
Abstract
Background. Lag screw-only fixation has been proposed as a less invasive alternative to traditional plating for simple oblique fractures of the distal fibula. This technique may reduce hardware-related complications while maintaining adequate stability and promoting fracture healing. This review aims to assess whether a lag screw-only construct can provide sufficient stability and reduce complications commonly associated with traditional lag screw-plus plate fixation in patients with simple oblique distal fibular fractures. Methods. A narrative review of the literature was conducted through PubMed, Embase, and the Cochrane Library. Studies were included if they reported clinical or biomechanical outcomes of lag screw-only fixation in simple oblique fibular fractures. Biomechanical studies and editorials relevant to the technique were also reviewed for context. Results. Eight clinical and 6 biomechanical studies were identified. Patients included primarily presented with Lauge-Hansen SER-type fractures without comminution. Across studies, lag screw-only fixation demonstrated 100% union rates, with clinical and functional outcomes comparable to traditional plating. Validated scores such as Olerud and Molander (OM), Foot and Ankle Ability Measure (FAAM), and Single Assessment Numeric Evaluation (SANE) indicated excellent postoperative function. Complication rates were generally low. Biomechanical models suggested similar stability to plating. Early mobilization and weightbearing were rarely implemented, with only a letter to the editor suggesting their safety. Conclusion. For selected cases, lag screw-only fixation may be a viable option in the treatment of distal fibular fractures. However, current evidence remains limited and heterogeneous. Further studies are needed to validate its safety and suitability for early rehabilitation protocols. This study is designed as a narrative review.
“This review aims to assess whether a lag screw-only construct can provide sufficient stability and reduce complications commonly associated with traditional lag screw-plus plate fixation in patients with simple oblique distal fibular fractures.”
Introduction
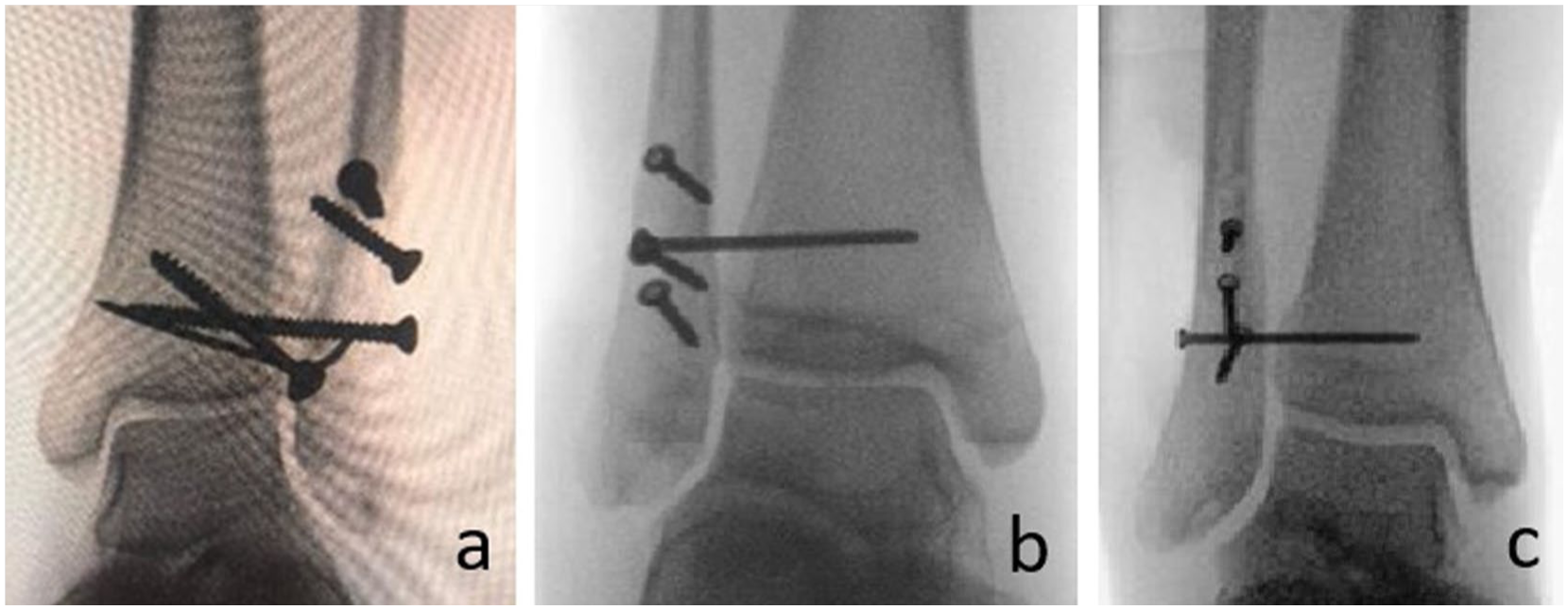
Traditionally, displaced simple oblique fibular fractures have been managed using a lag screw in combination with a neutralization plate.1,2 The lag screw provides interfragmentary compression by engaging only the far cortex, while the near cortex is over drilled. This configuration draws the distal fragment tightly against the proximal, creating stability that facilitates primary bone healing without callus formation.1,2 The neutralization plate is thought to protect interfragmentary compression by counteracting torsional, bending, and shearing forces; helping distribute mechanical stresses; and maintaining alignment under functional loads. However, the necessity of adding a plate in these fracture types has been questioned, particularly given the complications associated with its use, including soft tissue irritation, hardware prominence, wound-related issues, and the frequent need for implant removal.1 -4 From a biomechanical perspective, the fibula contributes minimally to weight transmission through the lower limb, bearing only about 6% to 17% of axial loads. 