
Abstract
Background:
Extracorporeal shock wave therapy (ESWT) is a widely considered treatment option for Achilles tendinopathy. Line-focused ESWT is a novel technique treating a larger tendon area than point-focused ESWT. Monitoring capacities of clinical symptoms with ultrasound under ESWT treatment are unknown.
Hypothesis:
Point- and line-focused ESWT have a superior outcome than placebo ESWT. ESWT leads to morphological tendon changes detectable with ultrasound.
Study Design:
Single-blinded placebo-controlled randomized contolled trial.
Level of Evidence:
Level 1.
Methods:
The study was conducted in 3 cohorts, namely ESWT point (n = 21), ESWT line (n = 24), and ESWT placebo (n = 21). Victorian Institute of Sports Assessment–Achilles (VISA-A) score was measured before the intervention (T0), after 6 weeks (T1), and after 24 weeks (T2). All cohorts performed daily physiotherapy for 24 weeks and received 4 sessions of point-focused, line-focused, or placebo ESWT in the first 6 weeks. Ultrasound was performed with B-mode, power Doppler, shear wave elastography (SWE) at T0 and T2 and with ultrasound tissue characterization (UTC) at T0, T1, and T2. Data were analyzed with a mixed analysis of variance and t test.
Results:
There was a significant VISA-A improvement over time for all groups (P < 0.001). ESWT point had the strongest VISA-A score improvement +23 (ESWT line: +18; ESWT placebo: +15), but there was no significant interaction between time and any of the groups: F(4, 116) = 1.393; P = 0.24. UTC, power Doppler, and B-mode could not show significant alterations over time. SWE revealed a significant increase of elastic properties for ESWT point in the insertion (t = −3.113, P = 0.03) and midportion (t = −2.627, P = 0.02) over time.
Conclusion:
There is a significant VISA-A score improvement for all study groups without a statistically significant benefit for ESWT point or ESWT line compared with ESWT placebo. Tendon adaptation could only be detected with SWE for ESWT point.
Clinical Relevance:
The present study could not detect any statistically relevant effect of ESWT compared to placebo. SWE is able to demonstrate tendon adaptation.
Extracorporeal shock wave therapy (ESWT) is a further therapeutic option for Achilles tendinopathy (AT). 33 However, comparison with placebo ESWT treatment has only been investigated in a few previous studies7,19,28,30 with small sample sizes, heterogeneous and limited outcome measures, and design flaws with heterogeneous protocols, so that there is a low level of evidence.
In focused ESWT, mechanical forces are applied locally with the maximum pressure in the focal spot. 33 ESWT with a point-focused area generates a small treatment volume with only a few millimeters in diameter (depending on the intensity level), so that the applicator has to be moved along the point of maximum pain to ensure an even distribution of the energy. Recently, a new line-focused ESWT applicator with an equally distributed energy density (ED) level on a line with 50 mm length (Richard Wolf GmbH, FBL 10x5 G2) has been introduced especially for applications with larger treatment volumes such as in wound healing or erectile dysfunction. 11 Although the maximum pressure is smaller compared with point-focused ESWT, line-focused ESWT may deliver a similar amount of energy to the tendon in total with the same number of pulses due to the larger treatment volume (Figure 1).
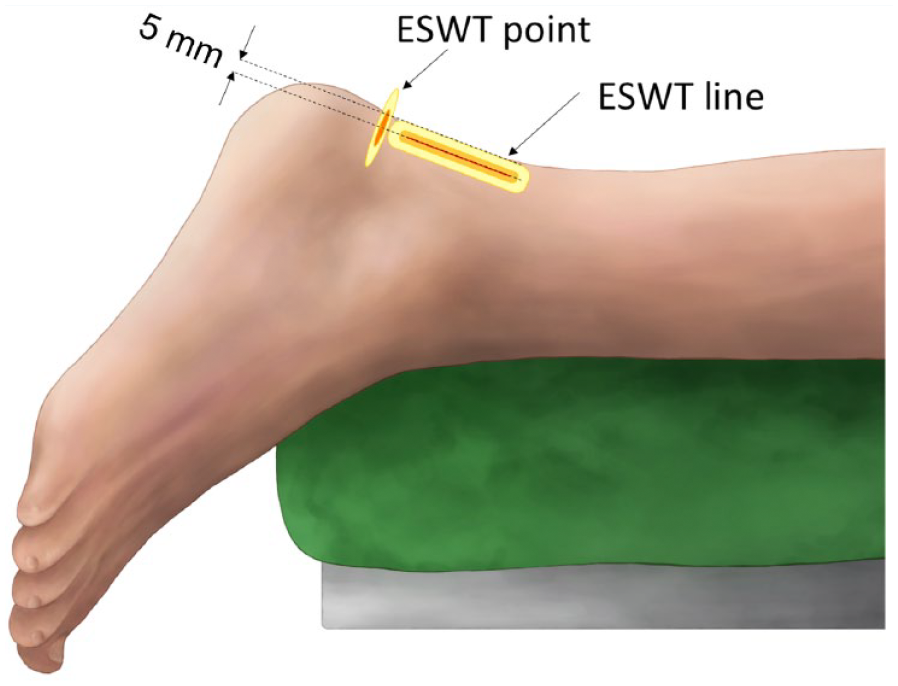
Point- and line-focused extracorporeal shock wave therapy (ESWT): the tendon volume treated with line-focused ESWT is larger than in point-focused ESWT. However, the maximum energy density is higher in point-focused ESWT than in line-focused ESWT.
