
Abstract
Background
Minimally invasive hallux valgus reconstruction is a technique that has been undergoing refinements since its inception. The fourth-generation technique differentiates itself with a transverse metatarsal osteotomy. The location of this osteotomy is a key consideration. It is desirable for this osteotomy to be as distal as possible while remaining extra-capsular and preserving the blood supply to the capital fragment. Limited guidance exists for identifying this position intraoperatively. This cadaveric investigation aims to identify an extra-capsular location for a transverse metatarsal osteotomy for fourth-generation hallux valgus reconstruction and assess the effects of this osteotomy on the blood supply to the capital fragment.
Methods
Ten clinical-grade cadaveric specimens were injected with radiopaque contrast to define the first metatarsophalangeal (MTP) joint capsule. Measurements from the metatarsal head and the sesamoids to the proximal edge of the capsule were recorded from the radiographic images. Using fluoroscopic guidance, a transverse minimally invasive osteotomy was performed near the capsule border. Anatomic dissections assessed capsular integrity and vascular supply to the distal first metatarsal.
Results
Radiographic measurements showed that the distance between the articular surface and proximal edge of the capsule was 27.3 mm. Mean distance from the articular surface of the metatarsal head to the osteotomy was similar at 27.3 mm. Distances from the medial and lateral sesamoids to the proximal edge of the capsule were 3.8 mm and 3.9 mm, respectively. An osteotomy at 29.5 mm from the articular surface would be extra-articular in 80% of specimens. Dissections confirmed extra-capsular osteotomy placement and preserved vascular integrity in all specimens.
Conclusion
Insertion of the first MTP joint capsule varies among specimens. A transverse osteotomy performed at 29.5 mm from the articular surface achieves an extra-capsular position in 80% of our specimens without compromising vascular supply to the capital fragment. These values provide reproducible intraoperative guidance.
Level of Evidence
(5) Clinical Research
Introduction
“The current fourth-generation technique features a transverse distal metatarsal osteotomy that is performed in an extra-articular fashion.”
Minimally invasive hallux valgus reconstruction is a technique that has been undergoing refinements since its first iterations in the 1980s by Wilson 1 and Bösch et al. 2 The current fourth-generation technique features a transverse distal metatarsal osteotomy that is performed in an extra-articular fashion.3,4 Unlike the third-generation minimally invasive chevron osteotomy,5,6 the transverse osteotomy allows for rotation of the metatarsal head, which may play an important role in deformity correction.4,7 Favorable short-term outcomes following fourth-generation hallux valgus reconstruction with improved patient-reported outcomes have been reported. 3 Although complications such as delayed union, non-union, and avascular necrosis are uncommon, 8 these recognized risks highlight the importance of a detailed understanding of the vascular anatomy and capsular boundaries to maximize favorable outcomes.
The location of the osteotomy of the metatarsal is a key consideration. It is generally accepted that the transverse osteotomy should be performed in an extra-capsular fashion.3,9 Theoretically, staying extra-capsular may avoid hemarthrosis and intra-articular debris, and thus result in less stiffness, pain, and better final range of motion. 10 At the same time, an important consideration is that stability of the osteotomy fixation with screws, which can be compromised if the lateral cortex of the first metatarsal is not engaged with the proximal screw. Placing the osteotomy too proximal will make this challenging or impossible.
In a previous cadaveric investigation, Chin et al 10 identified the boundaries of the first metatarsophalangeal (MTP) joint capsule and gave recommendations for the location of a third-generation minimally invasive (MIS) chevron osteotomy. To stay extra-capsular, they recommend that surgeons should keep the apex of the chevron 13 mm from the center of the metatarsal head, and the dorsal and plantar limbs of the osteotomy should extend 18 mm and 25 mm, respectively. 10 More recently, Carvalho et al 11 assessed the vascular supply to the metatarsal head following an MIS chevron osteotomy. In order to maintain the vascular integrity to the metatarsal head, they recommended maintaining the dorsal and plantar limbs of the osteotomy at a median distance of 25.6 mm and 23.9 mm, respectively, from the joint surface. Furthermore, they suggested avoiding penetration of the Shannon burr beyond 3.9 mm dorsolaterally or 4.0 mm plantarlaterally from the cortical bone exit. 11 Interestingly, the values Carvalho et al and Chin et al recommend are different, highlighting the potential significant anatomical variability between specimens and need for further investigation.
The proximal extent of the first MTP joint capsule as it pertains to the position of an extra-capsular transverse metatarsal osteotomy (fourth generation) has not been described. Furthermore, there is paucity of data regarding the effects of an osteotomy in this location on the blood supply to the capital fragment. Therefore, in this cadaveric investigation, we aimed to address this gap by quantifying the proximal extent of the first MTP joint capsule relative to the position of an extra-capsular transverse metatarsal osteotomy used for fourth-generation hallux valgus reconstruction. Furthermore, we aimed to assess the effect of this osteotomy on the main blood supply to the capital fragment.
