
Abstract
Background:
Tanimilast is a novel phosphodiesterase-4 inhibitor under clinical development for the maintenance therapy of asthma and chronic obstructive pulmonary disease (COPD). Since tanimilast is inhaled, it is important to evaluate lung deposition as part of its clinical development. The current study, therefore, used functional respiratory imaging, a validated, noninvasive quantification imaging methodology, to evaluate the lung deposition of tanimilast in patients with asthma or COPD.
Methods:
This retrospective study used data from 12 patients with asthma and 12 patients with COPD, primarily selected based on disease severity. Patients with COPD had chronic bronchitis, with minimal high-resolution computerized tomography evidence of emphysema. Total intrathoracic, central, distal, peripheral, and extrathoracic deposition of tanimilast 400 µg and 800 µg was evaluated using three inhalation profiles—inhalation durations of 1, 2, and 3 seconds, with associated peak flows of 100, 60, and 45 L/min, respectively.
Results:
Intrathoracic deposition as a percentage of the delivered dose was similar in asthma and COPD, with mean ± SD varying between 34.6 ± 8.5% and 44.9 ± 5.9%, increasing slightly with increasing inhalation duration (i.e., from 1 to 3 seconds), whereas extrathoracic deposition decreased progressively. Central deposition was low (<5%) regardless of inhalation duration (2.7 ± 0.9% to 4.4 ± 1.6%). Distal deposition was similar with the two tanimilast doses and although not impacted by inhalation duration was slightly higher in COPD than asthma. Peripheral deposition increased with increasing inhalation duration (e.g., in asthma for tanimilast 400 µg, from 14.1 ± 3.6% for a duration of 1 second to 19.9 ± 4.0% for a duration of 3 seconds) and was higher in asthma than in COPD.
Conclusions:
Tanimilast effectively reached all levels of the airway in patients with asthma or COPD. Peripheral deposition was enhanced by lower inspiratory flows (i.e., longer inhalation durations), suggesting that specific inhalation strategies may have the potential to improve therapeutic outcomes in obstructive lung diseases.
Introduction
Tanimilast is a novel phosphodiesterase-4 (PDE4) inhibitor that is under clinical development for the maintenance therapy of asthma and chronic obstructive pulmonary disease (COPD). The only currently available PDE4 inhibitor is roflumilast, which is approved for oral administration in a specific subgroup of patients with COPD (chronic bronchitis and a history of frequent exacerbations). 1 However, the oral administration of roflumilast is associated with a high incidence of systemic adverse events, resulting in high rates of treatment discontinuation,2–7 limiting acceptability and use. Ensifentrine is a dual PDE3 and PDE4 inhibitor, 8 approved for the maintenance treatment of COPD. 9 Although given by inhalation, ensifentrine is administered via a jet nebulizer connected to an air compressor, adding complexity to its use.
In contrast to roflumilast and ensifentrine, tanimilast is inhaled using a dry-powder inhaler (DPI; the proprietary NEXThaler) and has low systemic exposure. 10 This allows tanimilast to reach therapeutic concentration in the target organ, the lung, yet reduces exposure in the systemic circulation, thus limiting systemic adverse effects.11–13 In clinical studies, tanimilast inhaled twice daily demonstrated lung-targeted anti-inflammatory effects in patients with COPD who had a chronic bronchitis phenotype,14–16 and in those with atopic asthma in terms of the physiological response to an antigen challenge to a nonsignificant reduction versus placebo in sputum eosinophil counts. 17
Since tanimilast is inhaled, it is important to evaluate lung deposition as part of its clinical development. The current study therefore used functional respiratory imaging (FRI) to evaluate lung deposition of tanimilast in patients with asthma or COPD. FRI is a validated, noninvasive quantification imaging methodology 18 that provides the detailed measurement, visualization, and evaluation of lungs and airways, both regionally and in totality. FRI uses low-dose, high-resolution computerized tomography (HRCT) and computational fluid dynamics (CFD) to model airflow in the airways and calculate aerosol deposition patterns within the lung.
Materials and Methods
Study design
FRI is based on four components: (1) patient-specific three-dimensional (3D) airway geometry modeling; (2) inhaler and particle characteristics; (3) inhalation profiles generated from actual patient profiles; and (4) CFD simulations to model lung deposition of inhaled aerosol. This retrospective study used data from 12 patients with physician-diagnosed asthma and 12 with physician-diagnosed COPD, primarily selected based on disease severity from the FLUIDDA database, which includes data from multiple clinical trials (the inclusion and exclusion criteria applied are listed in Supplementary Data). In all cases, the diagnosis was established by physicians based on standard criteria for each of the diseases. Patients with COPD had chronic bronchitis to minimal HRCT evidence of emphysema (<10% voxels <950 Hounsfield units on the inspiratory scan). Lung deposition was evaluated based on airway geometry, aerosol characteristics, and in vitro breathing patterns using three inhalation profiles (inhalation durations of 1, 2, and 3 seconds) and associated peak flows of 100, 60, and 45 L/min, respectively.
