
Abstract
Background
Nylon sutures are the most commonly used sutures for closing surgical wounds and require a postoperative suture removal visit. Absorbable sutures improve patient satisfaction by circumventing these visits. The primary aim of this study is to analyze wound complication rates related to wound closure using nylon and polyglactin 910 (Vicryl Rapide, Ethicon, Cincinnati, Ohio) sutures in foot and ankle surgery.
Methods
A retrospective cohort study was performed at an academic medical center between 2014 and 2020. Patients over 18 years old who underwent foot and ankle surgery with polyglactin 910 or nylon sutures were included in the study. Exclusion criteria included type I or II diabetes, active pregnancy, incarceration, and pre-existing infection. Patient demographic data, operation performed, and follow-up complications were collected for review. Descriptive statistics, bivariate logistic regression, data normalcy, and appropriate tests of significance were used to compare the rate of postoperative surgical site infections (SSIs) and wound dehiscence across the 2 groups.
Results
A total of 1242 patients met our criteria: 863 were closed with nylon sutures (69.5%) and 378 with polyglactin 910 (30.5%). There was no difference between wound complications (3.18% vs 3.69%, P = .645), wound dehiscence (1.35 vs 2.82%, P = .122), or unplanned return to operating room (infection 1.08 vs 0.587%, P = .353 and dehiscence, 0.811 vs 1.52%, P = .314) between suture types.
Conclusion
This study demonstrates no significant difference in wound complication rates after foot and ankle operations between those closed with polyglactin 910 and nylon sutures. With the potential benefits to clinic efficiency and decreased patient burden with absorbable suture use, this suggests a role for polyglactin 910 suture closures in foot and ankle surgery.
Level of Evidence:
Level III
“Nylon sutures are the most commonly used sutures for closing surgical wounds and require a postoperative suture removal visit.”
Introduction
There has been discussion among orthopaedic surgeons about the efficacy and complications of absorbable sutures vs nonabsorbable sutures in surgical wound closure. Currently, nylon sutures are the most commonly used sutures in the closure of surgical wounds. 1 Nylon consists of an inert thermoplastic polyamide and is available as a monofilament or multifilament suture. 1 When compared to other braided, nonabsorbable sutures such as silk, polyglactin, and polyester, nylon showed significantly less microbe accumulation.1,2 The lack of microbial adhesion to the nylon suture contributes to its wide use in the surgical field today.3,4 Postoperative wound complications significantly impact the patients’ quality of life, leading to an increased risk of morbidity and mortality, while also increasing the financial burden and inconveniencing the patient.5-8 Furthermore, postoperative surgical site infections (SSIs) in an inpatient setting are associated with approximately $30 000 in additional hospital costs. 9 While nylon has been compared to a variety of suture materials, postoperative wound complication rates between nylon and the braided, absorbable polyglactin 910 (Vicryl Rapide, Ethicon, Cincinnati, Ohio) have yet to be analyzed in foot and ankle procedures.
Polyglactin 910 is a dissolvable suture used in superficial wound closure.10-15 It is a synthetic copolymer made from 90% glycolide and 10% L-lactide. The suture is meant to mimic the characteristics of collagen’s performance on wound healing. 16 This specific suture typically has 50% of its tensile strength at 5 days 11 and 0% of its tensile strength at 2 weeks.11,17 Absorption is in 7 to 14 days with the sutures falling off around 10 to 14 days. 11 A randomized prospective study by Al-Qattan found that when compared to the standard Vicryl-braided suture, Vicryl Rapide had fewer complications in pediatric hand surgeries. 5 Theopold et al 14 found in a subsequent randomized prospective study on adult carpal tunnel release surgeries that there was no difference in infection or scar cosmesis between polyglactin 910 and nonabsorbable sutures. Kotaluoto et al 18 performed a randomized control trial where they found no significant difference in wound infection rates when comparing absorbable vs nonabsorbable sutures in appendectomy procedures. Absorbable sutures have also been shown to reduce staffing costs and contribute to greater overall patient satisfaction.12,19 Suture removal visits are commonplace in surgical practices where nylon sutures are utilized and must be scheduled within an appropriate timeframe. While these visits offer an opportunity for examination and follow-up, the use of sutures which do not require removal may eliminate discomfort and inconvenience to the patient.12,14,19,20
The purpose of this study is to analyze the rates of superficial and deep wound complications when comparing closure with nylon vs polyglactin 910 suture in foot and ankle procedures. The authors hypothesize that there will be no significant difference in the rate of wound complication between patients closed with each of the suture types in foot and ankle procedures.
Materials and Methods
The Institutional Review Board (IRB) approval was obtained before the start of this retrospective chart review. Electronic Medical Records of postoperative patients undergoing foot and ankle surgery at an academic institution in an outpatient setting from the years 2000 to 2020 were reviewed. Initial inquiry identified 1884 patients at our institution who underwent foot and ankle surgery and had their surgical incisions closed with either nylon or polyglactin 910 suture. Of this group, 1242 patients met inclusion and exclusion criteria and underwent further analysis. The inclusion criteria were age between 18 and 90 years old, index surgeries determined to be within the specialty of foot and ankle surgery, surgery performed by one of 2, fellowship-trained foot and ankle surgeons, and the use of either nylon suture or polyglactin 910 suture for primary wound closure. There was no minimum follow-up requirement for inclusion in this study. Exclusion criteria were nonindex surgeries, patient history of diabetes, current pregnancy, pre-existing infection involving the surgical extremity, incarceration, and patient inability to comply with postoperative follow-up requirements (Figure 1).
