
Abstract
Introduction
Hallux rigidus is common and can be disabling for patients. Once conservative management is exhausted, surgical treatment is considered. For earlier stage hallux rigidus, cheilectomy can be offered to patients. Traditionally, open cheilectomy has been performed, but minimally invasive cheilectomy is becoming increasingly popular. The purpose of this systematic review is to compare the outcomes of minimally invasive vs open cheilectomy for hallux rigidus.
Methods
Two comprehensive literature searches of Ovid MEDLINE and EMBASE were performed for relevant publications from January 1, 1995 to April 9, 2024. Search terms focused on open and minimally invasive surgery (MIS) cheilectomy were used. All full-text, English-language, clinical studies reporting on MIS and open cheilectomy outcomes and/or complications were included. Article screening, critical appraisal, and data extraction were performed independently by 2 reviewers.
Results
Nine MIS cheilectomy studies were identified, reporting on a total of 442 patients (95 males, 214 females, and 133 not reported) with 464 feet operated on. The weighted mean age and follow-up were 50.7 ± 4.6 years and 33. 5 ±14.0 months, respectively. Fifteen open cheilectomy studies were identified, yielding 720 patients (199 males, 319 females, and 202 not specified) and 763 operated feet. The weighted mean age and follow-up was 53.2 ± 4.7 years and 64.5 ± 28.3 months, respectively. Functional outcomes are similar following open or MIS cheilectomy. The MIS cheilectomy studies reported a total of 37 complications (8.2%) and 43 revision surgeries (9.3%). Complications and revision surgery following open cheilectomy were 14.7% (n = 112) and 5.0% (n = 38), respectively. Complications following open cheilectomy were higher than with MIS cheilectomy (P = .001). However, revision surgery was found to be higher in patients following MIS cheilectomy (P = .003).
Conclusion
Surgical complications following MIS cheilectomy were found to be less common when compared to open cheilectomy. However, there may be an increased risk of revision surgery following MIS cheilectomy.
Level of Evidence:
III (systematic review of level III-IV studies)
Keywords
“The purpose of this systematic review is to compare the outcomes of minimally invasive vs open cheilectomy for hallux rigidus.”
Introduction
Symptomatic arthritis of the first metatarsophalangeal (MTP) joint has a reported prevalence of nearly 8% in individuals over the age of 50 and is the most common site of degenerative disease within the foot.1-3 Hallux rigidus, as it is commonly referred to, is characterized by pain and stiffness at the first MTP joint.2,4 This progressive pathology can lead to transfer metatarsalgia, paresthesias in the distribution of the dorsal medial cutaneous nerve (DMCN), and decreased push-off strength during gait, all of which can have a significant impact on the quality of life of patients.3,5
Hallux rigidus is commonly graded using the Coughlin and Shurnas (CS) classification 6 (see Figure 1.). Earlier stages of the disease are characterized by stiffness without pain and more severe disease presents with pain throughout the arc of motion and arthritis at the first MTP joint as well as a prominent dorsal osteophyte. 6 Less commonly used, but similar classification systems for hallux rigidus include the radiographic Hattrup and Johnson classification (grades 0-3) and Regnauld’s classification (grades 1-3) (see Supplemental Appendix 1).
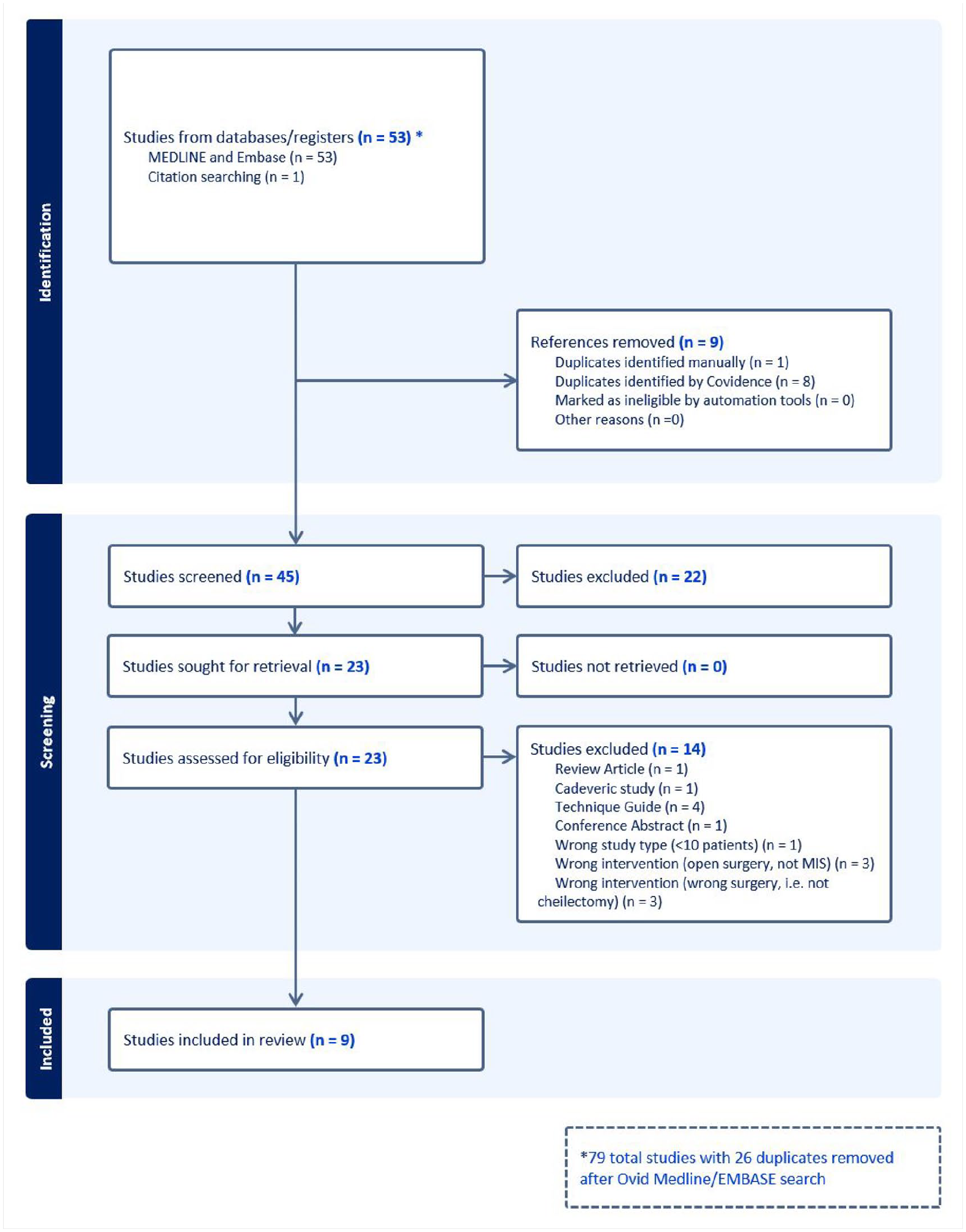
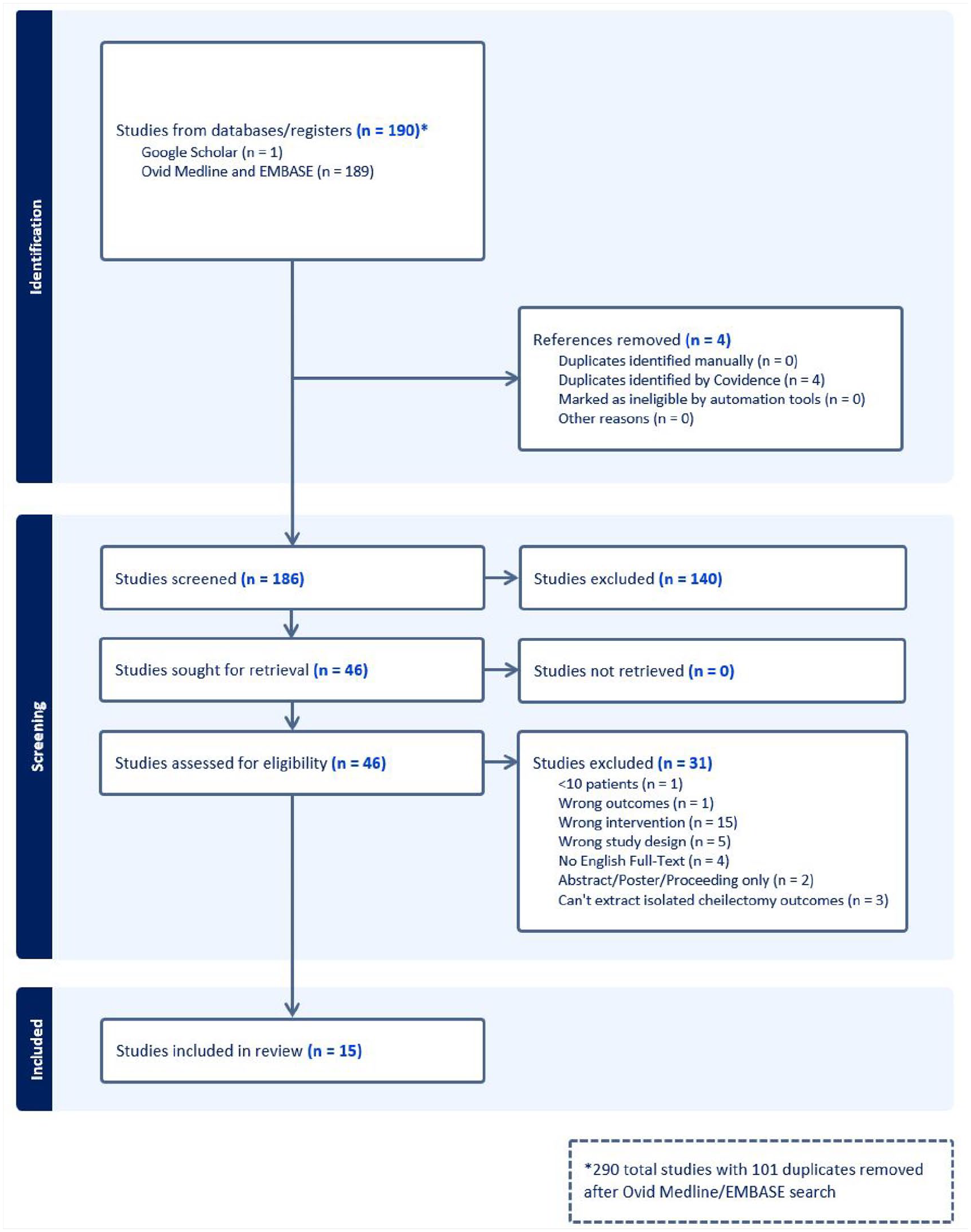
PRISMA flow diagram for MIS cheilectomy search.
