
Abstract
Hindfoot reconstruction is a frequently performed procedure for many complex hindfoot deformities including flatfoot, end-stage arthritis, and Charcot arthropathy. Literature has supported the treatment of these patients with a tibiotalocalcaneal (TTC) arthrodesis. However, this limb salvage procedure is complex in nature and is traditionally performed as an open surgery. Minimally invasive (MIS) tibiotalar and subtalar fusions have allowed for similar efficacy as the open procedure, with the potential for less wound complications. The current study presents a guide for TTC nailing with MIS preparation of the tibiotalar and subtalar joints for severe, progressive hindfoot deformity in the high-risk patient. This technique allows for maintenance of the soft tissue envelope; maintaining the integrity of these structures may help surgeons avoid many wound related complications, infections, or need for revision. This guide provides surgeons with an effective and reproducible approach to intervene in complex cases requiring hindfoot reconstruction.
“This technique allows for maintenance of the soft tissue envelope; maintaining the integrity of these structures may help surgeons avoid many wound related complications, infections, or need for revision . . . provides surgeons with an effective and reproducible approach to intervene in complex cases requiring hindfoot reconstruction”
Introduction
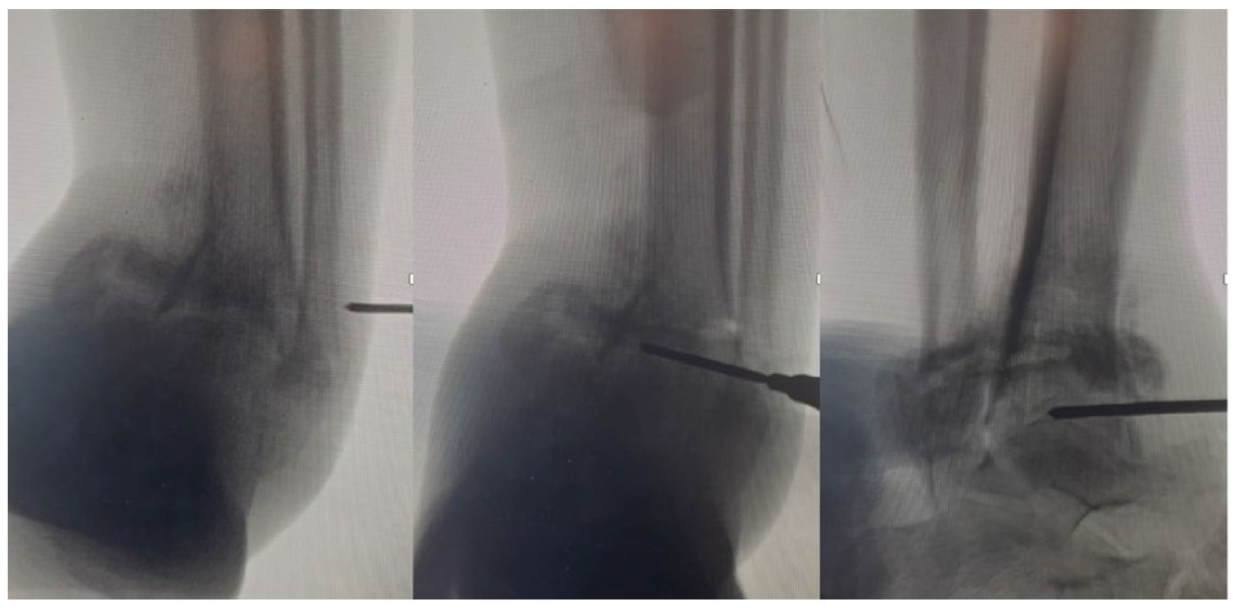
Hindfoot reconstruction is a frequently performed procedure for many complex hindfoot deformities including flatfoot, end-stage arthritis, and Charcot arthropathy. These deformities are commonly seen yet remain challenging pathologies for orthopedic foot and ankle surgeons to manage (Figure 1). Historically, these multifaceted deformities were treated with osteosynthesis implants such as Steinmann pins or angled blade plates. 1 More recently, literature has supported the treatment of these patients with a tibiotalocalcaneal (TTC) arthrodesis by way of intramedullary, hindfoot nailing. It has been demonstrated that TTC nailing allows for a stable construct, improved biology for fusion, early weightbearing, and less soft tissue dissection.1-3
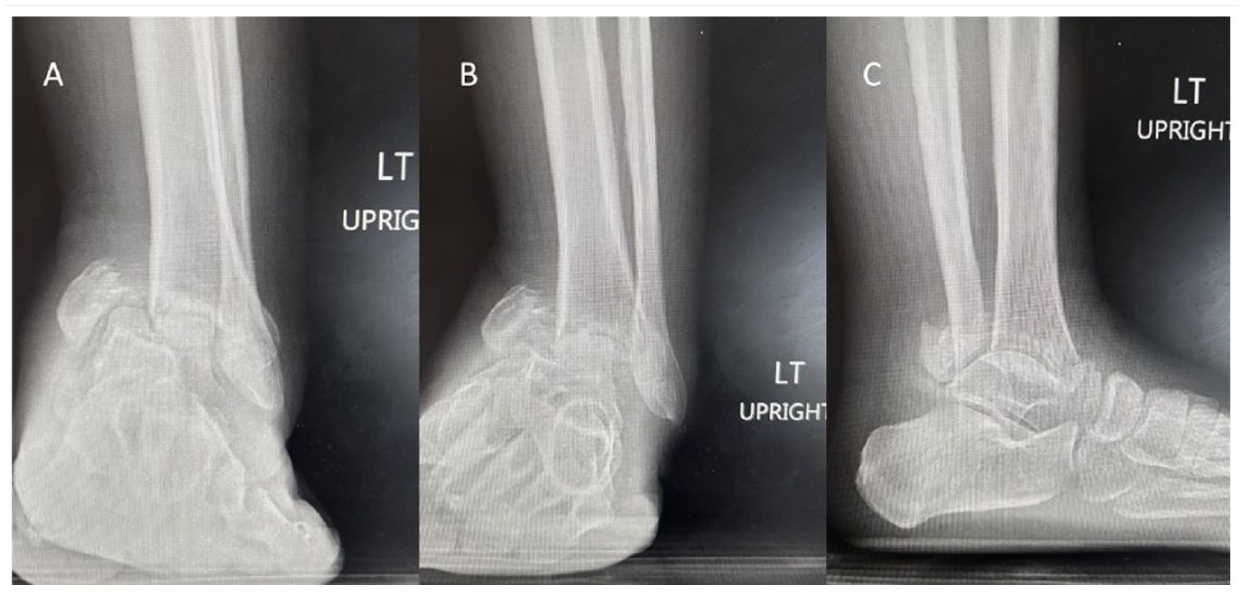
Preoperative AP (A), Mortise (B), and Lateral (C) ankle radiographs demonstrating severe left hindfoot deformity.
However, this limb salvage procedure is complex in nature and is traditionally performed as an open surgery. While the nail itself requires minimal dissection to implant, preparation of the tibiotalar and subtalar joints in an open fashion requires significant dissection and soft tissue stripping. Like many open procedures in foot and ankle surgery, there is a common concern for wound complications, infection, and nonunion, especially amongst at-risk patient populations undergoing the TTC procedure (ie, diabetic, or posttraumatic patients).4-7 Patients with Charcot, nontraumatic OA, diabetes, or chronic kidney disease were found to experience nonunion at a significantly higher rate than other patients.6,8 Similarly, patients over 60, patients with vascular disease, or patients with diabetes have been associated with a significantly increased likelihood of developing a postoperative infection after TCC arthrodesis.5,8 These challenges are not unique to TTC arthrodesis; many open procedures in the hindfoot and have been associated with similar rates of complications.4-7
When faced with these challenges, many surgeons have turned toward less-invasive procedures. In recent years, minimally invasive surgery (MIS) has become more common across foot and ankle orthopedics. While MIS techniques in the foot and ankle have been associated with a learning curve and potentially limited application in patients with most severe bone defects, MIS has demonstrated less swelling, lower wound complication rates, and fewer postoperative infections when compared to traditionally open procedures.9-15 Recently, the advantages of MIS in hindfoot reconstruction were highlighted in the systematic review by Vaggi et al. 16 Comparable clinical results were observed between MIS and open techniques, however a significant reduction in infections and postoperative neuropathy was reported in the MIS cohort. Relevant to the TTC arthrodesis procedure, MIS tibiotalar fusion and MIS subtalar fusions have demonstrated similar efficacy to the open procedure, with less wound complications. 17
Accordingly, in the current review, we present a case of TTC nailing with MIS preparation of the tibiotalar and subtalar joints for severe, progressive hindfoot deformity in the high-risk patient. This MIS technique includes a percutaneous lateral +/− medial osteotomy to acquire access to the joint space and correct the deformity. In addition, we describe a novel quadrant system to achieve MIS joint preparation. This nuanced technique allows for maintenance of the soft tissue envelope throughout the TTC nailing procedure. While outcome studies remain limited, the current authors have observed preservation of the soft tissue envelope throughout this MIS procedure to allow for high fusion and low complication rates. 18
Surgical Technique
The patient is placed in the supine position on a regular operating room table with a radiolucent extension. The heel is in line with the end of the table to ensure ease of intraoperative imaging and screw placement. A towel bump is generally placed under the ipsilateral hip so that the tibial tubercle is facing straight up with the leg at rest. A large C-arm is used. Of note, a tourniquet is not used during this procedure. The bleeding generated during the case will assist with cooling the bur and preventing thermal necrosis of the bone or skin.