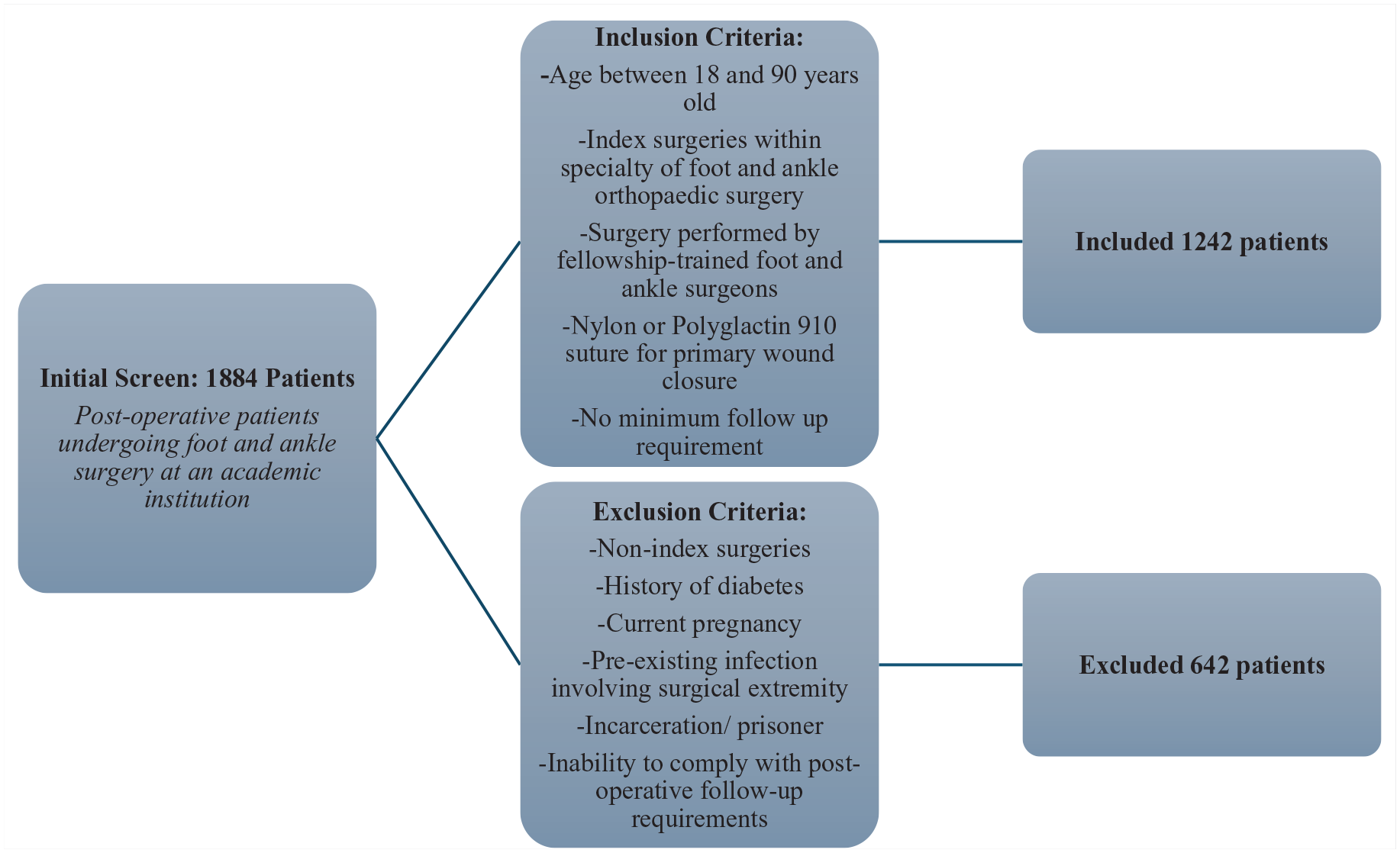
Inclusion and exclusion criteria.
For each patient included, baseline demographic data were recorded including age, body mass index (BMI), the American Society of Anesthesiologists (ASA) status, history of tobacco use, hypertension, alcohol abuse disorder, and renal failure. In addition to recording the specific procedure performed, procedures were subclassified into one of 3 groups: minimally invasive surgery (MIS), arthroscopic surgery, and open surgery. In addition, we recorded intraoperative variables including surgery duration, whether preoperative antibiotics were administered, estimated blood loss, whether an implant was used, and tourniquet time. Patients with missing data were included for analysis. Patients who did not complete follow-up as defined by the Center for Disease Control postoperative surveillance guidelines 21 were labeled as lost to follow-up (LTFU), and their average time of follow-up was calculated. Finally, we recorded whether a patient’s wounds were closed with nylon or polyglactin 910 sutures.
Descriptive statistics were used to categorize patient demographics, surgical variables, and postoperative follow-up, including the appropriate tests for normalcy and significance. Nonparametric variables were analyzed via Mann-Whitney tests. The primary outcome variable was the rate of postoperative SSIs and of wound dehiscence, including unplanned return to the operating room (UROR), which were stratified between the nylon and polyglactin 910 cohorts. Postoperative wound complications and SSI were defined using the Center for Disease Controls criteria. 21 After initial tests of significance, a secondary binary logistic regression was completed with outcomes as the dependent variable and patient demographics and surgical variables as covariates.
A post hoc power analysis was conducted to determine the required sample size for achieving 80% power, considering the observed differences in infection rates between the 2 suture groups (3.69 nylon vs 3.18 polyglactin 910), revealing that approximately 12 228 patients would be necessary to detect the modest effect sizes observed in our preliminary data. All statistical analyses were completed by the authors in SPSS (IBM, Chicago, Illinois) with a significance level of .05.