Methods
Specimens
Ten human cadaveric specimens, spanning from mid-tibia to tip of the toes (5 left and 5 right), were utilized. These comprised of 6 male and 4 female specimens of Caucasian ethnicity, without signs of musculoskeletal abnormalities, or previous fracture, or surgery. The mean age of the specimens was 82.8 years (range: 72-99 years). Cadavers were prepared with the Clinical Grade Cadaver—Sandeski Technique and stored at 4°C. This study was approved by the research ethics board of our institution for cadaveric laboratory research.
Cannulation and Radiographic Imaging
To investigate the blood supply to the metatarsal head after dissection, the anterior and posterior tibial arteries were cannulated and perfused with liquid latex mixture to highlight the vasculature. Under fluoroscopic guidance, radiopaque contrast (Omnipaque, iohexol) was injected into the first MTP joint capsule. This allowed visualization of the boundaries of the joint capsule on x-ray. Next, based on the proximal boundary of the capsule, a fourth-generation transverse osteotomy was performed using a 2 × 20 mm Shannon burr (Stryker) and a high-torque, low-speed handpiece and constant irrigation (Stryker). This osteotomy was performed in a line perpendicular to the shaft of second metatarsal. The osteotomy was then manually displaced, ensuring that it is complete. Fluoroscopic control was utilized throughout the procedure. The direction of the x-ray beam was perpendicular to the axis of the first metatarsal (Figure 1). Calibrated x-ray images of the feet were analyzed on a Java-based image processing program (ImageJ—NIH), which allowed us to calculate the mean distances and standard deviations from the articular surface of metatarsal head to the osteotomy site (Figure 2).
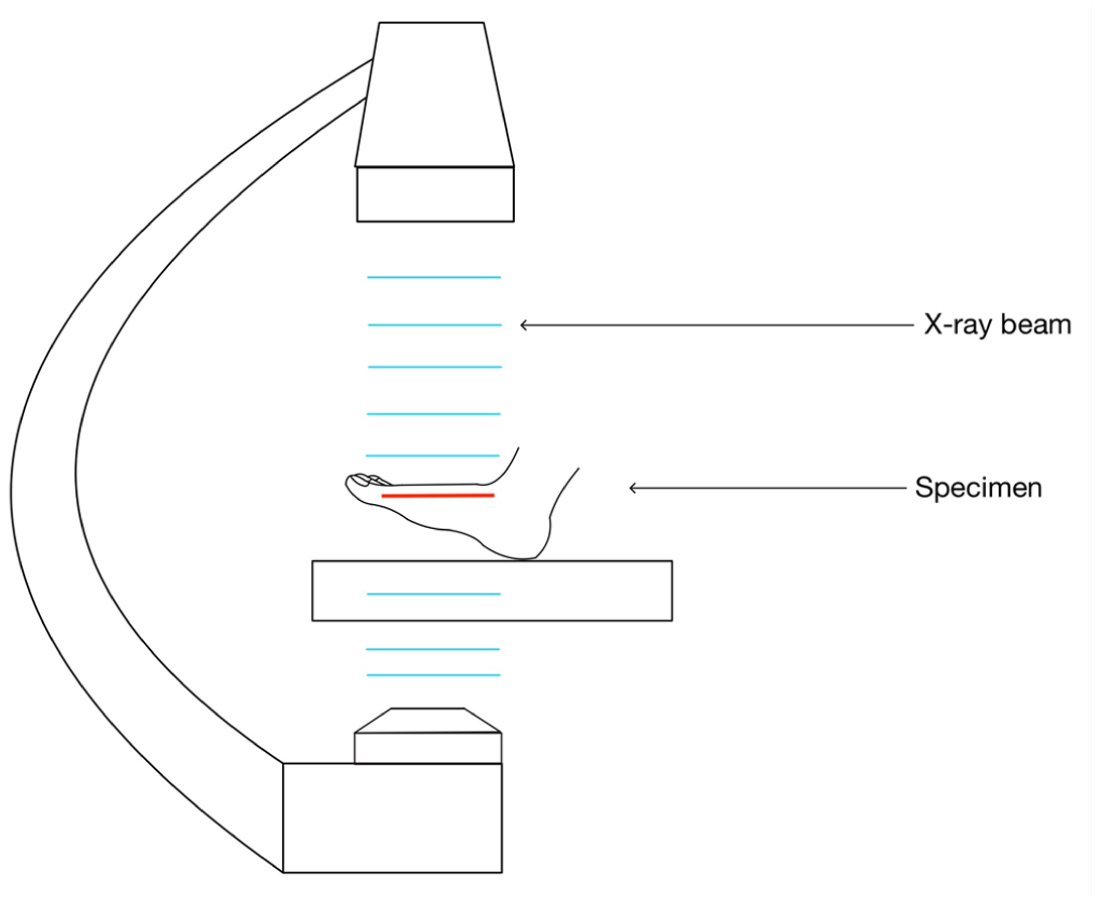
Fluoroscopic imaging technique showing specimen positioning and perpendicular x-ray beam alignment relative to the first metatarsal axis.

