
Abstract
Background:
Promoted as a safer alternative to tackle football, there has been an increase in flag football participation in recent years. However, examinations of head impact exposure in flag football as compared with tackle football are currently limited.
Hypothesis:
Tackle football athletes will have a greater number and magnitude of head impacts compared with flag football athletes.
Study Design:
Cohort study.
Level of Evidence:
Level 4.
Methods:
Using mouthguard sensors, this observational, prospective cohort study captured data on the number and magnitude of head impacts among 524 male tackle and flag football athletes (6-14 years old) over the course of a single football season. Estimates of interest based on regression models used Bayesian methods to estimate differences between tackle and flag athletes.
Results:
There were 186,239 head impacts recorded during the study. Tackle football athletes sustained 14.67 (95% CI 9.75-21.95) times more head impacts during an athletic exposure (game or practice) compared with flag football athletes. Magnitude of impact for the 50th and 95th percentile was 18.15g (17.95-18.34) and 52.55g (51.06-54.09) for a tackle football athlete and 16.84g (15.57-18.21) and 33.51g (28.23-39.08) for a flag football athlete, respectively. A tackle football athlete sustained 23.00 (13.59-39.55) times more high-magnitude impacts (≥40g) per athletic exposure compared with a flag football athlete.
Conclusion:
This study demonstrates that youth athletes who play tackle football are more likely to experience a greater number of head impacts and are at a markedly increased risk for high-magnitude impacts compared with flag football athletes.
Clinical Relevance:
These results suggest that flag football has fewer head impact exposures, which potentially minimizes concussion risk, making it a safer alternative for 6- to 14-year-old youth football athletes.
From 2010 to 2019, there has been a dramatic growth in public awareness and research on concussion and the risk for short- and long-term sequelae among athletes. More recently, researchers have increased their focus on examining head impact exposure and the potential risks of repeat or subconcussive head impacts among this population.9,15,17,18 Athletes who participate in contact or collision sports, such as American football, ice hockey, lacrosse, and soccer, are at increased risk for head impacts and are the focus of most investigations of head impact exposures.13,35,37,45 Examining head impacts among athletes is critical to evaluating strategies to minimize head injuries.
Data on head impact exposure are generally obtained through sensor technologies (such as those placed on helmets or in mouthguards and skin patches) that have been validated for this purpose.11,43 While sensor technologies vary, most are designed to collect number, magnitude, and location of impacts. Using helmet sensors, data from past studies demonstrate that as youth athletes increase in age, the number of impacts and magnitude of linear acceleration per athlete also increases (Table 1).8,9,15,17,18,41,52,54
