
Abstract
Background
The utilization of total ankle arthroplasty (TAA) continues to increase. Discharge to a post-acute care (PAC) facility can increase patient morbidity and postoperative costs. The purpose of this study is to investigate the effects of age and body mass index (BMI) on discharge to a PAC facility and hospital length of stay (LOS) following TAA.
Methods
A retrospective review of patients who underwent TAA from the National Surgical Quality Improvement Program (NSQIP) database was performed. Using overweight patients as the reference BMI group, sex- and age-adjusted log-binomial regression models were utilized to estimate risk ratios of BMI categories for being discharged to a PAC facility. A linear regression was utilized to estimate the effect of BMI category on hospital LOS.
Results
Obese patients had 1.36 times the risk of overweight patients (P = .040), and morbidly obese patients had 2 times risk of overweight patients (P = .001) of being discharged to a PAC facility after TAA. Men had 0.48 times the risk of women (P < .001). Compared with patients aged 18 to 44 years, patients aged ≥65 years had 4.13 times the risk (P = .012) of being discharged to a PAC facility after TAA. Relative to overweight patients, on average there was no difference in hospital LOS for underweight patients, but healthy weight patients stayed an additional 0.30 days (P=.003), obese patients stayed an additional 0.18 days (P = .011), and morbidly obese patients stayed an additional 0.33 days (P = .009). Men stayed 0.29 fewer hospital days than women (P < .001) on average.
Conclusion
Women and patients who are obese or morbidly obese have a longer hospital LOS and an increased chance of being discharged to a PAC facility. Increasing age is also associated with an increased risk of being discharged to a PAC. These may be important factors when developing and discussing the postoperative plan with patients prior to TAA.
Levels of Evidence:
Level III
Keywords
“The results of our study demonstrated that, compared with the overweight BMI group, obese and morbidly obese patients had a significantly increased length of hospital stay and a greater risk of being discharged to a PAC facility after TAA.”
Introduction
The ankle joint is subject to more pressure and is injured more commonly than any other joint in the body.1,2 An increasing number of young and older adults in their working lives and beyond are developing ankle arthritis. 3 Total ankle arthroplasty (TAA) is a safe and effective treatment for various ankle pathologies, including osteoarthritis, osteonecrosis, inflammatory joint diseases, and posttraumatic arthropathies.1,4 -8 Total ankle arthroplasty preserves motion at the ankle joint while still achieving the primary goal of pain relief. 9 With an increasing number of patients undergoing TAA, identifying modifiable preoperative factors that influence postoperative outcomes after TAA may be valuable. 10
Body mass index (BMI) plays a role in postoperative joint outcomes and previous literature has cited various postoperative complications associated with a very high and/or low BMI.11 -22 However, to our knowledge, no other study has evaluated the impact of BMI on discharge to a post-acute care (PAC) facility for TAA. As patient safety and decreasing cost of care are emphasized topics in medicine and discharge to a PAC facility has been shown to increase patient morbidity and long-term cost through postoperative adverse events and readmissions, it may be important to identify risk factors for discharge to a PAC facility.23 -25
The purpose of this study is to investigate the associations of age, sex, and BMI on discharge to a PAC facility and hospital length of stay following TAA. It was hypothesized that outcomes would be worse for underweight as well as morbidly obese patients, and that patients in these BMI categories along with those of increasing age would be more likely to be discharged to a PAC facility and have a longer total length of hospital stay.
Methods
After IRB approval from the Prisma Health Institutional Review Board [1954940], a retrospective review was performed to identify a large cohort of patients who underwent TAA from the American College of Surgeons–National Surgical Quality Improvement Program (ACS-NSQIP) database. This database is a robust, generalizable database from more than 700 participating institutions, which is collected by trained clinical reviewers and includes preoperative, demographic, comorbidity, and postoperative data.26 -28 It has been widely used in orthopaedic surgery to track the clinical course of patients.29,30
Adult patients (aged ≥ 18 years) who underwent TAA between 2006 and 2020 were identified by Current Procedural Terminology (CPT) code 27702. Patients were excluded from this study if they underwent hemiarthroplasty, revision TAA, or had an outpatient procedure. An individual patient’s outpatient/ambulatory surgical procedure status was defined by the institution in which they had the surgery, following that respective hospital’s criteria of being an outpatient. A total of 1653 patients were included in this study.
