprioception, potentially resulting in an increased injury risk for this group. 31 Although efforts have begun to reduce the risk of lower limb injuries in this cohort, research has yet to fully investigate injury-prevention and educational tools to address the high IR and substantial time loss due to shoulder injuries in youth Rugby. 40 In researching injury-prevention strategies, the role of an upper limb–strengthening programme with an emphasis on the practicality of the forwards’ role should be investigated. When forwards are contesting for the ball, the arm is often in a vulnerable position of abduction and external rotation, which appears to result in a greater incidence of injury for school-age Rugby players compared with in the professional game. 24 It is important to evaluate whether the introduction of an upper limb exercise programme would influence injury risk in this group, or whether a review of the policies around the laws of the tackle for this age cohort are required to reduce the risk of shoulder injury.
Concussions in this study, and indeed the wider literature, are reported predominantly due to the tackle event.1,3 Forwards in the current study sustained greater than 3 times the IR of concussions compared with backs, which can be assumed to be influenced by their increased involvement in the tackle. A study of head-injury events in professional Rugby reported that “tacklers” were 2.6 times more likely to be injured compared with the ball carrier. 42 Poor tackle technique has been associated with increased injury risk, and efforts have been made to educate young players on using their shoulder/arm as the first point of contact instead of their head/neck, to reduce the risk of concussion and cervical spinal cord injury.12,48 Previously, in youth Rugby, concussion incidence has been reported as an overall figure without accounting for positional influence. The IR of concussion in backs is noticeably lower than overall concussion incidence previously reported for similar-age cohorts.1,3,17,23 The significant increase in concussion incidence noted for forwards in this study suggests that a more positional-targeted approach may be appropriate for concussion prevention strategies. The success of recent law changes by World Rugby on reduced incidence of severe head injury has been welcomed and perhaps strengthens the argument for future investigation into further law changes in youth Rugby to reduce the disproportionate risk of head injury sustained by forwards. 36 It is also reasonable to consider the potential influence of overreporting of concussions in this cohort due to the “Recognize and Remove” protocol which requires all suspected concussions to be removed from the field of play and diverted into the Graduated Return to Play pathway. The success of movement control exercise programmes 25 and educational programmes for coaches and referees 10 may also be further enhanced by further investigation into the positional influence on head-injury risk in these cohorts.
While lower limb injuries in this study represented the majority of injuries (41%), various injury presentations have been reported across school Rugby research. Although, accumulatively, lower limb injuries were more frequent in this cohort, only ankle sprains featured in the top 3 injury diagnoses for both positional groups. The IR of ankle injuries in this study (7.2 per 1000 hours) is slightly higher than previously reported in the amateur game in Ireland (6.0 per 1000 hours), 52 but lower than IRs reported for the professional game (10 per 1000 hours). 38 Ankle sprains have been commonly reported in the top 3 injury locations across amateur Rugby research1,3,52; however, studies investigating positional ankle injury trends are scarce. In the current study, ankle sprains were the most common injury diagnoses for the backs. Backs have been shown to cover greater distances and speeds than forwards 14 and are generally involved in fewer tackles, 27 which may explain why the majority of ankle injuries in this group were the result of noncontact injuries. However, ankle injuries also featured in the top 3 injury locations for forwards, although superseded by shoulder and head injuries, of which the latter could be attributed to the increased exposure to tackles. This may suggest that injury-reduction strategies for lower limb injuries for the backs should be focused on noncontact injury mechanisms. For the forwards, the knee (5.8 per 1000 hours) also shared the place with the ankle (5.8 per 1000 hours) for the top 3 most common locations of injury; however, injury burden was relatively low, and severe injury to the knee was uncommon. A recent study of male and female community rugby in Ireland attributed the highest overall injury burden to anterior cruciate ligament (ACL) injuries for both groups. Although knee injuries represented 9% and 12% of injuries to the forwards and backs, respectively, interestingly, no ACL injuries were reported across the 2 seasons, which is consistent with other youth Rugby studies, where reported IRs range from 0.049 to 1.260 per 1000 hours.6,41 The stark differences in injury risk to the shoulder and head between forwards and backs was not echoed by the lower limb data, although noncontact mechanisms were more apparent in the backs. This has important implications for targeted injury-prevention programmes specifically for the lower limb, which has shown dramatic reductions of injury in noncontact sports such as soccer. 4 Such programmes may be more successful in Rugby if targeted more to the backs, while injury reduction strategies in the forwards could be more focused on reducing contact injuries such as education/training around tackle technique, and further scrutiny of the laws around the tackle event in youth Rugby.