Head impacts metrics from past tackle football studies, a United States
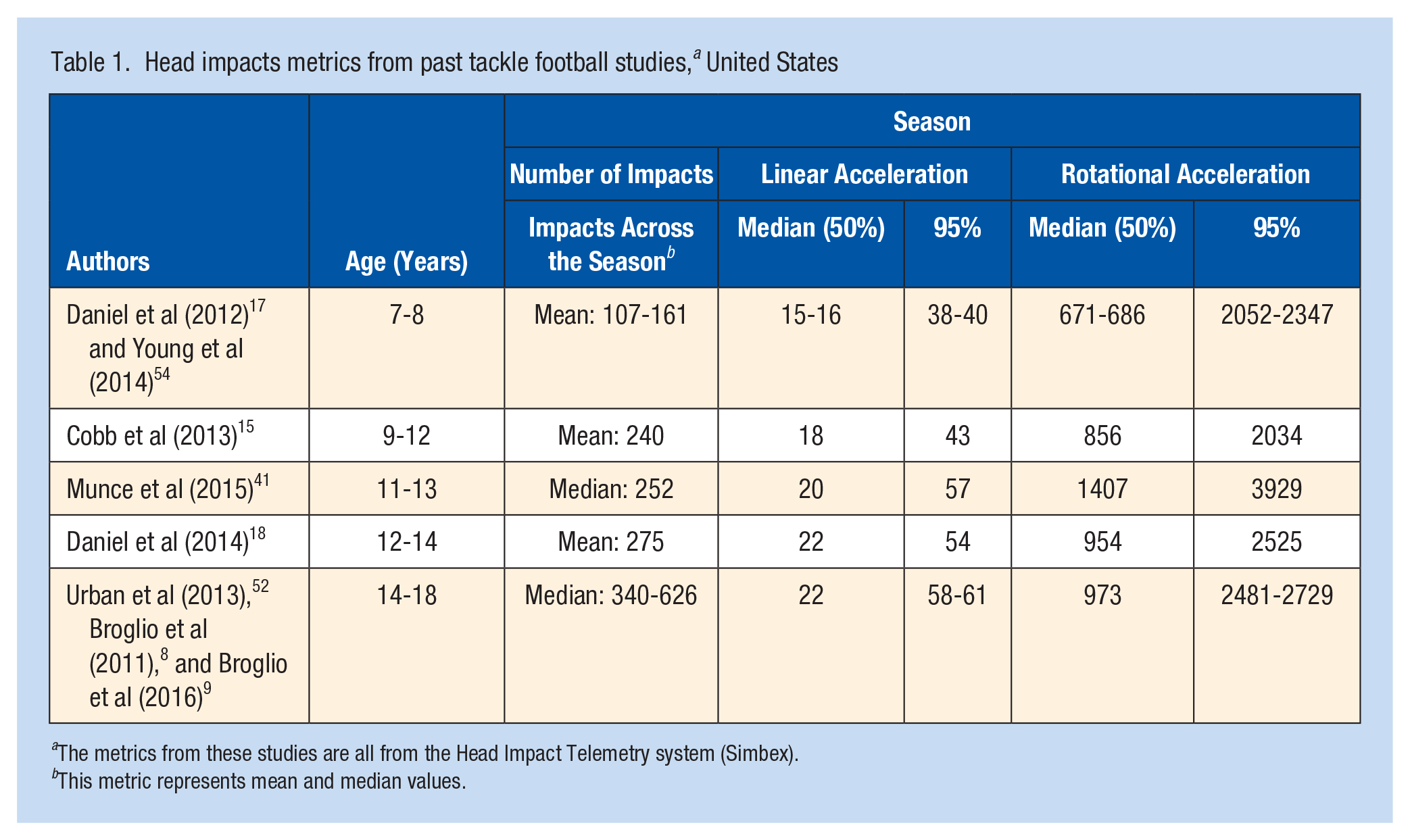
The metrics from these studies are all from the Head Impact Telemetry system (Simbex).
This metric represents mean and median values.
While head impacts may or may not result in clinical signs and symptoms, previous studies examining youth, high school, and college athletes explored the association between head impact exposure and the risk for physiological, cognitive, and behavioral sequelae. Studies using neuroimaging, such as functional magnetic resonance imaging and diffusion tensor imaging, observed potential changes among high school football players over the course of a single football season. They recorded increased cognitive deficits, changes in white matter diffusivity measures, and neurological injury as compared with a preseason baseline.2,34,50 These changes occurred in the absence of identified concussions. However, 2 studies that used tests to assess balance, oculomotor performance, reaction time, and self-reported concussion symptoms to evaluate for changes in performance immediately after the football season did not demonstrate changes from baseline measures.38,41 If sustained repeatedly, head impacts may lead to pathological changes over time that are linked to cognitive and behavioral sequelae.3,30,40,45 Still, why some athletes experience health effects after long-term exposure to repeat or subconcussive head impacts and others do not is currently unclear. Duration of exposure of repeated head impacts is one area of study. Montenigro et al 39 found that the more an athlete was athletes were exposed to repeat head impacts (that resulted in concussive and nonconcussive events) during their athlete career, the greater their risk for cognitive impairment, self-reported executive dysfunction, depression, apathy, and behavioral dysregulation later in life. Moreover, Alosco et al 1 found that professional football players who started playing the sport prior to age 12 years had an increased risk for cognitive impairments (specifically neuropsychiatric and problems of executive function) as adults, suggesting that negative outcomes may not manifest until later in life. Conversely, a study by Brett et al 6 found no associations between playing football before age 12 years and clinical outcomes. Researchers also posit that biological, environmental, or lifestyle factors may increase an athlete’s risk for adverse health outcomes, such as chronic traumatic encephalopathy, later in life.22,23 However, more research is needed to better understand the role of these risk factors on health outcomes after long-term exposure to head impacts while playing football and other sports.