Results
Of the 1242 eligible patients from the initial 1884 identified, 863 were closed with nylon sutures (69.5%) and 378 with polyglactin 910 (30.5%). The polyglactin 910 group was significantly older at 51.4 ± 17.9 years compared to 46.3 ± 16.1 years in the nylon group (P < .001). The BMI was slightly lower in the polyglactin 910 group (27.3 ± 5.39) than in the nylon group (28.2 ± 5.79, P = .011). The ASA scores also showed a significant difference, with the polyglactin 910 group averaging 1.93 ± 0.612 and the nylon group 1.81 ± 0.617 (P = .001). The prevalence of comorbidities such as chronic kidney disease and tobacco use did not differ between the groups, except hypertension, which was higher in the polyglactin 910 group (25.9 vs 20.9%, P = .049, Table 1). A total of 29 patients were found to be missing both estimated blood loss and tourniquet time from their data. A specific type of wound closure and stitches were not recorded in patient charts; thus, it could not be analyzed in our data. Typically, the surgeons’ wound closure preference when using polyglactin 910 is simple interrupted and horizontal mattress. In open surgeries, wound closures included simple interrupted, horizontal mattress, and vertical mattress. In MIS and arthroscopic surgeries, wound closures included simple interrupted and horizontal mattress.
Comparison of Demographics.
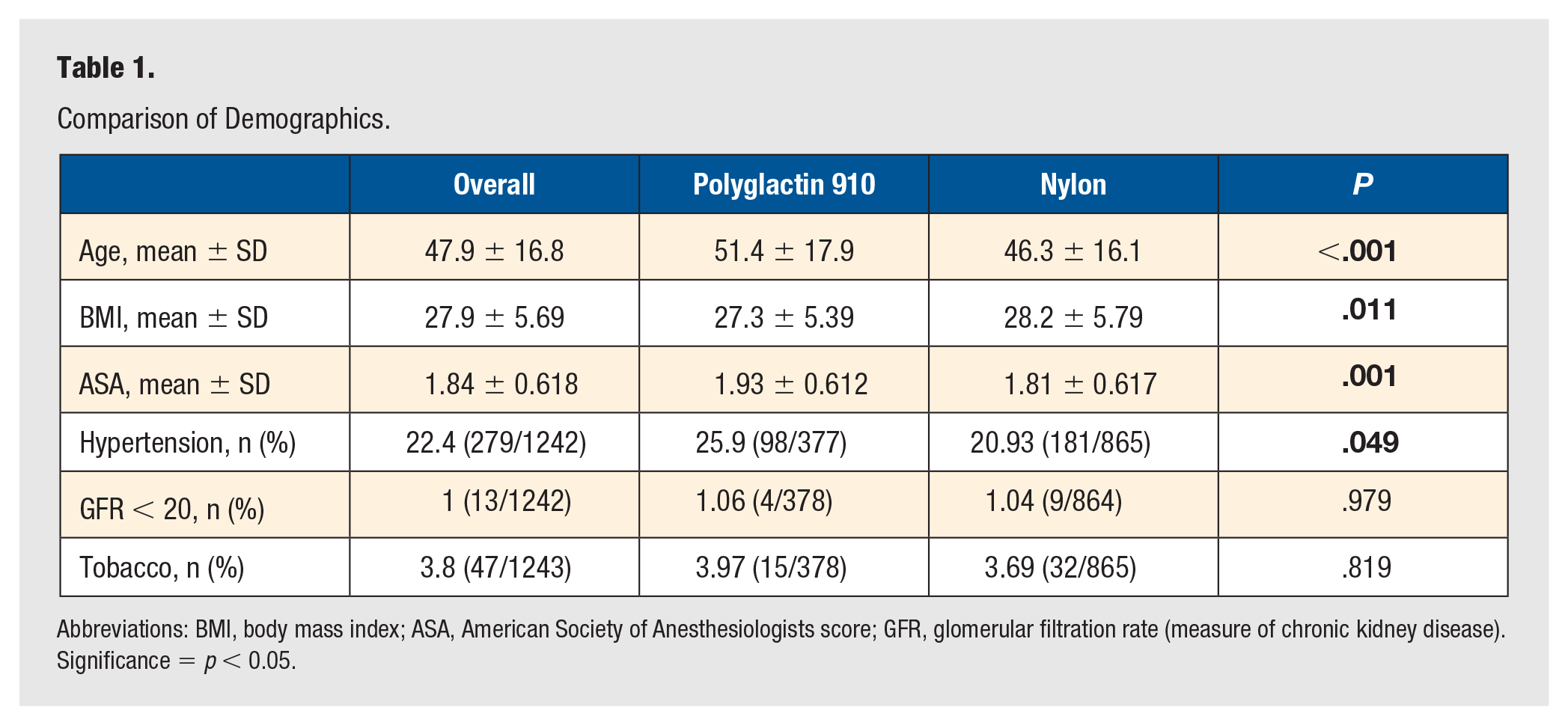
Abbreviations: BMI, body mass index; ASA, American Society of Anesthesiologists score; GFR, glomerular filtration rate (measure of chronic kidney disease).
Significance = p < 0.05.