There are many theories21,33 regarding the biological effect of ESWT like the activation of biological cascades through mechanical stimulation of shock waves, which may induce proliferation of tenocyte and collagen synthesis. Novel ultrasound imaging modalities evaluating tissue elasticity or providing semihistological information may help in a better understanding of the underlying mechanisms. Besides the conventional ultrasound modalities such as B-mode (B-US) or power Doppler (P-US), shear wave elastography (SWE) and ultrasound tissue characterization (UTC) revealed improved diagnosis and monitoring capacities for tendinopathies and sufficient correlation to clinical scores.10,14,35,36 However, SWE and UTC have not been used to investigate the treatment effects of ESWT on tendons yet.
The added value of this study is the clinical evaluation of ESWT application of point- and line-focused shock waves in comparison with a placebo treatment. The placebo-controlled study design with 3 cohorts adds further novelty. In addition, the clinical outcome will be considered in relation to ultrasound findings of structural changes evaluated with UTC and SWE. We hypothesized that point- and line-focused ESWT will reveal a superior outcome compared with a placebo treatment and that UTC and SWE demonstrate structural tendon improvement in line with clinical changes.
Methods
Based on the Consolidated Standards of Reporting Trials guidelines, this is a prospective randomized, single-blinded, placebo-controlled clinical trial comparing 3 intervention groups: group 1, physiotherapy + line-focused ESWT (ESWT line); group 2, physiotherapy + point-focused ESWT (ESWT point); group 3, physiotherapy + placebo ESWT (ESWT placebo). 32 The investigation was approved by the clinical ethics committee of the local medical faculty (EK 113/18) and registered in an official World Health Organization trial register (DRKS00014594). All participants provided written informed consent.
Inclusion and Exclusion Criteria
Participants were recruited from pharmacies, physiotherapist’s or doctor’s offices from July 2018 to May 2019. AT was confirmed by clinical history and a thorough physical examination by an experienced physician with pain provoked by palpation (sensitivity 84%, specificity 73%). 16 Inclusion criteria were insertional or midportion AT, age ≥18 years, minimum symptom duration of 3 months, and the physical ability to perform the physiotherapeutic exercises. Moreover, patients were excluded if they were pregnant, were over- or underweight (body mass index [BMI] >35 kg/m2; BMI <17 kg/m2), had injections in the past 6 months, a previous rupture or an operation in the area of symptoms, soft tissue malignancies or osteomyelitis in the lower limb, or a partial rupture revealed by ultrasound.
Study Design
Figure 2 gives an overview about the study design with 3 measurement time points for the score assessment and ultrasound examination: before intervention (T0), after 6 weeks (T1), and after 24 weeks (T2). Primary outcome measure was the Victorian Institute of Sports Assessment–Achilles (VISA-A) score, which is specifically designed for AT (0 points: maximum pain; 100 points: no pain). 23 Relevant clinical improvement or worsening was determined by a change of ±10 VISA-A score points and scores over 90 VISA-A points were considered as an excellent outcome.17,24,25 Additionally, we used the American Orthopaedic Foot and Ankle Society (AOFAS) as a general score for foot pathologies. 20 Personal assessment was scored by the patient with a 6-point Likert-type scale (1 = completely recovered, 2 = much improved, 3 = somewhat improved, 4 = hardly improved, 5 = not improved, 6 = worse) and the actual status with a 4-point Roles and Maudsley Scale (1 = excellent, 2 = good, 3 = acceptable, 4 = poor).27,31 Participants were randomly assigned to the 3 groups before the first appointment by an independent person, using sealed numbered envelopes. Patients were blinded to the dedicated therapy groups. However, because of the nature of the direct noticeable painful effect of ESWT, physicians could not be blinded. Sample size was calculated to n = 17, based on an α error of 0.05 and a β error of 0.2 assuming that the VISA-A score of the groups (SD 10) with the effective ESWT treatment would reach in general 10 VISA-A points more than the placebo group (power 0.80).