In the case presented, there was a chronic ankle fracture dislocation. This patient had no other contributory past medical or surgical history. It was not reducible and therefore in addition to joint preparation, bony correction was required as well to correct the deformity. First, standard anteromedial and anterolateral portals were created. A transfibular approach may be added when addressing pathology about the posterior talus. This lateral malleolar osteotomy was first made at the level of the tibiotalar joint. This allowed shortening of the fibula as well as access for percutaneous joint preparation. The location of the planned osteotomy is determined fluoroscopically with a mortise view of the ankle, after which a longitudinal 5mm incision is made laterally in the midcoronal plane of the fibula. Blunt dissection is carried down to bone with a hemostat. Next, a Shannon burr is advanced through both cortices of the fibula under fluoroscopic guidance, ensuring that it remains coplanar with the tibiotalar joint in the coronal plane (
Once the osteotomy was completed, access to the tibiotalar joint was obtained. The cartilage and subchondral bone of the joint are then taken down with the burr under the guidance of tactile feedback, fluoroscopy, and arthroscopy. A quadrant system is generally utilized by the surgeon as described in previous MIS literature.
20
We prefer to divide both sides of the joint into 4 quadrants each (anterolateral, posterolateral, anteromedial, and posteromedial), and it is often easier to work from lateral to medial if working from the transfibular portal. The contour of the tibial plafond and talar dome should be followed with the burr in order to maintain length and optimal bony contact of the planned arthrodesis. When performing for the first time, the surgeon may use a freer or other probe to “map” the contour of the joint before inserting the bur. This helps with the tactile navigation when using the bur. Alternatively standard anteromedial and/or anterolateral arthroscopic portals can be made additionally to access the joint as well. Anteroposterior (AP) and lateral fluoroscopic images are taken intermittently to confirm the location of the burr as well as demonstrate progression of joint surface debridement from lateral to medial. Lateral x-rays can be useful to confirm adequate joint preparation anterior to posterior. Arthroscopy is utilized to confirm adequate debridement of joint surfaces
The subtalar joint is then prepared in similar fashion. A lateral view of the subtalar joint is obtained to localize the incision. A 5mm longitudinal incision is made laterally, directly overlying the sinus tarsi or just anterior to the fibula at the level of the subtalar joint (Figure 2). The subtalar joint should be marked on the skin to help with bur control. A hemostat is then used to bluntly dissect through subcutaneous tissue, after which it is advanced into the subtalar joint and its location is confirmed fluoroscopically. Again, a quadrant system is used to systematically debride the joint surfaces, most commonly working from lateral to medial and posterior to anterior. A posterolateral portal is useful for preparation of the joint as well; and, anecdotally, it is easier to control the bur within the joint when learning the technique from the posterolateral approach (Figure 3). Fluoroscopy, freer palpation, and arthroscopy are again utilized to guide joint preparation and address missed areas of cartilage and subchondral bone. Once the subchondral bone has been exposed, the bur can be used to fenestrate the joint.
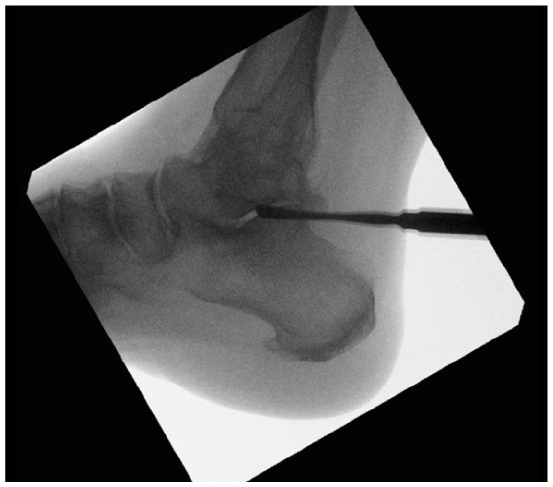
Lateral view of the subtalar joint is obtained to localize the incision to allow for preparation of the subtalar joint.
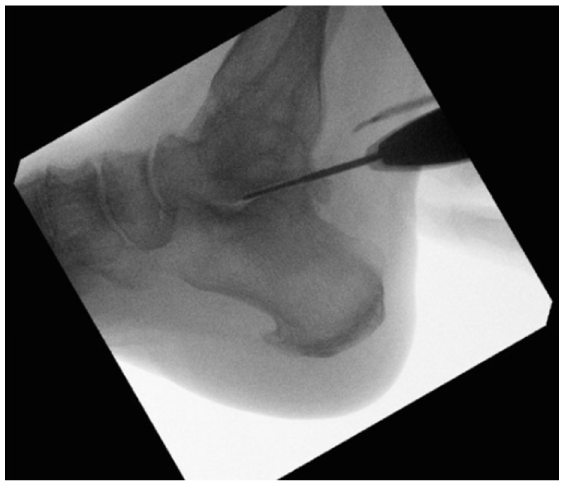
A posterolateral portal as utilized for preparation of the subtalar joint.