X-ray images taken from an anteroposterior view under fluoroscopy of the distal first metatarsal pre-injection (A) and post-injection of contrast (B), and after transverse osteotomy TO (C).
Dissection and Measurements
Following the procedure, a medial longitudinal approach to the first MTP was utilized to inspect for capsular damage and perform measurements (Figure 3). This was performed by an experienced fellowship-trained board-certified orthopaedic foot and ankle surgeon and an academic anatomist. The perfusion highlighted the vascular branches reaching the head of the first metatarsal. After the osteotomy procedure, the anatomical distribution of the perfused vessels was explored by anatomical dissection to map vascular networks concerning the operation. Two members of the research team performed measurements on the radiographic images.
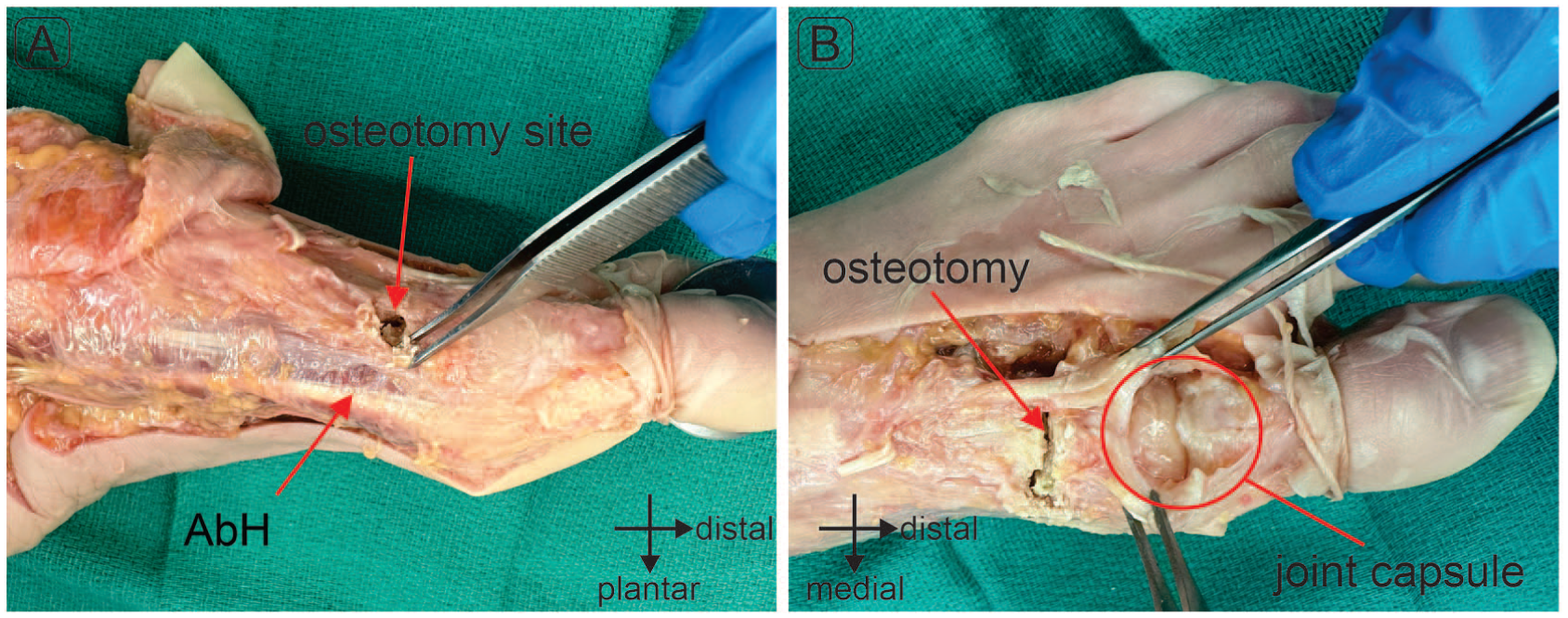
Exposure of the transverse osteotomy site (A) and intact joint capsule following the osteotomy (B).
Statistical Analysis
Descriptive analysis of the demographic and clinical variables was conducted. Inter-rater reliability between the 2 evaluator’s measurements was calculated using intraclass correlation coefficient (ICC, 2-way random, absolute agreement, single measure) and presented with the accompanying 95% confidence intervals.
Results
Average distances, standard deviations, and the ICC between the 2 observers are shown in Table 1. From the radiographic images, the average distance from the articular surface to the proximal edge of the capsule was 27.3 mm (median = 27.9 mm, IQR = 24.4-30.3) (Figure 4A). The distance from the medial and lateral sesamoids to the proximal edge was 3.8 mm (median = 3.7 mm, IQR = 2.8-4.9) and 3.9 mm (median = 3.9 mm, IQR = 3.3-5.1) (Figure 4B and C). The average distance of the articular surface to the osteotomy was 27.3 mm (median = 26.5 mm, IQR = 24.4-30.3), which was obtained from the radiographic image (Figure 4D).