The BMI groups were defined in accordance with the World Health Organization’s definitions as underweight (BMI <18.5; n = 7), healthy weight (BMI 18.5 to <25; n = 213), overweight (BMI 25 to <30; n = 594), obese (BMI 30 to <40; n = 714), morbidly obese (BMI ≤40; n = 125). 31 A sex- and age-adjusted logistic regression model was utilized on BMI categories to estimate odds ratios and then a sex- and age-adjusted log-binomial regression model was utilized on BMI categories to estimate risk ratios. Using overweight patients as the reference BMI group allowed for investigation of whether other BMI groups had an increased risk (relative to the reference group) of being discharged somewhere other than home, as in a PAC facility. Similarly, using the 18 to 44 years age category as the reference age group allowed for analysis of whether the middle and older age groups had an increased risk of being discharged to a PAC facility (relative to the youngest age group). Furthermore, selecting these respective reference groups allowed risk ratios to be reported as uniformly positive values.
In the case of BMI and age categories, indicator variables were included for all non-reference groups into the regression models. In so doing, the estimated coefficients represented the difference between the indicated group and the excluded reference group. In linear regression models, the estimated coefficient then represented the average outcome associated with the indicated group minus the average response of the reference group. If the coefficient was positive, the average outcome of the indicated group was larger than the average response of the reference group; if the coefficient was negative, the average outcome of the indicated group was smaller than the average response of the reference group. In either case, whether that difference was statistically significant is related to the associated P value of the test.
In logit-binomial regression models (logistic), the estimated coefficients are related through odds ratios. That is, the exponentiated coefficient of the indicated variable is the estimated odds ratio of the indicated group relative to the reference group. Similarly, in log-binomial regression models, the estimated coefficients are related through risk ratios. That is, the exponentiated coefficient of the indicated variable is the estimated risk ratio of the indicated group relative to the reference group. 32
Results
More than 80% of patients who underwent TAA provided a race identity, with the majority (77.6%) being white (Table 1). This trend is consistent with that of previous studies documenting racial disparities for the utilization of TAA in the United States.33,34 Obese patients had 1.36 times the risk of overweight patients (P = .079), and morbidly obese patients had 2 times the risk of overweight patients (P = .001) of being discharged to a PAC facility (Table 2). The unadjusted differences in rates illustrated in Table 1 show that 10.3% of overweight patients, compared with 20% of obese patients, were discharged to a PAC facility. This risk ratio was the strongest clinical signal in our analysis (based on the size of the adjusted risk ratios).
Patient Demographics.