Surgical Variables
Surgical duration was notably shorter in the polyglactin 910 group, averaging 79.9 ± 37.3 minutes, compared to 88.9 ± 38.1 minutes in the nylon group (P < .001). The study also highlighted differences in the types of surgeries performed, with arthroscopic surgeries being more common in the nylon group (23.9 vs 17.7%, P = .015), and minimally invasive surgeries (MISs) more common in the polyglactin 910 group (25.4 vs 17.4%, P < .001). In addition, the frequency of implant use was higher in the polyglactin 910 vs the nylon group (61.3 vs 42.6%, P < .001) and the administration of prophylactic postoperative antibiotics was significantly greater in the nylon group (32.6 vs 4.94%, P < .001). No open fractures were operated on in this setting. Preoperative antibiotics, blood loss, tourniquet time, and surgeon experience were comparable between the 2 groups (Table 2).
Comparison of Surgical Variables.
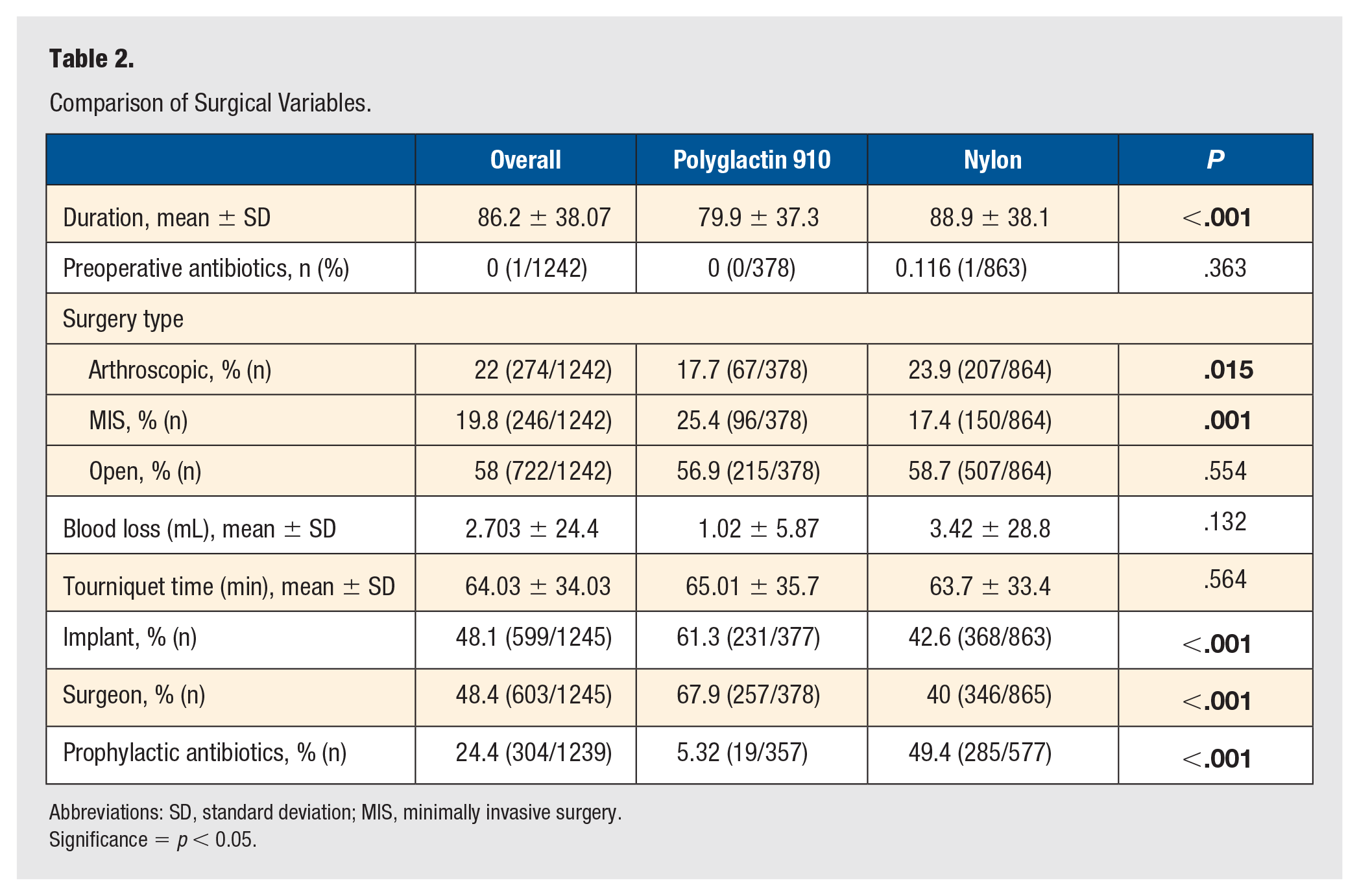
Abbreviations: SD, standard deviation; MIS, minimally invasive surgery.
Significance = p < 0.05.
Outcome Comparison
Outcome measures including any complications (3.18% vs 3.69%, P = .645), superficial SSI (1.89% vs 0.87%, P = .165) and deep SSI (0.27% vs 0.585%, P = .467), wound dehiscence (1.35% vs 2.82%, P = .122), and UROR (due to infection, 1.08% vs 0.587%, P = .353 and due to dehiscence, 0.811% vs 1.52%, P = .314) showed no difference between the polyglactin 910 and nylon groups (all values reported as polyglactin 910 vs nylon, Table 3). The time to recorded complication (in days) was different in the nylon group, although this did not reach statistical significance (28 ± 22.4 vs 32.7 ± 24.6, P = .406). A total of 27 patients did not reach the full 6 weeks of follow-up, which was different between the nylon and polyglactin 910 groups (2.31% vs 1.85%, P = .609), although again this finding was not statistically significant. Of the cohort of patients LTFU, those in the polyglactin 910 group had a significantly different follow-up time (42.1 ± 16.4 vs 24.05 ± 18.9, P = .042).