5 Its primary role is to stabilize the ankle mortise and maintain length and alignment. 6 This physiological characteristic supports the notion that minimal fixation can be sufficient in selected fracture patterns. From this standpoint, fibular osteosynthesis could be conceptualized similarly to fixation in non-weightbearing bones. For example, lag screw-only constructs are widely used in the treatment of oblique metacarpal fractures, where they have been shown to provide adequate stability and allow for early mobilization. 7 Given these findings, this article aims to review the available literature to date on the use of lag screw-only fixation for non-comminuted oblique fibular fractures (Weber B), including those occurring as part of a supination-external rotation (SER) injury pattern, with a focus on its potential to reduce complications commonly seen with traditional plate osteosynthesis (Figure 1).

Different number of lag screws. (a and b) Standard 2-screw configuration. (c and d) Extended 5-screw fixation of a long fibular spike.
Methodology
This narrative review was based on a literature search conducted across PubMed, Embase, and the Cochrane Library. The search strategy used the following terms: (“fibula” OR “peroneal” OR “lateral malleolus” OR “ankle”) AND (“lag screw”). In parallel, an independent PubMed search using a similar strategy—(“Fibula”[Mesh] OR “Fibula Fractures”[Mesh] OR fibul*[tiab] OR lateral malleolus[tiab] OR peroneal fracture*[tiab]) AND (“Bone Screws”[MeSH] OR screw*[tiab] OR lag screw*[tiab]) AND (“Fracture Fixation”[Mesh] OR fixat*[tiab])—was performed by a second reviewer. After removal of duplicate entries, the resulting articles were independently screened by 2 reviewers. The reference lists of included studies were searched (snowballing) to identify additional papers. Inclusion criteria focused on studies reporting clinical outcomes of patients treated with lag screw-only fixation for simple oblique fibular fractures. Relevant biomechanical studies and review articles discussing the technique or its implications were also included for comprehensive context. Intramedullary devices such as nails and intramedullary lag screws were excluded, given their traditional use in lower-demand patients, which contrasts with the clinical profile typically indicated for lag screw-only fixation.
Results
Six biomechanical studies1,2,8 -11 and 8 clinical studies 6 ,12 -18 were reviewed. In addition, several articles identified during the search were used to support the rationale behind lag screw fixation.3,4,19 -21
Biomechanical Considerations
Misaghi et al 1 evaluated long-oblique distal fibula osteotomies in sawbone models, comparing 3.5 mm lag screw constructs (1/2/3 screws) with a lag screw-plus-plate control (Table 1). The 3-screw configuration achieved comparable bending/rotational stiffness and failure torque to plating, whereas 2-screw fixation showed reduced bending resistance and single-screw constructs were biomechanically inferior.
Biomechanical Studies Comparing Lag Screw-Only Versus Plate Fixation.