Hindfoot correction is then trialed manually. Often, a significant correction can be obtained after the debridement of both the tibiotalar and subtalar joints. We aim for 0 to 3 degrees of hindfoot valgus from the anatomic and mechanical axes of the tibia. Adjunctive procedures such as percutaneous Achilles tendon lengthening, medial malleolar, or others may be employed at this time. Figure 4A and B demonstrate a common decision flow chart that can be useful when considering correcting the varus and valgus ankle and hindfoot during MIS TTC fusion, respectively.
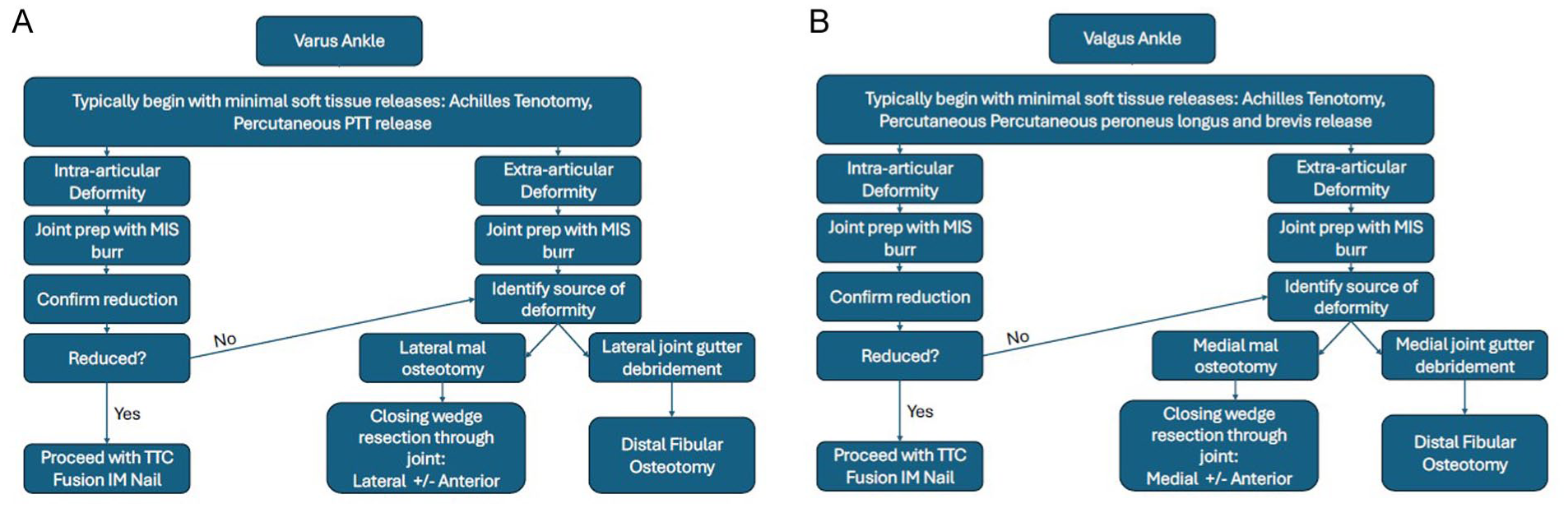
Surgical planning algorithm for correction of the (A) varus or (B) valgus ankle during MIS TTC fusion.
If required for correction, a medial malleolar osteotomy is made with the burr. This is done through the medial working portal or a separate medial 5mm incision can be made if needed directly medial and proximal to the joint line. It is completed in the same fashion as the lateral malleolar osteotomy, advancing the burr through both cortices in the midcoronal plane followed by completion of the osteotomy anteriorly and posteriorly. Of note, care must be taken during this step to inspect the skin medially and ensure that there is no undue tenting after the correction.
Unlike with open surgery which typically relies on soft tissue releases for deformity correction, the MIS technique relies on osteotomies to achieve the desired correction. Once complete, bone graft, bone graft substitute, growth factors, or a combination thereof are then placed in the tibiotalar and subtalar joints. At our institution, a mixture of calcaneal bone graft, allograft, and recombinant growth factors is utilized, though graft of choice may be used. There are multiple graft delivery systems, a simple option is to load the graft into a 1cc syringe that has been cut open at the tip. This can be inserted into the joint via the MIS portals and the bone graft delivered percutaneously (Figure 5).