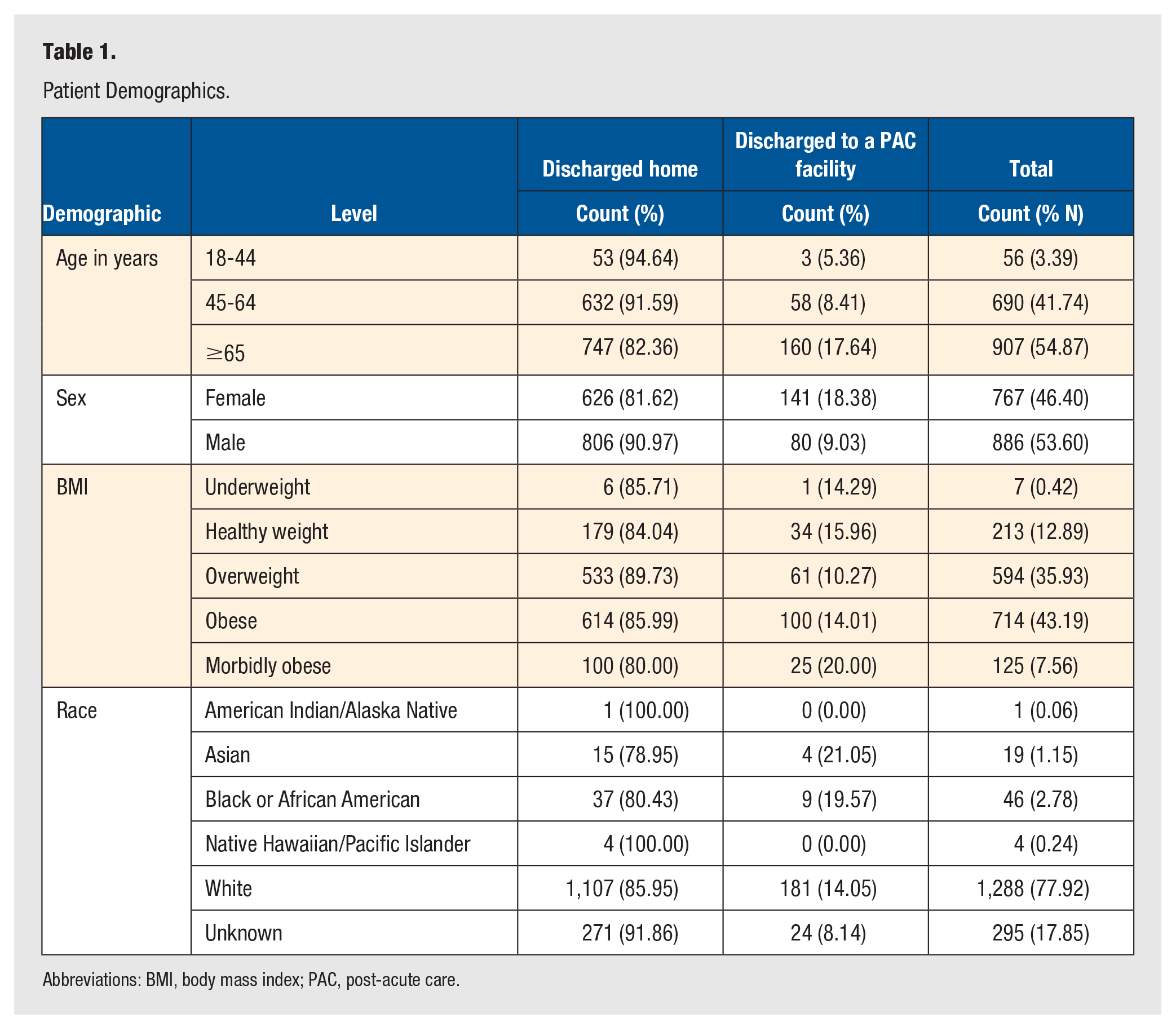
Abbreviations: BMI, body mass index; PAC, post-acute care.
Comparison of the Risk Ratios of Being Discharged to a PAC Facility for Different Preoperative Variables.