Treatment of hallux rigidus initially consists of optimizing conservative management including non–steroidal anti-inflammatory medication, shoe wear modification (ie, rocker bottom sole, Morton’s extension), and intra-articular steroid injections. 7 Surgical management varies depending on the clinical symptoms and disease severity. First MTP joint arthrodesis is considered the gold standard for managing advanced disease. However, earlier disease can be successfully treated with resection of the dorsal osteophyte, otherwise known as a cheilectomy, which has traditionally been done with an open approach.
Minimally invasive surgery (MIS) has become increasingly popular within the foot and ankle subspecialty. Minimally invasive techniques have been used for many traditionally open procedures including displacement calcaneus osteotomy and hallux valgus correction. 8 Benefits such as decreased wound healing complications, improved cosmesis, and shorter postoperative recovery time have been reported with the MIS techniques.9,10 However, there have also been perioperative complications seen with the minimally invasive approaches. In the case of MIS cheilectomy, retained bone fragments, extensor hallucis longus (EHL) tendon injuries, and DMCN injuries have been reported.11,12
No studies to date have compared outcomes between the more modern MIS technique and the traditional open cheilectomy. Therefore, the aim of this systematic review is to summarize and compare the outcomes and complications seen with MIS and open cheilectomy for the surgical management of hallux rigidus.
Methods
Search Strategy
Two comprehensive systematic literature searches were performed in MEDLINE and EMBASE databases for publications from January 1, 1995, to April 9, 2024. The searches conformed with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 13 Search terms were selected in consultation with content area experts. The search focus was on hallux rigidus, cheilectomy, and either arthroscopic/MIS/percutaneous surgery or open surgery. The exact search terms used can be seen in Supplemental Appendix 2. For consistency, arthroscopic, percutaneous, and MIS were all classified under the umbrella term “MIS.”
Eligibility Criteria
All English-language peer-reviewed clinical empirical studies with a sample size ≥10 patients reporting on MIS or open cheilectomy for hallux rigidus were included. If the publication reported on multiple MIS or open procedures, the article was included if the MIS and open cheilectomy patients and their outcomes were distinguishable from other patients and/or surgical procedures or if over half of the patients in the study population underwent concomitant procedures that comprised <50% of the study population.
Abstracts, summaries of meetings, summaries of oral presentations, and papers lacking a full text were excluded. We excluded studies reporting on (1) open or MIS treatments for conditions other than hallux rigidus (ie, hallux valgus, osteochondral defects, etc); (2) cadaveric studies; and (3) less than 10 patients. Studies that did not explicitly state whether cheilectomy was performed open or MIS, or those not reporting complications were also excluded.
Study Selection
Duplicate studies were removed from the identified articles. Two reviewers independently screened the titles and abstracts for potential inclusion using Covidence software (Veritas Health Innovation Ltd, Melbourne, Australia), which facilitated screening, quality appraisal, and data collection. 14 Disagreements or discrepancies were resolved by discussion or after review with the senior author (SS-HP).
Data Extraction
Data were extracted independently by 2 reviewers using a predefined data extraction template in Covidence (Veritas Health Innovation Ltd, Melbourne, Australia). The following data were extracted when available: study author, year of publication, study design, total number of patients, age and sex of patients, length of follow-up, grade of hallux rigidus, complications, revision surgeries, postoperative range of motion, and patient-reported outcome measures (PROMs).
The primary outcomes of interest were patient-reported and functional outcome measures as well as revision surgery. The secondary outcome was complications, both intraoperative and/or postoperative.
Quality Assessment
The Joanna Briggs Institute (JBI) critical appraisal checklists for case series, case-control, and cohort studies were used for quality assessment of the corresponding study type. Two reviewers independently performed the quality assessment with disagreements or discrepancies resolved through discussion. Quality assessment was focused on described patient demographics, operative indications, outcomes, and complications included in the studies. The overall quality of the evidence of this review was assessed using Murad et al’s 15 approach to Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology.
Statistical Analysis
Descriptive statistics were performed on demographic variables. Continuous variables were described with mean and standard deviation, while categorical variables were presented as counts and frequencies. Student’s t-test was used to compare continuous variables, while chi-square and Fisher’s exact tests were used for categorical variables. All analyses were performed using SAS Version 9.04 (Cary, North Carolina).
Results
Minimally Invasive Surgery Cheilectomy
The initial search yielded 79 papers, with 45 undergoing screening following duplicate removal. Nine papers met the inclusion criteria and were included in the final analysis. The illustrative PRISMA flowchart is shown in Figure 1. There were seven case series, one cohort study, and one case-control study. There was one study comparing MIS to open cheilectomy; however, the open cheilectomy patients were excluding in the analysis due to the high proportion of concurrent procedures alongside cheilectomy. 11 These are summarized in detail in Supplemental Appendix 3.
From the included studies, there were 442 patients with a total of 464 feet that underwent MIS cheilectomy. The population was made up of 95 males (21.5%) and 214 females (48.4%), with 133 patients (30.0%) who did not have their sex specified. 11 The weighted mean age of patients who underwent MIS cheilectomy was 50.7 ± 4.6 years. The weighted mean follow-up for these patients across all included papers was 33.5 ± 14.0 months. The patient demographics are summarized in Table 1.
Patient Demographics of Open and MIS Cheilectomy.
