
Abstract
Introduction
Ankle arthritis adversely affects patients’ function and quality of life. Treatment options for end-stage ankle arthritis include total ankle arthroplasty (TAA). A 5-item modified frailty index (mFI-5) has predicted adverse outcomes following multiple orthopaedic procedures; this study evaluated its suitability as a risk-stratification tool in patients undergoing TAA.
Methods
The National Surgical Quality Improvement Program (NSQIP) database was retrospectively reviewed for patients undergoing TAA between 2011 and 2017. Bivariate and multivariate statistical analyses were performed to investigate frailty as a possible predictor of postoperative complications.
Results
In total, 1035 patients were identified. When comparing patients with an mFI-5 score of 0 versus ≥2, overall complication rates significantly increased from 5.24% to 19.38%, 30-day readmission rate increased from 0.24% to 3.1%, adverse discharge rate increased from 3.81% to 15.5%, and wound complications increased from 0.24% to 1.55%. After multivariate analysis, mFI-5 score remained significantly associated with patients’ risk of developing any complication (P = .03) and 30-day readmission rate (P = .005).
Conclusions
Frailty is associated with adverse outcomes following TAA. The mFI-5 can help identify patients who are at an elevated risk of sustaining a complication, allowing for improved decision-making and perioperative care when considering TAA.
Levels of Evidence:
III, Prognostic
Keywords
“One interesting finding in this study was the identification of female sex as a risk factor for adverse discharge and any complication.”
Introduction
Ankle arthritis, while less common than hip and knee arthritis, has a similarly significant negative impact on the function and quality of life of affected individuals.1 -5 Ankle arthritis may also predispose the elderly to increased falls, placing these individuals at a higher risk of fracture.6,7 The most common surgical treatments for end-stage arthritis are ankle arthrodesis and total ankle arthroplasty (TAA). Similar clinical outcomes have been reported for both procedures, although ankle arthrodesis has historically been accepted as the gold standard.8,9 However, ankle arthrodesis eliminates tibiotalar joint motion, which has been shown to cause accelerated rates of arthritis in adjacent joints and to impair patients’ function long term.10,11 TAA is increasing in popularity, as it preserves ankle motion in addition to providing symptomatic relief. 12 Complication rates following TAA have decreased over the years with improvements in implants and surgical techniques and are now comparable with those of ankle arthrodesis.13 -16
Several patient comorbidities and characteristics have recently been identified as risk factors for complications following TAA, but risk-stratification models are just beginning to emerge.13,17 -20 Frailty, defined as a syndrome of age-related physiologic deficits that results in increased susceptibility to adverse health outcomes, has emerged as an important factor in predicting patient outcomes and complication rates within orthopaedics.21 -25 The Canadian Study of Health and Aging created the comprehensive 70-item frailty index, fueling the interest in frailty as a predictor of surgical outcomes.26,27 The index has been abbreviated over time, as certain data within the original index are no longer frequently reported.22 -28 A modified 5-item frailty index (mFI-5) based on specific National Surgical Quality Improvement Program (NSQIP) variables has been validated as a risk-stratification tool for several orthopaedic procedures, including total hip, knee, and shoulder arthroplasty.22 -25 However, TAA outcomes in relation to the mFI-5 have not yet been studied. The aim of this study was to evaluate the suitability of the mFI-5 as a risk-stratification tool for adverse outcomes in patients undergoing TAA. We hypothesized that patients with greater frailty, as defined by the mFI-5, would have higher rates of postoperative complications following TAA.
Methods
Data Collection
Data were taken from the NSQIP database from 2011 through 2017. The NSQIP database is a nationally validated database with nearly 700 hospital participants based on 30-day outcome data obtained from patients’ medical charts, with quality of data ensured by trained personnel and an auditing system. Patients were identified by querying the database for Current Procedural Terminology (CPT) code 27702 (arthroplasty, ankle; with implant [total ankle]). Data prior to 2011 were not included, as the NSQIP database did not include certain 30-day outcomes of interest for TAA (eg, unplanned readmission, unplanned reoperation) prior to this year. 29 Patients missing data for a variable of interest were excluded from any analysis which included that variable. Data collected from each patient included age, sex, race, American Society of Anesthesiology (ASA) classification, height, weight, and wound class. Body mass index (BMI) for each patient was calculated from height and weight data.