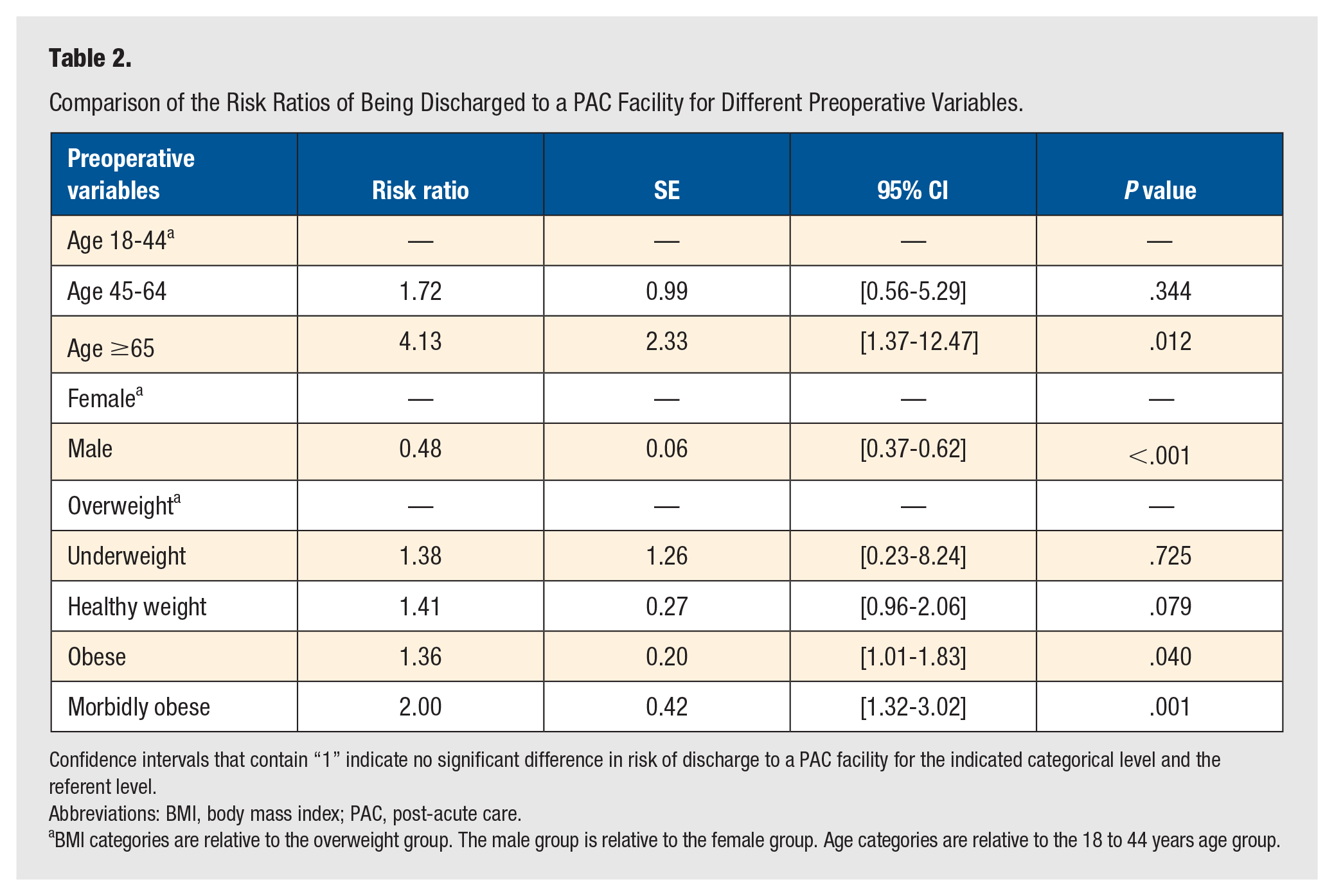
Confidence intervals that contain “1” indicate no significant difference in risk of discharge to a PAC facility for the indicated categorical level and the referent level.
Abbreviations: BMI, body mass index; PAC, post-acute care.
BMI categories are relative to the overweight group. The male group is relative to the female group. Age categories are relative to the 18 to 44 years age group.
Men stayed 0.29 fewer days in the hospital compared with women (P < .001; Table 3). Furthermore, 18% of women were discharged to a PAC facility versus just 9% of men (Table 1), demonstrating that men had only 0.48 times the risk of women (P < .001) of being discharged to a PAC facility (Table 2).
Comparison of Total Length of Hospital Stay for Different Preoperative Variables.