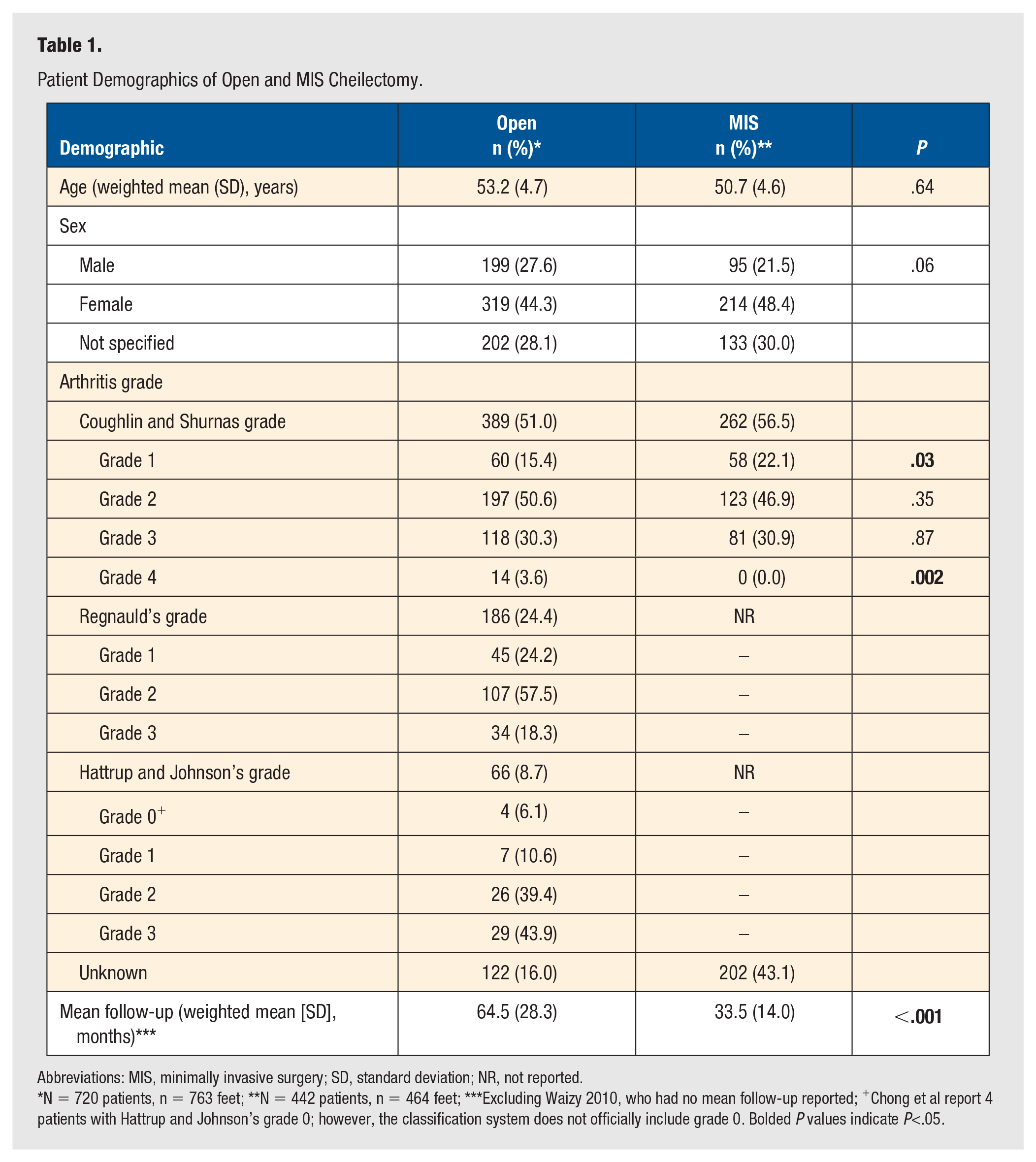
Abbreviations: MIS, minimally invasive surgery; SD, standard deviation; NR, not reported.
N = 720 patients, n = 763 feet; **N = 442 patients, n = 464 feet; ***Excluding Waizy 2010, who had no mean follow-up reported; +Chong et al report 4 patients with Hattrup and Johnson’s grade 0; however, the classification system does not officially include grade 0. Bolded P values indicate P<.05.
Of the 464 included MIS cheilectomies, 262 feet had their CS grade recorded and 202 were not reported. There were 58 (12.5%) feet graded as 1, 123 (26.5%) graded as 2, and 81 (17.5%) graded as 3. There were no reported feet with CS grade 4 hallux rigidus in the MIS cheilectomy studies (see Table 1).
Functional outcome scores reported by the studies were the American Orthopaedic Foot and Ankle Society (AOFAS) score, 16 PROMIS Physical Function score, and Manchester-Oxford Foot Questionnaire (MOxFQ).17,18 Pastides et al 16 stated their mean AOFAS was 87.1 in their cohort of 41 patients. Mean MOxFQ scores were 30.5 and 22.4 for the case series by Teoh et al 18 and Gauthier et al, 17 respectively. DiGiovanni et al reported a PROMIS Physical Function total score 19 and change score of 51.9 ± 8.5 and 2.8 ± 8.7, respectively. 20 Overall satisfaction was found to be high within the two included studies that reported on this parameter.21,22 A summary of the PROMs is presented in Table 2.
Open and MIS Cheilectomy Summary of Standardized Functional Outcomes.
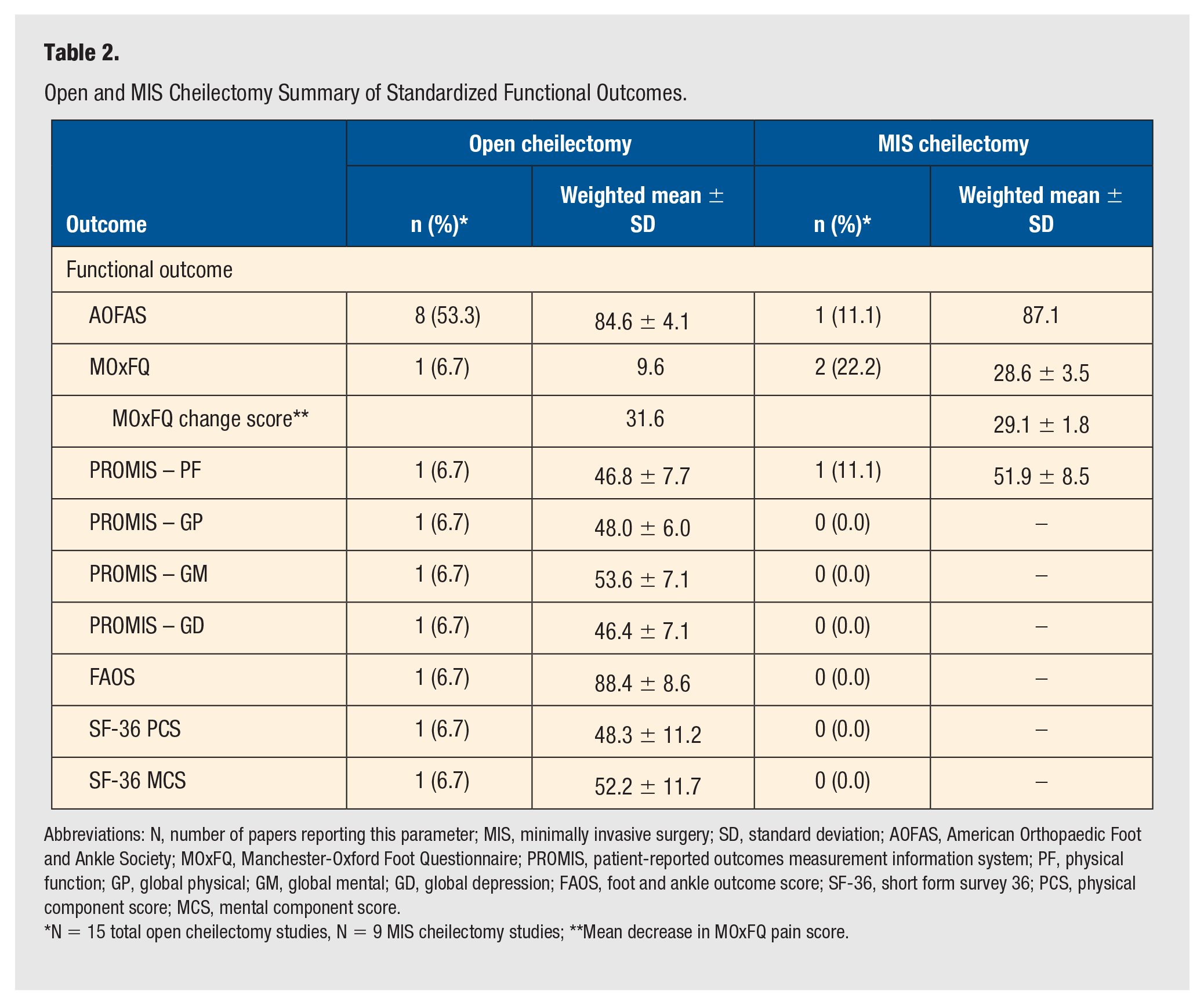
Abbreviations: N, number of papers reporting this parameter; MIS, minimally invasive surgery; SD, standard deviation; AOFAS, American Orthopaedic Foot and Ankle Society; MOxFQ, Manchester-Oxford Foot Questionnaire; PROMIS, patient-reported outcomes measurement information system; PF, physical function; GP, global physical; GM, global mental; GD, global depression; FAOS, foot and ankle outcome score; SF-36, short form survey 36; PCS, physical component score; MCS, mental component score.