An automated algorithm was used to segment the HRCT scans of the lungs into airways and parenchyma up to the point where no distinction could be made between the intraluminal and alveolar air. The segmented airways were then manually reviewed, and the reconstructed 3D lung lobes and airway tree model were smoothed and trimmed perpendicular to the centerline at the end of each terminal bronchus. 19 Any remaining artifacts due to noise in the HRCT images were removed manually.
The airways were divided into two groups: extrathoracic (the mouth and upper airways) and intrathoracic (the trachea and the remainder of the bronchial tree). The intrathoracic airways were further divided into three parts: central (trachea and mainstem bronchi), distal (all airways visible in the HRCT scan beyond the mainstem bronchi, i.e., diameter >2 mm), and peripheral (diameter ≤2 mm). Since peripheral airways cannot be resolved on HRCT scan, the total peripheral dose of aerosol was equated to that exiting the distal airways.
Tanimilast DPI particle characteristics (aerosol particle size distribution provided as mass deposition from the Next Generation Impactor stages and fine particle fraction) at doses of 400 and 800 µg (each in 20 mg of powder) were provided by Chiesi Farmaceutici SpA from the first batch fully representative of the to-be-marketed product to the particle distribution profiles at each flow generated from Next Generation Impactor analyses—the particle characteristics of tanimilast are flow-independent (Table 1). Patient-unique inhalation flow profiles were then generated and applied in CFD simulation of aerosols and airflow dynamics as follows: (1) An idealized flow profile was adopted; (2) for each patient, this profile was scaled to match the patient’s actual inhaled volume, derived from inspiratory and expiratory HRCT scans, and produce three inhalation durations, fixed at 1, 2, and 3 seconds. This resulted in three profiles per patient, with inhalation durations of 1, 2, and 3 seconds, each reflecting the same inhaled volume but differing in peak and mean flow, from which local flow resistance and aerosol deposition patterns were then calculated. 20
Particle Characteristics of Tanimilast 400 and 800 µg
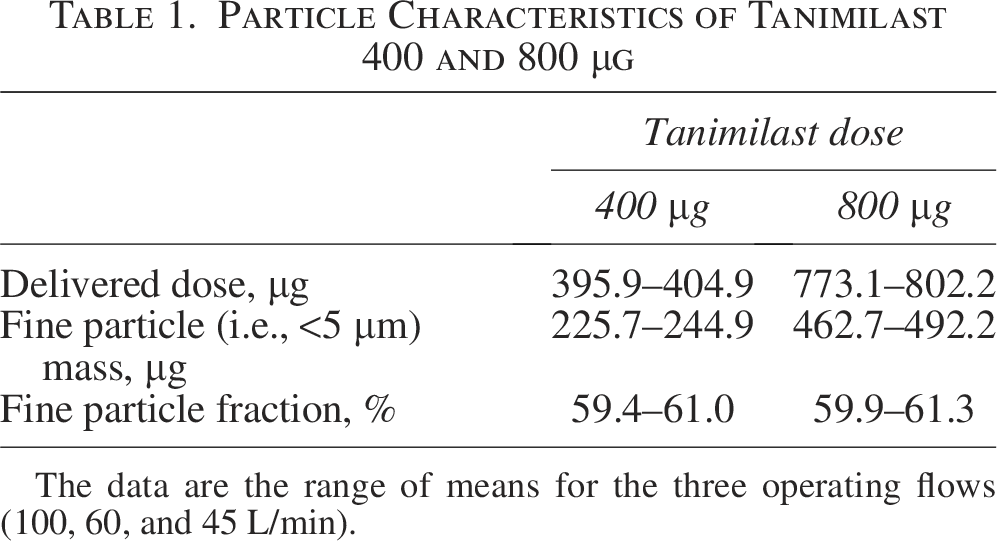
The data are the range of means for the three operating flows (100, 60, and 45 L/min).
All data were acquired retrospectively, with informed consent previously obtained from each patient, and ethical approval was granted by the Ethics Committee of the University Hospital in Antwerp, Belgium. The study was performed in accordance with the Declaration of Helsinki and Good Clinical Practice.
Outcomes
The primary objective was to determine the deposition characteristics of two inhaled doses of tanimilast DPI (400 and 800 µg) using three inhalation flow profiles in patients with asthma or COPD by means of FRI. The primary outcome parameters were total intrathoracic deposition (i.e., central plus distal plus peripheral) as a percentage of the delivered dose, and the absolute intrathoracic deposition. Central, distal, and peripheral deposition, and the distal to peripheral deposition ratio were calculated. Extrathoracic deposition (percentage and absolute) was also quantified. The results were analyzed separately for each patient population group.