Timing of Injury
While most injuries to the forwards and backs occurred during the third quarter, no significant relationship between timing of injury and playing position was found. In the wider literature, most injuries have also been reported occurring during the third quarter across the amateur 50 and professional game, 47 although timing-of-injury data are lacking in school Rugby research.1,3,28 In the current study, it was evident for both positional groups that the majority of tackle-related injuries occurred during the third quarter. A South African study of tackle-related injuries in a youth Rugby tournament reported a significant increase in the frequency of tackle-related injuries as the timing of play progressed. 12 It is hypothesized that physical fatigue has the potential to negatively impact a player’s tackle technique.8,11,13 However, an apparent drop of injury incidence is evident in the fourth quarter, which does not fully support this theory, although this fourth-quarter drop may also be influenced by substitutions. The spike of injuries in the third quarter could also be attributed to a lack of warm-up at half time. Data from soccer have indicated that inadequate half-time warm-ups result in reductions in work rate and performance in the second half.15,46 Further research is required to investigate the effect of half-time warm-ups on and the potential influence (if any) on work rate, performance, fatigue, and injury incidence in the second half of games. These data are valuable to help inform governing bodies on the structuring of match schedules and tournaments, and further enhance the development of injury-reduction programmes.
Strengths and Limitations
This study comprised a large cohort in an amateur setting, a low level of attrition, along with high data fidelity, and external validity. Injury data were collected prospectively to allow for the accurate recording of real-time injuries. Methods were standardized per best practice, 18 to allow for accurate comparison across the literature. Investigating injury trends in a school Rugby setting presents itself with many challenges and resulted in some limitations to this study. Injury recording by medical personnel was not always possible, as injury recorders varied from school physiotherapists/nurses to teachers and coaches. Nevertheless, the IRIS Web system was developed for the amateur cohort 51 and modified specifically for the school Rugby setting. Full training was provided to injury recorders, and injuries were recorded on their location and nature, rather than diagnoses, with final diagnoses and verification by the treating physician/physiotherapist/nurse only recorded at return to play to facilitate accuracy. In addition, it was not feasible to collect training exposure data to allow for the calculation of training injury incidence. To accurately record training exposure data in addition to match schedules, is often not sustainable by schools and researchers in a school setting.
Conclusion
The incidence of injury for schoolboy Rugby in Ireland is lower than previously reported for elite schoolboy rugby in England, although slightly higher than previously reported for standard schoolboy Rugby in England and Northern Ireland. The shoulder, head, knee, and ankle were most commonly injured, although clear differences in injury presentation and incidence were evident when comparing forwards versus backs. The high rate of head and shoulder injuries in the forwards suggests the need for more targeted injury-prevention strategies and further research on education and laws around tackle technique. The higher rate of ankle injuries in the backs were more commonly associated with noncontact activities, suggesting a role for a more individualized noncontact approach to injury-prevention strategies for the backs. The spike of injuries in the third quarter suggests that fatigue or inadequate half-time warm-up may be a contributing factor that warrants further exploration. This study demonstrates clear differences in injury presentation according to playing position in school Rugby and highlights the need for a more tailored approach to the design and implementation of injury-prevention strategies for schoolboy Rugby.
Footnotes
The following authors declared potential conflicts of interest: T.M.L. has received grant and support for travel fees to meetings from the Irish Rugby Football Union; I.C.K. has received grant and support for conference attendance from the Irish Rugby Football Union, M.J.C. has received grant and support for conference attendance from the Irish Rugby Football Union; G.D.W. has received grant and support for conference attendance from the Irish Rugby Football Union; R.C. has received grant and support for conference attendance from the Irish Rugby Football Union; A.J.H. has received grant and support for conference attendance from the Irish Rugby Football Union; M.L. has received grant and support for conference attendance from the Irish Rugby Football Union; L.G.G. has received grant and support for conference attendance from the Irish Rugby Football Union; K.O.S. has received grant and support for conference attendance from the Irish Rugby Football Union; T.M.C. has received grant and support for conference attendance from the Irish Rugby Football Union.