Each year, approximately 1 million high school students 42 and 1.8 million children aged 6 to 12 years play American football, 51 making it one of the most popular sports played by children and adolescents in the United States. To minimize the incidence of concussion, as well as other head and brain injuries, some football programs have implemented interventions aimed at reducing an athlete’s exposure to head impacts. These interventions focus primarily on tackling—the activity associated with the highest risk for concussion. 33 Examples of interventions include contact restrictions that limit the amount of tackling during practices and modified tackling techniques (such as shoulder-style tackling). 16 In its statement on Tackling in Youth Football in 2015, the American Academy of Pediatrics recommended noncontact or flag football programs for young athletes who want to play football but are concerned about the potential risks for injury. 16
Often promoted as a safer alternative to tackle football, there has been an increase in flag football participation in recent years. 51 However, examinations of head impact exposures and injury risk in flag football programs are currently limited. To assess injury rates between youth flag and tackle athletes, Peterson et al 44 examined injury data from athletes in 1 flag and 2 tackle football leagues; the overall injury rate for flag football leagues exceeded that of tackle leagues, but no differences were found for rates of concussion. The only study to examine head impact exposure in tackle and flag football compared head impact exposure between 25 tackle and 25 flag youth football athletes over the course of the season. 32 They found that tackle football athletes experienced more than 4 times the number of head impacts (>14g) per athletic exposure (AE; ie, game or practice) compared with flag athletes, and flag athletes had reduced odds of experiencing an impact greater than 20g. 32
Previous studies examining head impact exposure among tackle and/or flag football athletes have had small sample sizes and generally were confined to a narrow, typically older, age range. Improved understanding of the head impact burden among both youth tackle and flag football athletes may inform interventions being used by football programs and to further promote athlete safety. Our current study seeks to expand on existing knowledge by examining head impact exposure among a large sample of children aged 6 to 14 years who participated in a flag or tackle football league.
Methods
Participants
Institutional review board approval was obtained from the New England Independent Review Board. Head impact data were collected from 524 male tackle and flag youth football athletes (477 tackle and 47 flag athletes) from 36 youth tackle football and 6 youth flag football teams in New York (Table 2). Data were collected over the course of the tackle (fall 2017) and flag (spring 2018) football seasons. Youth tackle football athletes were aged 6 to 14 years and flag football athletes were aged 7 to 14 years. Both football leagues had 4 age-based divisions. For tackle football athletes, there were 8 games and an estimated average of 19 practices during the regular season (since no attendance data were collected for these athletes and there was no information on when practices occurred, this number was estimated based on the impact data). For flag football athletes, there were 7 games and an average of 6 practices during the regular season. A randomized controlled trial was implemented for the tackle football teams, examining differences between 2 tackling techniques and the use of robotic dummies. However, there were no differences in the number of head impacts (median [interquartile range (IQR)]control = 374.50 [111.75-609.25]; median [IQR]treatment = 385.00 [154.00-567.00]) or median linear acceleration (median [IQR]control = 18.08g [14.32g-26.20g]; median [IQR]treatment = 18.53 [14.51-27.28]) between the conditions, and so data were combined. Teams that agreed to participate in the study worked with the study team to obtain informed consent from the athletes’ parents and assent from the athletes.