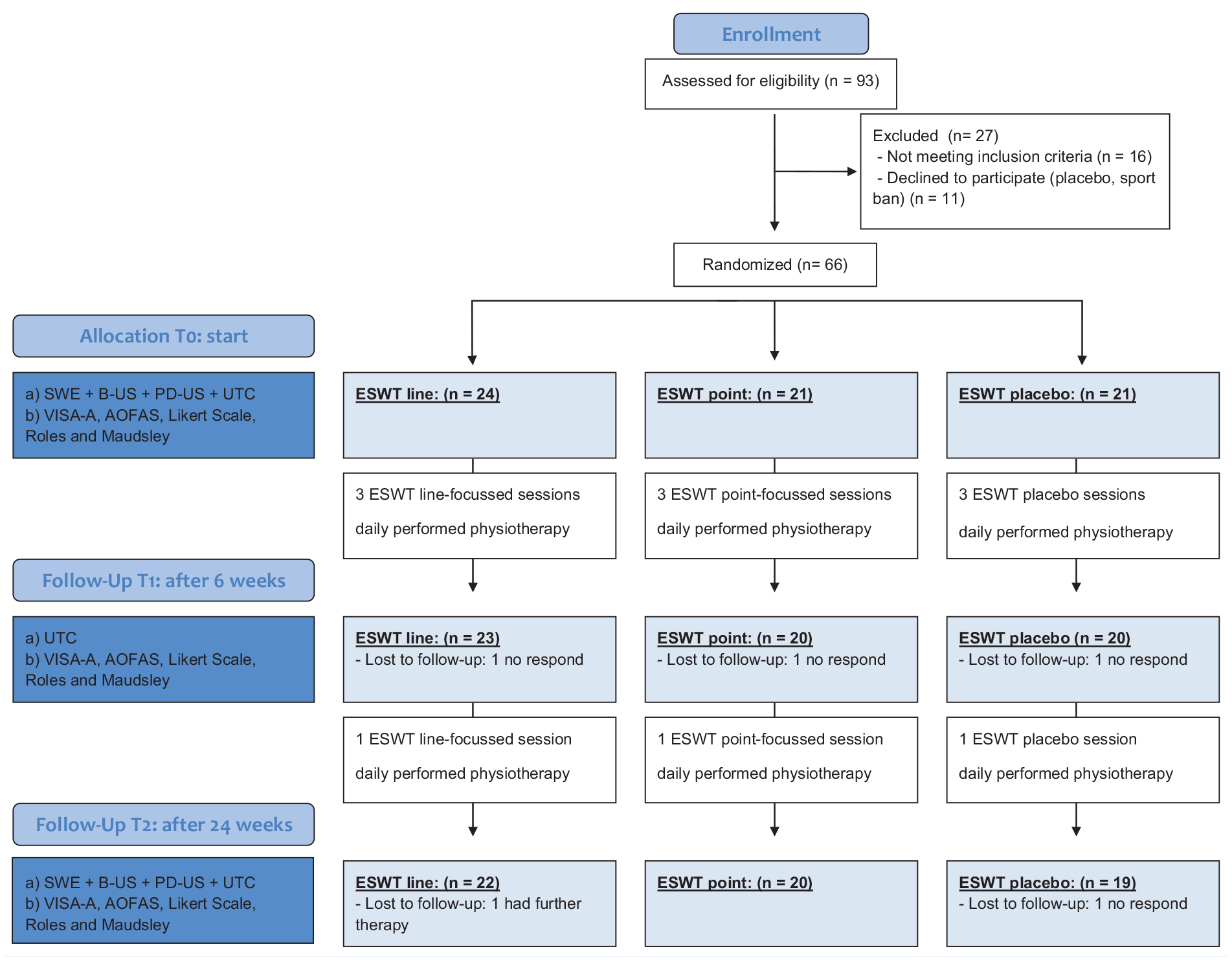
Flowchart of the study design. AOFAS, American Orthopaedic Foot and Ankle Society; B-US, B-mode ultrasound; ESWT, extracorporeal shock wave therapy; P-US, power Doppler ultrasound; SWE, shear wave elastography; UTC, ultrasound tissue characterization; VISA-A, Victorian Institute of Sports Assessment–Achilles.
