
Abstract
Background:
After a national policy change in 2013 disallowing body checking in Pee Wee ice hockey games, the rate of injury was reduced by 50% in Alberta. However, the effect on associated health care costs has not been examined previously.
Hypothesis:
A national policy removing body checking in Pee Wee (ages 11-12 years) ice hockey games will reduce injury rates, as well as costs.
Study Design:
Cost-effectiveness analysis alongside cohort study.
Level of Evidence:
Level 3.
Methods:
A cost-effectiveness analysis was conducted alongside a cohort study comparing rates of game injuries in Pee Wee hockey games in Alberta in a season when body checking was allowed (2011-2012) with a season when it was disallowed after a national policy change (2013-2014). The effectiveness measure was the rate of game injuries per 1000 player-hours. Costs were estimated based on associated health care use from both the publicly funded health care system and privately paid health care cost perspectives. Probabilistic sensitivity analysis was conducted using bootstrapping.
Results:
Disallowing body checking significantly reduced the rate of game injuries (−2.21; 95% CI [−3.12, −1.31] injuries per 1000 player-hours). We found no statistically significant difference in public health care system (−$83; 95% CI [−$386, $220]) or private health care costs (−$70; 95% CI [−$198, $57]) per 1000 player-hours. The probability that the policy of disallowing body checking was dominant (with both fewer injuries and lower costs) from the perspective of the public health care system and privately paid health care was 78% and 92%, respectively.
Conclusion:
Given the significant reduction in injuries, combined with lower public health care system and private costs in the large majority of iterations in the probabilistic sensitivity analysis, our findings support the policy change disallowing body checking in ice hockey in 11- and 12-year-old ice hockey leagues.
Every year, 1 in 3 youth are expected to seek medical attention for a sport-related injury in Canada.6,9 Ice hockey has one of the highest injury rates among youth sports.6,9,18 There is a strong body of research suggesting that policy allowing body checking in youth ice hockey increases the risk of injury. A meta-analysis of large cohort studies demonstrated a 67% reduction (incidence rate ratio [IRR] = 0.33; 95% CI, 0.25-0.45) in concussion rate in Pee Wee (ages 11-12 years) ice hockey leagues where policy disallows body checking. 7 After years of debate, Hockey Canada and USA Hockey raised the age at which body checking is allowed in games from the Pee Wee level (ages 11-12 years) to the Bantam level (ages 13-14 years). 15 This national body-checking policy change led to a reduction in the incidence rate of all injury by 50% (IRR = 0.5; 95% CI, 0.33-0.75) and concussion specifically by 64% (IRR = 0.36; 95% CI, 0.22-0.58) in Pee Wee ice hockey players in Alberta, Canada. 3 Similarly, in nonelite levels of Bantam (lowest 60% of players by division of play; ages 13-14 years) in regions disallowing body checking, there was a 56% reduction in injury rates (IRR = 0.44; 95% CI, 0.27-0.74) compared with policy allowing body checking in games in nonelite levels of Bantam. 5
Evaluating the cost-effectiveness of policy disallowing body checking in Pee Wee in Quebec (2007-2008) demonstrated significant projected health care cost savings associated with fewer injuries compared with Alberta (allowed body checking) prior to the national body-checking policy change.8,11 The cost-effectiveness of policy disallowing body checking after it was implemented nationally in Pee Wee has not been evaluated previously. The objective of this study was to determine if the injuries and injury-related costs differ for Pee Wee (11-12 years) ice hockey players in the season after a national policy change disallowing body checking in games (2013-2014) compared with a season when body checking was allowed (2011-2012) in the province of Alberta.
Methods
A cost-effectiveness analysis (CEA) was conducted comparing the rate of game injuries and injury-related costs in a cohort of Alberta Pee Wee hockey players in a season where body checking was allowed in games (2011-2012) with a cohort of players in a season where body checking was not allowed (2013-2014). Data on injuries and health care resource use were collected in a prospective cohort study and details of the design, recruitment, and data collection procedures have been published previously. 3 The CEA had a 1-year time horizon, and the base case took the public health care system perspective. Other scenarios considered private health care spending and total public and private health care spending.
Effectiveness
Injury comparisons were standardized using rates of game injury/1000 player-hours between cohorts.