Comparison of Outcomes.
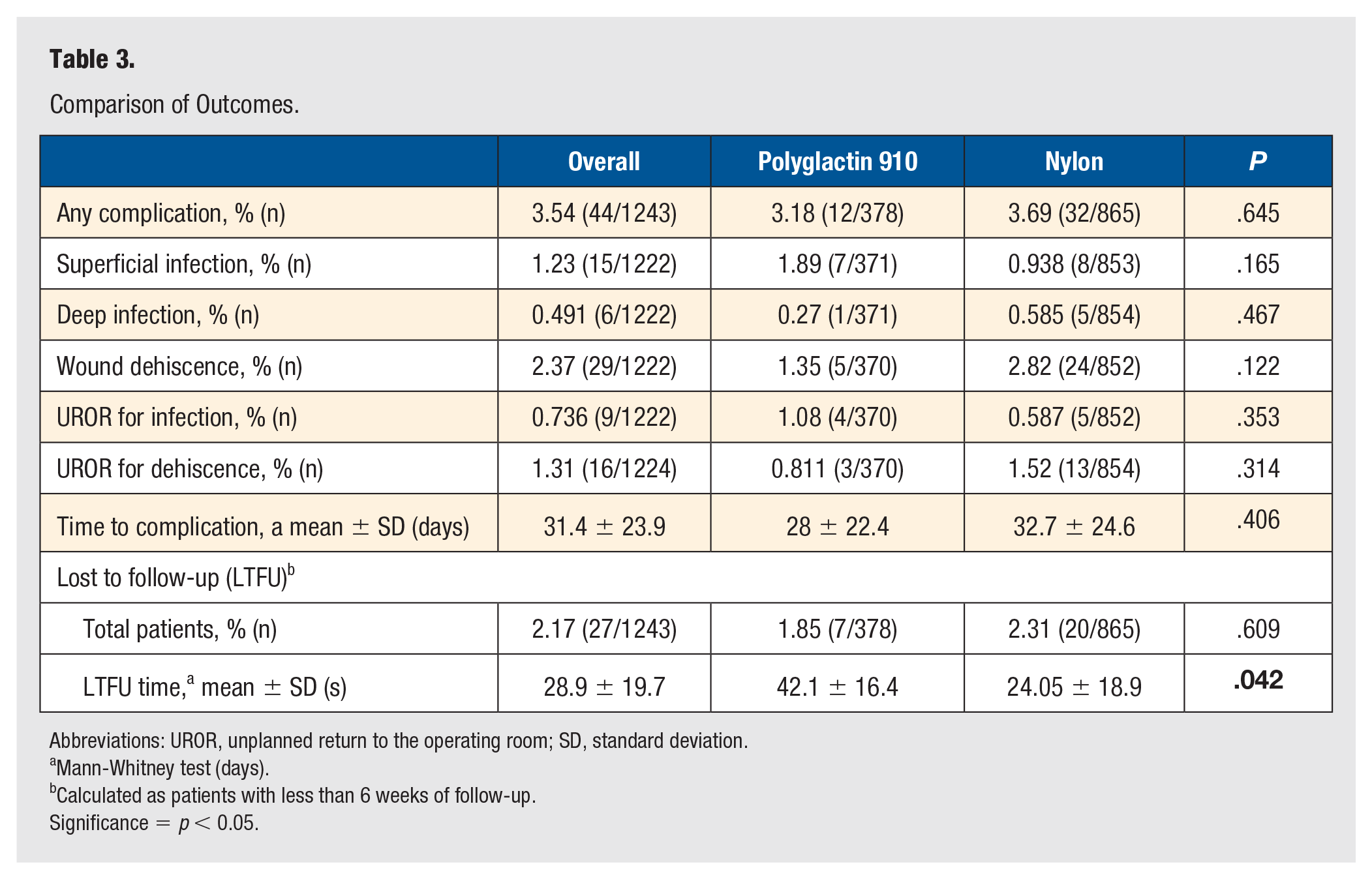
Abbreviations: UROR, unplanned return to the operating room; SD, standard deviation.
Mann-Whitney test (days).
Calculated as patients with less than 6 weeks of follow-up.
Significance = p < 0.05.
Regression Analysis
Binary logistic regression for risk factors of postoperative complications showed that patients with pre-existing kidney failure (odds ratio [OR] = 389, 95% confidence interval [CI] = 7.35-20638, P = .003) and active tobacco users (OR = 74, 95% CI = 4.34-1262, P = .003) had a higher likelihood of developing a deep infection (Table 4 and Figure 2). In addition, hypertension was noted to be a risk factor for any postoperative complication (OR = 2.26, 95% CI = 1.18-4.36, P = .015). Contrary to these factors, the type of suture material was not found to have a significant impact on postoperative acute infection (OR = 1.46, P = .734), deep infection (OR = 0.390, P = .519), or any complication (OR = 0.703, P = .358).
Regression Analysis.