Sample size and statistical methods
No formal sample size calculation was performed since this was an exploratory study. All statistical analyses were conducted using R version 3.2.5 or higher (The R Foundation for Statistical Computing, Vienna, Austria), with data analyzed descriptively.
Results
The characteristics of the included patients are presented in Table 2.
Patient Characteristics
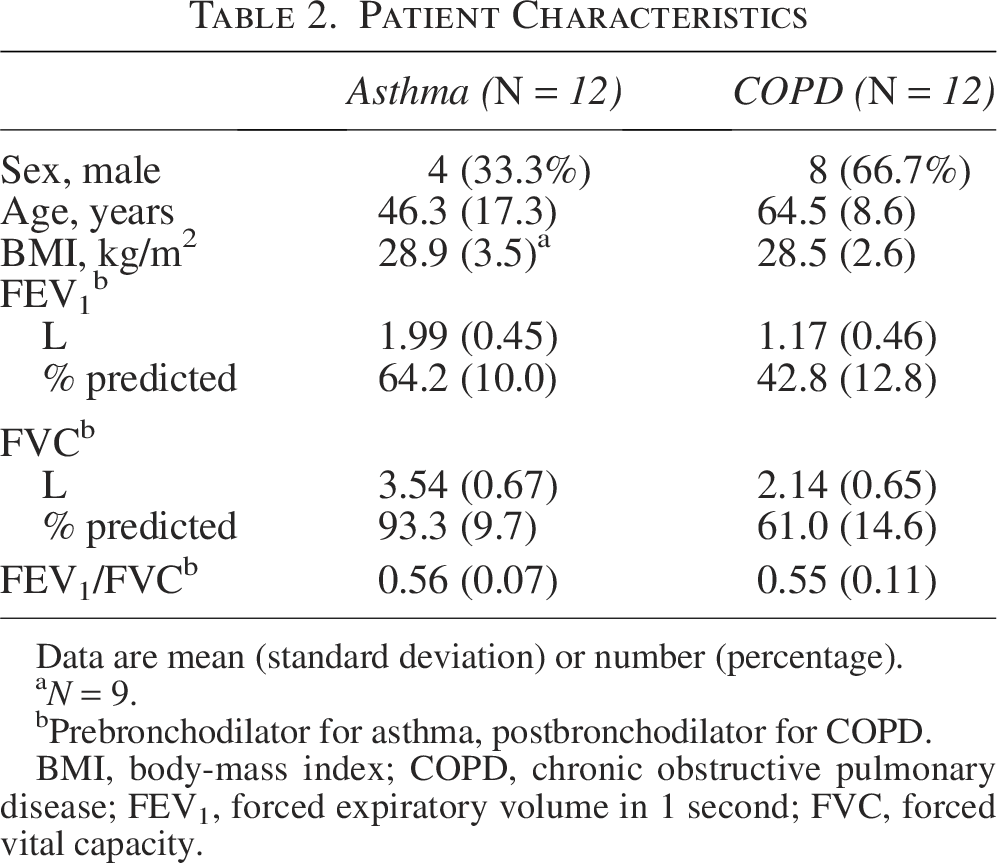
Data are mean (standard deviation) or number (percentage).
N = 9.
Prebronchodilator for asthma, postbronchodilator for COPD.
BMI, body-mass index; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
Intrathoracic deposition (as a percentage of the delivered dose) was similar in both patient groups and for the two tanimilast doses (Fig. 1). For example, for tanimilast 400 µg, the mean ± standard deviation varied between 36.8 ± 6.1% and 44.5 ± 5.4% in patients with asthma and between 35.2 ± 7.6% and 40.0 ± 7.6% in patients with COPD. As would be expected, absolute deposition was higher for tanimilast 800 µg than for 400 µg (Supplementary Fig. S1). In both groups, intrathoracic deposition increased slightly with increasing inhalation duration (i.e., from 1 to 3 seconds, associated with peak flows decreasing from 100 to 45 L/min). In a post hoc analysis using an analysis of variance (ANOVA) for repeated measures including intrathoracic deposition as an independent variable and inhalation times as dependent variables, the differences across inhalation time were statistically significant (p < 0.001 for patients with asthma; p = 0.002 for patients with COPD). Extrathoracic deposition (i.e., in the mouth and upper airways) decreased progressively with increasing inhalation duration (Supplementary Figs. S2 and Figs. S3).
