
Abstract
Syndactyly-polydactyly-ear lobe (SPEL) syndrome is a rare, genetic, congenital limb malformation syndrome that can be characterized by 6 different human phenotypes. We report a rare case of SPEL syndrome in a young woman with right earlobe malformations and asymptomatic preaxial polydactyly with partial duplication of the right hallucal distal phalanx without a supernumerary toe. Unique aspects of our patient’s clinical presentation include lack of a supernumerary digit with a bifurcated distal phalanx, associated earlobe malformations, adult age, and no reported familial history of SPEL syndrome. Syndactyly-polydactyly-ear lobe syndrome has not been reported in the literature since 1976, making the present case particularly noteworthy.
“Syndactyly-polydactyly-ear lobe (SPEL) syndrome is a rare, genetic, congenital limb malformation syndrome first described by Goldberg and Pashayan . . .”
Introduction
Syndactyly-polydactyly-ear lobe (SPEL) syndrome is a rare, genetic, congenital limb malformation syndrome first described by Goldberg and Pashayan 1 in 1976. The authors followed 10 individuals from the same family over the span of 3 generations who all presented with a syndrome involving syndactyly, polydactyly, and earlobe malformations. Some family members had feet with either a broad great toe or a preaxial supernumerary toe. Nodule and deep horizontal groove deformities were also seen in the earlobes of these 10 family members. The authors determined that the family displayed an inheritance pattern compatible with an autosomal dominant trait and identified 6 phenotypical variations of this condition: (1) preaxial hand polydactyly, (2) preaxial foot polydactyly, (3) broad toe, (4) 1 to 2 toe complete cutaneous syndactyly, (5) bifid distal phalanx of toe, and (6) abnormal earlobe morphology.
The study by Goldberg and Pashayan 1 remains the only published study on SPEL syndrome. Following the publication of their study, SPEL syndrome was identified as a new syndrome in 1976 but has not been reported in the literature since. There are several types of syndromes that may be associated with pedal syndactyly or polydactyly. These syndromes may also have other congenital anomalies, which may consist of tarsal and metatarsal fusions, complex bony syndactyly of all toes, or craniofacial abnormalities. The main 3 distinguishing features of SPEL syndrome include very specific anatomic areas of the ear lobe, the ulnar border of the hand, and the preaxial border of the foot.
In patients with multiple malformations in different parts of the body, a complete phenotypic description of the malformations should be obtained and referral to a clinical geneticist is advised, so that, specific genetic testing can be carried out to confirm or exclude syndrome diagnosis. Although our patient was not referred to a clinical geneticist, we still felt it necessary to highlight this underreported syndrome, especially since our patient presented with 4 of the 6 phenotypes of SPEL syndrome.
We present the case of a woman who presented to our clinic with 4 of these 6 phenotypes and was subsequently diagnosed with SPEL syndrome and underwent surgical treatment to correct functional limitations caused by this condition. The patient was informed and gave written consent for details from her case to be published.
Case
A healthy, 21-year-old African American woman with a past medical history significant for depression presented to our clinic with a large soft tissue mass caused by keloid formation extending from the right ear helix (Figure 1) and concerns of a broad right hallux (Figure 2) present since birth. The patient denied having any pain in her toe but reported difficulty with finding shoes to properly accommodate her toe deformity. She also expressed overall discontentment with the cosmetic appearance of the toe. She reported that 3 years prior, a dermatologist had surgically removed the 2 keloids from her right ear helix and earlobe; however, the keloid on her helix started to grow back about 1 year following the initial removal. She had no prior surgical intervention on the bifid hallux. There was no family history of SPEL syndrome known to the patient.