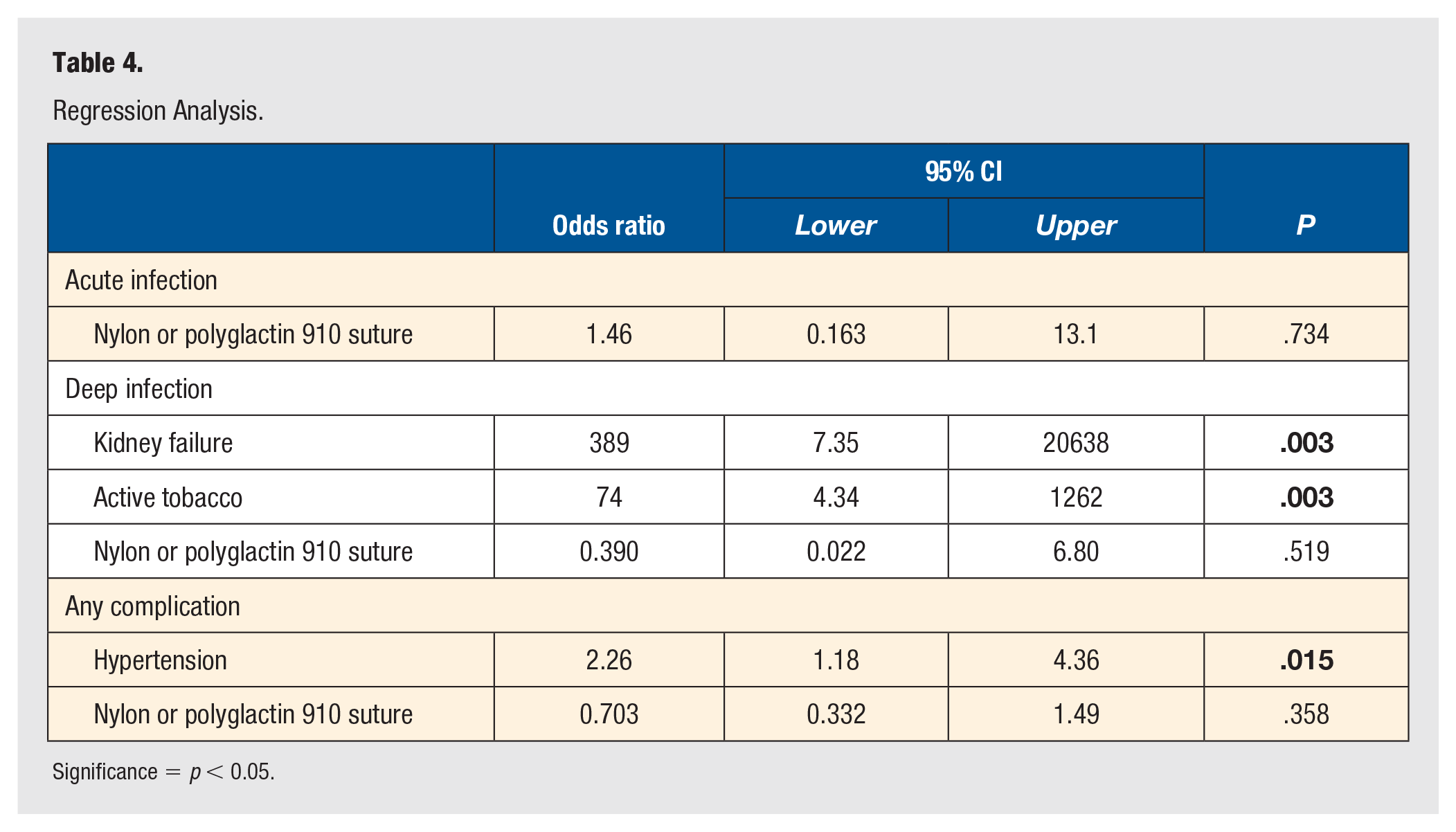
Significance = p < 0.05.
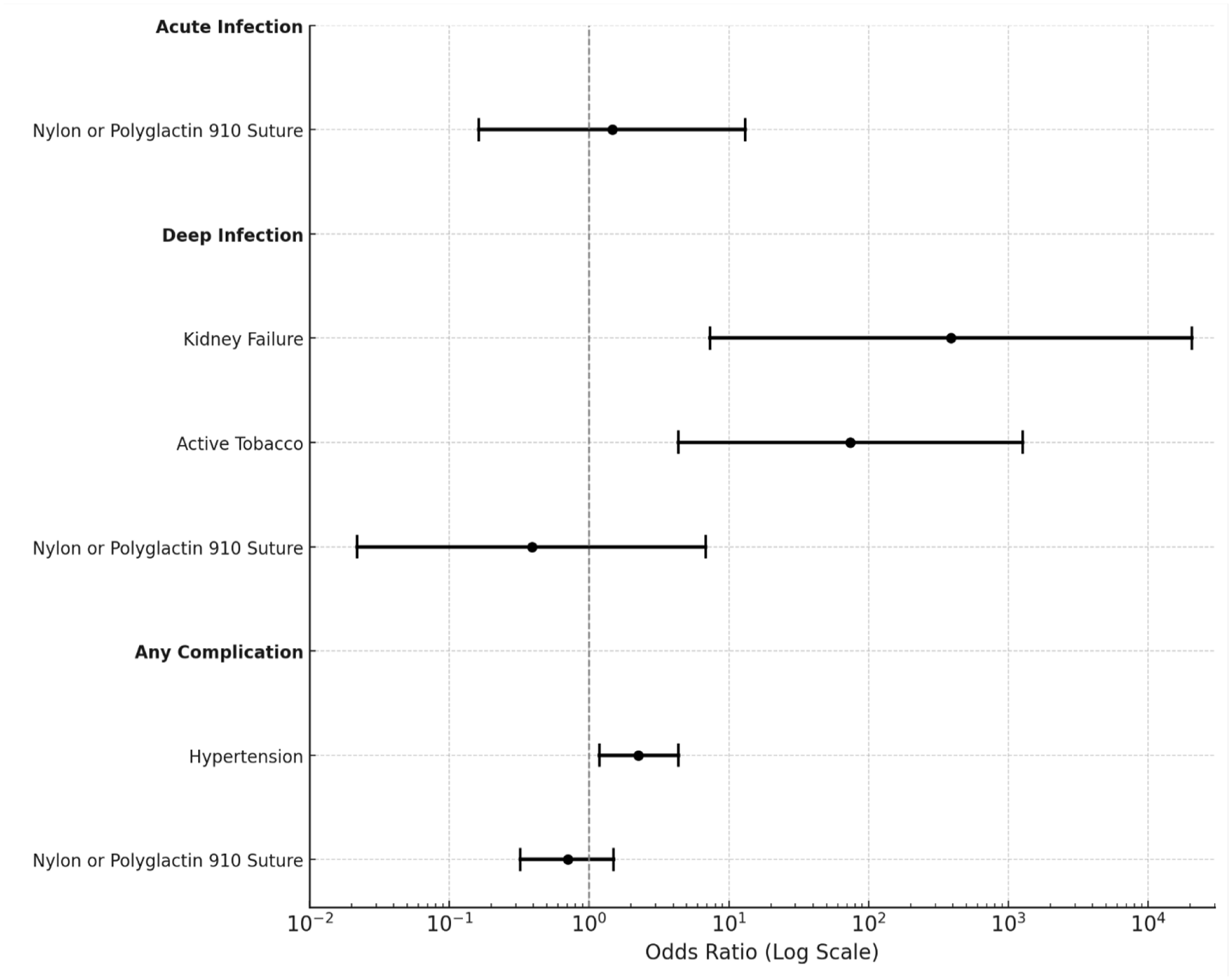
Odds ratios of regression analysis.
Discussion
To our knowledge, this is the largest study assessing surgical outcomes when comparing the use of absorbable polyglactin 910 and nonabsorbable nylon sutures for superficial closure in foot and ankle orthopaedic surgery. In general, factors such as wound healing, wound type, stitch technique, tensile strength, aesthetic of scar, and potential for local reaction are common determinants in choosing a suture material.17,22,23 Ultimately, suture is chosen based on its characteristics with the goal of a successful and uncomplicated wound closure. In situations where primary closure is difficult such as oncologic resections, collaboration with plastic surgery for soft tissue reconstruction may be required.24,25 The aim of this study was to specifically compare postoperative complications, including infection, dehiscence, and unplanned return to the OR, between nylon sutures used in foot and ankle procedures. This study demonstrates no significant difference in the incidence or severity of postoperative wound complications between polyglactin 910 and nylon sutures in our patient cohort.
Two meta-analyses comparing the morbidity of nonabsorbable sutures and absorbable sutures in skin closure across all medical specialties did not find any difference in wound infection or dehiscence, which is consistent with our findings.20,26 Our findings are also consistent with a randomized control trial performed by Yao et al 27 investigating wound closure with nonabsorbable sutures, absorbable sutures, and metallic staples in foot and ankle surgery. They analyzed 124 patients and found no significant difference in complication rates regardless of closure type. The nonabsorbable suture cohort in this study had significantly more pain at 6 weeks postoperation, and the authors suggest avoidance of use for this reason.
The study by Yao et al and the results of the present study are important in improving patient satisfaction and clinical efficiency. With potentially similar risk for postoperative wound complications when using absorbable compared to nonabsorbable sutures, absorbable sutures could offer benefits beyond wound closure. The use of absorbable rather than nonabsorbable suture may decrease overall postoperative pain for patients.7,16 Furthermore, in clinical settings that are under-resourced or serve a patient population that is in lower socioeconomic status, absorbable suture