Demographics and concussions of tackle and flag athletes, ages 6 to 14 years, New York, United States, 2017 and 2018
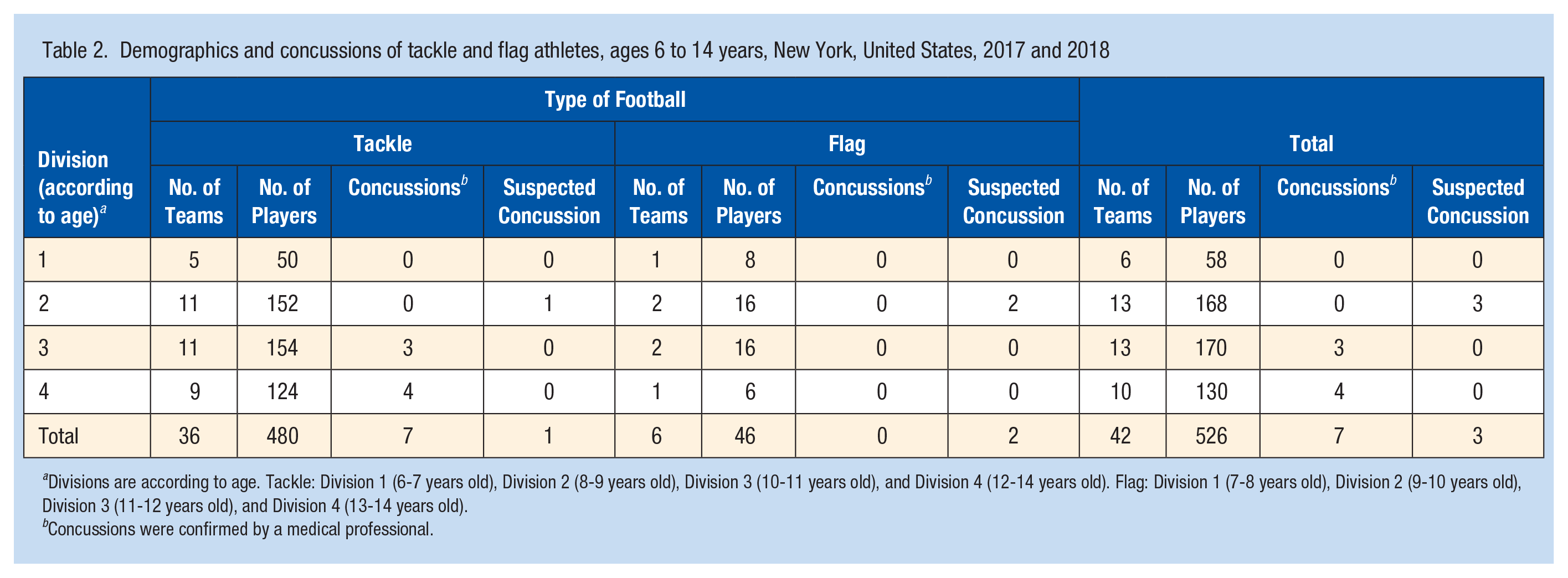
Divisions are according to age. Tackle: Division 1 (6-7 years old), Division 2 (8-9 years old), Division 3 (10-11 years old), and Division 4 (12-14 years old). Flag: Division 1 (7-8 years old), Division 2 (9-10 years old), Division 3 (11-12 years old), and Division 4 (13-14 years old).
Concussions were confirmed by a medical professional.
Mouthguards
Youth football athletes were equipped with the Vector MouthGuard (manufactured by Athlete Intelligence). The mouthguard measured magnitude of head acceleration and was optimized for impacts between 10g and 200g. As flag football athletes in this study did not wear helmets, mouthguards allowed for the assessment of head impacts using a consistent method. The mouthguard was fitted for each athlete’s bite through a standard boil-and-bite process for a secure custom fit. The mouthguard used a triaxial accelerometer to measure peak linear acceleration and a triaxial angular rate gyroscope to measure peak rotational kinematics. 11 Data acquisition was triggered when the sensor measured 3 consecutive samples greater than 10g in any axis. When triggered, the instrumentation stored 16 ms of pretrigger and 80 ms of posttrigger data on the mouthguard’s memory chip. Coaches or their designee uploaded the data using Athlete Intelligence’s sideline receiver and base station (product #350-00003). To determine impact (total = 186,239) versus nonimpact (total = 1,405,808) events, events were classified 2 ways. First, to reduce the likelihood of false-positive impacts, a capacitive in-mouth sensor determined when the mouthguard was present in the mouth. Thus, impacts that occurred outside an athlete’s mouth were removed. Second, a support vector machine classifier was used to reject nonimpact events, such as chewing, clenching, and drinking. From previous studies, the sensor has been shown to have high validity compared with an anthropomorphic test device and is consistent with what is seen in another mouthguard sensor and helmet sensors.4,11,21,25,46 For example, peak linear acceleration measurements across all 128 impact sites were highly correlated between the mouthguard sensor and an anthropomorphic test device (r2 = 0.96) and demonstrated a 9.9% ± 4.4% average normalized root mean square error (±SD) for impact time traces for linear acceleration. For more in-depth information about the sensor and sensor validation, refer to Camarillo et al 11 and Snyder and Haensly. 49 Impacts were not verified using video.