Health Care Resource Use
Costs were considered from the publicly funded health care system perspective in the base case, as well as scenarios including private health care costs borne by families. Health care utilization by players as a result of their injuries were self-reported by player or parent and recorded during the study by a team designate (parent volunteer) on an injury report form (IRF), which also included individual weekly exposure to hockey sessions and injuries. The IRFs were reviewed by a study therapist (physical therapist or athletic therapist) for accuracy who also followed up with the participant by phone if needed. Health care utilization included visits to health care professionals, treatment, imaging, hospitalization, and equipment. In the case where it was indicated that there was a visit/test but the number of tests/visits was missing, we made the assumption that there was 1 visit/test. This was the mode number of visits/tests for all but magnetic resonance imaging (MRI) where the number of tests was missing, so it was not possible to use the mode; however, we made the assumption that only 1 MRI was performed.
Unit Costs
Alberta physician fee schedules 1 were applied to visits to family physicians, orthopaedic surgeons, pediatricians, emergency department (ED) physicians, and radiologists. Unit costs from the Alberta Health Services Calgary Zone were applied to ED, radiography, computed tomography scans, MRI, bone scans, surgery, and fiberglass casts. Unit costs 2 for private health care costs paid by families for physical therapy, chiropractic treatment, massage and athletic therapy, joint bracing, splints, crutches and tensors were obtained from a local Calgary company operating multiple clinics throughout the city. The cost of ambulance trips was sourced from Alberta Health. All costs were adjusted to 2017 Canadian dollars using the Consumer Price Index 2009 medical basket (annual 2002 = 100, geography = Canada, commodities and commodity groups = health care). Transfer costs, such as goods and services tax, were not included in cost calculations. Discounting was not applicable given the 1-year time horizon.
Health care costs were estimated as cost/1000 player-hours. The total cost for each cohort was calculated by multiplying utilization by the respective unit cost and summing across types of utilization for each player. These values were summed to produce the total cost for each group.
Cost-Effectiveness Analysis
The differences in injury rate per 1000 player-hours and differences in the health care cost per 1000 player-hours were calculated for no body checking minus body checking. There are a number of possible combinations of cost and effect differences. If disallowing body checking resulted in lower cost and a lower rate of injuries, then the policy was said to be dominant and would be recommended. In scenarios where there were fewer injuries but higher costs, an incremental cost-effectivness ratio would be calculated, which was the ratio of the difference in mean costs and the difference in injury rate. In that case, judgment would be required to determine if reduction in the injury rate justified the extra costs.
Provincial Projection
The results of the cost-effectiveness analysis were used to project the change in total injuries and health care costs to all Pee Wee hockey players registered in Alberta in the 2015-2016 season (n = 8768). 11 The projected change in total injuries and costs was calculated for each of the public health care system, private health spending, and total costs using the total player population, and then applied to the average player game-hours from the study.
Statistical Analysis
All calculations and statistical analyses were conducted in STATA V14.2 IC. Absolute risk reduction (no body checking minus body checking) was calculated, as well as injury and cost rates for each group while accounting for player game exposure hours. 3 Cost data were not normally distributed; therefore, a nonparametric probabilistic sensitivity analysis using bootstrapping with 10,000 iterations, while accounting for clustering by team, was used to estimate the percentile-based 95% CIs around the costs per body-checking group.