Radiographic Measurements of Distances to Anatomic Landmarks Relative to the First MTP Joint Capsule.
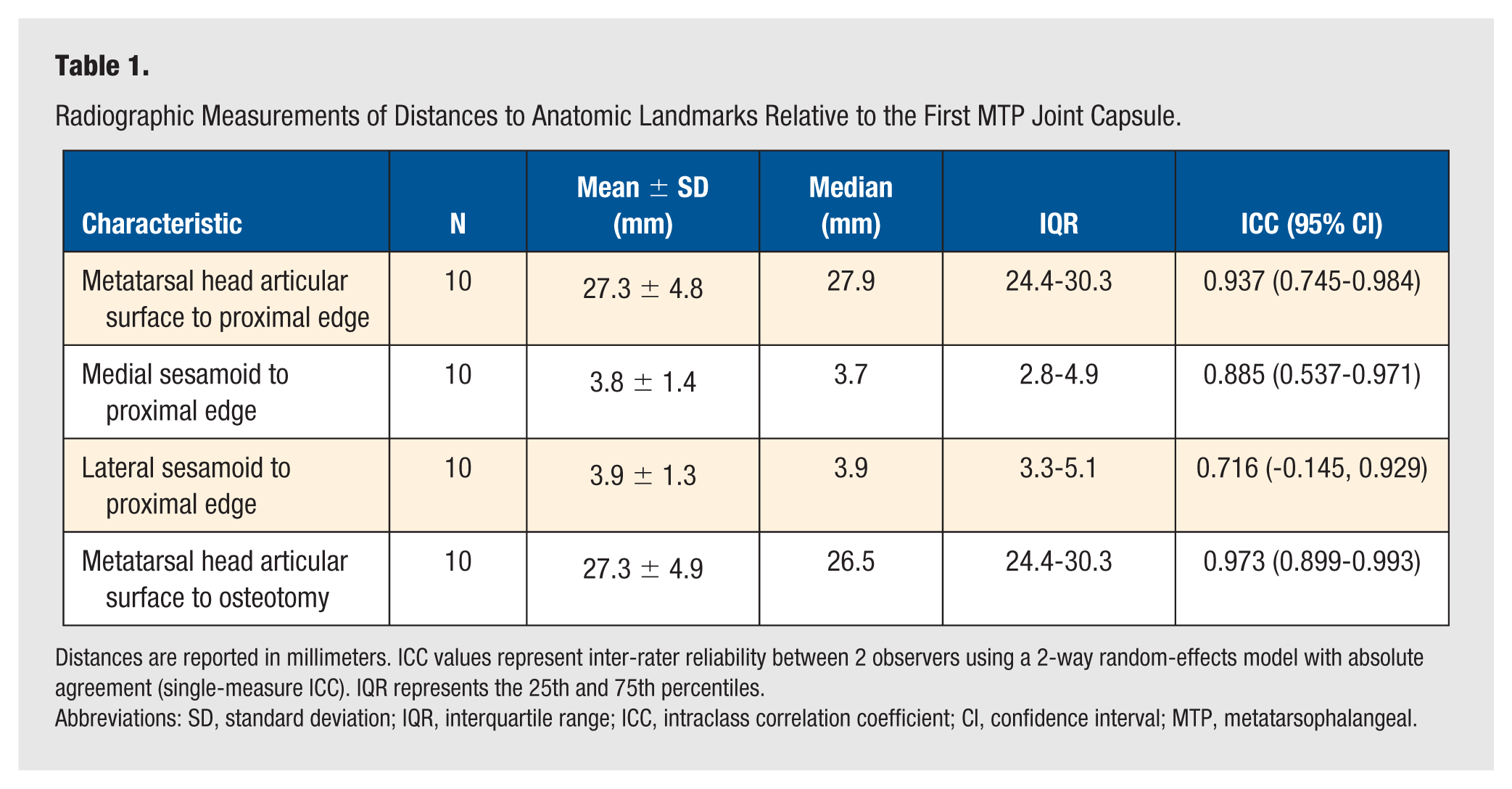
Distances are reported in millimeters. ICC values represent inter-rater reliability between 2 observers using a 2-way random-effects model with absolute agreement (single-measure ICC). IQR represents the 25th and 75th percentiles.
Abbreviations: SD, standard deviation; IQR, interquartile range; ICC, intraclass correlation coefficient; CI, confidence interval; MTP, metatarsophalangeal.