Data Analysis
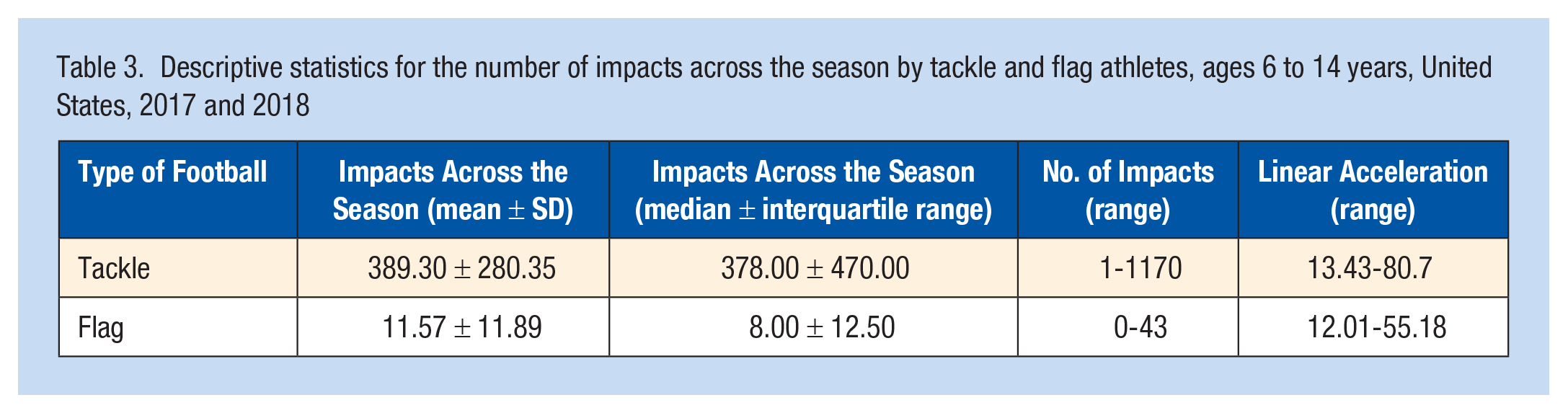
The analysis solely included head impacts collected during the regular football season because of differences in pre- and postseason activities between flag and tackle football programs. The analysis excluded data from impacts (n = 3,857, accounting for 2% of the data) with an inconsistent time stamp (eg, a head impact occurred prior to or after a practice or game) due to sensor error. The statistical packages OpenBugs Version 3.2.3 and SAS Version 9.4 were used for analyses. Descriptive measures of frequency and central tendency (median ± IQR) were calculated for head impact metrics (Table 3). Head impact exposure was quantified in terms of number of head impacts (≥10g) and high-magnitude impacts (≥40g). While there are no definitive threshold parameters for concussive events, 20 these thresholds were chosen as they are consistent with current literature.12,17,18,52 In addition, the linear acceleration 50th and 95th percentile impacts for each athlete were calculated and then averaged across athletes. For head impact exposure, estimates of interest based on regression models developed using Bayesian methods with 95% credible intervals (ie, 95% probability that the effect falls within that range) were run to estimate differences between tackle and flag athletes. A Poisson distribution was used to estimate number of impacts for tackle and flag effects and adjusted for player-level random effects. For 50% and 95% linear acceleration, the model assumed a Student t distribution to address overdispersion. A zero inflated Poisson distribution was used to estimate high-magnitude impacts. We examined a variety of models for each outcome including the effect of athlete age and team-level effects. In all cases, inclusion of these terms did not substantially change the estimates of interest. Thus, the more parsimonious model was selected. Additional details on the underlying assumptions, handling of missing values, identification of outliers, fitting approaches, and goodness-of-fit evaluations used in the modeling process are provided in the Supplemental Appendix (available in the online version of this article).