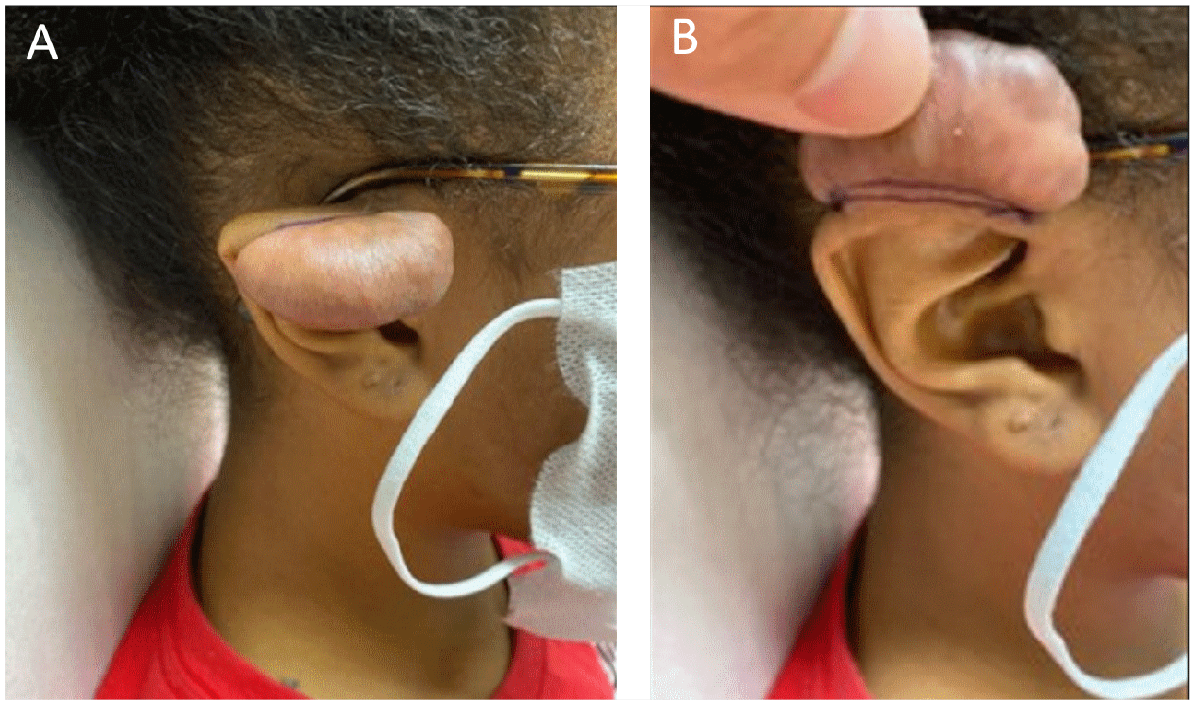
Preoperative appearance of right ear keloid extending from the ear helix caused by helix piercing (A). Inferior view of keloid extending from the ear helix (B).

Preoperative images of the patient’s broad right hallux. Comparison of abnormal broad right hallux with normal size left hallux (A). Dorsal view of broad right hallux showing central linear depression of nail plate but no other significant nail plate pathology (B). Plantar view of broad right hallux slightly underriding second toe (C).
Clinical examination revealed a broadened right hallux without an extra digit. The great toenail was also widened, with a linear depression noted centrally within the nail plate (Figure 2). The patient had no pain to palpation at the hallux interphalangeal joint (IPJ), and range of motion within this joint was full and pain-free. Mild valgus rotation of the hallux was noted, but no flexion deformity at the hallux IPJ.
Radiographic examination revealed a bifid distal phalanx of the hallux (Figure 3). The radiograph report further described the bifid distal phalanx as a congenital segmentation anomaly with a fused rudimentary distal phalanx at the medial aspect of the base of the distal phalanx and a mild hallux valgus deformity.

Preoperative radiographs showing a bifid distal phalanx of the hallux with two distal phalanges of the right great toe that appear to be fused at the base. Radiographic appearance of the duplication of the phalanges appear to be within a single digit (polydactyly with accompanying syndactyly).