Mixture of calcaneal bone graft, allograft, and recombinant growth loaded into a 1cc syringe.
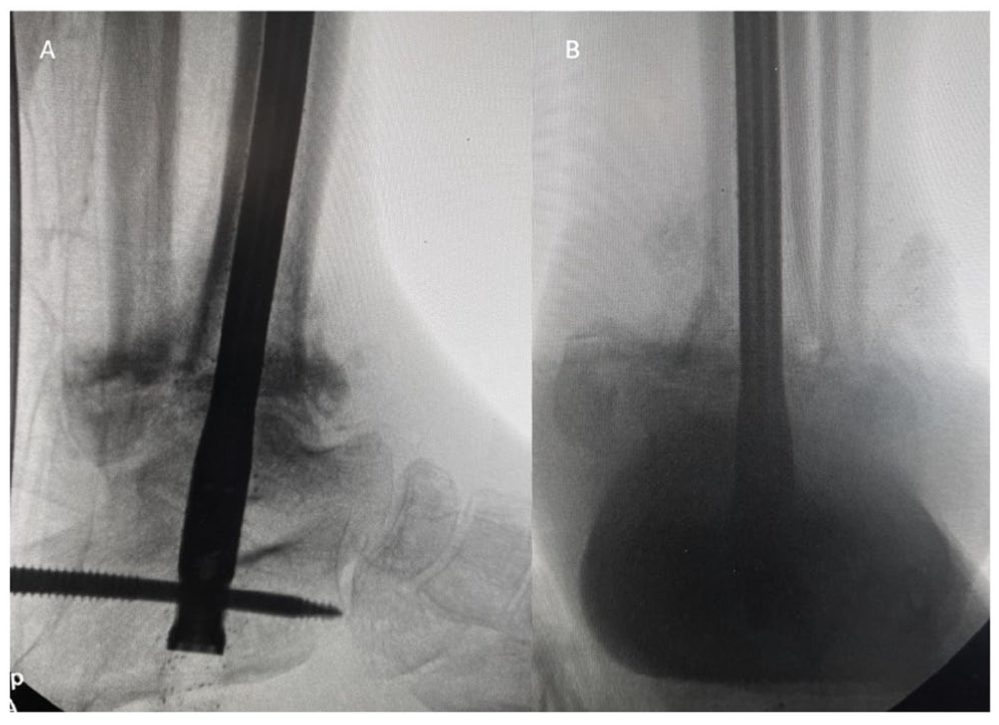
The procedure then continues with TTC nailing. Hindfoot correction is first provisionally held with 2 threaded guidewires or large K-wires to remove the assistant’s hands from the field for ease of imaging. These are placed out of the way of the planned nail (Figure 6). A threaded guidewire is then inserted percutaneously into the plantar surface of the calcaneus, in line with the talus and tibial shaft in both the coronal and sagittal planes, and advanced into the tibial shaft. The calcaneus, talus, and tibia are then reamed in sequential fashion. An intramedullary nail is then placed with multiple interlocking screws proximally and distally (Figure 7). The authors typically use a nailing system with the possibility for dynamic, postoperative compression (DynaNail, DJO, Lewisville, TX) if there is not considerable bone loss or other reason for risk of significant shortening, but any modern TTC nail with internal compression may be considered.

Intraoperative fluoroscopy demonstrating placement of 2 threaded guidewires or K-wires to provisionally hold hindfoot correction, out of the way of the planned nail.
Intraoperative, fluoroscopic view of Shannon burr within the bony interface.
The remainder of the case is completed in standard fashion with irrigation, closure, and splinting with a bulky dressing (Figures 8-11). Importantly, while the entirety of the procedure is completed percutaneously, these wounds must all be inspected prior to closure to identify any areas of thermal necrosis. If any indication of such is found, sharp debridement should be performed prior to closure.
Intraoperative lateral (A) and AP (B) fluoroscopic image following TTC nail placement.

Final closure demonstrating minimal incisions about the lateral left foot and ankle.