Modified Frailty Index
The mFI-5 is composed of 5 risk factors: history of diabetes mellitus requiring treatment with an oral hypoglycemic agent or insulin, history of hypertension requiring medication, history of CHF (either newly diagnosed within 30 days prior to surgery, or chronic CHF with an acute exacerbation within 30 days prior to surgery), history of severe COPD or current pneumonia, and non-independent functional status (requiring some or complete assistance with activities of daily living). 30 The mFI-5 for each patient was calculated by counting the number of these criteria present, for a possible score of 0 to 5.
Outcomes and Complications
Select 30-day outcome data were gathered from the NSQIP database and collated into the following systems-based complication groups: cardiac (cardiac arrest and myocardial infarction), pulmonary (pneumonia, pulmonary embolism, and unplanned intubation), hematology (blood transfusions and deep venous thrombosis/thrombophlebitis occurrences), renal (renal insufficiency and acute renal failure requiring dialysis), stroke/central nervous system (stroke/cerebrovascular accident [CVA]), infection (superficial and deep surgical site infection), and wound (wound dehiscence). Clavien-Dindo IV (CDIV) complications were analyzed separately, comprising unplanned intubation, pulmonary embolism, prolonged ventilator requirement, cardiac arrest, myocardial infarction, acute renal failure requiring dialysis, septic shock, and stroke/CVA. Mortality, 30-day readmission, 30-day reoperation, and adverse discharge (discharge to any location other than home) data were also collected and analyzed as complications. The rate of patients experiencing at least 1 of the aforementioned complications was the primary outcome.
Statistical Analysis
All variables were described using frequency and proportion for categorical variables or mean and standard deviation for continuous variables. Patients were sorted into 3 groups (mFI-5 score of 0, 1, and ≥2) to facilitate analysis. Bivariate analysis was performed separately for each complication to assess for association with the patient-level variables mentioned above, with t tests and chi-squared/Fisher’s exact tests used to test for association with categorical and continuous variables, respectively. Bivariate analysis allowed for the identification of differences in complication rates in patients with varying mFI-5 scores. Logistic regression was then performed to control for any possible confounding variables and ascertain independent risk factors for each complication. Any variable found to have a P value of less than .2 on bivariate analysis with that complication was included in the corresponding logistic regression. Age, sex, BMI, length of stay (LOS), total operative time, and mFI-5 score were included in the models, regardless of P value. A P value of less than 0.05 was considered to be statistically significant. For any complication and for adverse discharge, we performed an additional forward stepwise regression starting with a model including only the score, and leaving out race, as this variable was missing a larger amount of data (n = 135). All statistical analysis was performed using the R statistical package. 31
Results
Patient Demographics
A total of 1035 patients were identified, with 1028 patients having complete data allowing for mFI-5 calculation. Roughly, half (51.1%) of the patients were male. The predominant race (83.1%) was white. Mean patient age was 63.9 years. Most patients had an ASA class of 2 (56%) and were either overweight (35.7%) or obese (27%), with an average BMI of 31.0 (Table 1).
Patient Demographics.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
mFI-5 Scores
Scores ranged from 0 to 4; no patients had an mFI-5 score of 5. The number of patients with each of the mFI-5 scores was as follows: 420 patients scored 0, 479 patients scored 1, 122 patients scored 2, 5 patients scored 3, and 2 patients scored 4. When combined, 129 patients (12.6%) had an mFI-5 score of ≥2.
Thirty-Day Postoperative Complications Based on mFI-5 Score
The overall complication rate for all patients was 10.4%. The rates of systems-based complications, CDIV complications, and mortality were low (Table 2). As mFI-5 score increased from 0 to ≥2, the rate of patients sustaining any complication increased from 5.2% to 19.4% (P < .0001, Table 2). The only systems-based complication impacted by mFI-5 score was the wound complication group. The rate of sustaining a wound complication was 0.2% in patients with an mFI-5 score of 0, and 1.6% in patients with an mFI-5 score ≥2 (P = .02; of note, there were no wound complications in patients with an mFI-5 score of 1).