Intervention: Physiotherapy
The baseline therapy for all groups were home-based eccentric and isometric exercises and static stretching. At baseline, all exercises were demonstrated by a physician with a background as a physiotherapist and the participants received a brochure. At every follow-up appointment, the correct performance of the exercises was evaluated and the frequency of the exercises actually done was noted. Participants were instructed to perform eccentric exercises twice per day (3 sets with 15 repetitions) and static stretching (1 set) and isometric training (1 set with 5 repetitions) once per day for the whole study period. The exact physiotherapy protocols have been described previously. 12
Intervention: ESWT
For ESWT treatment, all patients were placed in prone position unable to see the machine but able to hear the characteristic ticking sound. Patients were informed that discomfort does not allow to draw conclusion on a sham or effective ESWT treatment giving misleading information that sham treatment could also be painful by the contact pressure or that sham treatment might be a new painless ESWT technique. The ESWT protocol was based on previous unpublished data15,30 of the company and a recommended consensus of ESWT practitioners with a maximum delay of 14 days between sessions. Participants received in total 4 standardized ESWT sessions at T0, T0 + 2 weeks, T0 + 4 weeks, and T1 by 2 carefully trained physicians. ESWT was generated by Piezowave 2 (Richard Wolf GmbH; gel pad 5-mm penetration) using the point-focused applicator F10G4 for ESWT point and the line-focused applicator FBL10x5G2 for ESWT line. In the sham treatment group, the gel pad contained an air-filled cavity, so that shock wave propagation was blocked. Using the line-focused applicator, a larger area of the tendon is treated with each shock wave (5 MPa focal area: point: A = 85 mm2 vs line: A = 170.1 mm2, at maximum intensity level 20, Figure 1), but it has to be considered that the applied ED is less (point: ED = 0.83 mJ/mm2 vs line: ED = 0.16 mJ/mm2, at maximum intensity level 20). At each session, 2000 shocks were delivered at 5 Hz at the Achilles tendon with a sliding motion of the applicator concentrating on the painful area. For line- and point-focused ESWT treatment, the intensity level (1-20) was individually adjusted to a submaximal tolerable pain level and the individual mean doses were noted for each session. Moreover, 500 additional shocks (5 Hz, level 20) were applied to the calf muscles of each affected limb to diminish muscular tension. 18 Local anesthesia or ultrasound guidance was not used. During the phase of ESWT treatment (T0 to T1+ 2 weeks) no sporting activity was allowed.
Data Acquisition With B-US, PD-US and SWE
Every participant underwent a standardized multimodal ultrasound protocol consisting of B-US, PD-US and SWE at T0 and T2 based on previously published protocols (Aixplorer, Supersonic Imagine; probe: SuperLinear SL 18-4).12,13 In B-US, tendon thickness in longitudinal and transversal planes and the greatest cross-sectional area (CSA) were measured. Using PD-US, neovascularization was rated according to the Öhberg score. 26
SWE evaluates tissue elasticity, measuring shear wave speed propagation (m/s) within the tissue and by deducing the Young’s modulus (up to 800 kPa, 16 m/s) with a high reliability (interobserver: 0.940, intraobserver: 0.916).22,36 The standard size of SWE measurement window was 1 cm2 with a region of interest (ROI) of 3 mm in the most rigid part of the measurement window (ROI 3 mm) and an individual ROI covering the whole tendon area (ROI ind.). Tendon stiffness was rated separately according to insertion (0-2 cm of the calcaneus) and midportion (2-6 cm) with 3 measurements for each localization.12,13
Data Acquisition With UTC
UTC (UTC Tracker, UTC Imaging; probe: SmartProbe 12L5-V, Terason 2000+; Teratech) offers semihistological data about tendon properties quantifying the consistency of gray level and offers sagittal, coronal, and transverse planes with reliable results for Achilles tendon imaging (excellent [0.92-0.95] interobserver reliability). 35 Based on previously published standardized protocols, UTC scans were performed by 2 experienced examiners at T0, T1, and T28,29,35 with a ROI quantification of the CSA of the tendon structure in the axial planes: insertion (proximal calcaneus 0-2 cm; interval 2 mm), midportion (2-6 cm; interval 4 mm), and the whole tendon (0-6 cm, interval 2/4 mm). Using the standardized UTC algorithm (17 continuous images), tendon bundles were classified into 4 color-coded echo types: echo type I—intact (green); echo type II—discontinuous wavy (blue); echo type III—fibrillar (red); and echo type IV—amorphous matrix (black). 35
Statistical Analysis
For all analyses, SPSS 24.0 was used to assess statistical significance (P < 0.05). Normal distribution was evaluated with a Kolmogorov-Smirnov test and Shapiro-Wilk test. One-way analysis of variance (ANOVA) with repeated measures (Greenhouse-Geisser correction), mixed ANOVA, t test, and Friedmann test rated significant changes over time for the VISA-A and AOFAS score and ultrasound values in relation to group differences and the interaction between time and groups, respectively. Post hoc tests used the Bonferroni correction. Pearson’s correlation coefficient analyzes the correlation in between the VISA-A scores and the intensity level of ESWT.