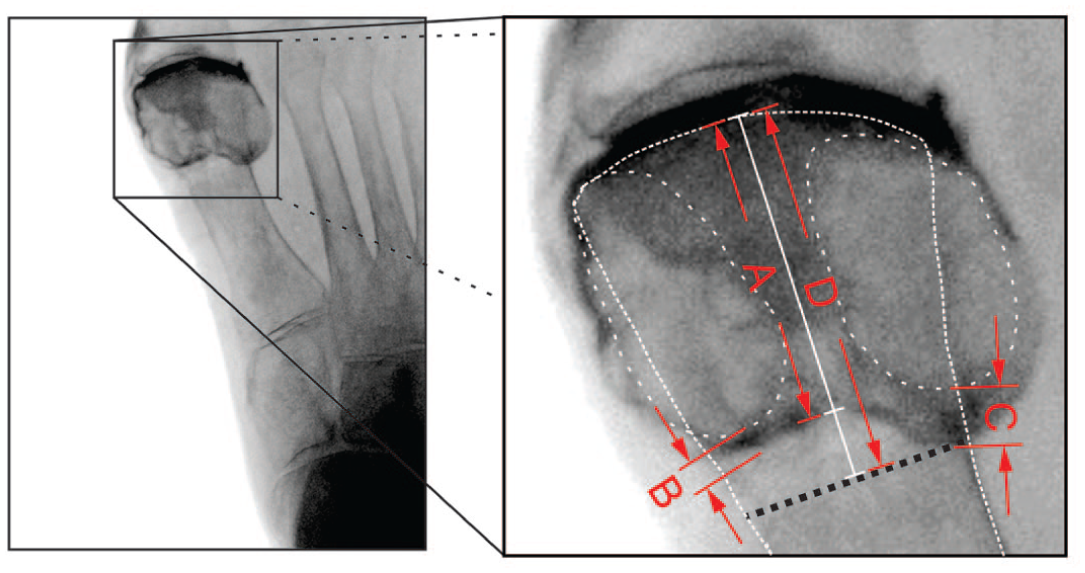
Measurements taken on the first MTP joint capsule: (A) Articular surface to the proximal edge, (B) medial sesamoid and (C) lateral sesamoid to proximal edge, and (D) articular surface to osteotomy.
Individual measurements of the specimen for distances A-D are provided in Table 2. Measurement D (articular surface to osteotomy) had a measurement of 29.5 mm, which was the largest measurement to the osteotomy site that theoretically would have remained extra-capsular if applied to 8 out of 10 specimens. Specimens 4 and 5 had capsular insertions that would have been compromised if a cut at 29.5 mm was made.
Individual Specimen Measurements of Radiographic Distances (A-D) Relative to the First Metatarsophalangeal Joint Capsule.
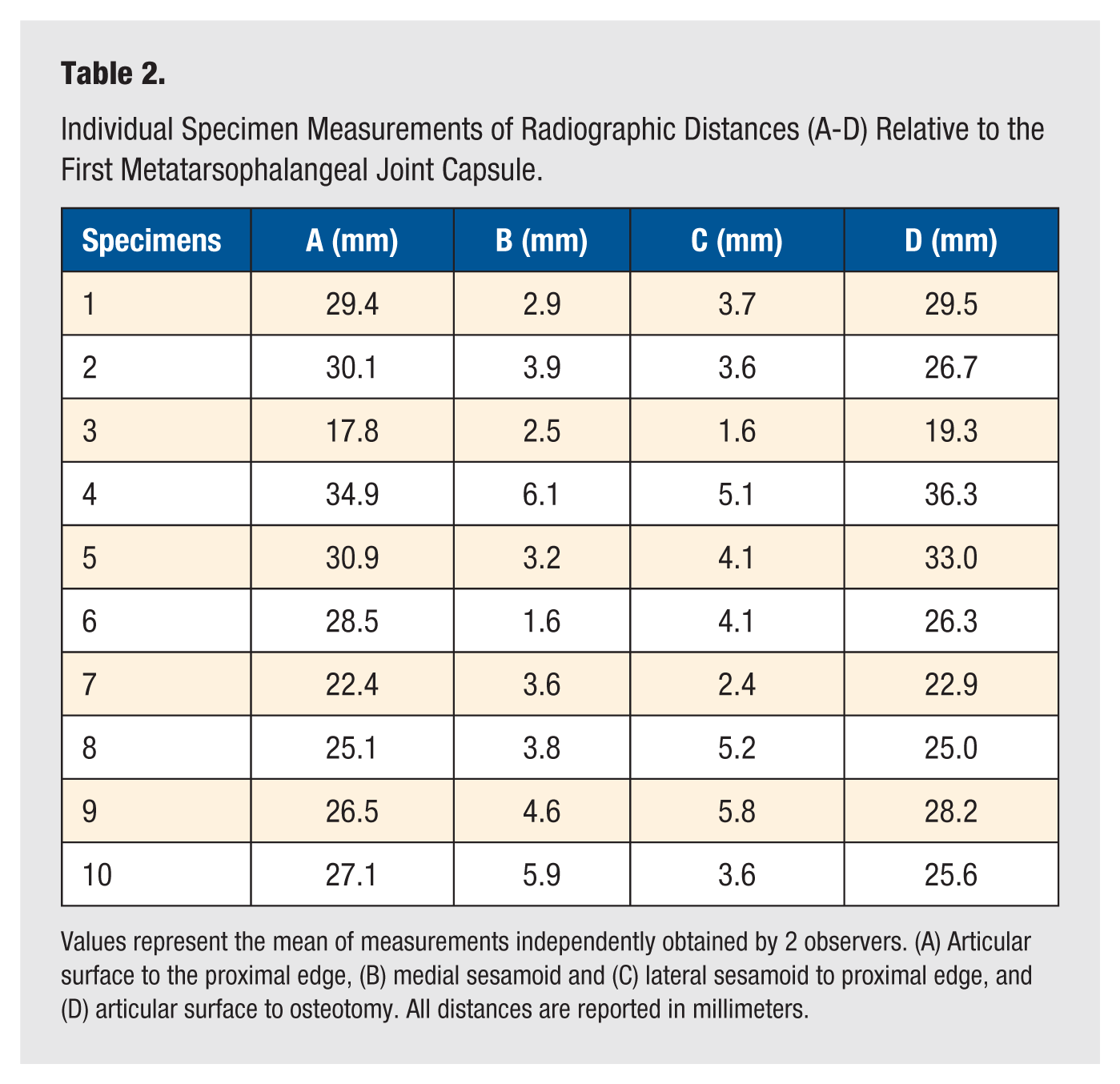
Values represent the mean of measurements independently obtained by 2 observers. (A) Articular surface to the proximal edge, (B) medial sesamoid and (C) lateral sesamoid to proximal edge, and (D) articular surface to osteotomy. All distances are reported in millimeters.