use obviates the absolute necessity for patient follow-up at the 2-week postoperative mark for removal. While an initial postoperative visit within this time frame is still recommended as it allows for examination and a check-in with the patient, the use of absorbable suture allows for more leeway in timing, which may decrease scheduling burden for both the patient and clinic. This also eradicates the potential need for last-minute clinic additions if the wound is not ready for suture removal at the time of the pre-scheduled appointment. This is encouraging as clinical efficiency and patient satisfaction could potentially be improved by rendering suture removal in the clinic unnecessary. In addition, elimination of suture removal decreases the length of time needed for initial postoperative visits and allows for improved flow and efficiency. In our own practice, we still undergo our routine 2-week postoperative visit for wound check, followed by 6-week visits for postoperative X-rays. However, the use of the polyglactin 910 suture allows for the 2-week wound check visit to require much less time and reduces the need for ancillary staff for suture removal for that particular visit. Importantly, for patients who are indeed LTFU, there is no concern for retained nonabsorbable sutures if polyglactin 910 sutures are used for closure.
Similar findings have been demonstrated in studies across other orthopaedic subspecialties, including hand and upper extremity. A retrospective review by Bridges et al 28 in 2023 examined the postoperative complications and number of visits following open trigger finger release procedures comparing absorbable and nonabsorbable sutures. When comparing the 2 suture types, like in our study, they found no significant difference between cohorts in the number of postoperative complications including superficial SSI, deep wound infections, wound complications, and number of antibiotic prescriptions. The patients who were closed with absorbable sutures had significantly fewer postoperative visits when compared to those closed with nonabsorbable sutures. A prospective cohort study by Tzimas et al 15 in 2022 examined infection rates, postoperative pain, upper extremity function, and scar cosmesis at 2 and 6 weeks following carpal tunnel surgical decompression, comparing closures between interrupted mattress nylon sutures and running subcuticular polyglactin 910. They similarly found no difference in infection rates as well as no difference in pain, upper extremity function, or scar cosmesis.