Descriptive statistics for the number of impacts across the season by tackle and flag athletes, ages 6 to 14 years, United States, 2017 and 2018
Results
There were 186,239 head impacts (10g-200g) recorded during the regular football seasons: 185,695 for tackle football and 544 for flag football. Of these, there was a median of 378.00 ± 470.00 head impacts per tackle football athlete and 8.00 ± 12.50 head impacts per flag football athlete (Table 3). On average, per AE, there were 9.19 (8.18-10.32) impacts for a tackle athlete and 0.63 (0.43-0.92) impacts for a flag athlete (Table 4); a tackle football athlete had 14.67 (9.75-21.95) times more impacts per AE compared with a flag football athlete. The linear acceleration 50th percentile impact for each athlete, averaged across athletes, was 18.15g (95% CI, 17.95-18.34) for a tackle football athlete and 16.84g (15.57-18.21) for a flag football athlete. The 95th percentile of linear acceleration per athlete, averaged across athletes, was 52.55g (51.06-54.09) for a tackle football athlete and 33.51g (28.23-39.08) for a flag football athlete. Examining high-magnitude impacts (≥40g), a tackle football athlete is estimated to sustain approximately 100 impacts per 100 AEs, whereas a flag football athlete is estimated to sustain approximately 4 impacts per 100 AEs. This translates to a tackle football athlete sustaining 23.00 (13.59-39.55) times more ≥40g impacts per AE compared with a flag football athlete.
Model estimates for tackle versus flag athletes’ outcome variables, ages 6 to 14 years, New York, United States, 2017 and 2018
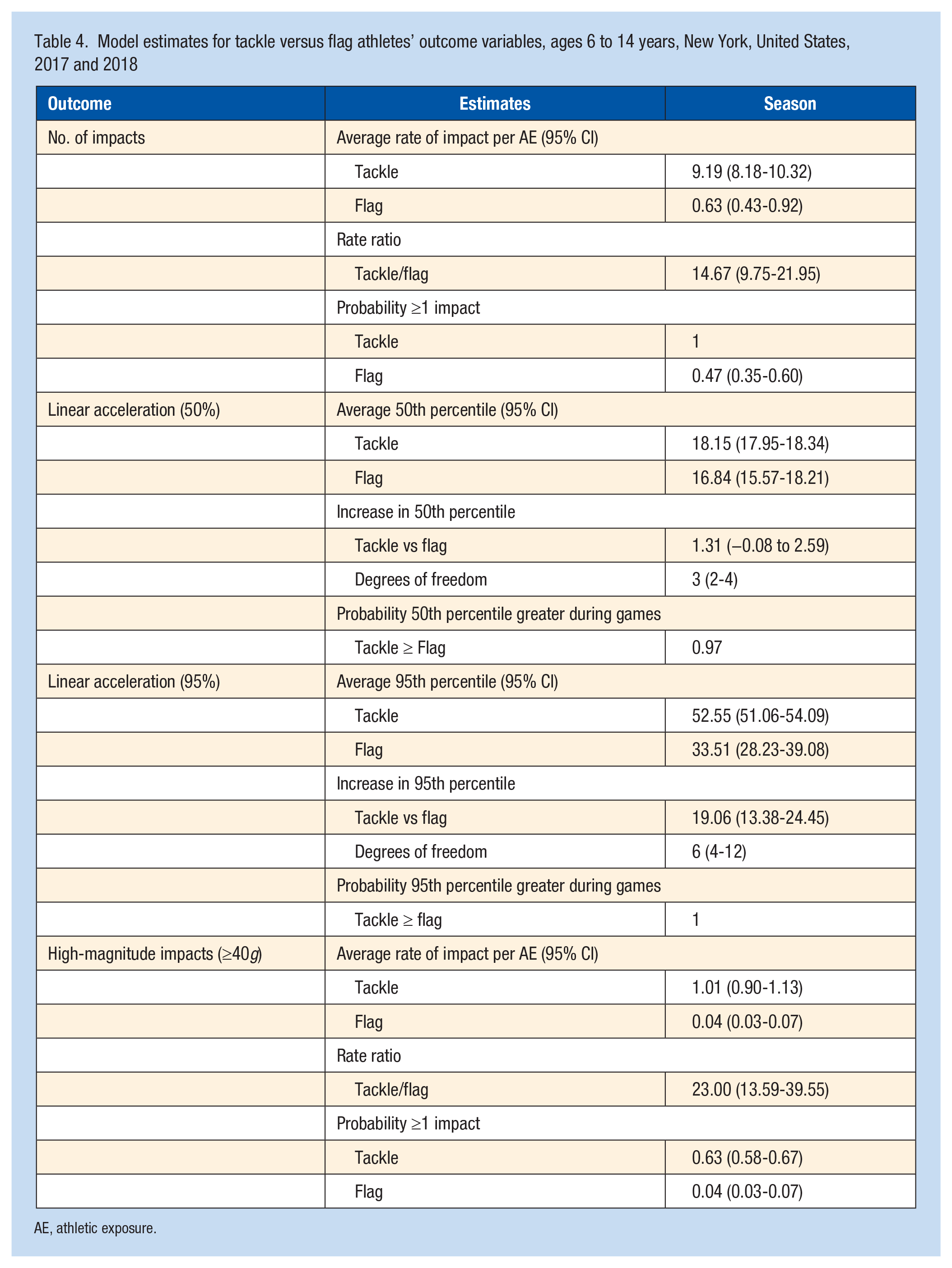
AE, athletic exposure.
Discussion
Tackle football athletes sustained a greater number of head impacts per AE and were at increased risk for high-magnitude impacts compared with flag football athletes. Health care providers may consider these findings when consulting with youth and parents during football preparticipation medical examinations, especially those athletes with an increased risk for concussion (eg, athletes with a history of concussion). 31
Differences in head impact exposure risk between tackle and flag football athletes may be explained by the nature of the game (tackling is part of regular game play) and differences in the athletes who play tackle versus flag football. Tackling increases an athlete’s risk for head impacts and contributes to approximately two-thirds of concussions among high school football athletes.26,33 Moreover, a study by Kontos et al 26 found that almost half (45%) of concussions in tackle football result from head-to-head contact. Both linear and rotational acceleration play a role in sustaining a concussion. 