The articular surface to proximal edge (ICC = 0.937) and articular surface to osteotomy (ICC = 0.973) showed excellent reliability displaying consistency among these measurements. The apex medial sesamoid to proximal edge (ICC = 0.885) also has good reliability but had some variation. The apex lateral sesamoid to proximal edge (ICC = 0.716) was within moderate reliability range.
Anatomical dissection following a transverse minimally invasive distal metatarsal osteotomy did not reveal any capsular damage, confirming that all osteotomies were extra-capsular.
All the specimens were successfully perfused with liquid latex. The arterial distribution to the area of interest was supplied by branches from the dorsal pedis and deep medial plantar arteries. In all our cases, the first dorsal metatarsal artery (FDMA) was a direct continuation of the dorsal pedis artery. The deep plantar arteries were recognized as the deep continuation of the dorsal pedis artery toward the first metatarsal space. The anatomical dissection of the FDMA showed its intact morphology, closely associated with the transverse osteotomy (TO) (Figure 5A, dorsal view). A collateral branch of the FDMA (CBFDMA) continued in a plantar direction, deeply to the adductor hallucis (AbH) tendon, before anastomosing with the superficial branch of the medial plantar artery (SBMP) and the first plantar metatarsal artery (FPMA) forming a plantar neck plexus (PNP) near the metatarsal head (Figure 5B, plantar view). The TOs were in proximity to vessels near the metatarsal neck; however, no damage to those vessels was detected. Damage to the vessels may be considered if there is excessive penetration of the cutting blade.
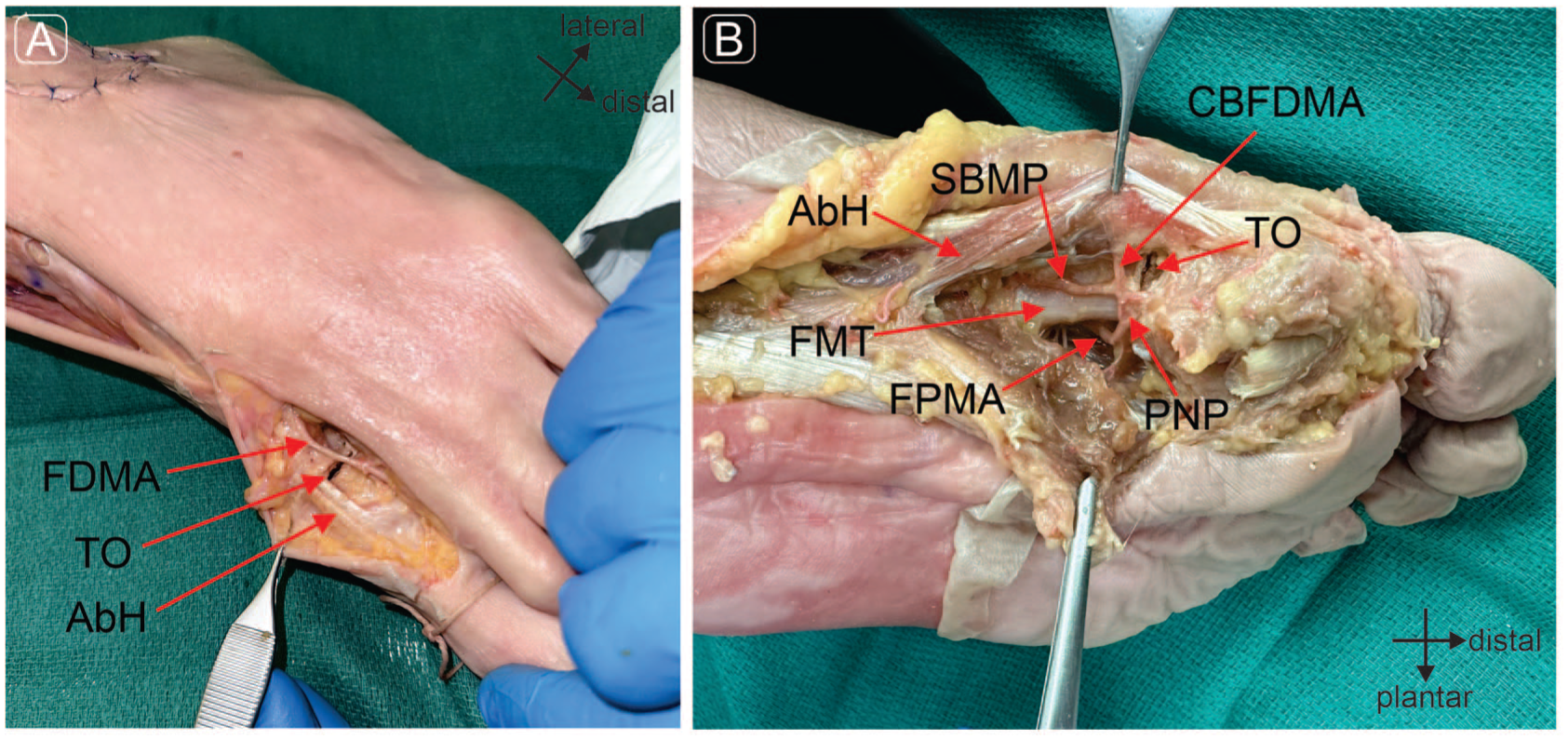
Photograph of anatomical dissection of (A) dorsal view and (B) plantar view. TO, transverse osteotomy; FDMA, first dorsal metatarsal artery; AbH, abductor hallucis tendon; FMT, first metatarsal; FPMA, first metatarsal plantar artery; PNP, plantar neck plexus; SBMP, superficial branch medial plantar artery; CBFDMA, collateral branch first dorsal metatarsal artery; TO, transverse osteotomy.
Therefore, there was no damage to the branches of the first dorsal metatarsal artery (FDMA) and first plantar metatarsal artery (FPMA) after anatomical dissection.
Discussion
Minimally invasive hallux valgus reconstruction relies on appropriate bony realignment in order to address the underlying deformity. The fourth-generation hallux valgus reconstruction features a transverse distal metatarsal osteotomy, which is ideally carried out in an extra-capsular fashion. 3 Determining this precise location for the osteotomy is important; however, few guidelines exist.