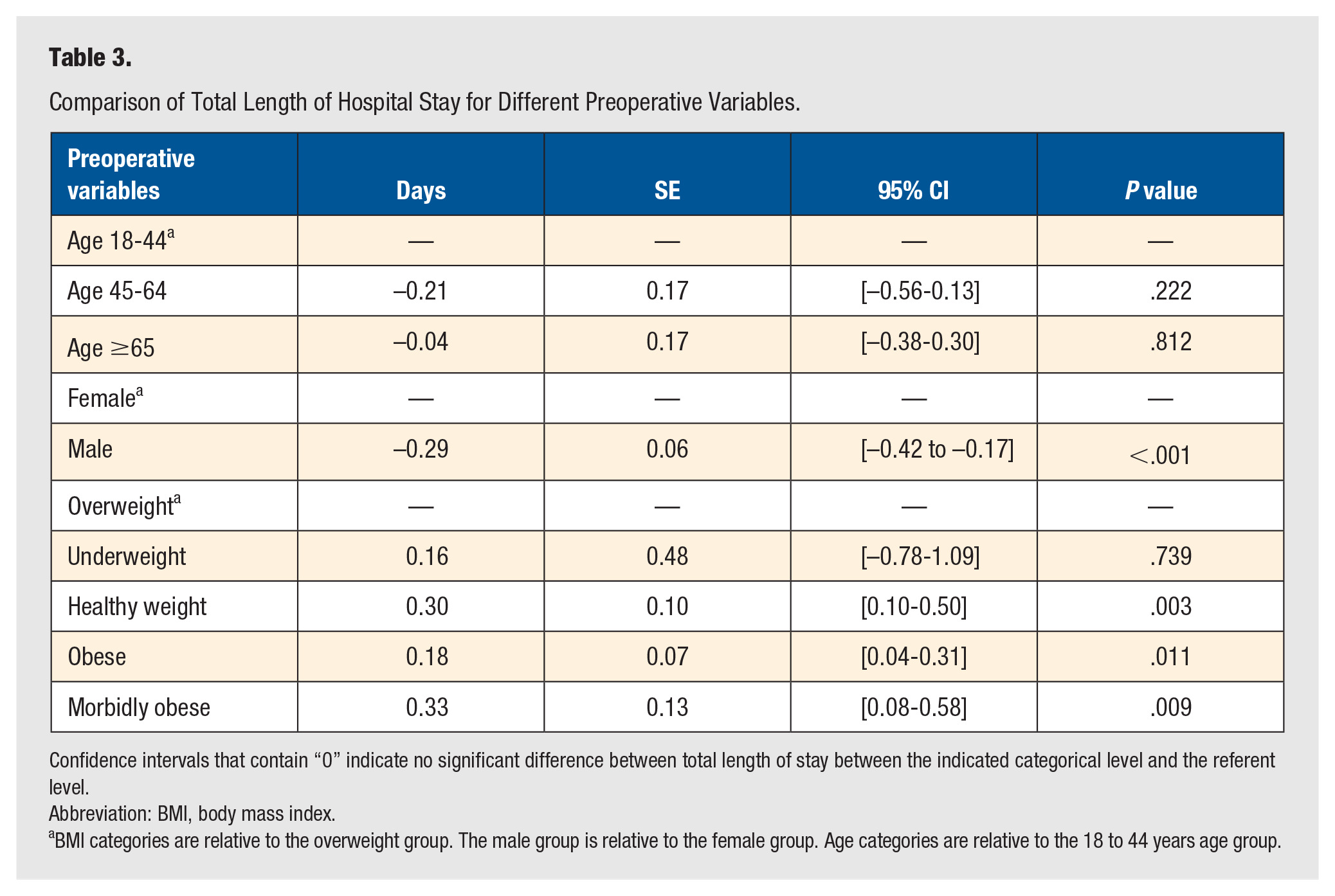
Confidence intervals that contain “0” indicate no significant difference between total length of stay between the indicated categorical level and the referent level.
Abbreviation: BMI, body mass index.