Bivariate Analysis: Adverse Outcome Versus mFI-5 Score.

Abbreviations: mFI-5, modified 5-item frailty index; NA, not applicable.
Statistically significant (P < .05).
Adverse discharge occurred in 8.4% (n = 87) of subjects; specifically, 3.8% of patients with an mFI-5 score of 0, 10.7% of patients with an mFI-5 score of 1, and 15.5% of patients with an mFI-5 score of ≥2 were discharged to a location other than home (P < .0001).
Risk of 30-day readmission increased significantly with higher mFI-5 scores, with a readmission rate of 0.2% in patients with an mFI-5 score of 0, 1.0% in patients with an mFI-5 score of 1, and 3.1% in patients with an mFI-5 score of ≥2 (P = .017). Mortality, reoperation, and CDIV complication rates were not associated with mFI-5 score (Table 2).
Multivariate Logistic Regression Analysis
Multivariate logistic regression demonstrated that, compared with patients with an mFI-5 score of 0, patients with an mFI-5 score ≥2 were over twice as likely to experience a complication (odds ratio [OR] = 2.28, 95% confidence interval [CI] = 1.08-4.82, P = .03; Table 3). In the stepwise model excluding race, patients with an mFI-5 score of 1 had nearly 2 times the odds of experiencing any complication (OR = 1.85, 95% CI = 1.05-3.29, P = .04), while patients with an mFI-5 score ≥2 retained over 2 times the odds of developing a complication (OR = 2.49, 95% CI = 1.20-5.17, P = .01).
Multivariate Logistic Regression for Any Complication, 30-Day Readmission, 30-Day Reoperation, Clavien-Dindo IV Complications, and Adverse Discharge (CI = 95%).
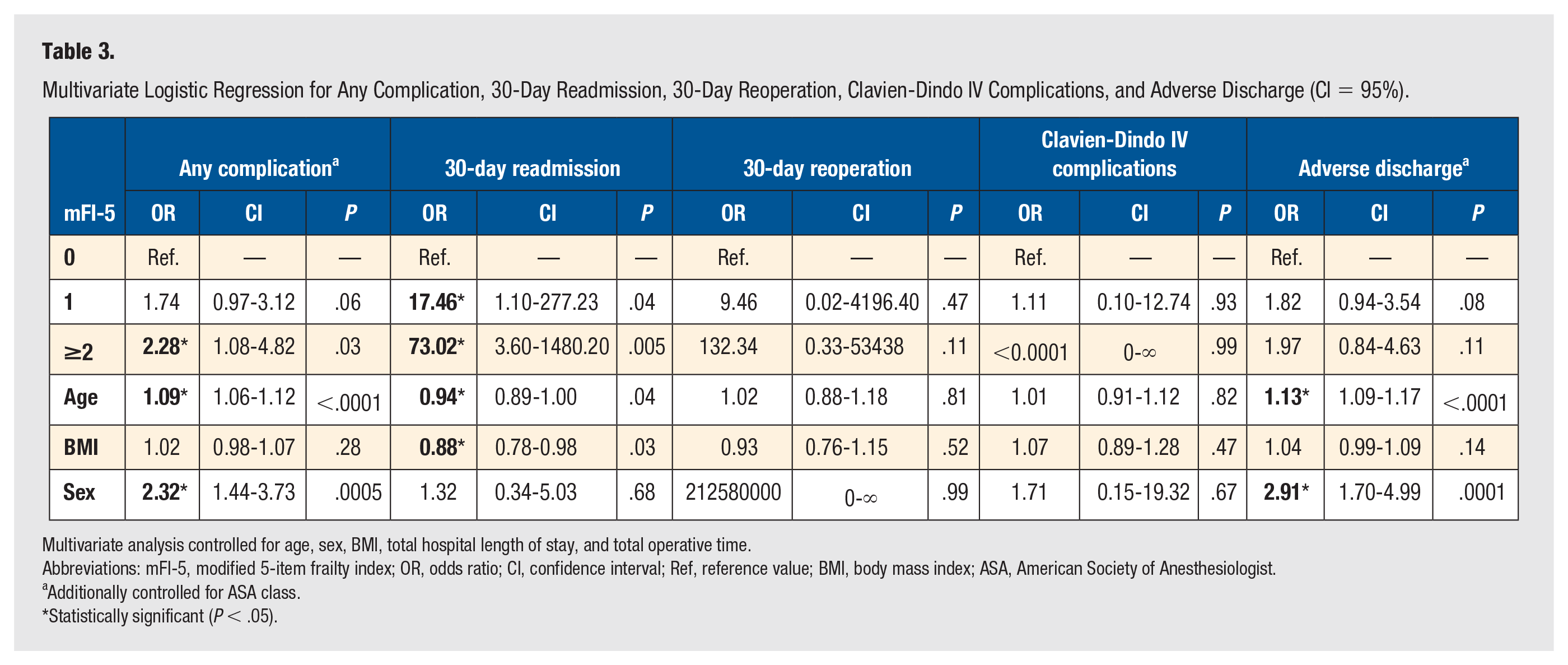
Multivariate analysis controlled for age, sex, BMI, total hospital length of stay, and total operative time.