However, there is some evidence against the use of absorbable braided sutures in contaminated wounds. In an in vivo contaminated wound mouse model study by Morris et al 29 in 2017, the authors found that absorbable monofilament and barbed monofilament sutures had less bacterial adherence, biofilm formation, and tissue reactivity than absorbable braided sutures. Our study excluded patients with active infection and did not have any open fractures, which suggests absorbable braided sutures such as polyglactin 910 should be avoided in these settings.
It is important to note that due to the retrospective nature of this study, there is marked heterogeneity within our cohort, limiting our study’s generalizability. The variability in demographics between patients may influence SSI risk. Specifically, age, ASA, MIS, implant use, BMI, surgical duration, arthroscopic surgeries, and prophylactic postoperative antibiotic use all have the potential to be confounding variables. In our cohort, age, ASA, BMI, and history of hypertension were the demographic variables with significant variability between the 2 groups. In review of the literature regarding ASA and postoperative infections in operative ankle fractures, it was found that only ASA of 3 or 4 is associated with increased risk of postoperative infection.30,31 In our cohort, both the polyglactin 910 and nylon cohorts had a mean ASA <2, suggesting that ASA status is less likely to have an effect on outcomes in this study.
Similarly, a literature review of all SSIs across orthopaedic surgeries and their demographic risk factors showed that age >65 years old significantly increased the risk of postoperative infection. 32 In our cohort, the mean age of both the polyglactin 910 and nylon cohorts was <65 years old, suggesting that age could be less likely to be a confounding variable in our study. Specifically in younger populations, polyglactin 910 has been shown to be effective in pediatric hand surgery due to its rapid absorbing properties when compared to normal Vicryl sutures 10 and effective in pediatric lateral ray foot surgery by reducing pain associated with suture removal and decreasing tissue damage with no scarring complications. 12 A review conducted in 2019 by the Dutch National Surveillance Network revealed that BMI >30 significantly increased the risk for infection across all surgery types. 33 Similarly, a 2020 meta-analysis of abnormal BMI in orthopaedic trauma patients by Kinder et al 34 found overall postoperative complication rates are increased when BMI >30. Our patient cohort had a mean BMI <30, so again this is less likely to be a confounding variable in our study.
One major difference between our patient groups was the use of postoperative antibiotics, which were prescribed significantly more frequently in the nylon group. This was largely due to surgeon preference and experience with wounds that were determined to be difficult to close or located in a subjectively high-risk region. Because the tendency to prescribe antibiotics was largely subjective, it is difficult to generalize this result. However, it adds credence to our primary outcome in that even with a large number of patients receiving postoperative antibiotics in the nylon group, there was still no significant difference in overall postoperative wound complications between cohorts.
Another major difference between our groups was the use of arthroscopic and MIS techniques vs open techniques. In our study, polyglactin 910 was used significantly more often in the arthroscopic and MIS groups, and nylon was used significantly more often in the open procedures. These tendencies suggest a preference for our surgeons to use nonabsorbable sutures in patients who may have a higher subjective risk of wound complication. While overall there was no difference in postoperative complication rate between suture types, patient selection in terms of incision type may have contributed to our primary outcome.
This study has several strengths and limitations: Our post hoc analysis revealed that a larger sample size of patients would be needed to reach appropriate power; to our knowledge, this is the largest sample size comparing the outcomes of nylon vs polyglactin 910 sutures in foot and ankle surgery wound closure. In addition, our findings are consistent with the current literature across multiple orthopaedic subspecialties and operations. This is a retrospective and single-center study, which provides a lower quality of evidence and an inherent heterogeneity within patient demographic data. As with all retrospective reviews, the data analysis was limited by the thoroughness of the notes taken during the operative and postoperative periods and could be subject to unmeasured confounders. Incision/closure length and stitch type were also not recorded and could be a variable related to the wound complication rates. Due to data collection limitations, an exact percentage of open surgeries that were due to fractures potentially causing soft tissue damage could not be identified. Since data were collected from patients undergoing surgery in solely an outpatient setting, there could be some inherent patient selection bias present. Finally, there were 27 patients LTFU, which was 2.17% of the total cohort. However, this is an acceptably low number and likely did not significantly influence our results.
Conclusion
Our retrospective review of orthopaedic foot and ankle surgery patients undergoing primary wound closure with nylon vs polyglactin 910 sutures revealed no difference in the incidence of postoperative wound complications. Specifically, there was no difference in postoperative wound infections, dehiscence, or unplanned return to the operating room. This suggests that, while nylon suture is currently more commonly used for foot and ankle surgery, the use of absorbable polyglactin 910 is a safe alternative. Future studies should specifically investigate patient-reported outcome measures, clinical scheduling efficiency, larger sample size for sufficient power to detect moderate effects, stratification of surgery location between forefoot, midfoot, hindfoot, and ankle with wound complication rates, and realized cost savings between these cohorts.
Footnotes
Author Contributions
JP organized and wrote the manuscript. AL collected data and assisted with writing the manuscript. AR collected data and assisted with writing the manuscript. SKS performed statistical analyses and generated tables. ND assisted with writing the manuscript. GH reviewed the manuscript. MH organized the project and IRB approval. CK provided guidance and reviewed the manuscript. EG provided guidance and reviewed the manuscript.
Data Availability
The data sets generated during and/or analyzed during the current study are not publicly available due to identifiable patient factors but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the UC Davis IRB (1801553-1).
Informed Consent
Informed consent was not sought for the present study because this is a retrospective chart review.
Trial registration
Not applicable.