Operative Technique
The decision for surgical treatment was based on functional limitations the patient was having with footwear of normal shoes. Before prepping the foot, a partial nail avulsion was done to remove about one third of the medial aspect of the nail plate (Figure 4A). This was done to reduce the spread of contaminants during the prepping process. Incisional planning was completed to include a wedge incision made at the dorsomedial aspect of the hallux, encompassing the terminal nail matrix of the recently avulsed portion of the nail plate. The incision was made full thickness down to bone (Figure 4B). This portion of bone was resected utilizing a sagittal bone saw, so that, the medial collateral ligament and articular surface of the IPJ were preserved. Further resection of the rudimentary phalanx was completed using a pineapple burr and assessed under fluoroscopy to confirm that a natural anatomical contour of the distal phalanx had been created. Afterwards, skin closure was completed by simple interrupted sutures utilizing 4-0 polypropylene through the nail plate and 4-0 nylon sutures in the skin (Figure 4C).
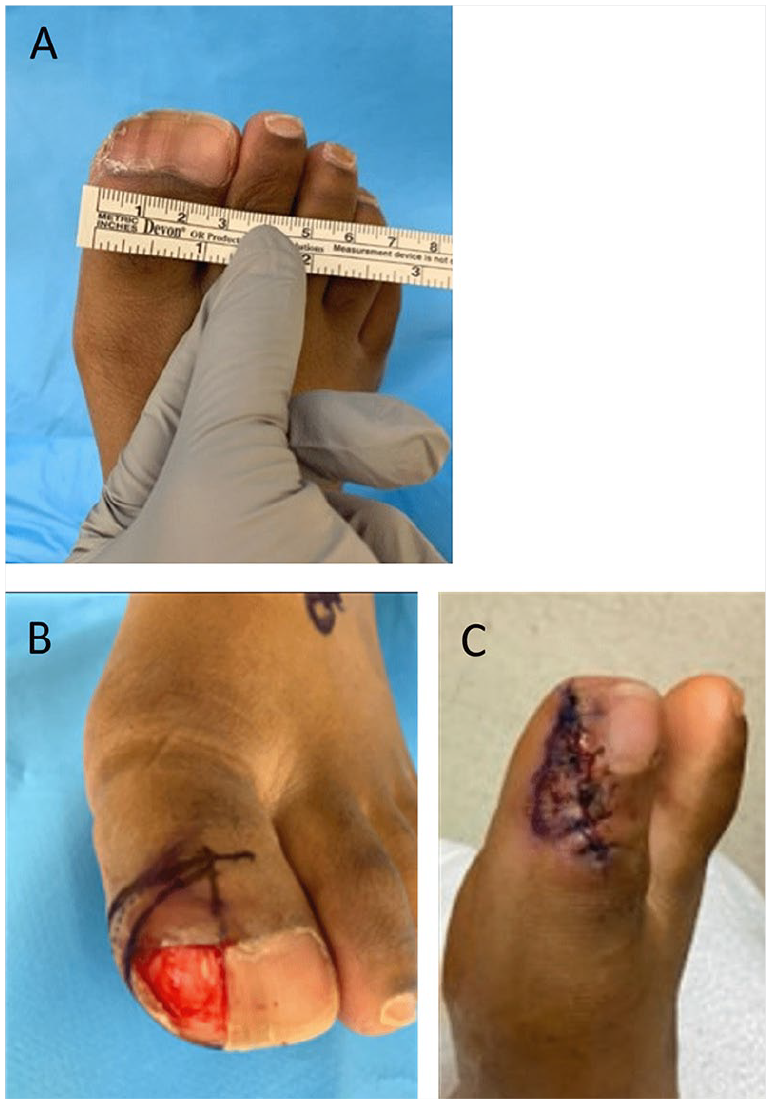
Partial nail avulsion done to remove about one third of the medial aspect of the nail plate preoperatively (A). Wedge incision made at the dorsomedial aspect of the hallux, encompassing the terminal nail matrix of the recently avulsed portion of the nail plate. The incision was made full thickness down to bone (B). Skin closure completed by simple interrupted sutures utilizing polypropylene through the nail plate and nylon sutures in the skin (C).