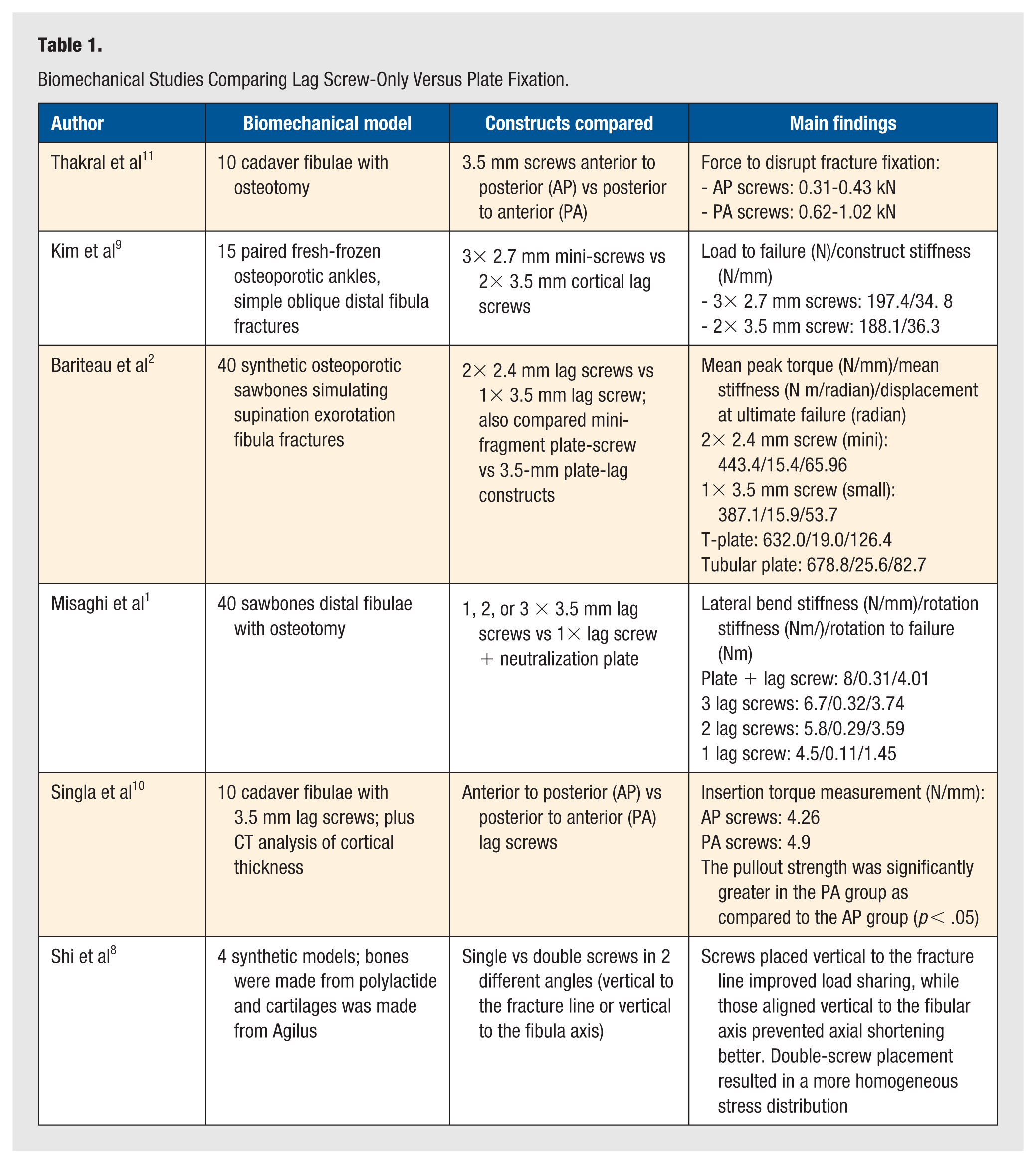
The use of more than 1 screw in lag screw-only fixation is also supported by the study of Shi et al, 8 who performed a combined finite element and in vitro analysis using sawbone models. They found that double-screw fixation provided superior biomechanical stability than single-screw fixation. In addition, they incorporated ankle movement into their analysis, showing that dorsiflexion reduced displacement compared to the neutral position and plantarflexion.
Two other additional aspects found in the reviewed studies concern, on one hand, the use of mini-fragment screws, and on the other hand, the biomechanical performance of different constructs in osteoporotic bone,2,9 where achieving reliable interfragmentary compression is challenging and increases the risk of iatrogenic damage. Bariteau et al 2 conducted a torsional biomechanical study using osteoporotic sawbone models, evaluating 4 fixation constructs: two 2.4-mm mini-fragment lag screws, one 3.5-mm lag screw, two 2.4-mm lag screws with 2.4-mm mini T-plate, and a 3.5-mm lag screw with one third tubular plate (Figure 2).
Different diameter lag screws depending on the size of the fibula per-operatively: (a) 3.5-mm small-fragment, (b) 2.7-mm mini-fragment, and (c) 2.4-mm mini-fragment screws.