N = 15 total open cheilectomy studies, N = 9 MIS cheilectomy studies; **Mean decrease in MOxFQ pain score.
Seven papers reported on pain outcomes, with three studies using the visual analogue scale (VAS), three using a Likert scale, and one using the PROMIS Pain Intensity and Interference scores. Reported mean VAS were ≤3.0 indicating no pain.12,17,18 These are summarized in Table 3.
Open and MIS Cheilectomy Summary of Standardized Pain and Range of Motion Outcomes.
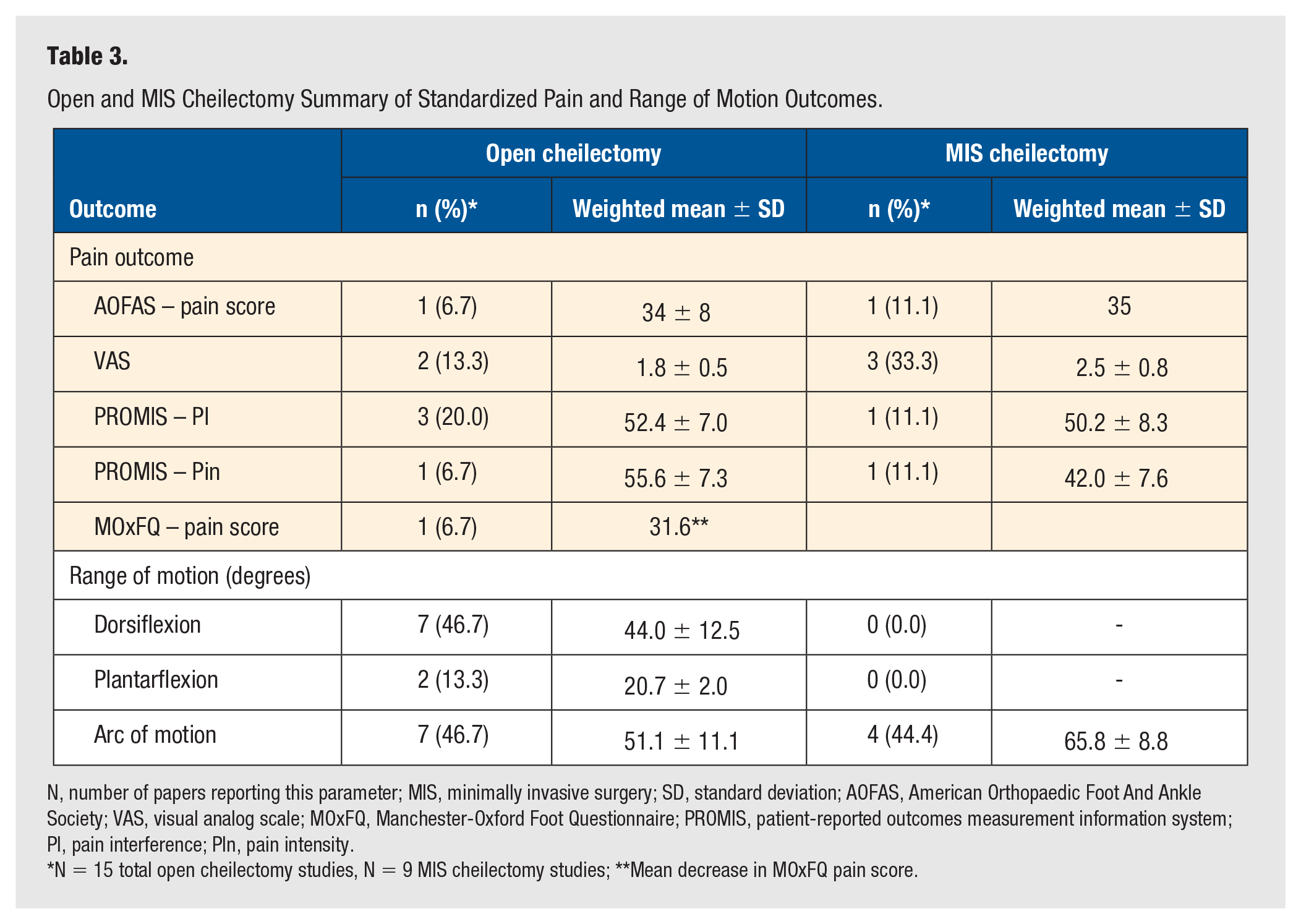
N, number of papers reporting this parameter; MIS, minimally invasive surgery; SD, standard deviation; AOFAS, American Orthopaedic Foot And Ankle Society; VAS, visual analog scale; MOxFQ, Manchester-Oxford Foot Questionnaire; PROMIS, patient-reported outcomes measurement information system; PI, pain interference; PIn, pain intensity.
N = 15 total open cheilectomy studies, N = 9 MIS cheilectomy studies; **Mean decrease in MOxFQ pain score.
Revision surgery was performed in 43 patients (9.3%) at the time of follow-up. This was most often in the form of a revision to arthrodesis (n = 23, 4.7%) or a revision cheilectomy (n = 15, 3.2%). Two patients (0.4%) required a subsequent hallux valgus correction, two patients underwent EHL primary repair, and one patient (0.2%) underwent a subsequent interpositional arthroplasty (Supplemental Appendix 4).
The overall complication rate pooled across all studies was 8.2% (n = 37). The most common complication was injury to the DMCN (n = 9, 1.9%), with its effects most reported as transient (n = 5, 55.6%), rather than permanent (n = 4, 44.4%). Residual stiffness of the first MTP joint and persistent pain following MIS cheilectomy was also common, each affecting seven patients (1.5%). Less common complications included delayed wound healing (n = 4, 0.9%), EHL injury (n = 3, 0.6%), infection (n = 2, 0.4%), retained bony fragments (n = 2, 0.4%), and neuropathic pain/complex regional pain syndrome (CRPS) (n = 2, 0.4%).
The revision surgeries and complications are listed in Table 4.
Revision Surgery and Complications Following Open and MIS Cheilectomy.
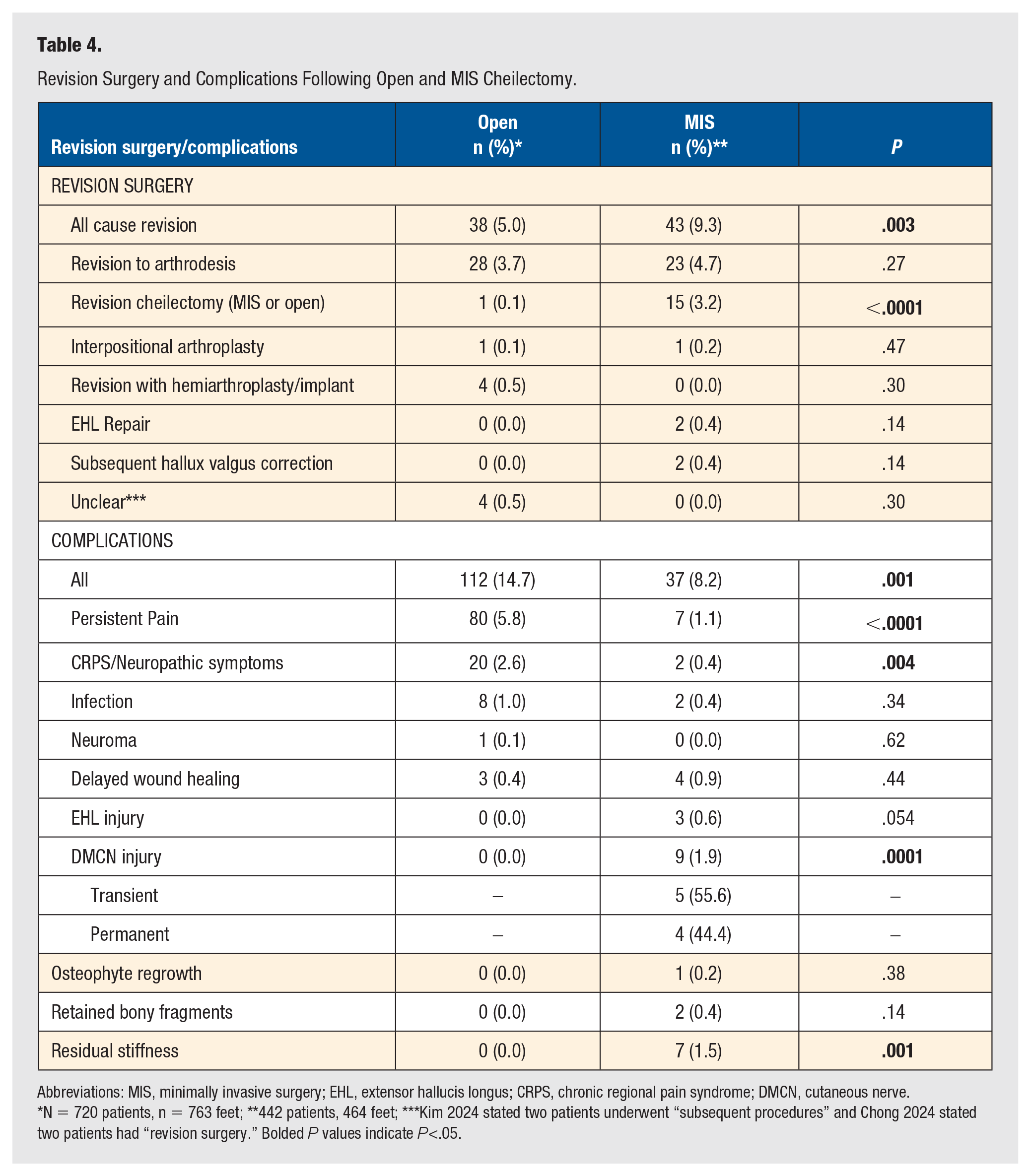
Abbreviations: MIS, minimally invasive surgery; EHL, extensor hallucis longus; CRPS, chronic regional pain syndrome; DMCN, cutaneous nerve.