Abbreviations: mFI-5, modified 5-item frailty index; OR, odds ratio; CI, confidence interval; Ref, reference value; BMI, body mass index; ASA, American Society of Anesthesiologist.
Additionally controlled for ASA class.
Statistically significant (P < .05).
Patients with an mFI-5 score of 1 and ≥2 had approximately 17 times (OR = 17.46, 95% CI = 1.10-277.23, P = .04) and 73 times (OR = 73.02, 95% CI = 3.60-1480.20, P = .005) higher odds of being readmitted within 30 days when compared with patients with an mFI-5 score of 0, respectively. Risk of reoperation within 30 days increased with mFI-5 score, with a marked 132 times greater likelihood in patients with an mFI-5 score of ≥2 when compared with an mFI-5 score of 0, but these findings were not significant (Table 3). The rate of adverse discharge increased with mFI-5 score, but this finding was not significant, even within the stepwise model (Table 3).
Discussion
With end-stage ankle arthritis increasingly being treated with TAA, preoperative risk factors placing patients at a higher risk of adverse outcomes must be identified. Clinical knowledge relating to risk factors is especially critical, as TAA is a relatively new and continuously evolving procedure, with an overall complication rate currently higher than what is experienced following hip, knee, and shoulder arthroplasty.22,25 This study demonstrates that frailty is associated with higher complication rates following TAA, and that the mFI-5 might be utilized as a tool to predict which patients are more likely to sustain complications. Specifically, even after controlling for possible confounding factors, the overall odds of incurring any complication were found to be nearly 2 times higher in patients with an mFI-5 score of 1, and over 2 times higher in patients with an mFI-5 score of ≥2 compared with those with a score of 0. Previous studies have shown patient factors, such as diabetes and smoking are associated with increased complication rates, and that patients with increased comorbidities as defined by the Functional Comorbidity Index (including, but not limited to chronic obstructive pulmonary disease [COPD], congestive heart failure [CHF], and diabetes) have lower surgical success rates following TAA.13,32 Thus, association of the mFI-5 with adverse outcomes following TAA is not unexpected.
While this is the first study to use the mFI-5 to investigate outcomes following TAA, several prior orthopaedic studies have helped to validate the mFI-5 as a risk-stratification tool.22 -25 The limited information required to calculate the mFI-5 in comparison with other indices enhances the clinical feasibility of utilizing the mFI-5.26 -28 Several other risk-stratification tools, such as the Charlson-Deyo comorbidity score and the Functional Comorbidity Index, exist, with increasing scores found to be associated with increased readmission rates and lower treatment success following TAA, respectively.32 -34 However, these tools require a relatively extensive amount of information regarding patient comorbidities, potentially requiring prolonged workup of patients preoperatively, and are also not commonly used within orthopaedics.