Results
In total, n = 24 patients (44a, 50% male, BMI = 25 kg/m2) were included for ESWT line, n = 21 patients (42a, 70% male, BMI = 27 kg/m2) for ESWT point, and n = 21 patients (51a, 60% male, BMI = 25 kg/m2) for ESWT placebo. Table 1 demonstrates the demographics showing no statistically significant differences between the groups. The flowchart in Figure 2 depicts the exact group sizes during the study period. Until T1, all patients were performing the basic physiotherapy on average 5 times/wk, while afterward they performed physiotherapy only 3 times/wk without significant differences between the groups. There were no side effects of ESWT or physiotherapy.
Demographic data a
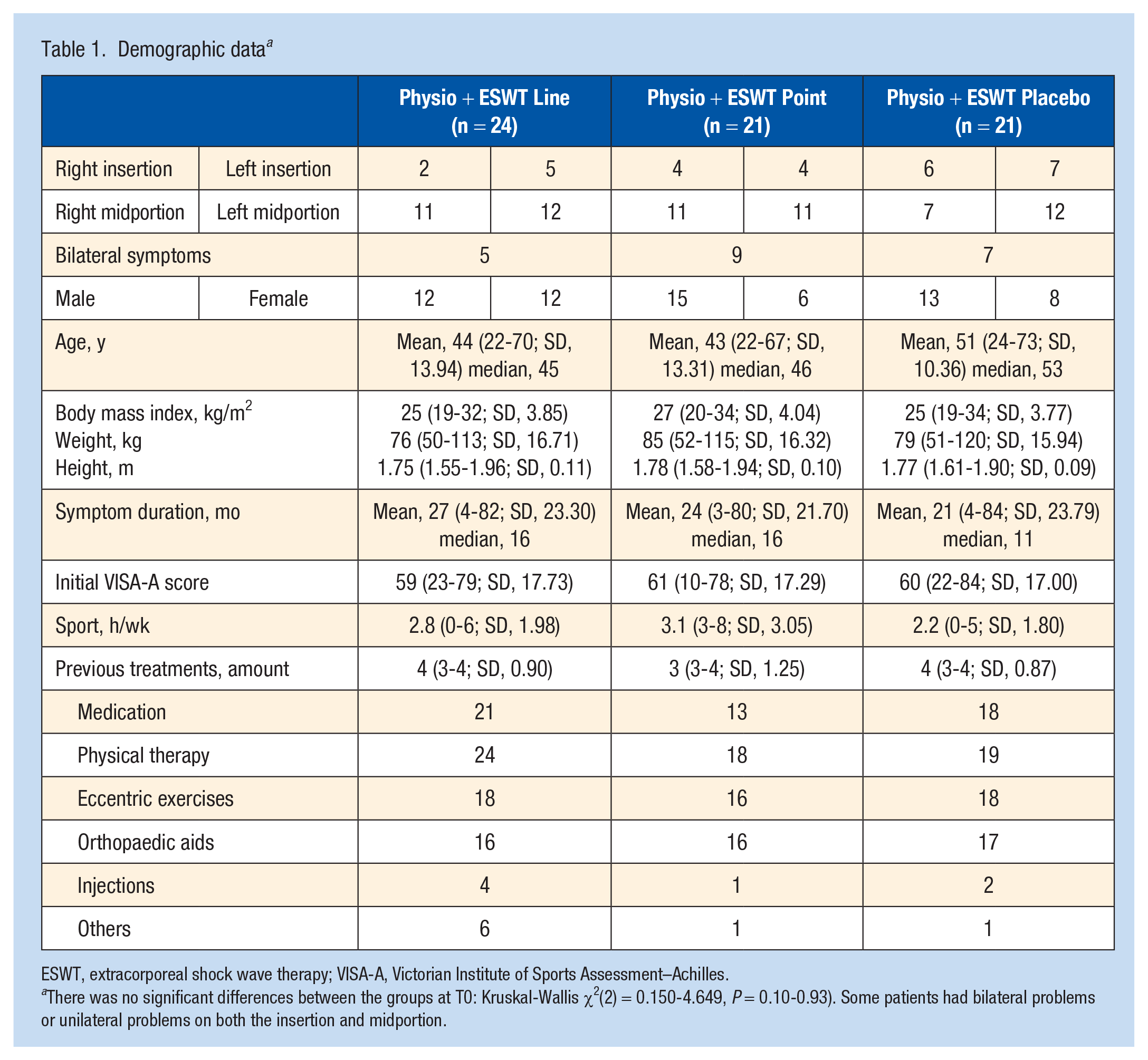
ESWT, extracorporeal shock wave therapy; VISA-A, Victorian Institute of Sports Assessment–Achilles.
There was no significant differences between the groups at T0: Kruskal-Wallis χ2(2) = 0.150-4.649, P = 0.10-0.93). Some patients had bilateral problems or unilateral problems on both the insertion and midportion.