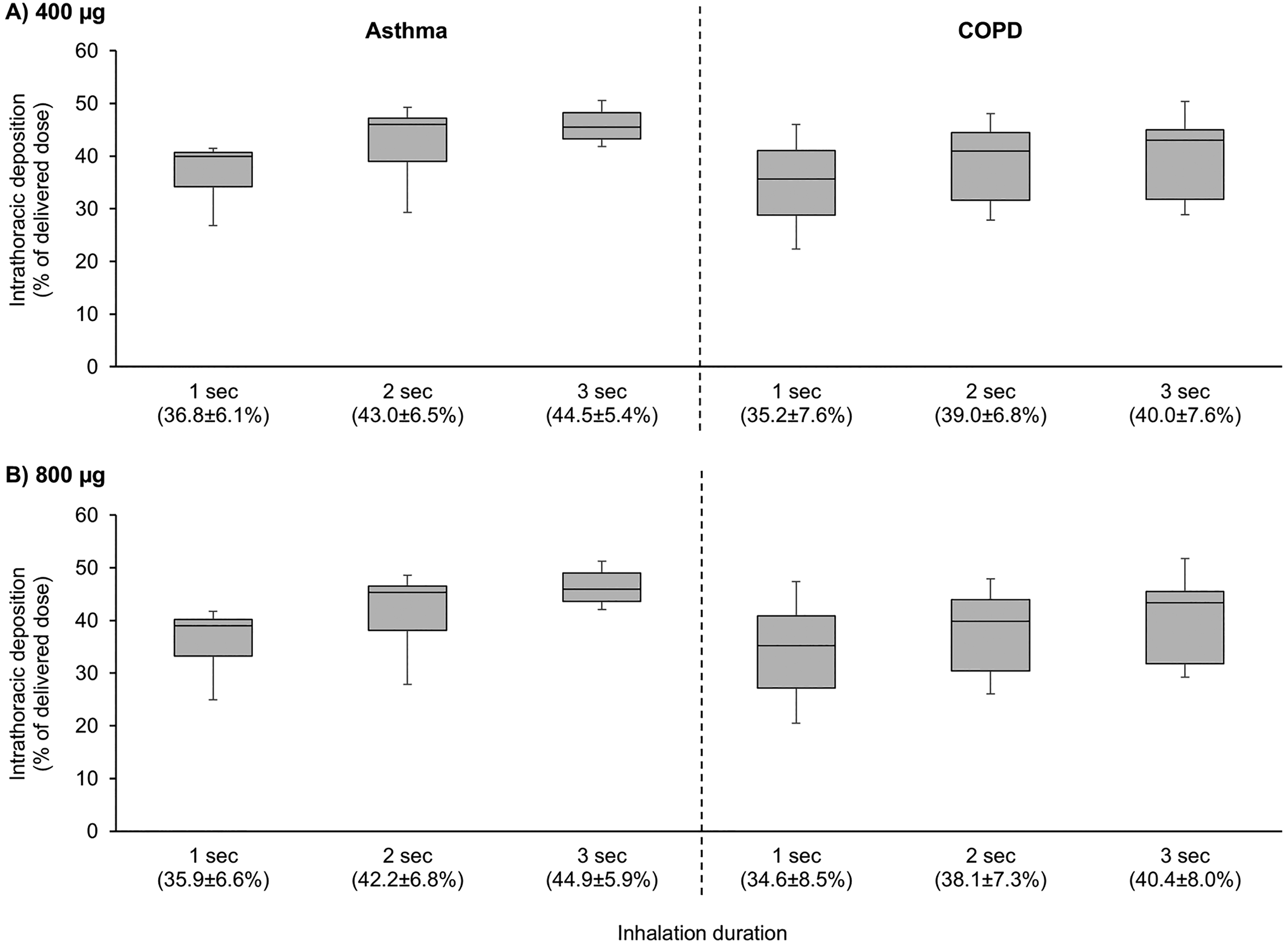
Intrathoracic deposition as a percentage of the delivered dose for three inhalation durations for
Central deposition (i.e., in the trachea and main bronchus) was low in both patient groups and was not influenced by inhalation duration, with mean deposition <5% of the delivered dose (Figs. 2 and 3, to absolute deposition, as shown in Supplementary Figs. S4 and Figs. S5). Distal deposition as a percentage of the delivered dose was slightly higher in patients with COPD (22.1 ± 6.5% to 24.0 ± 6.0%) than with asthma (19.8 ± 4.6% to 22.8 ± 5.4%), was similar to the two tanimilast doses, and was not impacted by inhalation duration (Figs. 2 and 3). In contrast, peripheral deposition increased with increasing inhalation duration (e.g., in asthma for tanimilast 400 µg, from 14.1 ± 3.6% for an inhalation duration of 1 second to 19.9 ± 4.0% for an inhalation duration of 3 seconds), with the trend statistically significant in a similar post hoc ANOVA analysis to that conducted for intrathoracic deposition (p < 0.001 in both asthma and COPD). Peripheral deposition was slightly higher in patients with asthma (12.9 ± 3.4% to 19.9 ± 4.0%) than with COPD (8.0 ± 1.9% to 12.9 ± 2.7%). As a consequence, the distal to peripheral ratio decreased with increasing inhalation duration in both diseases, especially in patients with COPD (Fig. 4). Example CFD scintigraphy-like images constructed from the CFD simulation results for two patients (one with asthma and one with COPD) at the three inhalation durations are shown in Supplementary Figure S6.