BMI categories are relative to the overweight group. The male group is relative to the female group. Age categories are relative to the 18 to 44 years age group.
Age was not found to have a significant impact on hospital length of stay (age 45-64 years: P = .222, age ≥65 years: P = .812; Table 3). However, 17.6% of patients aged 65+ years were discharged to a PAC facility versus just 5.4% of patients aged 18 to 44 years (Table 1), representing a 4-fold increased risk (P = .012) of being discharged to a PAC facility for the older adults relative to the 18 to 44 years age group (Table 2).
Finally, relative to overweight patients, there was no difference in average length of hospital stay for underweight patients, but healthy weight patients stayed an additional 0.30 days (P = .003), obese patients stayed an additional 0.18 days (P = .011), and morbidly obese patients stayed an additional 0.33 days (P = .009) on average.
Discussion
Some potential factors, such as age, sex, socioeconomic status, and preoperative diagnosis are not acutely modifiable. 35 However, modifiable risk factors such as BMI could be addressed preoperatively to maximize the patient’s chances of postoperative morbidity associated with PAC utilization and to limit unnecessary health care costs. The results of our study demonstrated that, compared with the overweight BMI group, obese and morbidly obese patients had a significantly increased length of hospital stay and a greater risk of being discharged to a PAC facility after TAA. In addition, our results noted that men had a decreased risk of being discharged to a PAC facility and a shorter total length of hospital stay when compared with women. In addition, patients aged ≥65 years had an increased risk of being discharged to a PAC facility compared with the 18 to 44 years age group after TAA.
Several studies have analyzed BMI and length of hospital stay; whereas some studies found that a higher BMI is associated with a longer hospital stay, other studies found no evidence of a statistically significant association between BMI and length of hospital stay.36 -39 Our results showed that, compared with the overweight BMI group, all BMI categories, except for underweight patients, had longer hospital stays on average (Table 3). Overall, our results indicated that the overweight BMI group had the shortest length of hospital stay although this was not statistically different from the normal weight group. This more favorable outcome for the overweight group could be explained by inaccuracy with the cutoffs when using BMI as a measuring method. This system overpredicts the weight of muscular individuals and underpredicts the weight of those with less muscle, which could skew results.
Previous studies have described the association between obesity and medical complications, such as thrombotic events, postoperative falls, and revision/failures.11,12,17,18,20 In addition, the chronic, low-grade systemic inflammation and impaired functional status associated with a higher BMI has been shown to compromise postoperative recovery after certain procedures. 15 Therefore, physicians may believe that patients with a higher BMI need to be monitored more intensely due to their increased risk for postoperative complications and impaired ability to heal. This potential need for extra support may explain the results of our study that obese patients had 1.36 times the risk (P = .040) and morbidly obese patients had 2 times the risk (P = .001) of being discharged to a PAC facility after TAA, when compared with the overweight BMI group. Patients with higher BMIs being more likely to be discharged to a PAC facility may also contribute to the reason why previous studies have found heavier patients to have increased postoperative costs. 40 It may be important for surgeons to consider that obese and morbidly obese patients are more likely to be discharged to a PAC facility. In increasingly cost-constrained environments where it may be favorable to avoid discharge to a PAC facility due to both cost and complication risks, it may be a consideration for the surgeon to discuss lifestyle changes, such as diet and exercise, to help lower the patient’s BMI before surgery to avoid discharge to a facility other than home. However, being underweight has also been associated with increased mortality and worse outcomes postoperatively in the literature.13,14,16,19,23,41 Despite this, the results of our study demonstrated that underweight patients did not have an increased risk of being discharged to a PAC facility (P = .725). Of note, this lack of statistical significance may have been skewed by the small sample size of the underweight BMI group in our study, which therefore may not be representative of the true effect for this cohort.