7 While the exact contribution of each type of acceleration on concussion and concussion severity is not clear yet, some evidence suggests that linear acceleration is related to the compression of cerebral tissue, while rotational acceleration is involved in shearing of cerebral neurons (for more information about the biomechanics of head impacts, concussion, and the role of sensors please see Broglio et al 7 ). As tackling is not part of flag football, an athlete’s exposure to head impacts is reduced. Tackle football may also draw more parents and athletes who are less apprehensive about athlete-to-athlete collisions. Tackle football players who were less cautious tended to incur higher magnitude hits. 54 Differences in head impact exposures between tackle and flag football athletes may also result from factors such as variations in practice intensity, coaching style (including the types of practice drills), and athletic intensity, as well as differences in positions and helmet usage.8,12,24,26,36 Mihalik et al 36 found that helmet-only practices are associated with more frequent and higher magnitude head impacts. Greater head impact exposure among helmeted athletes may be attributed to perceived injury susceptibility (eg, wearing a helmet will protect an athlete from injury, and thus they are more apt to collide with opposing players). 29
The only previous study comparing flag versus tackle football impacts found that tackle football athletes had 4.61 times more impacts (>14g) per AE compared with flag athletes. In addition, flag football athletes also had reduced odds of sustaining impacts greater than 20g. 32 Consistent with Lynall et al, 32 our results also found that tackle football athletes were more likely per AE to experience a head impact and sustain greater magnitude impacts over the course of a football season. However, in our study, a tackle football athlete may sustain 14.67 times more impacts ≥10g during an AE compared with a flag football athlete. Some reasons for the discrepancy in findings may be due to a lower threshold of the sensor (10g vs 14g) as well as due, more likely, to different metrics being analyzed (number of impacts per AE vs likelihood of sustaining at least 1 impact per AE). In addition, because our study used a mouthguard sensor while Lynall et al 32 used a sensor embedded in a headband or skullcap, the metrics of 2 studies may not be directly comparable.4,11,46
While more research is needed to determine the effect of repetitive, lower magnitude head impacts, high-magnitude head impacts are associated with a greater risk for concussion 47 and with changes to brain functional and structural integrity. 48 Youth tackle football athletes in the current study sustained an estimated 23.00 times more high magnitude (≥40g) impacts per AE as compared with a flag football athlete. Our findings also suggest that for high-magnitude impacts, a tackle football athlete is expected to sustain approximately 100 impacts at ≥40g per 100 AEs, while a flag football athlete is expected to sustain approximately 4 impacts at ≥40g per 100 AEs.