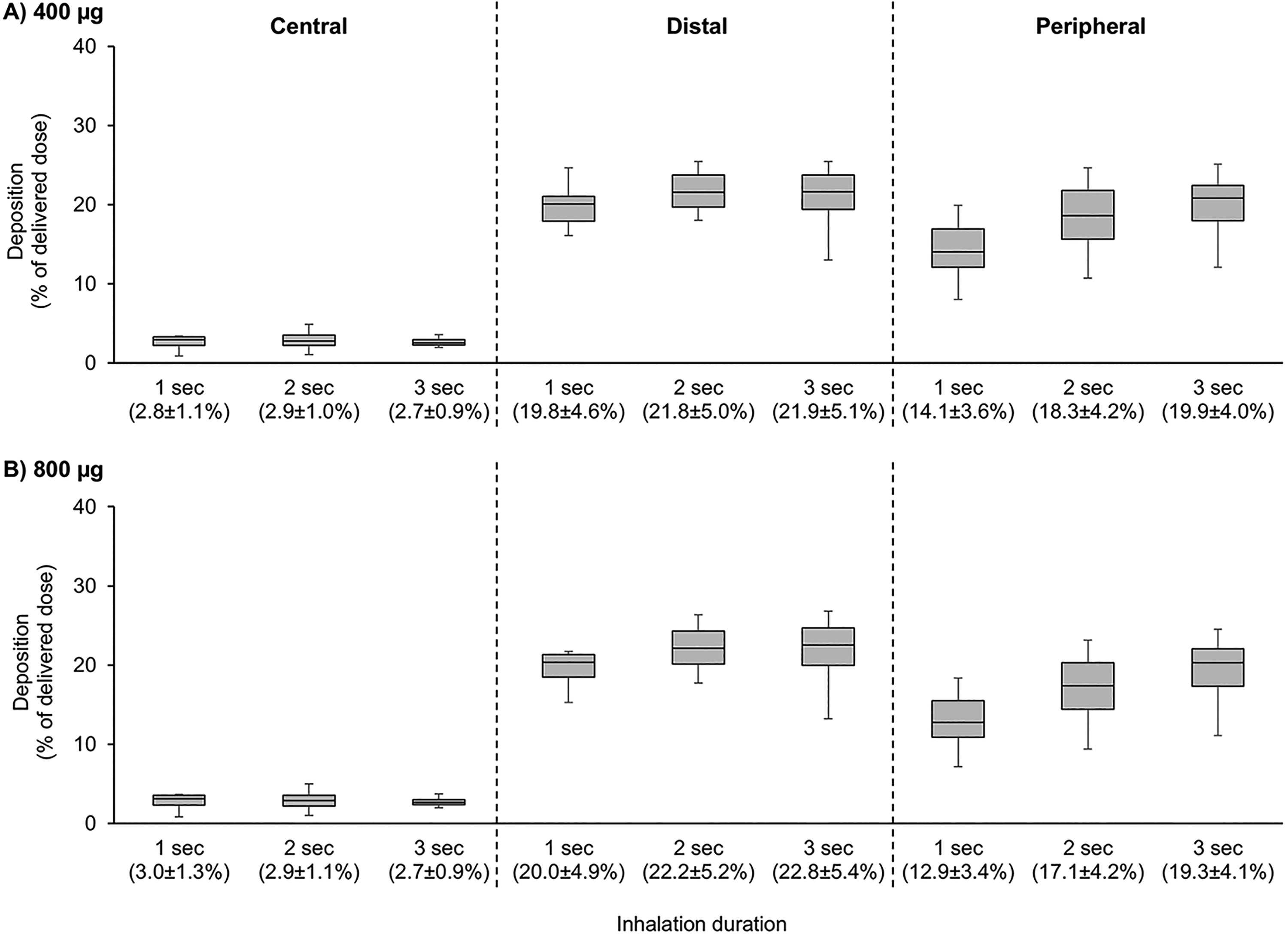
Central, distal, and peripheral deposition in patients with asthma as a percentage of the delivered dose for three inhalation durations for
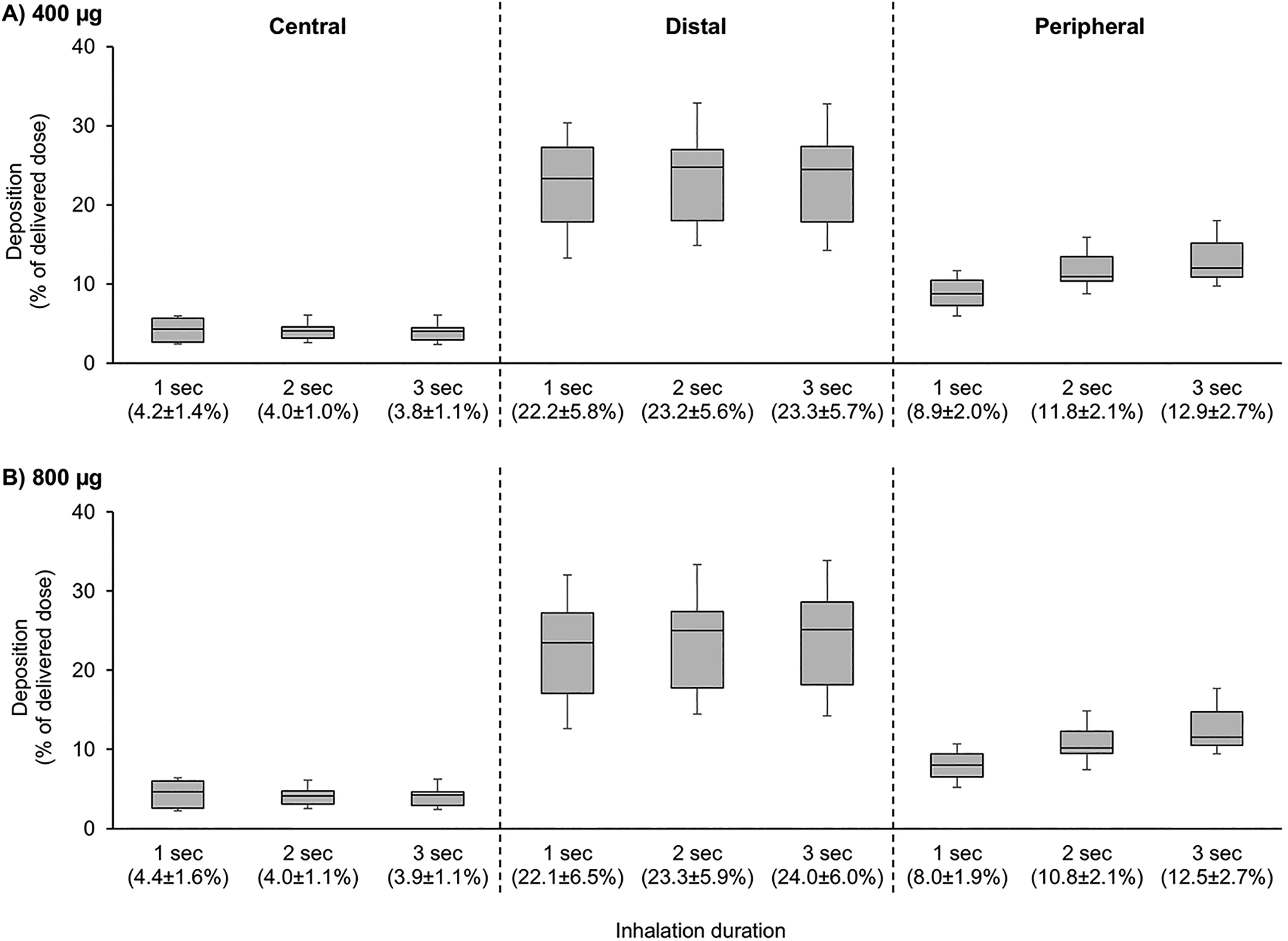
Central, distal, and peripheral deposition in patients with COPD as a percentage of the delivered dose for three inhalation durations for
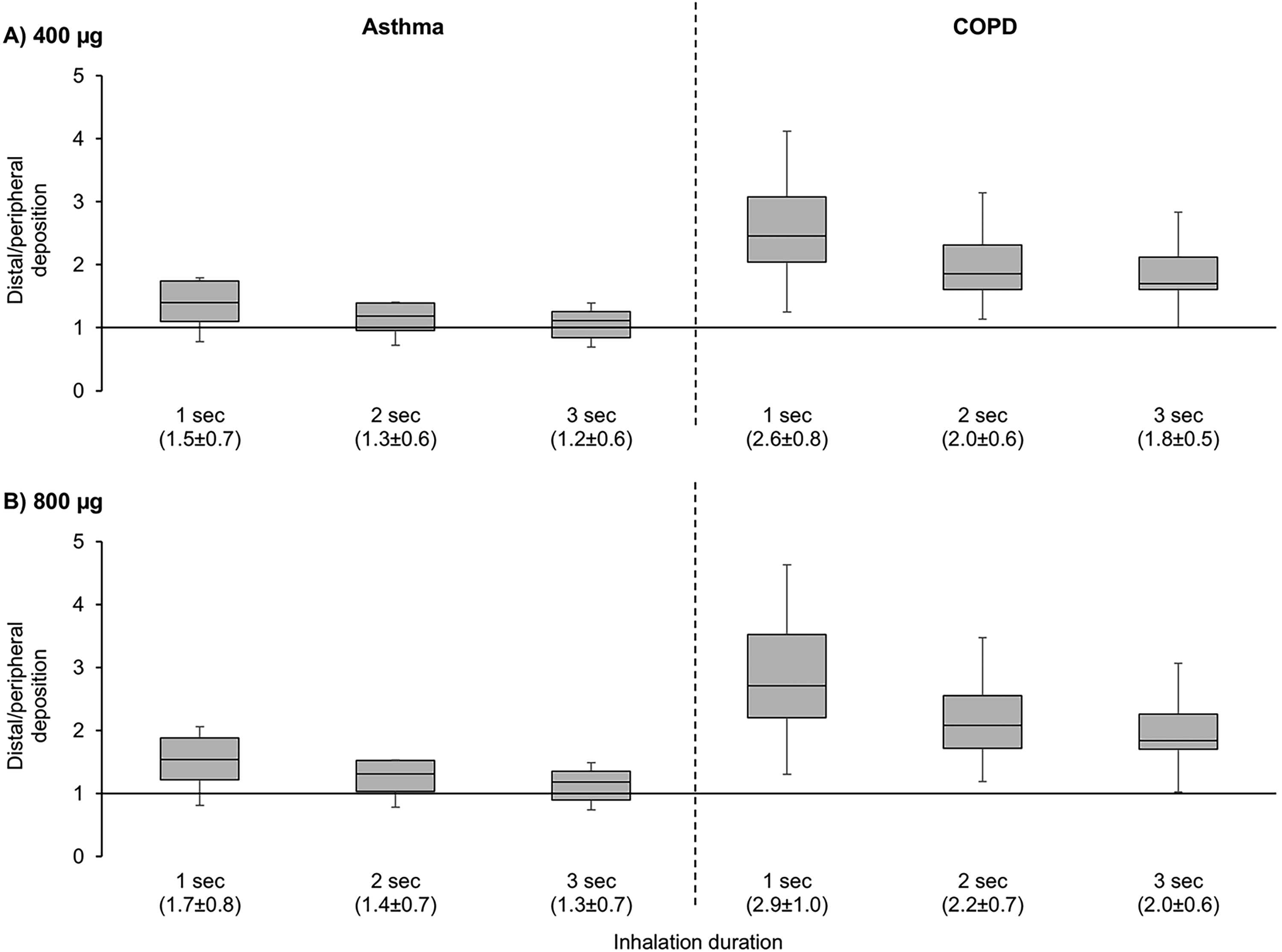
Distal to peripheral deposition ratios for three inhalation durations for
Discussion
Overall intrathoracic deposition following the inhalation of tanimilast delivered using the NEXThaler DPI had a similar distribution in the two groups of patients and (as a percentage of the delivered dose) was similar following the inhalation of the 400 and 800 µg doses. Importantly, however, intrathoracic deposition increased