N = 720 patients, n = 763 feet; **442 patients, 464 feet; ***Kim 2024 stated two patients underwent “subsequent procedures” and Chong 2024 stated two patients had “revision surgery.” Bolded P values indicate P<.05.
The results of the JBI critical appraisals are summarized in Table 5. Overall, the study quality of the included studies was good. Most of the case series, the single case-control, and cohort studies scored 8 out of 10 (11 for cohort studies) on the quality criteria or higher. The quality of the evidence according to the adapted GRADE methodology is reported in Table 6.
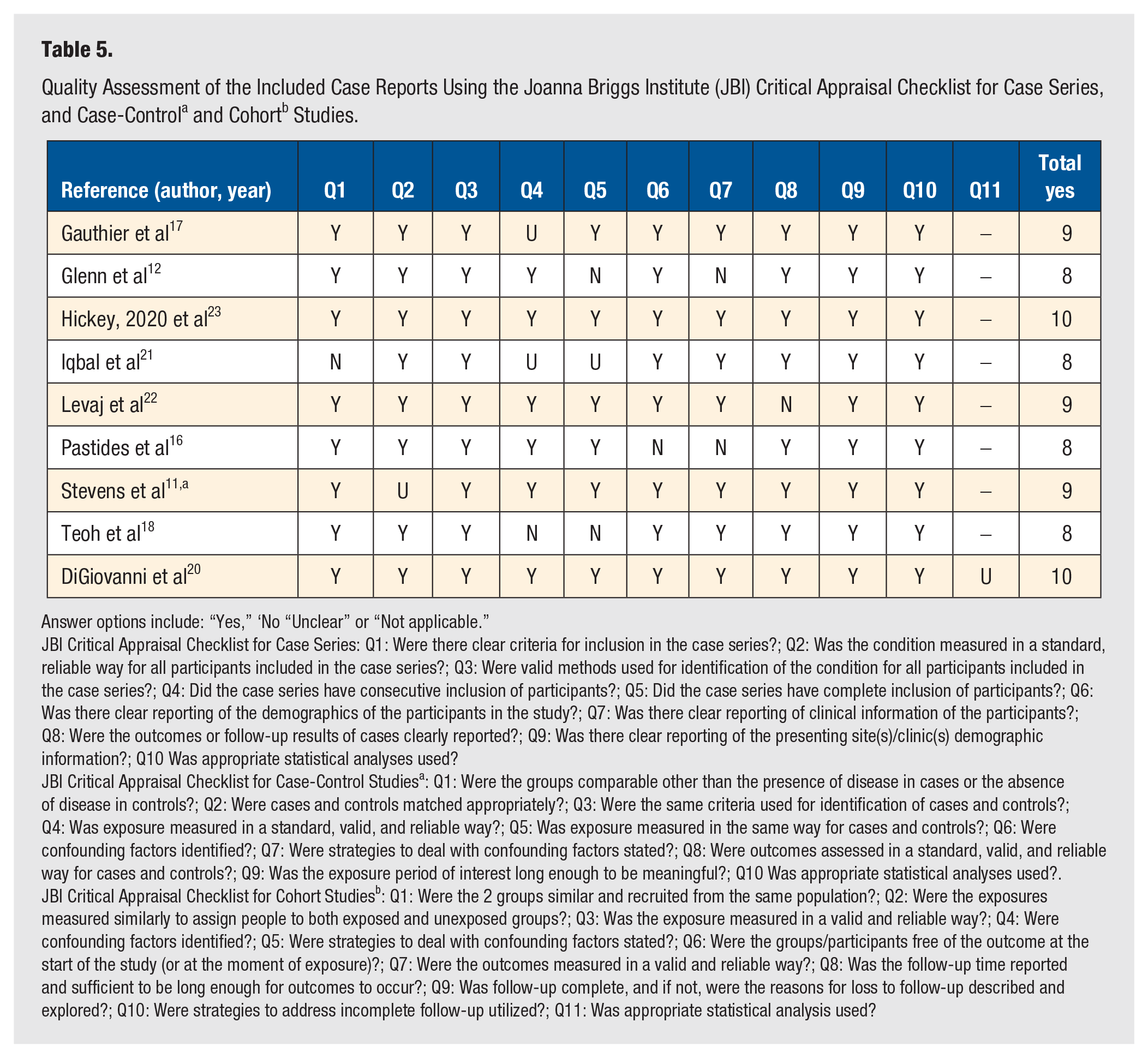
Answer options include: “Yes,” ‘No “Unclear” or “Not applicable.”
JBI Critical Appraisal Checklist for Case Series: Q1: Were there clear criteria for inclusion in the case series?; Q2: Was the condition measured in a standard, reliable way for all participants included in the case series?; Q3: Were valid methods used for identification of the condition for all participants included in the case series?; Q4: Did the case series have consecutive inclusion of participants?; Q5: Did the case series have complete inclusion of participants?; Q6: Was there clear reporting of the demographics of the participants in the study?; Q7: Was there clear reporting of clinical information of the participants?; Q8: Were the outcomes or follow-up results of cases clearly reported?; Q9: Was there clear reporting of the presenting site(s)/clinic(s) demographic information?; Q10 Was appropriate statistical analyses used?
JBI Critical Appraisal Checklist for Case-Control Studiesa: Q1: Were the groups comparable other than the presence of disease in cases or the absence of disease in controls?; Q2: Were cases and controls matched appropriately?; Q3: Were the same criteria used for identification of cases and controls?; Q4: Was exposure measured in a standard, valid, and reliable way?; Q5: Was exposure measured in the same way for cases and controls?; Q6: Were confounding factors identified?; Q7: Were strategies to deal with confounding factors stated?; Q8: Were outcomes assessed in a standard, valid, and reliable way for cases and controls?; Q9: Was the exposure period of interest long enough to be meaningful?; Q10 Was appropriate statistical analyses used?.
JBI Critical Appraisal Checklist for Cohort Studiesb: Q1: Were the 2 groups similar and recruited from the same population?; Q2: Were the exposures measured similarly to assign people to both exposed and unexposed groups?; Q3: Was the exposure measured in a valid and reliable way?; Q4: Were confounding factors identified?; Q5: Were strategies to deal with confounding factors stated?; Q6: Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)?; Q7: Were the outcomes measured in a valid and reliable way?; Q8: Was the follow-up time reported and sufficient to be long enough for outcomes to occur?; Q9: Was follow-up complete, and if not, were the reasons for loss to follow-up described and explored?; Q10: Were strategies to address incomplete follow-up utilized?; Q11: Was appropriate statistical analysis used?