Our study also evaluated the effect of sex on discharge disposition to PAC. Prior literature found that being male was associated with a decreased likelihood of discharge to an extended care facility after total knee arthroplasty.42,43 Our study corroborated this finding for patients undergoing ankle arthroplasty and, as noted in our results, men had only 0.48 times the risk of women of being discharged to a PAC facility after TAA (P < .001). Our results also demonstrated that men stayed in the hospital on average 0.29 fewer days than women (P < .001), which is consistent with data from previous studies noting that women undergoing orthopaedic procedures were more likely to have longer hospital stays.44,45
In addition, we analyzed age as a risk factor for discharge to a PAC. Prior literature has shown that increased age is associated with adverse outcomes after surgical intervention.39,46 -51 The results of our study found that patients aged ≥65 years had 4.13 times the risk of being discharged to a PAC facility after TAA (P = .012). We also analyzed the effect of age on hospital stay duration and our results demonstrated that age category did not have a statistically significant impact on hospital length of stay. This was in contrast to prior literature that noted an association between patient age and hospital length of stay.52,53 However, these studies analyzed age as a continuous variable, which may decrease the validity of their findings. The impact that each year older in age makes is likely different among the younger population compared with the older population. Therefore, we feel that the method of analyzing age as a categorical variable that differentiates younger, middle, and older age groups provides more clarity.
The use of PAC has grown substantially in the past several decades. 54 More than 40% of Medicare beneficiaries receive PAC after hospital discharge. 55 In 2015, Medicare spent more than $60 billion on PAC, an amount that has been rapidly increasing.56,57 However, the choice of setting for PAC can impact patient outcomes and cost. A 2016 study found that, after elective total joint arthroplasty, discharge to a skilled nurse facility or an inpatient rehabilitation facility increased the risk of post-discharge adverse events when compared with discharge home. 23 Another 2016 study found that patients who underwent revision total joint arthroplasty and were discharged to a skilled nursing facility or an inpatient rehabilitation facility had significantly increased risk for unplanned readmissions when compared with patients discharged home. 24 Of note, the average readmission cost following total joint arthroplasty is approximately $24 000. 58 These studies showed that discharge destination is an independent risk factor for adverse events requiring readmission, leading to increased patient morbidity and unnecessary health care costs. Discharge destination has also been found to be an independent risk factor for hospital readmissions in older trauma patients despite controlling for injury severity and comorbidities. 25 Given this, identifying a modifiable preoperative variable such as larger BMI to carry a greater risk of being discharged to a PAC facility may predict the risk of patient morbidity and substantially higher health care costs, but that is outside the scope of this study.
Many prior studies have used healthy weight as the reference group to facilitate the evaluation of the effect of BMI on postoperative complications and outcomes. However, given that patients in our data set were more likely to be obese or overweight, we chose to highlight the comparison of other BMI categories with a more represented BMI group (overweight patients). In addition, given that the average BMI in the United States continues to increase, we felt that the frequency of each BMI group in our study reflects the patient population that a surgeon is more likely to encounter.59 -61 Therefore, using the overweight BMI category as the reference group may be the most useful information for surgeons to consider for this topic.
There were several limitations to our study. We utilized a large database to attempt to analyze these questions and there are well-described potential problems in utilizing this data set, such as coding bias and solely including in-hospital data.62,63 In addition, this retrospective database had unknown interrupter reliability for coding and did not account for comorbidity, socioeconomic, or psychosocial factors, which may influence discharge destination.
Conclusion
This study found that, compared with the overweight BMI group, obese and morbidly obese patients had a significantly increased hospital length of stay and a greater risk of being discharged to a PAC facility after TAA. Men had a decreased risk of being discharged to a PAC facility and a shorter hospital length of stay when compared with women. Patients aged ≥65 years had an increased risk of being discharged to a PAC facility after TAA. There are both modifiable and non-modifiable risk factors for increased length of stay and the chances of being discharged to PAC facility after TAA that surgeons may want to consider preoperatively and discuss with their patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Prisma Health Institutional Review Board [1954940].
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.