Results
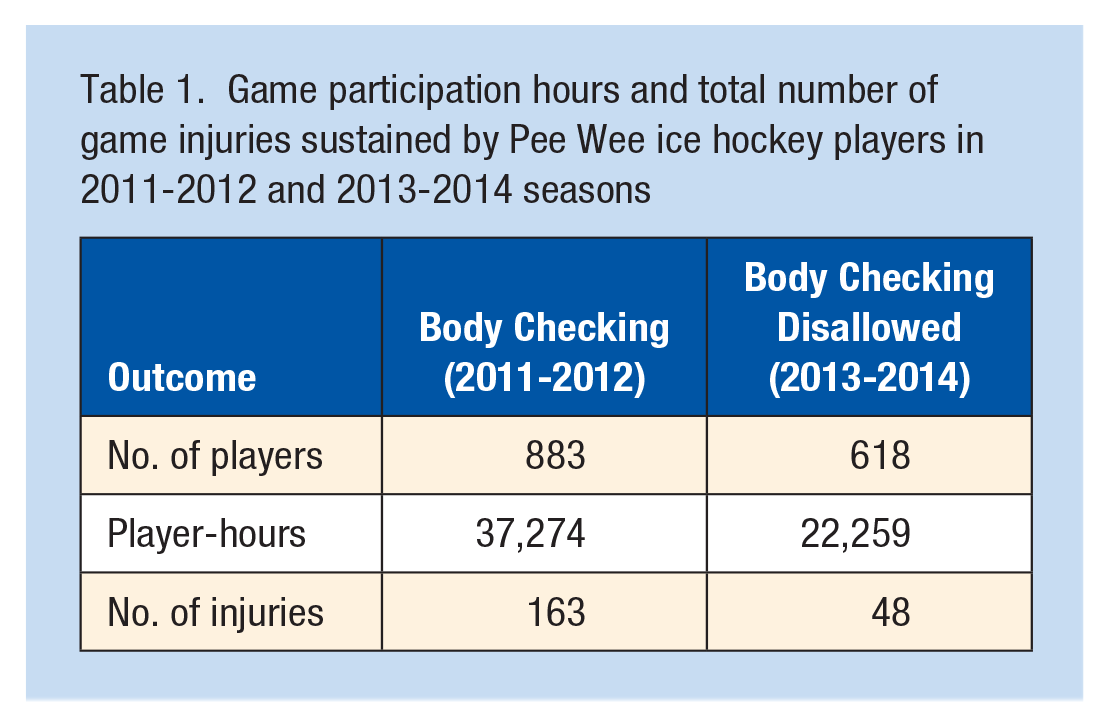
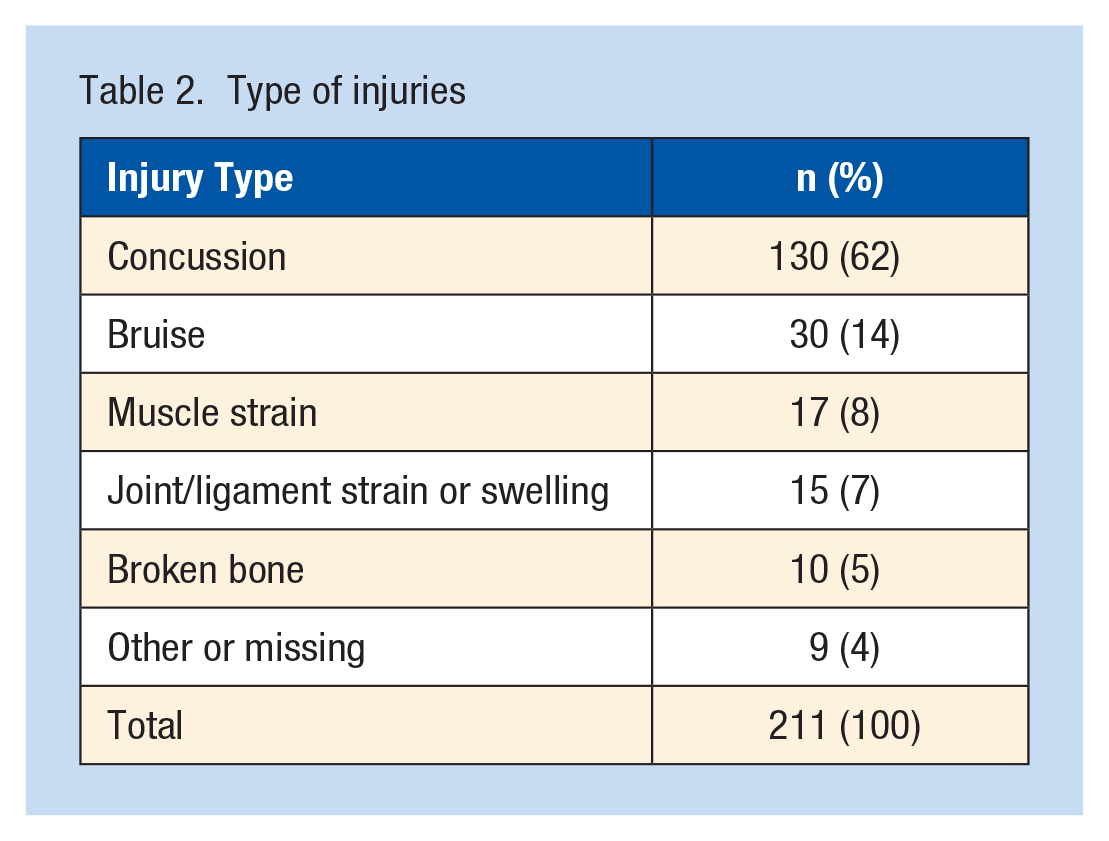
The cohort where body checking was allowed (2011-2012) had 883 players from 59 teams (Table 1), while the cohort where body checking was disallowed (2013-2014) had 618 players from 73 teams. Looking at the unadjusted data (not accounting for player-hours), there were a total of 163 game injuries when body checking was allowed compared with 48 game injuries when it was not allowed. The most common injury type (Table 2) was concussion (62%) followed by bruising (14%) and muscle strains (8%). For 21 of the 211 players with injuries, there was some missing information about the number of visits or treatments when it had been indicated that there was a visit/treatment, in which case it was assumed that there was 1 visit/treatment of the specified type. This accounted for 14.8% of the total costs in the body-checking group, and 15.4% of the total costs in the group where body checking was not allowed.