The patient was seen 3 days postoperatively and was pleased with the physical appearance of the great toe. There were no local signs of infection. She had mild swelling within the toe consistent with surgical intervention and reported no pain. At 3 months postoperatively, she denied having any complications or limitations in walking or with wearing shoes (Figure 5). Radiographs at this time also showed good resection of the bifid distal phalanx (Figure 6). She expressed that she was satisfied with the surgical outcome. The patient did not provide outcome scores.
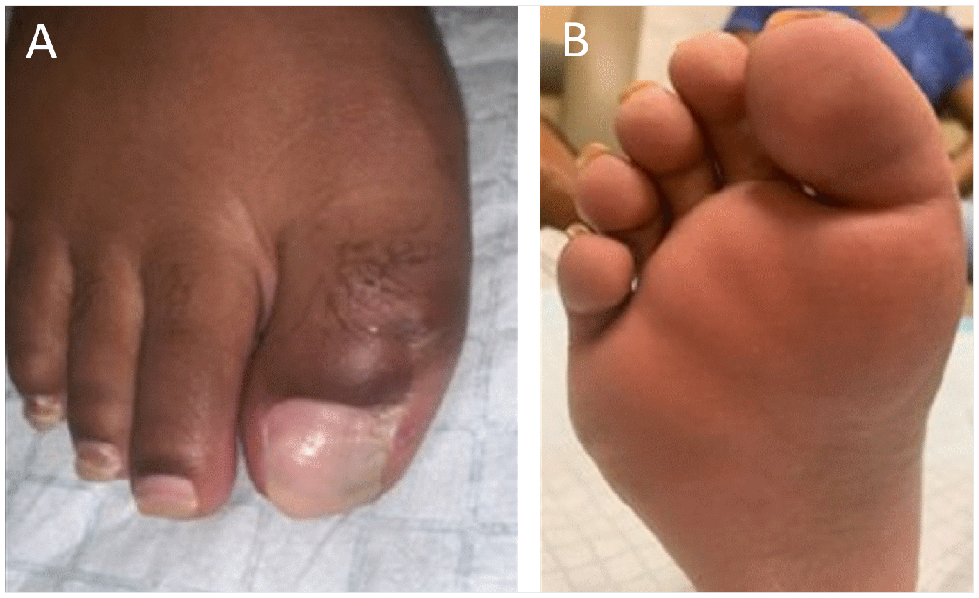
Postoperative result after 3 months showing reduction of right great toe dorsally (A). Plantar aspect of right great toe at 3 months postoperative (B).

Radiographs taken 3 months postoperatively showing resection of the bifid distal phalanx.
Four months after her toe procedure, the patient also underwent dermatological surgery to excise the recurrent ear helix nodule (Figure 7). We found it interesting to note that the earlobe malformations and broad hallux were both on the right side.