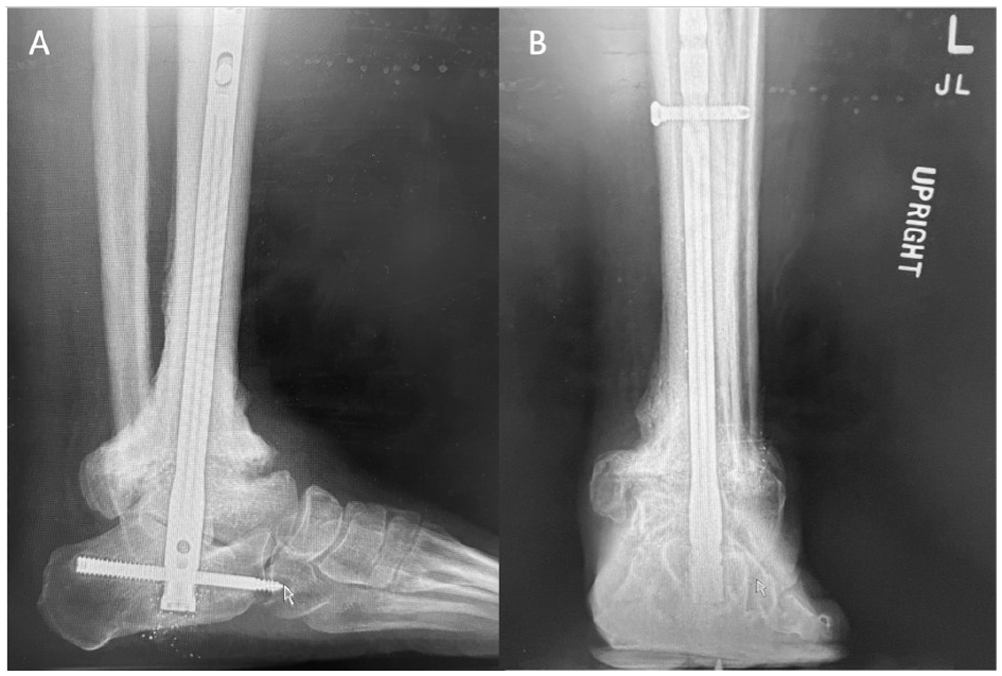
Postoperative weightbearing lateral and AP radiographs of left ankle, demonstrating MIS TTC nail.
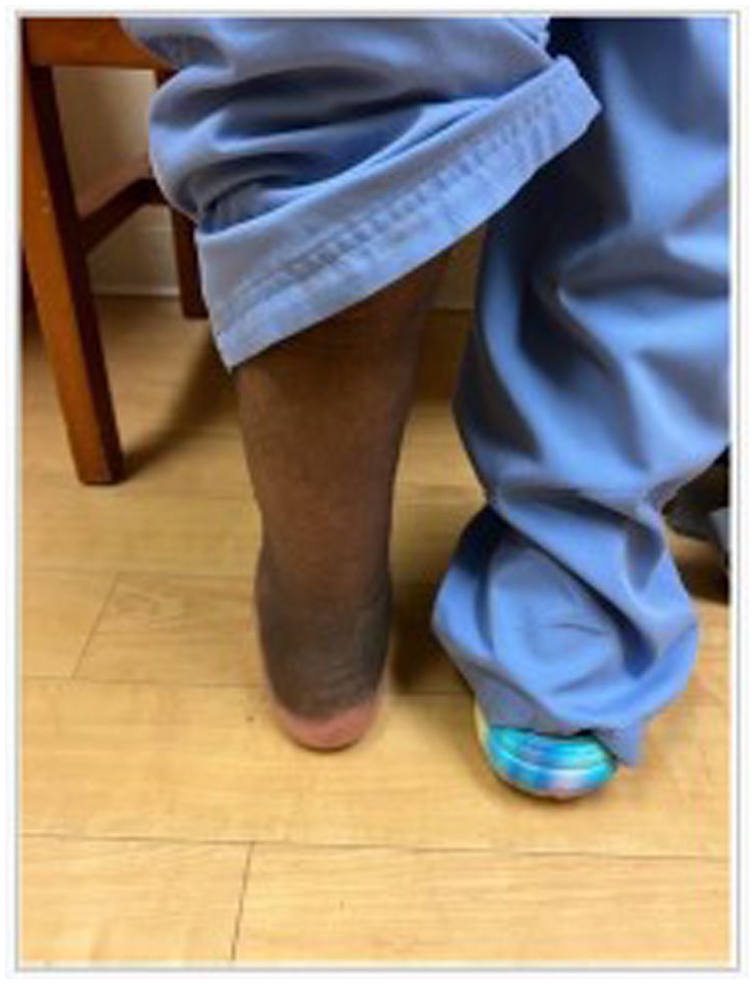
Postoperative image of posterior foot alignment following MIS TTC nailing.
Discussion
The current study presented a minimally invasive alternative to the standard TTC arthrodesis for hindfoot reconstruction. The standard TTC arthrodesis is most commonly performed as an open surgery, despite the ability for fixation to be placed percutaneously (i.e. hindfoot nailing). The open technique therefore carries inherent risk of wound complications, infection, and nonunion. 21 In addition, the open procedure relies primarily on soft tissue releases to allow for deformity correction, while the presented MIS technique relies on osteotomies. As cases requiring hindfoot reconstruction are complicated and often limb salvage cases, many of these patients (especially diabetic or posttraumatic patients) are already at an increased risk for wound complications, infection, and nonunion.4-7 The technique presented here allows for maintenance of the soft tissue envelope, which theoretically allows for a higher success rate and fewer complications. By maintaining the integrity of soft tissue structures, we may be able to circumnavigate many wound related complications, infections, nonunion, and ultimately the need for revision.