slightly with increasing inhalation duration (from 1 to 3 seconds, associated with peak flows decreasing from 100 to 45 L/min) and with corresponding decreases in extrathoracic deposition. These increases in intrathoracic deposition, thus, occurred because more aerosol made it past the upper airways as the flow decreased. This is not unexpected since high inhalation flows in the upper airways predispose to the impaction of aerosol particles on the back of the throat due to inertia, while lower flows allow particles to more easily pass the vocal cords and into the lungs. 21
Central airway deposition of tanimilast was low in both groups of patients (mean <5%) and was not impacted by inhalation duration, and distal deposition was also unaffected by inhalation duration. The increasing intrathoracic deposition with increasing inhalation duration was primarily due to increasing peripheral deposition, as demonstrated by the decreasing distal-to-peripheral deposition ratios in both groups of patients. Although aerosol flow dynamics in the lung periphery were not explicitly modeled, these findings reflect what likely takes place in an actual lung since gas transport in the very distal airspaces takes place predominately by diffusion rather than convection. 22 A longer inspiratory duration means that tanimilast aerosol particles have a longer residence time in the lung periphery and, thus, have more time to diffuse to, and collect on, the epithelial surfaces. Furthermore, lower inspiratory airflow (hence, air velocity) causes less aerosol impaction on airway walls, thereby allowing deeper aerosol penetration.