Game participation hours and total number of game injuries sustained by Pee Wee ice hockey players in 2011-2012 and 2013-2014 seasons
Type of injuries
Public and private health care resource use and costs (unadjusted for differences in players or exposure between groups) are presented in Table 3. Total public health care costs were higher at $18,613 when body checking was allowed compared with $8496 when it was disallowed (Table 3). All components of publicly funded health care utilization were higher when body checking was allowed except for ED visits. The difference in public health care costs was largely driven by visits to sports medicine physicians (30%), general practitioners (31%), and radiographic imaging (35%). Total private health care costs were also higher when body checking was allowed for all items except for athletic therapy. The difference in private costs were largely driven by physical therapy visits (64%) when body checking was allowed. In total private health care costs, $6389 was spent when body checking was allowed and $1969 when body checking was disallowed.
Units of health care resources and direct health care costs (2017 CAD$) incurred by injured players during games in the seasona
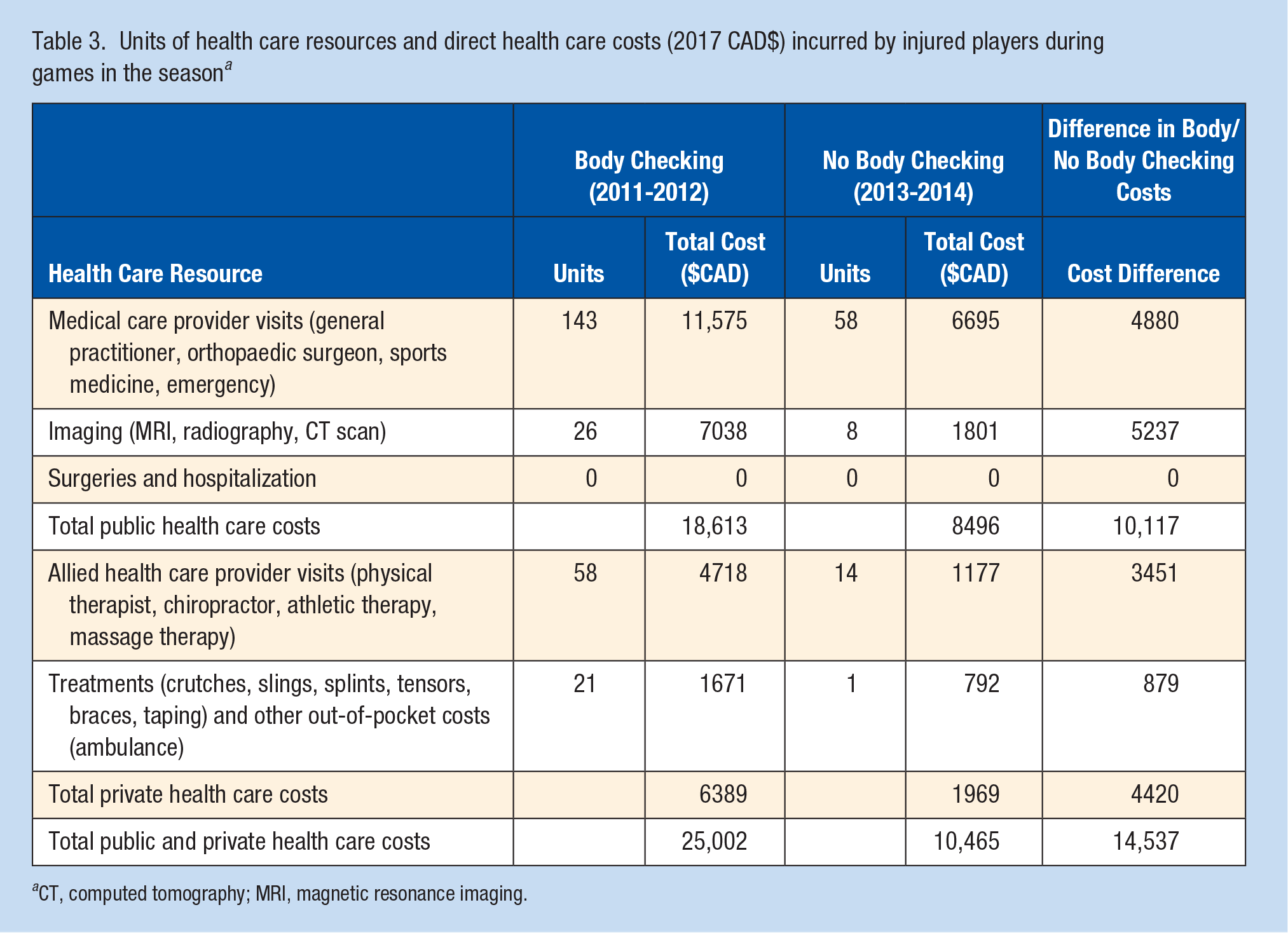
CT, computed tomography; MRI, magnetic resonance imaging.
CEA Results
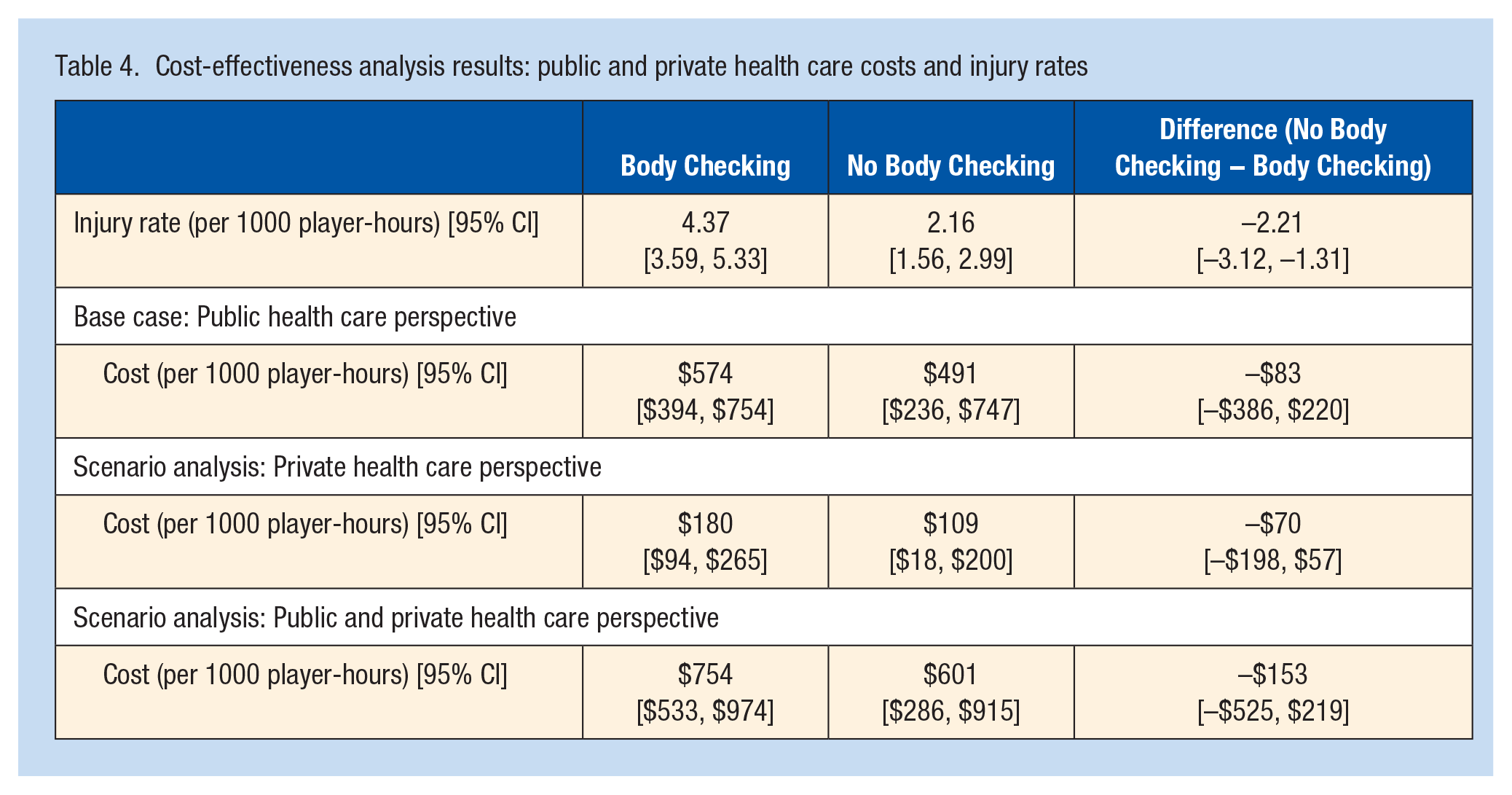
Disallowing body checking was associated with a statistically significant reduction in the rate of injuries in games by 2.21 (95% CI [−3.12, −1.31]) per 1000 player-hours. 3 From the publicly funded health care perspective, we did not find a statistically significant difference in costs (−$83 per 1000 player-hours, 95% CI [−$386, $220]) (Table 4). Similarly, for the private health care perspective and the total health care perspective, we did not find a statistically signicant difference in costs (−$70 per 1000 player-hours, 95% CI [−$198, $57]) and (−$153 per 1000 player-hours, 95% CI [−$525, $219]). Regardless of perspective, the point estimates of both injury rates and costs indicate that disallowing body checking is dominant (ie, with lower costs and lower injury rates).