Their results showed that both plated constructs provided greater ultimate torque and torsional stiffness compared to any screw-only configuration. However, while plating demonstrated superior mechanical stability, the use of osteoporotic sawbones reflects the already mentioned limitation of achieving consistent interfragmentary compression and overall construct stability in poor bone quality, particularly in lag screw-only fixation. Of note, the study also found that two 2.4-mm lag screws performed equivalently to a single 3.5-mm lag screw, suggesting that smaller-diameter screws may be an equivalent and more feasible option when placing more than one screw is desired, or when the goal is to reduce the potential for hardware-related discomfort.
Similarly, Kim et al 9 carried out a comparison using fresh-frozen cadaveric ankles simulating simple oblique distal fibula fractures. Each pair was randomized to receive 3 bicortical 2.7 mm mini-screws (not applied as classic lag screws) or two 3.5-mm lag screws. It is worth noting that the study implemented osteoporotic specimens (confirmed via calcaneal bone mineral density [BMD]). Nevertheless, using 3 bicortical 2.7-mm mini-screws without traditional lag screw compression was found to be non-inferior to the conventional 3.5-mm lag screw approach. This technique may offer a viable alternative for screw-only fixation in poor bone quality, helping to avoid complications associated with attempting interfragmentary compression in these cases. Furthermore, mini-screws preserve more bone stock and allow for the placement of multiple screws within a limited area.
Regarding technical considerations, a key insight for improving lag screw-only construct stability arises from cadaveric studies by Thakral et al 11 and Singla et al. 10 Both demonstrated that posterior-to-anterior interfragmentary screw placement outperforms the traditional anterior-to-posterior trajectory, likely due to better engagement of the thicker anterior fibular cortex (Figure 3).
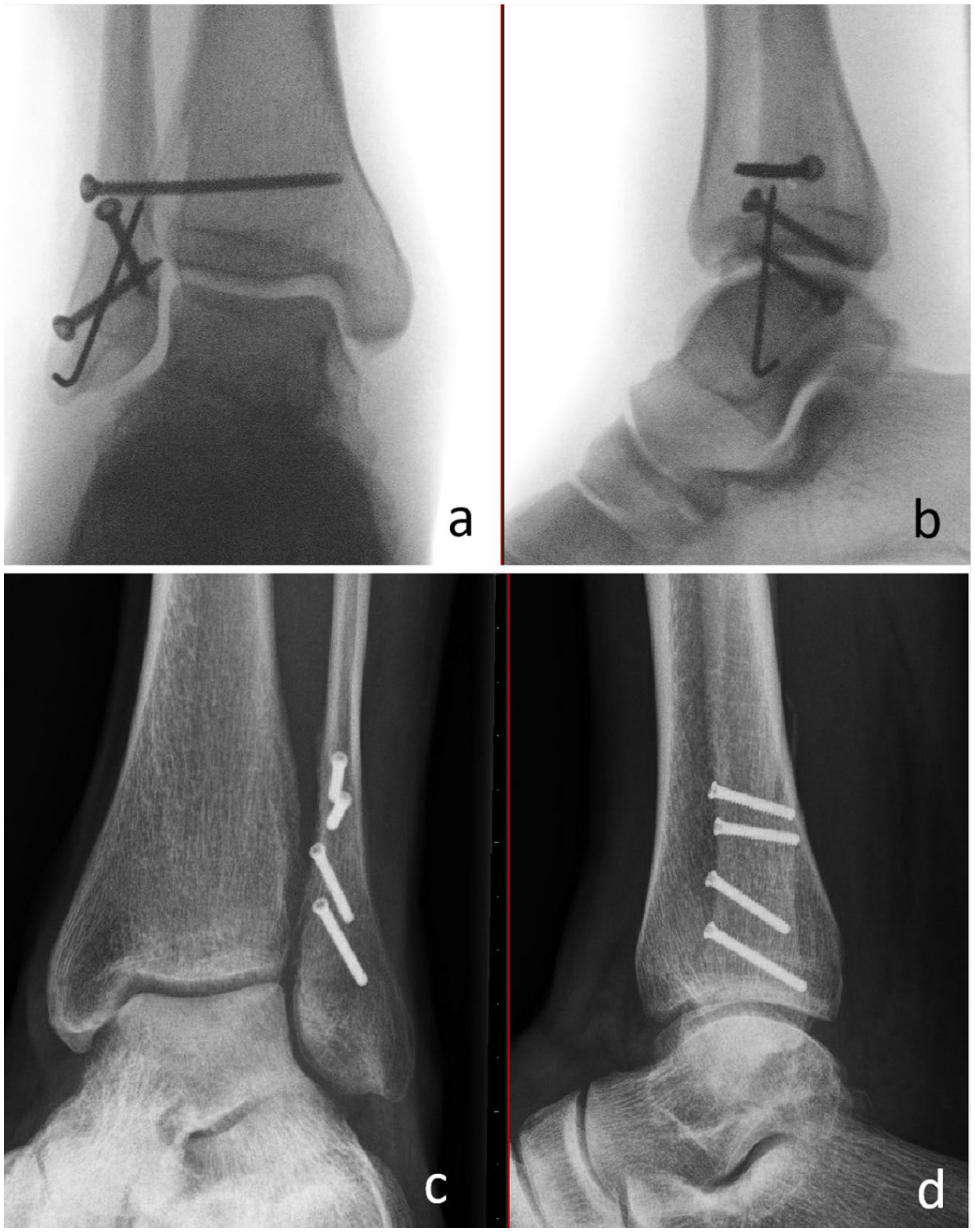
Technical tips regarding the use of lag screws. (a and b) Alternating the screw direction from anterior-posterior to posterior-anterior increases strength, and (c and d) using locking screws as lag screws sinks the head into the near cortex and potentially diminishes the rate of implant-related complaints.