Clinical Outcome
ANOVA with repeated measurements revealed a significant VISA-A score improvement over time for all groups: ESWT line F(2/42) = 14.592, P < 0.001, η2 = 0.410; ESWT placebo F(1.5/26.3) = 8.909, P = 0.003, η2 = 0.331; ESWT point F(2/38) = 29.8551, P < 0.001, η2 = 0.611 (Figure 3). ESWT point had the strongest VISA-A score improvement of +23 throughout the whole study period (ESWT line: +18; ESWT placebo: +15) and a significant score change directly after 6 weeks (P = 0.001). However, a mixed ANOVA could not report a statistically significant VISA-A score benefit for one group over the other (F(4, 116) = 1.393, P = 0.24, η2 = 0.455). Secondary outcome measures showed more satisfied patients for ESWT line and point in the self-reporting Roles and Maudsley Score and the Likert-type scale at T2 (Appendix Figure 4, available in the online version of this article).
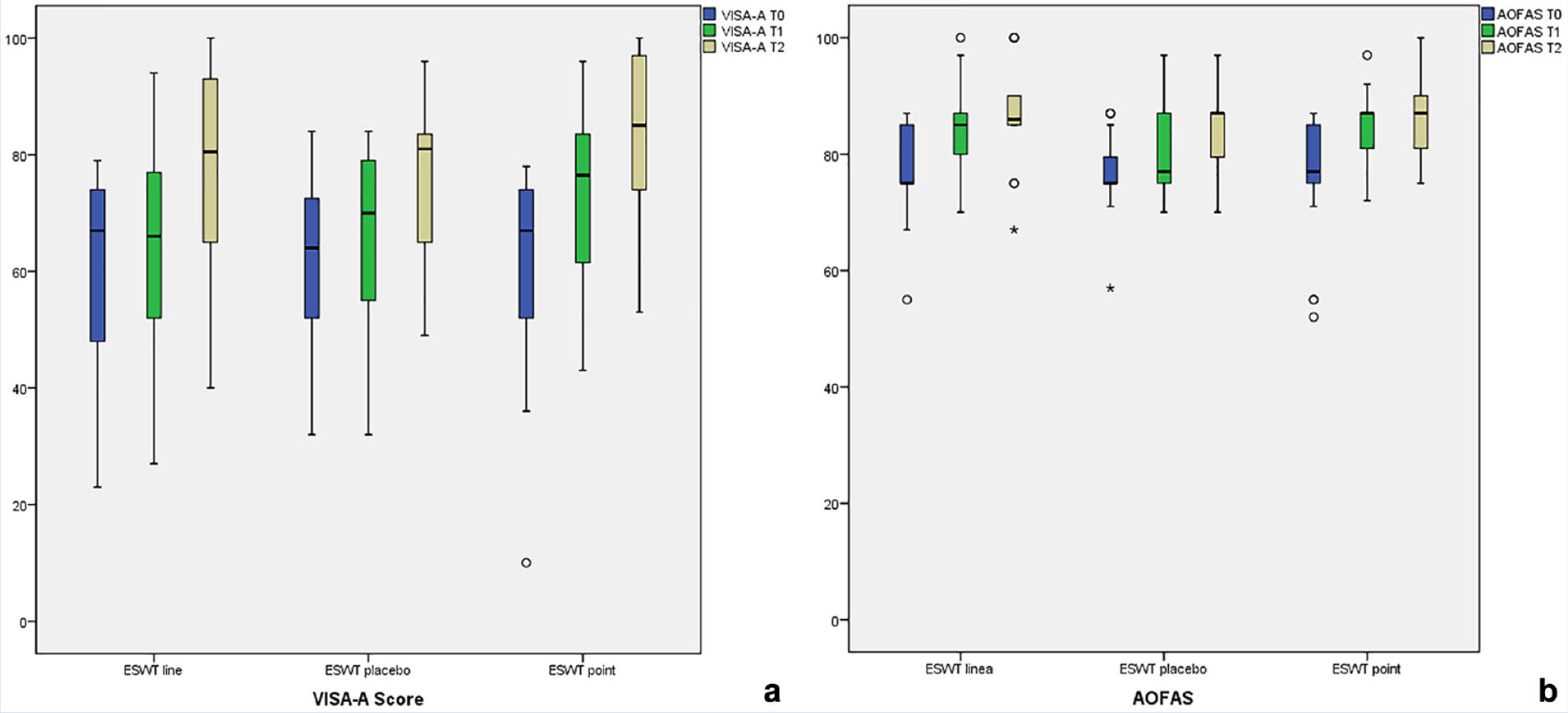
(a, b) Box plots illustrating VISA-A, Victorian Institute of Sports Assessment–Achilles (VISA-A) and American Orthopaedic Foot and Ankle Society (AOFAS) score. ESWT, extracorporeal shock wave therapy.