Numerous studies have reported that 20% to 40% of their patients will have a major complication following open TTC arthrodesis, and 20% to 30% of these cases will require a revision surgery.8,9 In a retrospective study of 101 patients, Pitts et al 8 reported a 28.7% nonunion rate amongst patients who underwent TTC arthrodesis. Separately, Levinson et al 6 reported 17% of the 47 patients included in their retrospective study had experienced hardware failure, 75% of which led to nonunion. A nonunion rate of 10% amongst patients who did not experience hardware malfunction was reported (21.3% nonunion overall). When faced with these common complications to many open foot and ankle procedures, many in the field have turned toward MIS techniques. For example, Carranza-Bencano et al 17 found similar union rates with MIS subtalar fusions in comparison to those reported for open procedures (92.2%), yet with zero wound complications (superficial or deep). Zhao et al 22 similarly found no difference in efficacy with the MIS tibiotalar fusion preparation in a cadaveric model in comparison to open techniques.
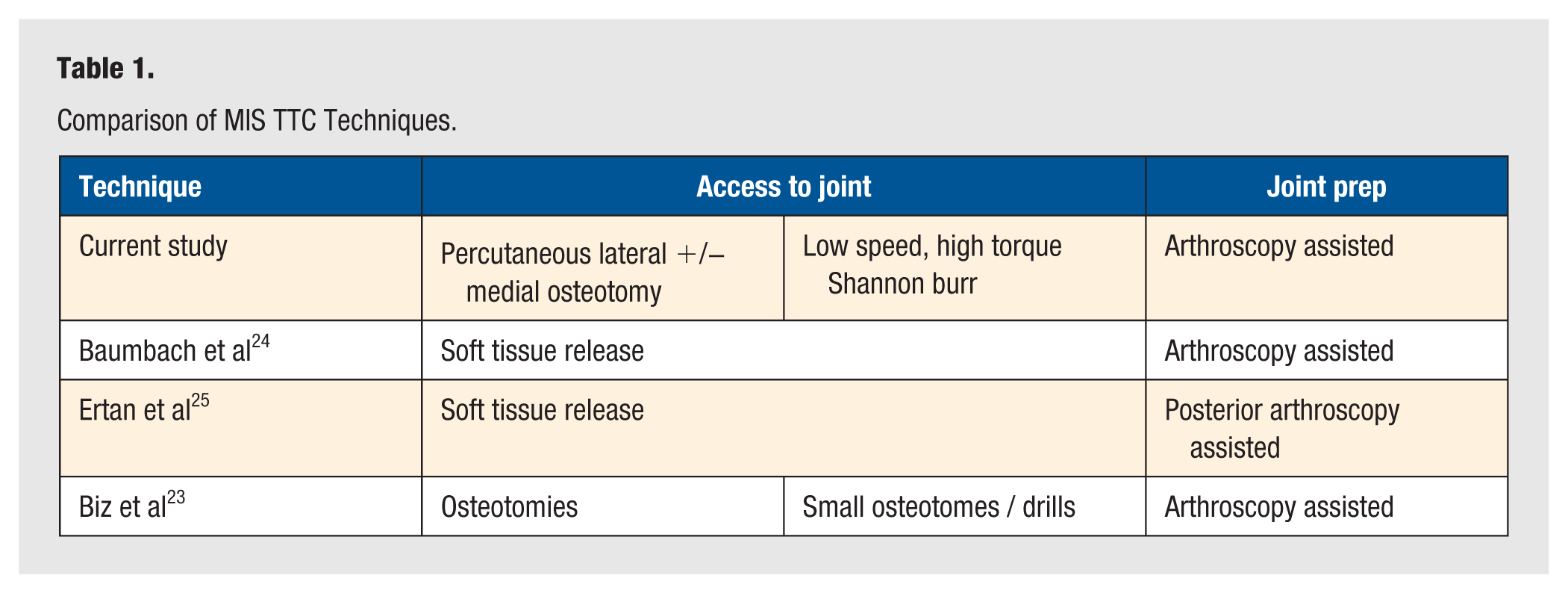
Previously, authors have reported success with less invasive TTC nailing techniques, including arthroscopy.23-25 Baumbach et al 24 described acceptable correction and a reduction in total complications (33% vs 63%) and wound specific complications (50% vs 0%) in patients who underwent arthroscopic TTC nailing versus open TTC nailing, respectively. Separately, through a posterior arthroscopic-assisted approach, Ertan et al 25 reported a significant improvement in AOFAS and VAS scores at 12 months post operation; a 12% major complication rate and 8% minor complication rate was observed. Similar to the current study, Baumbach and Ertan utilized arthroscopy to visualize the preparation of joints; however in contrast, both techniques include release of soft tissue structures to access joint surfaces and allow for deformity correction. Instead, our technique obtains access to joint surfaces and deformity correction through a percutaneous lateral +/- medial osteotomy.