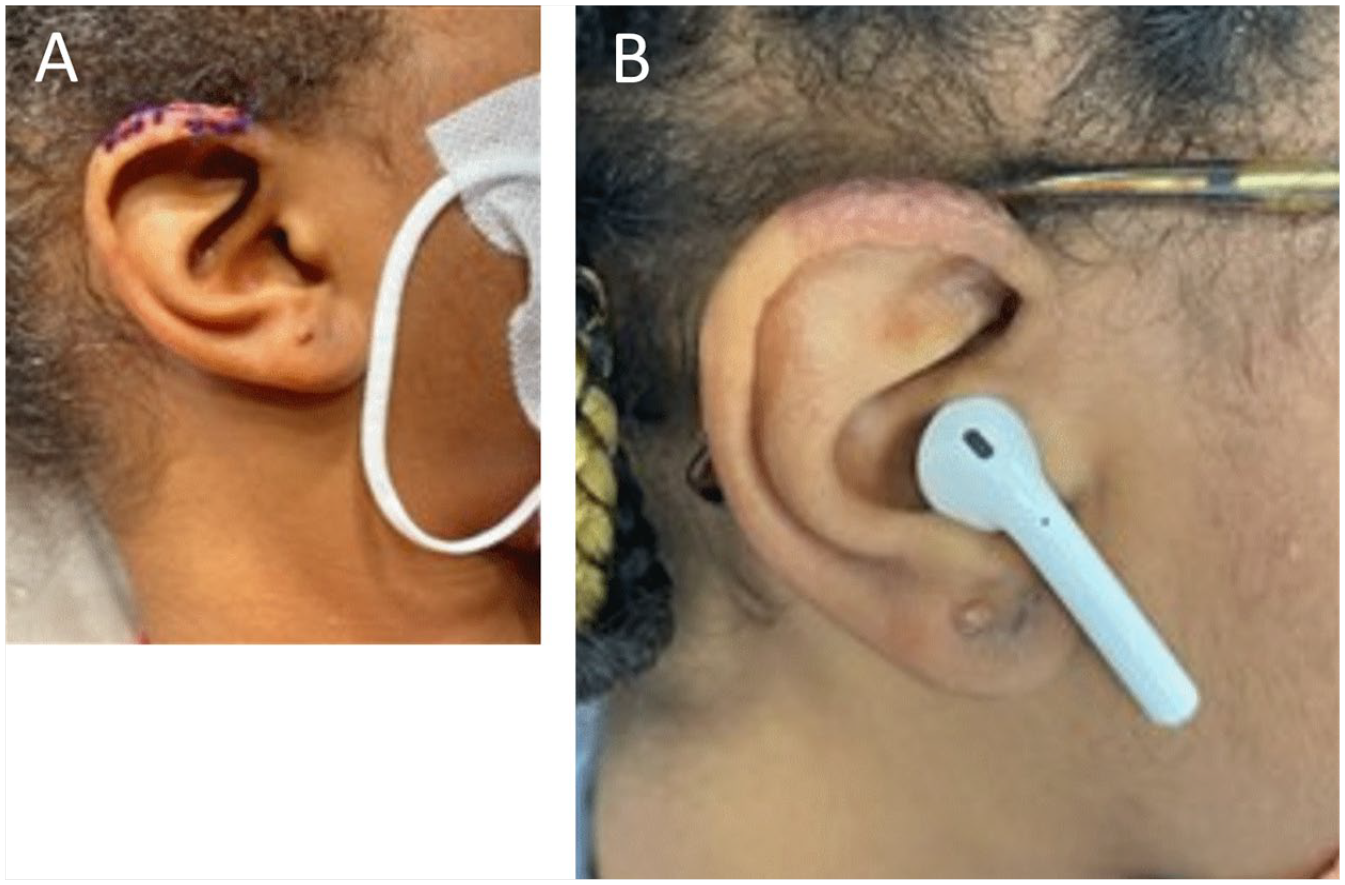
Postoperative images showing excision of recurrent ear helix nodule with sutures still intact (A). Postoperative result of right helix nodule excision after 2 months (B).