In our sample of 10 cadavers, we found that the capsular boundary is located approximately 27.3 mm proximal to the articular surface of the metatarsal head. All osteotomies performed in this study were extra-capsular at the same approximate distance of 27.3 mm, which was confirmed using contrast and dissection. It is notable that in 4 of the 10 specimens, measurement A (articular surface to proximal edge) was greater than measurement D (articular surface to osteotomy) (Table 2). We believe that the reasoning for this lies in the anatomy of the capsule. The articular capsule has an inherent pouch or slack on its dorsal surface that allows flexion of the metatarsophalangeal joint. Since the dorsal part of the capsule lies farther from the x-ray intensifier, its appearance on the 2D fluoroscopic image is relatively magnified compared to the osteotomy. This contributes to image superimposition and results in larger A measurements in those 4 cases. Despite this, the osteotomies in these 4 specimens were confirmed to be extra-capsular after dissection.
There was notable variability in the capsular insertions between specimens; therefore, a single measurement may not be reliably applied in surgical practice. When individual specimen data was analyzed (Table 2), we identified that a transverse osteotomy that is performed at 29.5 mm from the articular surface would have spared the capsule across 80% of the specimens. Therefore, a distance of 29.5 mm represents a practical guideline that maximizes safety while remaining proximal to the capsule and acknowledging anatomic variability. As was evident in the specimen dissections (Figure 3), the capsule of the first MTP joint inserts over a distance of a few millimeters and therefore an osteotomy which is placed very close to the capsular boundary may still remain extra-articular. Clinically, the distances we identified are based on landmarks that are available to surgeons intraoperatively and therefore may serve as a useful reference.
To our knowledge, this study provides the first evidence regarding the fate of the blood supply to the capital fragment following a fourth-generation MIS transverse osteotomy. While this issue had been previously investigated by Carvalho et al using a MIS chevron osteotomy, who identified minimal vascular damage, 11 our findings extend this understanding to the transverse osteotomy. We observed no damage to the major vascular structures supplying the capital fragment (Figures 4 and 5), confirming the safety of performing an extra-capsular transverse osteotomy. Indeed, the preservation of blood supply is likely an important factor allowing high union rates with MIS osteotomies, despite the large shifts required for correction.5,11 Although non-union following minimally invasive hallux valgus surgery is uncommon, it remains a recognized complication. Non-union may be attributed to both patient-related factors and technical considerations, including thermal injury from burr use or perioperative tourniquet application. 8 Preservation of the vascular supply to the capital fragment may therefore play an important role in reducing this risk; however, further investigation using clinical outcome data is required.