In 2016, Biz et al described a technique that is perhaps the most similar to the technique presented in the current article. In their prospective study based in Italy, Biz et al presented a MIS TTC nailing technique that utilized percutaneous and arthroscopic preparation of the ankle. They describe the use of small osteotomes and drills to access and prepare joint surfaces. Biz et al 23 demonstrated a postoperative improvement in AOFAS and VAS scores (P < .05) in addition to low total complication (28.56%) and wound specific complication (0%) rates. In contrast, the current technique includes novel description of percutaneous osteotomies with a Shannon burr to allow access joint surfaces and correction of deformity. We also describe removal of cartilage and sclerotic bone with a standardized MIS quadrant system. In addition, of note, the current study offers a comprehensive guide to demonstrate important preoperative and perioperative decisions when treating patients with varus or valgus deformities (Table 1).
Comparison of MIS TTC Techniques.
The authors recommend the technique presented here for any patient undergoing hindfoot reconstruction where TTC nailing with open joint preparation would otherwise be required, especially in higher risk populations (eg, diabetic and posttraumatic). While the authors have found success with this procedure in comparison to the open technique, it is not without its own limitations. In patients with large defects that require structural bone grafting or other implants such as a cage, the MIS technique would be limited due to the necessity for open exposure regardless of joint preparation method. Furthermore, there may be a learning curve as with other MIS techniques. 12 This may add to operative time and difficulty initially, though our authors experience has been a reduction in operative time in comparison to the open procedure due to saved time during both exposure and closure.
Minimally invasive surgery techniques may induce a risk for thermogenic osteonecrosis and skin edge necrosis. However, even in this patient population, who are potentially at higher risk of nonunion, the authors feel the benefits of the MIS technique presented here outweigh the potential risk. Furthermore, the risk of procedure failure due to wound complications or infection with the open procedure is much greater than the risk of nonunion due to thermal necrosis in the MIS.8,9,26 The authors take great care to continuously apply copious cooled irrigation while burring. It is advised to also pause the burr every 10 seconds to allow for heat dissipation. Many previous studies have demonstrated no increased risk of thermal necrosis when using this burring technique when performing MIS bunion corrections, MIS Zadek osteotomies, other MIS calcaneal osteotomies, and/or MIS ankle arthrodesis. 19 ,27-33 Another concern is that this MIS approach theoretically may leave behind fragmented cartilage that was debrided throughout the procedure. In agreement with previous authors, 5 the authors of the current study do not feel that there is significant consequence to this given the adequacy of debridement back to healthy, cancellous bone.
While few previous studies have compared the outcomes of open versus MIS tibiotalar and subtalar arthrodesis procedures, literature remains limited in similar open versus MIS comparisons of the TTC nail technique.17,18,22 Future prospective cohort studies may be warranted to directly compare the outcomes, complications, and patient satisfaction following the open versus MIS preparation for TTC nailing. This may allow for a closer look into the more specific indications for this MIS procedure in comparison to the open approach.
Conclusion
Tibiotalocalcaneal arthrodesis has the potential to result in wound complications or infection, particularly in complex deformities or patients with medical comorbidities. Our proposed MIS TTC nailing technique allows for preparation of the subtalar and tibiotalar joints while maintaining the soft tissue envelope and minimizing dissection, therefore potentially minimizing these risks. We hope this guide will provide surgeons with a novel approach to successfully intervene in complex cases and high-risk patients requiring hindfoot reconstruction.
Footnotes
Author Contributions
CAP, SHK, CM, TAG: concept production, writing, manuscript preparation, image and figure generation. JO, EV, JBJ: concept production, manuscript editing.
Data Availability
Not applicable as this manuscript is a technique tip.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CAP, SHK, JO: none. EV: Consultant for Novastep, Treace, Vilex, Surgebright; Royalties: Surgical Fusion Technologies, Treace Medical Concepts, Vilex. JBJ: consultant for Synthes. CM: consultant for Enovis. TAG: Consultant for Treace Medical Concepts Inc, Surgical Fusion Technologies, Stryker, Enovis, Exactech, Surgebright; Royalties: Surgical Fusion Technologies, Treace Medical Concepts, Vilex.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
As this manuscript is a technique tip, IRB approval was not applicable.
Trial registration
As this manuscript is a technique tip, trial registration was not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.