Several limitations impacted this study. Retrospective studies are unable to discern between risk factors’ association with, versus causation of, outcomes. Other inherent limitations include relying on the accuracy of information reported to the NSQIP database and being restricted to only studying outcomes of interest provided by the database. For instance, the NSQIP database limits the ability to analyze intraoperative complications, such as medial malleolus fractures, which are known to be associated with surgeon experience, but whose likelihood of occurrence may also be negatively impacted by frailty. 13 The NSQIP database also only provides information on the 30-day postoperative period, so any complications occurring after this period were not captured. There is inherent selection bias, as not every hospital participates in the NSQIP database, and among participants, the number of TAAs performed can vary greatly. 18 Thus, results may not be generalizable to hospitals or surgical centers that perform fewer TAAs, or to hospitals do not provide data to the NSQIP database.
The ease of calculating the mFI-5 can also be seen as a weakness of the index. The mFI-5 gives equal weight to each of its risk factors, and thus does not take into account the range of severity of its constituent illnesses. For example, a patient with uncontrolled diabetes requiring insulin therapy who is on several medications for hypertension would receive the same mFI-5 score as a patient with well-controlled diabetes and hypertension taking 1 oral hypoglycemic agent and 1 antihypertensive medication, respectively. However, the mFI-5’s simplicity is also one of its strengths. Virtually anyone can calculate mFI-5 score with a few questions and a brief chart review, and the mFI-5 still serves its purpose as a risk-stratification tool to facilitate informed discussions about surgical expectations and potential complications with patients preoperatively.
The sample size for this study was small compared with other mFI-5 studies, but this is not unexpected given the low incidence of ankle arthritis. The study sample was also composed of predominantly white patients; thus, results may not be generalizable to minority groups. Notably, 13.79% of black/African American patients sustained a complication, compared with 10.35% of white patients, although this finding was not significant. Only a small number of complications were recorded within this study’s data set, with the calculated overall complication rate lower than those reported by some previous studies.14,15 This finding is possibly a reflection of being unable to examine procedure-specific intraoperative and mid- to long-term complications, as previous studies on outcomes following TAA utilizing NSQIP data have reported similarly low rates of major complications. 35 CDIV complications were notably not significantly associated with mFI-5 scores, in contrast to prior mFI-5 studies, and may also be primarily explained by the overall low incidence of these complications within our study group.22 -25 High ORs and large CIs sustained within our multivariate analysis may also be explained by these low rates of complications, and possibly overestimate the actual relative risk that exists. As newer studies emerge, it would not be unexpected that complication rates continue to trend downward as implants and techniques improve and TAA more commonly becomes an outpatient procedure. 36 Regardless, the low incidence of complications in this study implies that our findings are suggestive, but not definitive, with the need for more research to provide stronger practice recommendations.
One interesting finding in this study was the identification of female sex as a risk factor for adverse discharge and any complication. This result may be in part explained by sex differences in bone density, as estrogen is a protective factor against osteopenia and osteoporosis that is largely lost after menopause, and our subjects were of relatively older age. Further research incorporating bone density measurements into frailty risk-stratification models like the mFI-5 may elucidate this finding and yield useful data. Another potential confounder to this finding may be the prevalence of inflammatory arthritis as the preoperative diagnosis for patients undergoing TAA. Inflammatory arthritis is more common in women, has historically been associated with longer LOS following arthroplasty procedures, and is a recently identified risk factor for complications following TAA.37 -39 However, in contrast to our findings, 1 recent database study including 2340 patients actually found that men are at a significantly increased risk of developing any complication within the 30-day postoperative period. 18 Investigating this factor in future studies is warranted.
This study is the first to demonstrate the utility of the mFI-5 in assessing patient risk of complications following TAA and reinforces the importance of recognizing frailty as a risk factor for adverse outcomes following orthopaedic procedures. Patients with frailty as defined by the mFI-5 were found to be at an increased risk of overall complications, 30-day readmission, and LOS. The mFI-5 has proven its value as a practical preoperative clinical tool to help assess patients’ risk of short-term complications postoperatively. Further research should be conducted to investigate the mFI-5’s capability of predicting complications specific to TAA prospectively, as well as long-term outcomes following TAA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vinod Panchbhavi is a consultant for Stryker Orthopaedics as well as an editor for Lippincott Williams and Wilkins Publishing. The other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.