Previous research by Malal et al 12 observed the vascular supply to the first metatarsal head and highlighted which vessels are at risk during a traditional, open chevron osteotomy. Their study also had identified a plexus at the plantar-lateral aspect of the metatarsal neck. Based on this anatomy, an osteotomy performed proximal to the capsule could theoretically risk damaging the plexus. However, in the present study, performing a fourth-generation transverse osteotomy in an extra-capsular fashion resulted in the preservation of the vascular supply to the capital fragment. Anatomical dissection demonstrated the plantar neck plexus (PNP) to be intact in all specimens following the procedure (Figure 5B).
We identified the proximal edge of the capsule to be at a distance of 27.3 mm from the articular surface of the first metatarsal head. This is consistent with Carvalho et al’s micro-CT finding of 25.6 mm from a dorsal aspect and 23.9 mm from a plantar aspect. 11 Furthermore, we identified that the medial sesamoid is 3.8 mm and the lateral sesamoid is 3.9 mm from the proximal edge. It is important to note that in most cases of hallux valgus, the sesamoids are subluxated or dislocated and therefore cannot be reliably used as a reference point for the osteotomy site. The sesamoid measurements reported in this study are primarily to enhance anatomical knowledge regarding capsule dimensions.
Based on these findings, an osteotomy performed 29.5 mm from the articular surface of the first MTP joint is likely to remain extra-capsular, while avoiding any damage to both the vascular supply and the capsule. However, due to possible anatomical variability in the first MTP joint capsule dimensions, an extra-capsular osteotomy may not always be practical. In some cases, placing the osteotomy in an extra-capsular fashion requires a very proximal position on the metatarsal, potentially complicating obtaining stable fixation. Therefore, while obtaining extra-capsular position is typically desirable and achievable, surgeons performing MIS hallux valgus reconstruction may be forced to perform an intra-capsular osteotomy to facilitate stable fixation. Further analysis with a greater sample size and particular attention to overall metatarsal dimensions may help identify these situations.
Strengths
To our knowledge, this is the first study to evaluate the location of a fourth-generation minimally invasive transverse metatarsal osteotomy in relation to the first MTP joint capsule. Furthermore, the effect on the blood supply to the capital fragment was assessed. An extra-capsular location for the osteotomy was identified based on landmarks that are available intraoperatively, such as the articular surface. This will be helpful for surgeons planning and performing minimally invasive hallux valgus reconstruction.
Limitations
Our study has a number of limitations. The cadaveric specimens in our study were all Caucasian, potentially limiting the generalizability of the findings to the general population. We recognize there are anatomical differences of feet between ethnicities as stated by Castro-Aragon et al. 13 Our study has a limited sample size which does not reflect the overall anatomic diversity; however, this sample size is in line with other cadaveric investigations.10,11 The measurements we obtained were from fluoroscopic images, which are subject to parallax, projection distortion, and variability, potentially introducing minor inaccuracies in absolute distance measurements.14,15 After performing the osteotomy, the metatarsal head was manually displaced laterally to ensure the osteotomy is complete. The amount of displacement was not quantified; therefore, the effect of displacement on blood supply cannot be assessed in this study. Furthermore, while we had clear visualization of the main arteries and the peri-capsular plexus, it is possible that certain small peri-capsular vessels were not visualized. An in-depth inspection of the smaller vessels would be required with advanced imaging, such as micro-CT. Finally, and most importantly, these specimens did not have a hallux valgus deformity. It is possible that the anatomical dimensions of the joint capsule differ in feet with hallux valgus deformity. Further cadaveric studies assessing the joint capsule dimensions in feet with hallux valgus deformity are necessary to elucidate this issue.
Conclusion
This cadaveric investigation demonstrates that when performing a fourth-generation MIS transverse osteotomy for a hallux valgus, an extra-capsular position is obtainable in at least 80% of our specimens when the osteotomy is performed at 29.5 mm from the articular surface. At this location, no significant disruption of the blood supply to the capital fragment was encountered.
Footnotes
Acknowledgements
We would like to express our gratitude to the donors and the Dalhousie Body Donation Program for their invaluable contributions to this project. We also extend our thanks to the Horizon Health Department of Surgery for facilitating access to the C-arm. We are deeply thankful to the Saint John Regional Hospital Foundation for funding resources used in this study. Finally, we are appreciative of the volunteers at the Canada East Spine Centre for their hard work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Saint John Regional Hospital Foundation. Additional funding was provided by Dalhousie University through the Helen Watson Research Endowment as part of a student research fund.
Ethical Approval
This study was approved by the Horizon Health Network Research Ethics Board under RS #: 2024-3369.
Consent to Participate
Individuals in the Human Body Donation Program at Dalhousie University provide premortem informed consent and dedicate their bodies to medical education and research. The Body Donation office retains the informed consent signed by the donor/next of kin, or legal executor.