Clinical Outcomes
Out of the 8 published studies that have reported on the clinical outcomes of lag screw-only fixation for distal fibular fractures, 7 were conducted in adult patients and 1 involved adolescent patients (Table 2). All but one of the studies were retrospective, where cohorts of patients with similar fracture types were selected to compare postoperative outcomes.
Clinical Studies Reporting Outcomes of Lag Screw-Only Fixation.
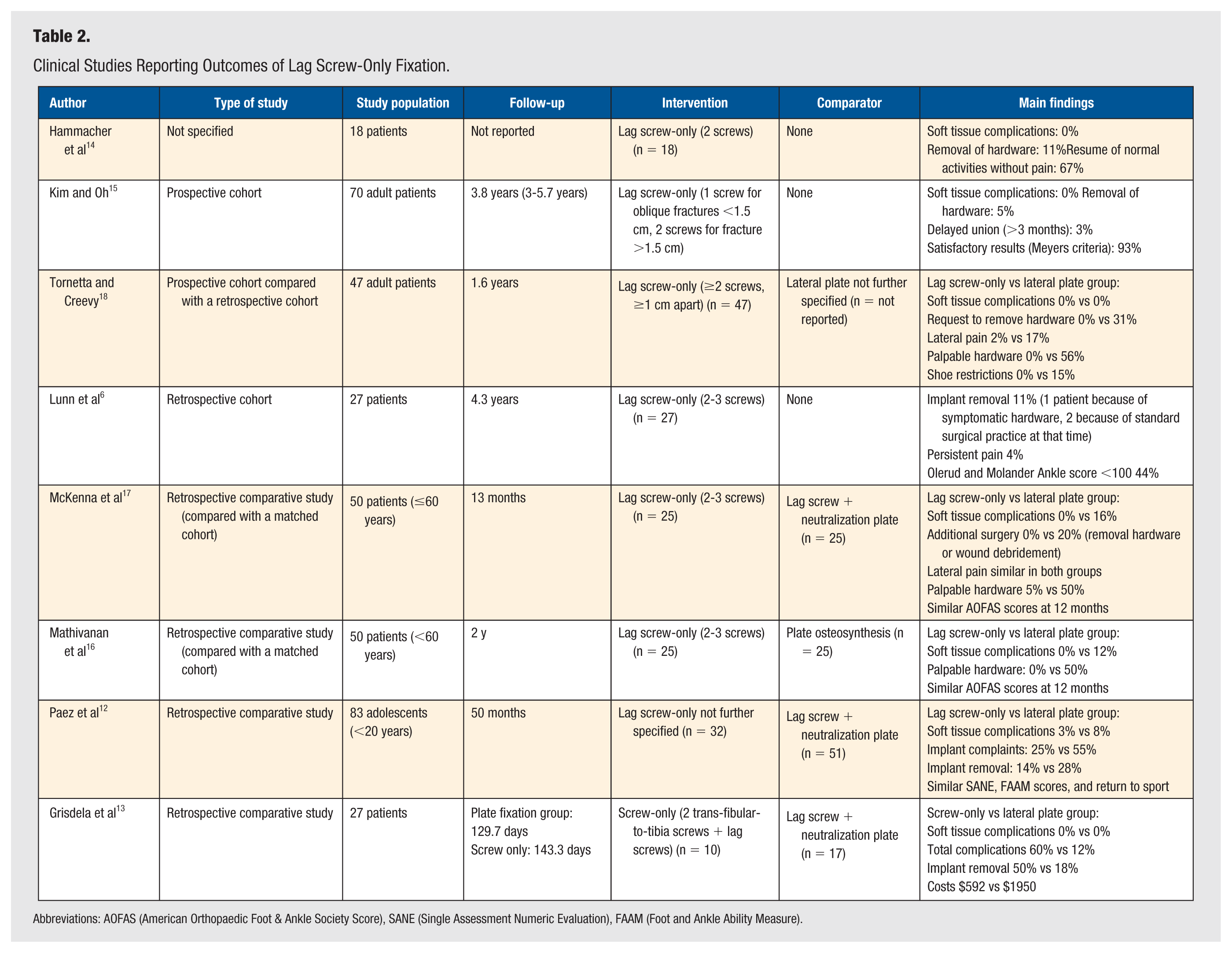
Abbreviations: AOFAS (American Orthopaedic Foot & Ankle Society Score), SANE (Single Assessment Numeric Evaluation), FAAM (Foot and Ankle Ability Measure).