Cost-effectiveness analysis results: public and private health care costs and injury rates
In the probabilistic sensitivity analysis (Figure 1) for the public health care system perspective, disallowing body checking was a dominant policy (associated with reduced injuries and public health care costs) in 78% of 10,000 iterations. For the private health care perspective, 92% of 10,000 iterations found disallowing body checking to reduce the rate of injuries and reduce private health care cost spending. When the perspective included both public and private health care costs, disallowing body checking reduced both injuries and costs in 87% of the iterations.
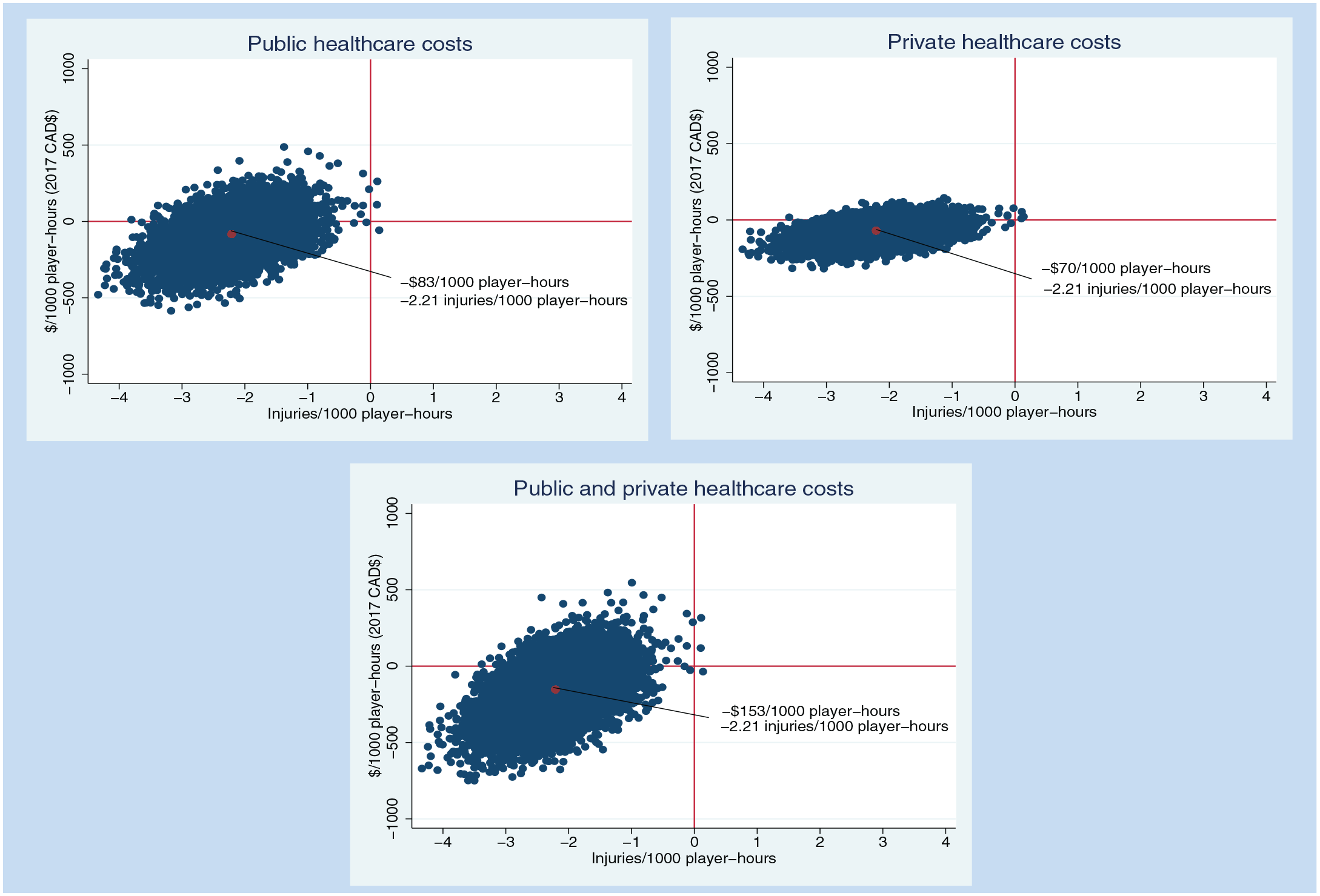
Results of the probabilistic sensitivity analysis for body checking compared with body checking disallowed (body checking minus body checking disallowed).
Provincial Projection Results
Using the estimates of injury and cost reductions from the study to project for the 2015-2016 season for all players in Alberta, 772 injuries could have been prevented due to the change in policy from allowing body checking to disallowing body checking in hockey games (95% CI [−1085, −456]). We did not find a statistically significant difference in provincial costs for any of the perspectives. The point estimates and confidence intervals were $24,399 in public health care cost savings over a season, 95% CI [−$68,856, $19,822], $28,864 in private health care savings, 95% CI [−$134,234, $76,507] and, in total, $53,207 in public and private health care savings, 95% CI [−$182,573, $76,159].
Interpretation
There were 2.21 fewer injuries per 1000 player-hours in Alberta Pee Wee ice hockey after the national policy change in 2013 disallowing body checking in games at all levels of Pee Wee (ages 11-12). Although point estimates of the cost differences were not statistically significant, when costs were considered along with the injury reduction in probabilistic sensitivity analysis, we found that in 78% of iterations in the public health care system perspective and 92% of the iterations in the private health care system, injuries and costs were lower, thus indicating that the no body checking policy is dominant.