Distal deposition was higher than peripheral deposition both in patients with asthma and in those with COPD. However, the relative patterns of distal to peripheral deposition differed between the two groups. Specifically, distal deposition was higher in patients with COPD than asthma, whereas peripheral deposition was higher in patients with asthma than COPD. The characteristics of the recruited patients may explain this difference: patients with COPD had a predominantly chronic bronchitis phenotype (with <10% emphysema), making it likely that their distal airways were significantly narrowed, due to excessive airway mucus and smooth muscle hypertrophy. 23 This would decrease the average distance between the tanimilast particles and the airway wall as the inhaled aerosol flowed through the distal airways, increasing the rate of impaction on the walls. In addition, the destruction of the smallest airways is known to occur in patients with COPD even prior to the overt development of emphysematous destruction.24,25 This would increase the resistance of the peripheral airways in patients with COPD, 23 thereby increasing the barrier to progression of aerosol into the lung periphery. Of course, asthma is also associated with increased mucous production and smooth muscle hypertrophy,26,27 although airway narrowing in this group may not have been as severe as in the COPD group. Indeed, the pulmonary function evaluations indicate less severe obstruction in the recruited patients with asthma. Differences in the two populations could also perhaps explain why there was a greater variability in the data in patients with COPD than asthma (as indicated by the width of the interquartile ranges). COPD is inherently more variable between patients, and the recruited population was, therefore, less homogeneous than the asthma population. Furthermore, the patients with COPD were, on average, older than the patients with asthma, potentially also increasing the heterogeneity (and, thus, variability).
Another potential explanation for the differences in distal deposition in asthma versus COPD relates to the airway-parenchymal interdependence, which is so crucial for maintaining airway patency in a normal lung. This interdependence was likely still intact during inspiration in patients with asthma because flow limitation is a predominantly expiratory impairment in this disease. 28 In contrast, patients with COPD typically have reduced airway-parenchymal interdependence, due to emphysematous tissue destruction, and as a result, may have experienced sufficient decrease in airway patency to increase the distal impaction of aerosol. It is also possible we may have underestimated the degree of emphysema in some of these patients.
The main limitation of the study is the retrospective, in silico design using computational modeling to simulate patients’ inhalation of tanimilast, and thus we can draw no conclusions on the clinical implications (either efficacy or safety) of the lung deposition profiles. Furthermore, while the inhaled particles remaining in the visible airways were considered as the exhaled dose, it was assumed that the portion exiting distal airways was entirely deposited in the peripheral airways, rather than being exhaled,29,30 although this assumption is supported by the results from a previous study using different molecules.31,32 Finally, the analyses were not blinded—although given they used retrospectively-collected data, we do not believe that this would have a substantial impact on the results.
Conclusion
Taken together, the data from this study provide evidence that following inhalation via DPI, tanimilast is able to penetrate all levels of the airway in patients with asthma or COPD. Peripheral deposition was higher in patients with asthma than in those with COPD, which may reflect differences in small airway caliber between the two groups. However, in both diseases, peripheral airways deposition was enhanced by lower inspiratory flows (i.e., longer inhalation durations). This suggests that specific inhalation strategies may have the potential to improve therapeutic outcomes in obstructive lung diseases.
Authors’ Contributions
N.M.T.: Methodology, formal analysis, investigation, visualization, and writing—review and editing. R.O.: Methodology, supervision, visualization, and writing—review and editing. D.S.: Formal analysis, supervision, visualization, and writing—review and editing. L.C.: Methodology, supervision, visualization, and writing—review and editing. J.H.T.B.: Visualization and writing—review and editing. D.G.: Supervision, visualization, and writing—review and editing. J.D.B.: Methodology, investigation, visualization, and writing—review and editing. H.S.: Methodology, investigation, visualization, and writing—review and editing. G.S.: Conceptualization, supervision, visualization, and writing—review and editing.
Footnotes
Acknowledgment
Writing support was provided by David Young from Young Medical Communications and Consulting Ltd. This support was funded by Chiesi Farmaceutici SpA.
Author Disclosure Statement
N.M.T., J.D.B., and H.S. are employees of FLUIDDA, the company that owns and implements FRI and that was engaged by Chiesi to conduct the analyses referred to in the article. R.O., D.S., L.C., D.G., and G.S. are employees of Chiesi. J.H.T.B. declares receiving consulting fees from Chiesi, payments for expert testimony from Stamoulis & Weinblatt, NY, and stock or stock options from Respiratory Sciences, Inc. and Oscillavent, Inc., all outside the scope of the current article.
Funding Information
There is no grant number for the funding.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.