Discussion
Our patient presented with abnormal earlobe morphology and preaxial polydactyly of the foot in the form of a bifid distal phalanx, resulting in a broadened great toe, representing 4 of the 6 phenotypes of SPEL syndrome. 1 Preaxial polydactyly of the foot occurring at the hallux is not as commonly seen as postaxial polydactyly, which occurs at the fifth toe.2,3 Both are subtypes of polydactyly, a common congenital limb condition usually diagnosed in utero occurring at a frequency of 1 in approximately 1000 live births.4,5
Polydactyly in the feet has 3 main phenotypes based on the location of the duplicate digit: preaxial (tibial/hallux), central (central 3 lesser digits), and postaxial (fibular/fifth toe).2,5-7 Preaxial polydactyly is rare and makes up about 15% of pedal polydactyly cases.2,3,5,7 Although lacking in our patient, preaxial polydactyly is usually characterized by supernumerary digits on the medial aspect of the feet. Surgical treatment is largely debated for asymptomatic cases, but is overall determined based on osseous involvement, pain, and functional limitations imposed by the extra digit. 8 Patients with polydactyly in the feet may have difficulty finding accommodative shoes, resulting in discomfort and overcrowding of the toe box. 4
Another interesting phenotype of SPEL syndrome is abnormal ear morphology, as seen in our patient. Although polydactyly without a supernumerary digit has been reported in the literature,2,5,9,10 there has only been 1 reported study that specifically correlates adult preaxial polydactyly with an earlobe abnormality. 1 The study, published by Goldberg and Pashayan, 1 did not specify whether the earlobe malformations in their case family were congenital or resultant of trauma, as is often seen with keloid formation of the ear. The patient in our case was diagnosed with keloids following trauma from ear piercings in her ear lobe and ear helix.
Surgical treatment is still controversial when polydactyly is asymptomatic, and some surgeons will not operate on polydactyly cases solely for cosmesis. Our patient was originally denied surgical treatment by a prior surgeon since she was not experiencing any toe pain. Our decision to operate was largely based on limitations the patient was having in finding shoes to accommodate her broad great toe due a bifid hallux. It should be noted that osseous involvement is often absent in cases of polydactyly, making the present case even more interesting. 11
Unfortunately, there is little surgical literature on preaxial polydactyly of the foot. For this reason, it is difficult to provide a solid comparison of the literature as it relates to the present study. Current literature on preaxial polydactyly of the foot focuses more on classification and technique for removal of the extra digit(s). To our knowledge, there is limited clinical guidance for the surgical treatment options for patients with this specific pedal anomaly. The current study is essential in that it will offer insight on surgical options when treating preaxial polydactyly, even if asymptomatic. These patients often simply want a normal-appearing foot without extra digits.
Therefore, cosmesis was not without consideration in surgical planning.12-15 Although controversial and often overlooked in foot surgery, cosmesis is not necessarily an absolute consideration in cases of polydactyly. 15 This is especially true when treating young adult women with polydactyly. Women have greater societal demands unnecessarily placed on them regarding body appearance and this may also include foot symmetry. 13 Our patient was interested in having a normal-looking big toe that mirrored the contralateral foot for both aesthetics and functionality. Although emphasis should be placed on individualizing the surgical approach in any polydactyly case, 9 pain should not be the sole determining factor when deciding on whether polydactyly patients need surgery.
Surgical resection of the preaxial portion of the bifid distal phalanx of the hallux was an appropriate procedural choice for our patient since it did not impair biomechanical functionality. Furthermore, a desirable cosmetic outcome was achieved, which was crucial for patient satisfaction. 11 Our patient was equally pleased with surgical removal of the ear helix nodule, completed by dermatology. Both procedures seemed to enhance her self-esteem.
This case report sheds light on this rare condition and may help other clinicians make the correlation between polydactyly and the possibility of other associated phenotypes of SPEL syndrome, while also discussing the appropriateness for surgical intervention in asymptomatic cases of polydactyly in adults.
Footnotes
Acknowledgements
Many thanks to the patient for allowing her case to be presented and published, and to Dr Kathleen Kroger from the Department of Dermatology at the University of Texas Medical Branch for providing some of the clinical images presented herein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board’s (IRB) approval for this case study was waived in accordance with our institution’s policies: Case reports do not involve systematic investigation; however, the intent is to contribute to generalizable knowledge. Case reports are not considered to be research involving human subjects and do not require prior IRB review and approval.
Informed Consent
The patient provided informed consent for details from her case to be published.
Trial Registration
Not a clinical trial.