Patient Selection
Included patients had simple oblique distal fibula fractures without comminution and with sufficient length for ≥2 lag screws (>20 mm or ≥1 cm spacing), predominantly Lauge-Hansen SER-type injuries. The majority of studies included patients below the age of 50 to 60 years and excluded those with known bone disease. Two studies included elderly individuals, although the median age still reflected a predominantly younger population. Paez et al 12 only included adolescent patients (<20 years or age).
Surgical Technique
In the majority of patients, a lateral incision was used to expose the fracture site, and a minimum of 2 lag screws was used. Paez et al 12 treated posterior malleolus fractures with 4 mm screws when >20% of the articular surface was involved using a posterolateral approach. Fractures of the medial malleolus were treated with open reduction and internal fixation (reported in 2 studies) or based on surgeon’s preference, not further specified (1 study). In the studies with comparison groups, they consisted of patients with a lateral plate fixation (in 2 studies further specified as an interfragmentary lag screw combined with a neutralization plate). In terms of technical tips, several reports have emphasized that well-positioned lag screws—perpendicular to the fracture line and ideally with a safe-zone trajectory aiming toward the medial edge of the Achilles tendon 19 —can maintain reduction under physiological loading conditions.1,2,11
Postoperative Treatment
Adult patients wore a splint or cast for up to 6 weeks, while adolescents had it for 2 to 6 weeks. Weight bearing began between 2 and 6 weeks, and it was mostly done protected using a cast. However, not all studies clearly specified whether the cast was maintained at the time weightbearing began. Regarding postoperative ankle mobilization, most applied a conservative protocol with immobilization for 4 to 6 weeks before initiating active range of motion. 6 ,12 -18 Interestingly, a letter to the editor by Lindsjö 20 describes a more aggressive rehabilitation strategy. The author reports allowing full weightbearing from the second or third postoperative day under plaster protection and initiating early unloaded joint exercises within the first 48 hours. This approach is based on the premise that restoring ankle congruence permits early functional recovery.
Postoperative Results
A union rate of 100% was achieved in both the lag screw-only group and the comparison group in all studies. 6 ,12 -18 In terms of functional outcomes, studies that assessed recovery using validated scales (OM, FAAM, SANE) report excellent results with lag screw fixation. Functional limitations such as persistent pain during stair climbing, stiffness, or swelling were documented in 4 patients (6.7%), primarily linked to high-energy trauma or delayed surgical intervention in the study by Kim and Oh. 15 Hammacher et al 14 reported that 17 out of 18 patients achieved good or excellent outcomes following osteosynthesis with 2 lag screws.
As for return to sport, Lunn et al 6 found that although young athletes reached maximal functional scores postoperatively, only 54% returned to their previous level, mainly due to lack of confidence or mild discomfort. In contrast, Paez et al 12 reported a 95% return-to-sport rate in adolescents treated with lag screws, compared to 86% in the plating group.
Complications
Wound-related complications were reported in 3 studies. McKenna et al 17 documented a 16% surgical site infection rate in the plating group compared to 0% in the lag screw-only group. Paez et al 12 noted an 8% rate of wound dehiscence in the plating group and none in the lag screw-only cohort. Mathivanan et al 16 reported 3 infections among 24 patients, all in the plating group, although limited methodological detail reduces the strength of their conclusions.
Secondary surgeries—primarily implant removal or management of wound issues—were variably reported across studies. McKenna et al 17 found that 20% of plated patients required reoperation, while none in the lag screw-only group did. Paez et al 12 reported a 6% secondary surgery rate in the lag screw-only group (removal of osteosynthesis material of the medial malleolus and wound-related problems). In the plating group, secondary procedures were solely for implant removal, although their incidence was not reported.