Correlation of ESWT Level With VISA-A Score
In ESWT line, the mean intensity level of 4 sessions was 17.2 (13.1-19.3; SD, 1.5), corresponding to ED = 0.126 mJ/mm2, pmax = 9.5 MPa and E5MPa = 11.51 mJ. In ESWT point, the mean intensity level was 15.8 (7.7-19.2, SD 3.4), corresponding to mean shock wave parameters ED = 0.6 mJ/mm2, pmax = 50.3 MPa, and E5MPa = 15.45 mJ.
Moreover, there was no significant correlation for ESWT point and ESWT line between absolute VISA-A score improvement and mean ESWT intensity level regarding T0, T1, and T2 (ESWT point: r = −0.86 to 0.111, P = 0.58-0.74; ESWT line: r = −0.154 to 0.84, P = 0.44-0.91).
Imaging Findings
Appendix Table 2 (available online) demonstrates the development of B-US and PD-US parameters, showing no significant change in tendon diameter or CSA after 6 months (P = 0.29-0.10). Although the neovascularization decreased, a Friedmann test did not demonstrate a significant finding in PD-US, χ2(1) = 1.884, P = 0.17. Appendix Table 3 (available online) depicts SWE values for all groups and measurement points. Only ESWT point revealed a significant increase of SWE values in the insertion (P = 0.03; P = 0.05) and midportion (P = 0.02, P = 0.002) over the treatment period in comparison with the other groups (P = 0.05, P = 0.05) (Appendix Figure 5, available online).
Appendix Table 4 (available online) demonstrates UTC values for all groups and measurement points. The only significant improvement in tendon structure was seen for ESWT line (P = 0.04) and ESWT placebo (P = 0.02) after 24 weeks with a decrease of fibrillar matrix (type III). ESWT point treatment revealed a significant decrease of intact bundles (type I, P = 0.01) and an inverse increase of fibrillar matrix (type III, P = 0.05) after 6 weeks, which turns into baseline at T2 (Appendix Table 4, available online).
Discussion
The present placebo-controlled randomized controlled trial (RCT) study investigates the effect of line- and point-focused ESWTs in comparison to placebo ESWT, showing a significant VISA-A score improvement in all study cohorts without a statistically superior outcome for line- or point- focused ESWT. Even though ESWT point had the highest mean VISA-A score improvement after 6 weeks and at final follow-up the differences between the groups were statistically insignificant. The line-focused ESWT as a novel technique applying focused shock waves on a larger area of the tendon showed less clinical benefit than the established point-focused ESWT. However, it is difficult to compare the 2 technologies because of their extremely different energy distribution (EDmean: [point] 0.6 mJ/mm2 vs [line] 0.126 mJ/mm2). Although the present study could not reveal a correlation between shock wave intensity level and outcome scores, the reason for slightly better results of point-focused ESWT could be the higher maximal ED. Nevertheless, using ED as a primary shock wave parameter is questionable as it only represents the ED at a very small spot of the shock wave field. Hence, future studies should focus on finding a correlation between the clinical outcome and more specific ESWT sound field parameters.
The current literature only reveals limited and inconsistent results for placebo-controlled ESWT studies concerning AT. Rasmussen et al 30 stated an AOFAS score improvement in both the placebo and intervention group with better results in the radial shock wave group after 8 and 12 weeks. Costa et al 7 could not find differences in pain relief between control and focused ESWT after 12 weeks but using “pain during walking” as an unspecific parameter. Moreover, a recent study 28 could not find a difference at 24 weeks with the usage of radial ESWT for insertional AT compared with sham treatment, but the sample sizes were small (15 vs 16) and the visual analogue scale was used as an unspecific outcome parameter. Rompe et al 31 compared eccentric exercises versus eccentric exercises plus radial shock wave in an RCT study,31 showing a significant difference in favor of the combined approach after 16 weeks but not after 1 year.