The Certainty of Evidence Rated Using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach.
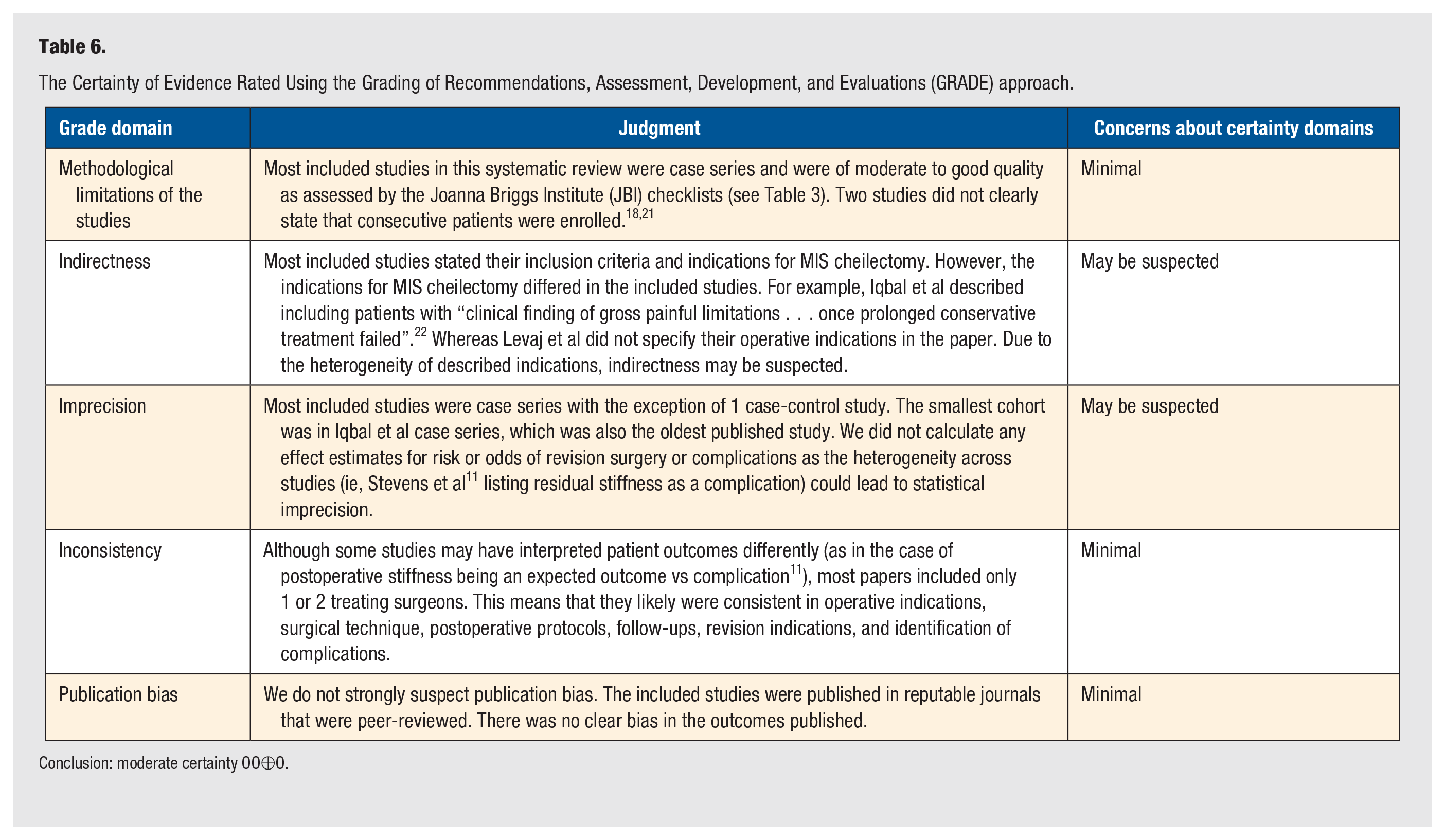
Conclusion: moderate certainty OO⊕O.
Open Cheilectomy
The search yielded 291 total studies with 105 duplicates, leaving 186 studies for screening. Fifteen papers met the inclusion criteria and were included in the final analysis. These consisted of five cohort studies and 10 case series. The illustrative PRISMA flowchart is shown in Figure 2.
PRISMA flow diagram for OPEN cheilectomy search.
From the included studies, there were a total of 720 patients and 763 feet that underwent open cheilectomy. The open cheilectomy population was made up of 199 males (27.6%) and 319 females (44.3%), with 202 patients (28.1%) who did not have their sex specified in the studies. 11 The weighted mean age of patients who underwent open cheilectomy was 53.2 ± 4.7 years, similar to the MIS group (P = .64). The weighted mean follow-up for these patients across all included papers was 64.5 ± 28.3 months, which was longer than in the MIS cheilectomy population (P<0.001). The patient demographics are summarized in Table 1.
Of the 763 included open cheilectomies, 641 had their arthritis graded by one of 3 classifications: CS (n = 389, 51.0%), Regnauld’s (n = 186, 24.4%), and Hattrup and Johnson’s (n = 66, 8.7%). One-hundred twenty-two (16.0%) were not graded. The arthritis grades for the open cheilectomy patients are reported in Table 1. Of the patients with their arthritis graded with the CS classification, there were a larger proportion of patients with grade 4 who underwent open cheilectomy compared to MIS (P = .002).
Functional outcome scores varied across the 10 papers that reported PROMs. The PROMs reported included PROMIS, 20 AOFAS, 6 ,24-30 MOxFQ, 31 and a Likert scale (Table 2). 32 Overall satisfaction was found to be high within the nine studies that reported on this parameter.6,25,27,28,30,32-35
Nine papers reported on pain outcomes, with five studies using the VAS, 6 ,25-27, 34 one using the AOFAS Pain scale, 30 one using MOxFQ pain score, 31 1 using the PROMIS Pain Intensity and Interference scales, 36 and, finally, one asking whether patients experienced pain with different levels of activity. 37 Reported mean VAS was ≤3.0 indicating no pain 6 ,25-27, 34 (see Table 3.).
Revision surgery was performed in 38 patients (5.0%) at the time of follow-up, which was lower than that seen in MIS cheilectomy (P = .003). This was most often in the form of a revision to arthrodesis (n = 28, 3.7%), which was not statistically significantly different to MIS cheilectomy (P = .27). However, the rate of revision surgery was found to be higher in the MIS group compared to open (P = .003).
The overall complication rate for open cheilectomy was 14.7% (n = 112) pooled across all studies, which was higher than that seen in MIS (P = .001). The most common complication was persistent pain (n = 80, 10.5%), followed by neuropathic pain type symptoms (n = 20, 2.6%; eg, hypoesthesia, paresthesias around surgical incision, dorsal web space numbness).
The revision surgeries and complications are listed in Table 4.
The results of the JBI critical appraisals for case series and cohort studies are summarized in Table 7. Overall, the study quality of the included studies was good. Most of the cohort studies scored 8 out of 11 on the quality criteria or higher, while all case series were 8 or 9 out of 10 as per the adapted GRADE methodology. This is summarized in Table 8.
Quality Assessment of the Included Case Reports Using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Series and Cohort a Studies.