Over the past decade, some sports programs have initiated steps to mitigate exposure to head impacts through contact restrictions and rule changes. The US ice hockey governing body prohibits body checking for athletes younger than 13 years, while the US soccer governing body prohibits heading instruction until athletes are 11 years old. 53 One of the major criticisms of these rules is a concern that lack of experience with contact sport play may lead to greater risk of concussion for athletes once contact is introduced. However, delaying the introduction of body checking in ice hockey did not result in an increase in head impacts once body checking was introduced. 10 Moreover, other studies5,19 have shown a 3-fold increase in concussion rates in leagues where body checking was permitted versus prohibited (though see Krolikowski et al 27 for an exception). A recent survey 14 found that most US parents support age restrictions for tackling in football. However, previous research has found a lack of access to flag football in some communities. 28 This may limit options for some parents making football participation decisions for their child and may contribute to health inequities, placing some youth football athletes at increased risk for injury. 28
This study has several limitations. First, there are likely differences in athlete characteristics between those who choose to play tackle versus flag football, and this may have affected the results. However, we attempted to address athlete-level differences for impact risk beyond those associated with the type of football through modeling of player-level random effects. Second, head impacts were not video verified. This may have resulted in the inclusion of some invalid head impact exposures. Third, the study did not collect attendance data (exposure) for the tackle football teams. We assumed a tackle football athlete was present at each session in which any athlete on the team had a recorded impact. This assumption results in an underestimate of the rate of impacts per AE for tackle football and represents a conservative estimate comparing the relative risk of impacts with flag football athletes. Fourth, the 95% credible interval for the ≥40g high-magnitude rate ratio was wider than for other estimates, indicating greater uncertainty. The large number of flag football athletes who did not sustain a ≥40g impact, as well as the lower number of flag football athletes, may have contributed to this uncertainty. This limited our ability to assess even higher impacts (≥60g or ≥80g). Fifth, an uneven distribution of playing time among athletes, and variations in the length of games and practices, may also explain some of the variation in the risk of sustaining head impact exposure. These factors were not available for inclusion in comparisons between flag and tackle football. Finally, concussion risk was not assessed as a part of this study. Further investigation, especially at the youth level, is warranted.
Conclusion
Athletes who played tackle football sustained a greater number of head impacts and were at increased risk for high-magnitude impacts, in comparison with flag football athletes. Flag football athletes are exposed to fewer head impacts and this may result in lower concussion risk, making it a safer alternative for youth football athletes.
Supplemental Material
sj-docx-1-sph-10.1177_1941738121992324 – Supplemental material for Head Impact Exposures Among Youth Tackle and Flag American Football Athletes
Supplemental material, sj-docx-1-sph-10.1177_1941738121992324 for Head Impact Exposures Among Youth Tackle and Flag American Football Athletes by Dana Waltzman, Kelly Sarmiento, Owen Devine, Xinjian Zhang, Lara DePadilla, Marcie-jo Kresnow, Kelley Borradaile, Andrew Hurwitz, David Jones, Ravi Goyal and Matthew J. Breiding in Sports Health: A Multidisciplinary Approach
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
This study was funded by the Centers for Disease Control and Prevention (CDC), contract solicitation BAA#2016-N-17798. The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the CDC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.