A further aim of the present study was to examine the effect of ESWT on morphological changes using ultrasound. In the present study, B-US and PD-US did not depict any alteration in tendon diameter or vascularization despite clinical score improvement. A previous ESWT study of Cheng et al 5 (n = 42, insertional AT) observed no significant alteration in CSA or AT thickness despite clinical improvement after 12 weeks, which is in line with our results. However, contrary to our results, Cheng et al 5 report a significant decreased Öhberg score after 12 weeks. Nonetheless, the role of neovascularization is discussed controversy, since no correlation between pain or disability could be found in patients treated with other therapeutic approaches other than ESWT.9,10 Moreover, SWE could demonstrate significantly higher elastic properties for ESWT point over the study period. These findings are partly in line with previous studies4,10,38 reporting correlation of symptom reduction with increased elastic properties under a physiotherapeutic approach or postsurgical after Achilles tendon repair. Increased elastic properties might be based on a reduced concentration of water-binding proteoglycans in the interfascicular tendon matrix interfering with fascicle sliding during locomotion in symptomatic AT.1,6,34,37 According to UTC findings, the present study demonstrated a significant decrease of fibrillar tendon matrix (type III) for ESWT line and ESWT placebo after 24 weeks, assessing a partly improved histological structure. Interestingly, ESWT point leads to a worsening of the tendon matrix after 6 weeks with reduced intact (type I) but increased fibrillar tendon bundles (type III). This might be based on a reversible subclinical tendon bundle damage, which turns into baseline at T2.2,3,21 However, the monitoring capacity of UTC might be limited with inconclusive association between UTC echo types and clinical outcome. 29
The results of the present study need to be interpreted in light of the following limitations. Improvements of the study design, for example, studying long-term effects, crossover design, or including a cohort only performing basic physiotherapeutic exercises could have elucidated which of the factors—basic physiotherapy or the placebo effect—was crucial for score improvement in ESWT placebo.7,28,30 However, we expected a higher dropout rate, if physiotherapy as the therapeutic gold standard would have been withhold. Moreover, there are possible confounding factors such as including both insertional versus midportion AT, reactive versus degenerative, unilateral versus bilateral, and nonathletes versus athletes or a mean symptom duration >6 months and the lack of blinded physicians or a general ESWT intensity application. Up to now, the role of these parameters for ESWT is still unclear. 19 Moreover, the moderate high standard deviation of the initial VISA-A score might be a possible reason for the statistically nonsignificant difference at T2.
Conclusion
This study revealed significant VISA-A score improvement for all groups during 24 weeks without a statistically significant outcome difference between ESWT point, ESWT line, and ESWT placebo. B-US, PD-US, and UTC have no clear benefit for monitoring clinical symptoms, while SWE could partly show significant increased elastic tendon properties in accordance with score improvement.
Supplemental Material
sj-docx-4-sph-10.1177_1941738121991791 – Supplemental material for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study
Supplemental material, sj-docx-4-sph-10.1177_1941738121991791 for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study by Matthias Gatz, Sebastian Schweda, Marcel Betsch, Timm Dirrichs, Matias de la Fuente, Nina Reinhardt and Valentin Quack in Sports Health: A Multidisciplinary Approach
Supplemental Material
sj-docx-5-sph-10.1177_1941738121991791 – Supplemental material for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study
Supplemental material, sj-docx-5-sph-10.1177_1941738121991791 for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study by Matthias Gatz, Sebastian Schweda, Marcel Betsch, Timm Dirrichs, Matias de la Fuente, Nina Reinhardt and Valentin Quack in Sports Health: A Multidisciplinary Approach
Supplemental Material
sj-docx-6-sph-10.1177_1941738121991791 – Supplemental material for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study
Supplemental material, sj-docx-6-sph-10.1177_1941738121991791 for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study by Matthias Gatz, Sebastian Schweda, Marcel Betsch, Timm Dirrichs, Matias de la Fuente, Nina Reinhardt and Valentin Quack in Sports Health: A Multidisciplinary Approach
Supplemental Material
sj-jpeg-2-sph-10.1177_1941738121991791 – Supplemental material for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study
Supplemental material, sj-jpeg-2-sph-10.1177_1941738121991791 for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study by Matthias Gatz, Sebastian Schweda, Marcel Betsch, Timm Dirrichs, Matias de la Fuente, Nina Reinhardt and Valentin Quack in Sports Health: A Multidisciplinary Approach
Supplemental Material
sj-jpeg-3-sph-10.1177_1941738121991791 – Supplemental material for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study
Supplemental material, sj-jpeg-3-sph-10.1177_1941738121991791 for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study by Matthias Gatz, Sebastian Schweda, Marcel Betsch, Timm Dirrichs, Matias de la Fuente, Nina Reinhardt and Valentin Quack in Sports Health: A Multidisciplinary Approach
Supplemental Material
sj-pptx-1-sph-10.1177_1941738121991791 – Supplemental material for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study
Supplemental material, sj-pptx-1-sph-10.1177_1941738121991791 for Line- and Point-Focused Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Placebo-Controlled RCT Study by Matthias Gatz, Sebastian Schweda, Marcel Betsch, Timm Dirrichs, Matias de la Fuente, Nina Reinhardt and Valentin Quack in Sports Health: A Multidisciplinary Approach
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
M.G. was supported by the START and Clinician Scientist programme of the Medical Faculty of RWTH University Aachen.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.