Grisdela et al 13 reported a 17.6% rate of additional surgeries in the standard fixation group, compared to 50% in the screw-only group. Although the screw-only cohort had a higher percentage, this may relate to a smaller sample size. A higher body mass index (BMI) was also observed in this cohort. Tornetta and Creevy 18 stated that 31% of plating patients requested hardware removal, compared to none in the screw-only group. Kim and Oh 15 reported low complication rates using lag screws without plating, similarly to Lunn et al. 6 In the series by Hammacher et al, 14 no hardware-related complications were documented, although 2 lag screws were later removed without specified indication.
Pitfalls in the placement of lag screws are: screws that are too long and interfere with the peroneal tendons 14 and screws that are placed too medial in the fibula and interfere with the fibular notch of the tibia 18 (Figure 4).
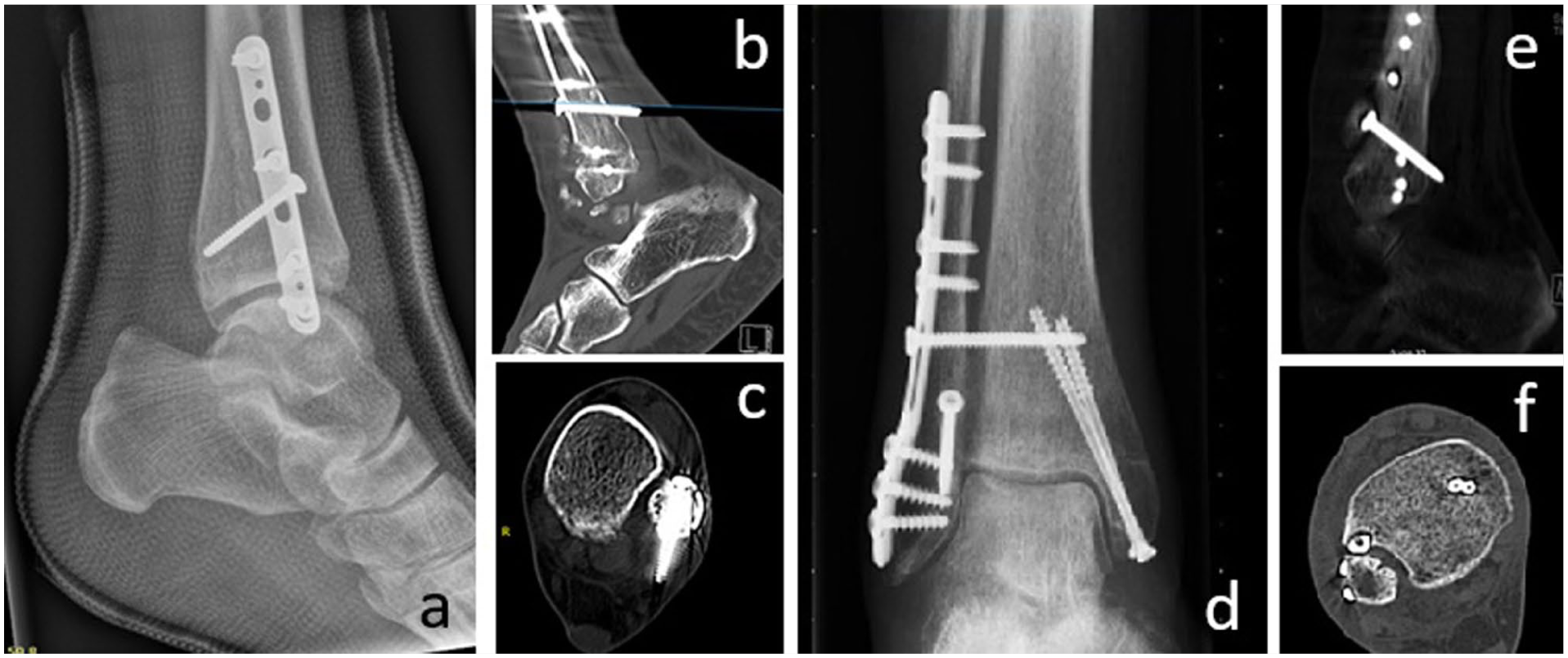
Pitfalls in the use of lag screws. (a) A too-long lag screw as seen on a conventional radiograph. (b and c) Confirmation on CT scan. (d) Close relation of the lag screw to the tibia. (e and f) Lag screw inside the fibular notch on CT scan.