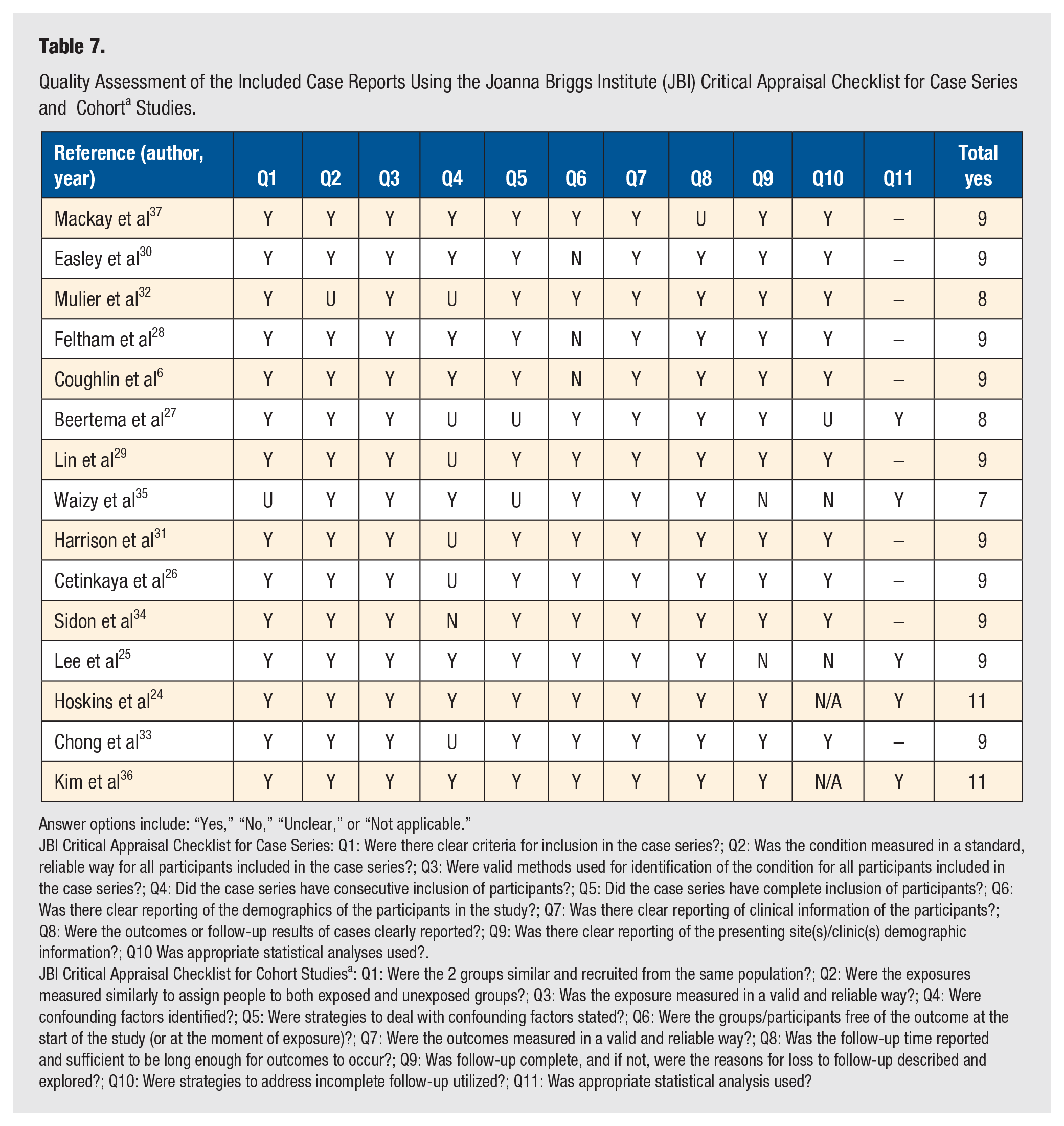
Answer options include: “Yes,” “No,” “Unclear,” or “Not applicable.”
JBI Critical Appraisal Checklist for Case Series: Q1: Were there clear criteria for inclusion in the case series?; Q2: Was the condition measured in a standard, reliable way for all participants included in the case series?; Q3: Were valid methods used for identification of the condition for all participants included in the case series?; Q4: Did the case series have consecutive inclusion of participants?; Q5: Did the case series have complete inclusion of participants?; Q6: Was there clear reporting of the demographics of the participants in the study?; Q7: Was there clear reporting of clinical information of the participants?; Q8: Were the outcomes or follow-up results of cases clearly reported?; Q9: Was there clear reporting of the presenting site(s)/clinic(s) demographic information?; Q10 Was appropriate statistical analyses used?.
JBI Critical Appraisal Checklist for Cohort Studiesa: Q1: Were the 2 groups similar and recruited from the same population?; Q2: Were the exposures measured similarly to assign people to both exposed and unexposed groups?; Q3: Was the exposure measured in a valid and reliable way?; Q4: Were confounding factors identified?; Q5: Were strategies to deal with confounding factors stated?; Q6: Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)?; Q7: Were the outcomes measured in a valid and reliable way?; Q8: Was the follow-up time reported and sufficient to be long enough for outcomes to occur?; Q9: Was follow-up complete, and if not, were the reasons for loss to follow-up described and explored?; Q10: Were strategies to address incomplete follow-up utilized?; Q11: Was appropriate statistical analysis used?
The Certainty of Evidence Rated Using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach.
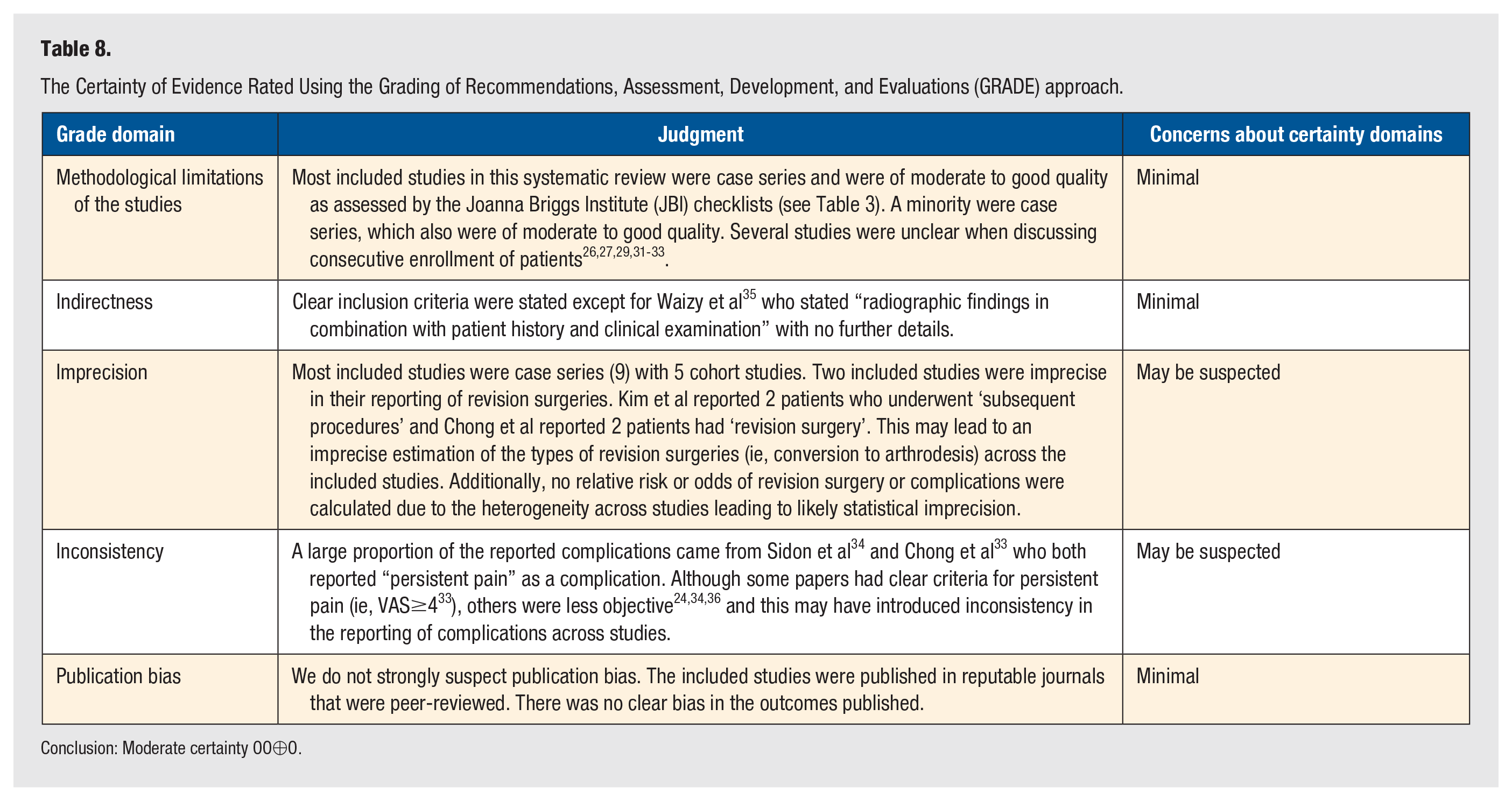
Conclusion: Moderate certainty OO⊕O.
Discussion
Minimally invasive surgical techniques are becoming increasingly popular within foot and ankle surgery. A large reason for this is that they have been shown to decrease soft tissue complications and reduce recovery times.11,18,38,39 The results of this systematic review demonstrated a higher proportion of complications in patients undergoing open cheilectomy compared with those having a minimally invasive approach for hallux rigidus. However, patients who underwent MIS cheilectomy had a higher rate of revision surgery than seen with open cheilectomy.