There is a paucity of literature assessing the public health burden of injury from a health economic perspective.16,17,19 With the limited available health care resources and funding, economic analyses have gained recognition as an objective decision-making tool for policy makers across many disciplines of medicine. 4 Assessing injuries from an economic viewpoint is relatively new in the sport injury prevention and sport medicine fields. These studies are, however, beginning to gain traction.10-12,14,21 A previous evaluation comparing injury rates and health care costs in Pee Wee in Quebec (2007-2008) demonstrated significant projected health care cost savings ($213,280) associated with fewer injuries (1273 injuries) compared with Alberta (which permitted body checking) prior to the national body checking policy change. 11
A recent economic evaluation of another sport-related injury prevention intervention (neuromuscular training warm-up program in 13- to 18-year-old youth soccer) in Alberta demonstrated a significantly greater projected injury reduction of 4965 soccer-related injuries and health care (public and private) cost savings of $2.7 million annually. 12 The projected injury reduction and associated health care cost savings in Alberta were greater in the neuromuscular training program in 13- to 18-year-old soccer players compared with policy disallowing body checking in 11- to 12-year-old ice hockey players. One reason for this difference is that there are much higher participation rates in soccer in Alberta (ages 13-18) compared with participation rates for 11- to 12-year-old ice hockey players. Despite similar incremental injury rates between the control and training groups in 13- to 18-year-old soccer players (−1.27, 95% CI [−2.2 to −0.22]) injuries/1000 player-hours) and the body-checking policy change in 11- to 12-year-old ice hockey players (−2.21, 95% CI [−3.12 to −1.31]) injuries/1000 player-hours], there are 9880 Pee Wee players compared with 58,000 soccer players. 12 The consequence of a body-checking policy affected fewer players in hockey and so the projected cost savings and annual injuries saved was expected to be smaller. In addition, more than 50% of injuries in Pee Wee ice hockey players were concussions in both the body-checking and non–body checking cohorts. In soccer, the proportion of injuries that were concussions was less than 10%. This is important in that the health care costs associated with concussion are considerably lower compared with other more prevalent injury types in soccer (eg, anterior cruciate ligament injuries requiring surgical intervention and injuries requiring hospitalization). 12 In this hockey study, there were no reported surgeries or hospitalizations.
Limitations to our study related to dropout, missing exposure hours, and injury rates were previously addressed and do not suggest any systematic bias. 3 While access to study therapists and physicians, standardized follow-up, and return-to-play guidelines may have influenced health care utilization practices, the direction of this influence is unknown. It is possible that with increased awareness of clinicians treating youth concussion after the 4th International Consensus on Concussion in Sport published between the 2 cohort years may have influenced a more conservative approach to return to play after the policy change disallowing body checking in Pee Wee in 2013. 14 Our analysis controlled for game time exposure and team clustering, but we did not control for potential differences in risk factors for injury (eg, year of play, previous injury or concussion, player size, position, and level of play). As described in the Methods section, we used conservative assumptions surrounding health care resource use for the few injury cases that had missing details. In addition, we did not assess costs related to productivity loss for players and parents or guardians due to reduced working capacity (which is a particularly important consideration for concussion injuries) since they did not fall within the defined scope for our analysis. As these costs account for approximately 46% of the total costs associated with injuries in Canada, 20 our results likely underestimate the full economic impact of body checking in youth ice hockey by a substantial margin. Concern has been raised about the serious, long-term health consequences of concussions. 13 However, the time horizon of our study was limited to 1 season of play, and thus potential long-term impact of these injuries or the related implications for health care utilization and quality of life was not captured.
Conclusion
Hockey Canada’s decision to disallow body checking was effective in reducing the rate of injury in Pee Wee ice hockey players, which at the time was estimated to prevent 770 injuries a year in Alberta alone when projected on a provincial basis. Furthermore, although the point estimates of cost differences were not statistically significant, the sensitivity analysis found that the probability of the policy disallowing body checking being associated with both lower costs and a reduction in injuries was between 78% and 92% depending on the cost perspective. From an injury prevention and economic standpoint, these findings support disallowing body checking in 11- and 12-year-old ice hockey leagues.
Footnotes
The following authors declared potential conflicts of interest: A.M.B., L.P.-D., B.E.H., and C.A.E. have received grants from Canadian Institutes of Health Research (CIHR) and Alberta Innovates Health Solutions. A.M.B. has grants pending from National Football League Safety Advisory Board. D.A.M. has received hospitality payments from Illumina and ISPOR. D.A.M. was supported by the Arthur J. E. Child Chair in Rheumatology Research, a Canada Research Chair, Health Systems and Services Research (2008-18).
This study was supported by a grant from the Collaborative Research and Innovation Opportunities program from Alberta Innovates (grant notification No. 20130178). This study was also supported by the CIHR (No. 293332), Alberta Children’s Hospital Research Institute and Hotchkiss Brain Institute. The University of Calgary Sport Injury Prevention Research Centre is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee. Ethics approval was received from the University of Calgary Conjoint Health Research Ethics Board (ID#20252 and REB14-0348).