Discussion
Lag screw-only fixation appears to be a viable treatment option in appropriately selected cases. Across the reviewed studies, union rates reached 100% in both lag screw-only and plating groups, with excellent functional outcomes reported using validated scales. Return to sport was also favorable: while Lunn et al 6 found that only 54% of young athletes returned to their pre-injury level—often due to psychological barriers—Paez et al 12 reported a 95% return-to-sport rate in adolescents treated with lag screws, compared to 86% in the plating group. Based on the current literature, the ideal candidate for lag screw-only fixation is a patient with a non-comminuted, simple oblique or spiral distal fibular fracture (typically Danis-Weber type B or Lauge-Hansen SER pattern) with a fracture line long enough to accommodate at least 2 perpendicular (and preferably 3) lag screws.
However, we must acknowledge the limitations of our study, particularly in relation to the heterogeneity of the available literature. Although most reports focused on non-comminuted oblique distal fibular fractures, fracture patterns and associated injuries were not entirely uniform. Surgical techniques also varied, especially regarding the number and diameter of lag screws—2 or 3 screws may offer greater interfragmentary compression and stability but can require slightly larger incisions and greater technical precision than a single-screw construct. These factors do not negate the positive outcomes reported for lag screw-only fixation but rather suggest cautious interpretation and highlight the need for future research with more consistent methodology.
Moreover, while contemporary fracture management promotes fixation that tolerates early mobilization and weightbearing, none of the studies reviewed implemented such protocols, with the exception of a letter to the editor describing early full weightbearing with protected immobilization. In this context, it is worth highlighting the findings of the biomechanical study by Shi et al 8 : dorsiflexion reduces fracture displacement and implant stress, while plantarflexion increases mechanical loads. These findings could support postoperative protocols focused on dorsiflexion-based mobilization while limiting plantarflexion in the early phases. However, as this evidence derives from biomechanical studies and anecdotal reports, its clinical translation warrants further investigation.
With respect to the use of mini-fragment implants, our review identified biomechanical studies suggesting that mini-fragment screws in lag screw-only constructs could provide adequate stability while allowing for the placement of a greater number of screws. However, although the use of mini-fragment plates for fibula fractures has been more documented in the literature, 5 to our knowledge, no clinical studies have reported on the use of mini-fragment screws in lag screw-only constructs.
Osteoporosis is a key factor to consider, as traditional management favors the use of locking plates while avoiding interfragmentary compression due to concerns over inadequate stability and iatrogenic bone damage, especially with 3.5 mm screws. The biomechanical study by Kim et al is particularly noteworthy, as it explored a screw-only construct using bicortical 2.7 mm screws applied as position screws rather than for interfragmentary compression. The construct proved non-inferior to conventional lag screw fixation, suggesting a potential alternative in osteoporotic bone. This technique has also been described in hand bone fractures with favorable outcomes. 7
We excluded other minimally invasive fixation options such as intramedullary nails and compression screws, as well as the more recent use of nitinol staples. Although intramedullary devices have traditionally been reserved for older, lower-demand patients or for cases with soft tissue compromise, their use is increasingly expanding to younger and more active individuals. Chen et al 22 reported good outcomes using intramedullary fixation, mainly in middle-aged patients. Zhang et al 23 similarly demonstrated applicability in both elderly and middle-aged cohorts. However, intramedullary implants present limitations, including risk of malrotation and occasional need for mini-incisions to assist reduction, which could diminish their minimally invasive advantage. Lag screw-only fixation allows small incisions with direct reduction control, although no studies have compared it with intramedullary devices. Nitinol staples, widely used in foot and ankle surgery, 24 have shown promising results, 25 but limited availability and higher cost highlight the need for comparative research on indications and cost-effectiveness.
Finally, obesity remains an underexplored variable. While the fibula does not carry significant axial load during gait, 5 this load may be clinically significant in patients with elevated BMI. In the study by Grisdela et al, 13 the screw-only group had a higher average BMI and a greater rate of implant removal (50%) compared to the plating group (17.6%), although no causal relationship was established. These findings raise the hypothesis that increased body weight may influence construct tolerance, but further studies are needed.
Conclusions
Lag screw-only fixation for distal fibular fractures appears to be a viable option in carefully selected patients with simple oblique or spiral fracture patterns and adequate bone quality. Biomechanical evidence supports the use of multiple screws to improve stability, and clinical series report high union rates and favorable functional outcomes. Further high-quality clinical studies are required to validate its efficacy across broader patient populations, including those with obesity or osteoporosis. In addition, the use of mini-fragment screws in lag screw-only fixation for fibular fractures warrants further research.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Trial Registration
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
Not applicable.
Code Availability
Not applicable.