The all-cause rate of revision surgery of 9.3% demonstrated in the MIS cheilectomy patients was found to be statistically significant and higher than the 5.0% seen in patients who underwent an open approach. For both MIS and open approaches, the most common surgical revision was conversion to first MTP joint arthrodesis. Despite the open cheilectomy group having a longer mean follow-up than the MIS group, there was a similar proportion of patients undergoing conversion to arthrodesis. This finding is consistent with what is already known. While the dorsal cheilectomy procedure for hallux rigidus helps to improve range of motion of the first MTP joint, it does not address the arthritic joint itself. Thus, finding no difference in rates of revision to joint arthrodesis between the two surgical techniques is not surprising and understandable. However, the main reason for the higher rate of revision surgery with MIS cheilectomy was due to the need for secondary revision cheilectomy. Specifically, 3.2% of patients who underwent MIS cheilectomy underwent a revision cheilectomy, when compared to only 0.1% in the open group. This suggests that the MIS technique may lead to inadequate resection of the dorsal osteophyte(s) requiring revision surgery when compared to the open approach. Patients should be made aware of the risk of revision cheilectomy with the MIS technique.
This systematic review found the PROMs such as AOFAS and PROMIS did not differ between the MIS and open approaches. 16 -18,24,28,31 However, due to the heterogeneity and the insufficient numbers, the data could not be pooled to perform a statistical comparison. The MOxFQ scores appeared different between the open and MIS approaches. However, when preoperative MOxFQ scores are taken into account, the change scores were similar between both groups.17,18,31 In general, there was good to excellent patient satisfaction with both procedures.6,25,27,28,30,32-35 Pain outcomes using the VAS, AOFAS, and PROMIS (pain intensity and interference) pain scores were also similar between both groups, but the heterogeneity in reporting also precluded statistical comparison. The findings suggest both MIS and open procedures achieve similar clinical outcomes and patient satisfaction.
There have been some concerns regarding the potential for a higher risk of complications with MIS cheilectomy when compared to the open approach. 40 The case-control study by Stevens et al 11 reported a complication rate of 11.3% in their MIS group compared to 2.8% in their open cheilectomy group (P = .059). This reported difference is likely in part due to the small sample size of their open cheilectomy group of 38 patients, while their MIS cheilectomy group was comprised of 133 patients. Of note, the study by Stevens et al did not meet the criteria for inclusion in the open cheilectomy group in our systematic review due to the high proportion of patients who underwent ancillary procedures in addition to the open cheilectomy.
When examining the rates of complications in open vs MIS cheilectomy, this systematic review found the opposite of the findings by Stevens et al. 11 Higher complications were seen in the open cheilectomy group. Two of the biggest driving factors for the high complications rates with open cheilectomy were persistent pain and CRPS or neuropathic symptoms. One reason for the higher proportion of persistent pain with open cheilectomy could be the greater proportion of severe arthritis grades within the patient population. However, the higher risk of CRPS and neuropathic symptoms seen in the open cheilectomy group is a relevant finding that surgeons can use to educate patients during the preoperative discussion.
With regard to MIS cheilectomy, our systematic review found higher rates of DMCN injury and residual stiffness. In addition, there was a 0.0% incidence of EHL tendon injury with MIS cheilectomy, compared to 0% incidence with open approaches. The higher rates of DMCN injury and EHL tendon injury are likely both related to the lack of direct visualization of these structures when doing minimally invasive surgery.41-43 A cadaveric study has described the DMCN to be at risk when using a dorsomedial stab incision. The DMCN was found to be a mean of 3.8 mm from the dorsomedial stab incision. The authors described the danger zone for damaging the DMCN to be proximal to the first MTP joint at 1/3 of the length of the metatarsal. 41 Another cadaveric study described the “clock method” for identifying potential sites where the DMCN could be at risk. The authors determined that the DMCN and dorsolateral digital nerve were always found between 10 o’clock and 2 o’clock positions regardless of foot laterality. 42 Surgeons should utilize caution where the DMCN is at risk intraoperatively, and patients should also be made aware of the potential for DMCN injury with the MIS cheilectomy procedure.
Interestingly, we found there was a higher rate of residual stiffness after MIS cheilectomy compared to open cheilectomy. One explanation for this is that retained bony fragments may occur following MIS cheilectomy and have been postulated to contribute to persistent pain and arthritic progression.11,18 Some advocate for MIS cheilectomy to be performed concurrently with first MTP joint arthroscopy to facilitate visualization and removal of the bony debris. 12 Combining MIS cheilectomy with first MTP joint arthroscopy could help minimize retained bony debris.
It is important to note that the mean follow-up was much longer in the open cheilectomy patients than the MIS patients (67.8 vs 33.3 months). This may underestimate the complication and revision surgery rates for MIS cheilectomy, as some longer-term complications and/or revisions may not be represented in this population. However, this should not have influenced the rate of infection, delayed wound healing, and neuropathic symptoms following MIS cheilectomy, as these should have been adequately captured with short-term follow-up. In our systematic review, we found no differences in wound healing or infection between MIS and open cheilectomy.
The strengths of this systematic review include the analysis of a large cohort of both MIS and open cheilectomies from diverse institutions, enabling some comparisons on these common surgical interventions. To the best of the authors’ knowledge, there are only 2 studies comparing MIS and open cheilectomy in the current literature.11,44 In 1 study, over 50% of patients in the open cheilectomy had concomitant procedures, which could affect complication and revision surgery rate. 11 The second study comparing open to MIS cheilectomy is a published abstract, therefore not meeting the inclusion criteria of this systematic review. 44 This is the first systematic review directly comparing MIS vs open cheilectomy that provides surgeons with the clinical outcomes and complications of each approach based on the current literature.
Another strength is the methodologically rigorous approach including a systematic literature search, data extraction, quality assessment, and amalgamation of results was utilized. The included case series, cohort studies, and single case-control study were of good quality with low uncertainty in regard to the GRADE domains included from each search.
The limitations of our systematic review were largely related to the quality of studies in the literature. All included studies were observational in nature, and mean follow-up differed between MIS and open cheilectomy papers, therefore limiting the overall level of evidence for this review. Another limitation of this systematic review was the heterogeneity of included PROMs and pain outcomes, which precluded statistical analyses for comparison of MIS versus open cheilectomy. It is also important to consider variability in the reporting of complications and revision surgery, such as persistent pain reported as a complication in some studies and not others. This inconsistency can lead to bias in the comparison of these factors in both cohorts but was included in this study in keeping with previous literature. 45
Conclusion
This systematic review demonstrates that MIS cheilectomy yields similar functional outcomes and patient satisfaction when compared to traditional open cheilectomy for patients with hallux rigidus. Complications with the MIS technique are uncommon, but DMCN injury, persistent pain, and residual stiffness are most frequently reported in addition to rarer complications such as EHL tendon injury. Subsequent revision surgery following MIS and open cheilectomy is most often conversion to first MTP joint arthrodesis, but the need for secondary revision cheilectomy is more commonly required for MIS cheilectomy. Larger case-control and cohort studies with long-term follow-up are required to study the longitudinal outcomes of MIS cheilectomy.
Supplemental Material
sj-docx-1-fas-10.1177_19386400251345538 – Supplemental material for Outcomes Following Minimally Invasive vs Open Cheilectomy for Hallux Rigidus: A Systematic Review
Supplemental material, sj-docx-1-fas-10.1177_19386400251345538 for Outcomes Following Minimally Invasive vs Open Cheilectomy for Hallux Rigidus: A Systematic Review by Caroline Cristofaro, Michael Mercier, Darius Luke Lameire, Mansur Halai, Johnny Lau and Sam Si-Hyeong Park in Foot & Ankle Specialist
Footnotes
Author Contributions
Dr SS-HP is the guarantor of the clinical content of this submission. Drs JL and MH contributed to the conception, editing, and final approval of the paper. Drs MM, DLL and CC contributed to critical analysis of the relevant literature, data collection, and drafting of the manuscript. Dr CC completed the statistical analyses. All authors agree to be accountable for all aspects of the work to ensure the integrity of the work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr MH receives educational fees for less than $5000 from Smith & Nephew and Bonesupport. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought for the present study, as it involves only secondary use of publicly available published research studies.
Informed Consent
Not Applicable.
Trial Registration
Not Applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.