
Abstract
Background
Modified Lapidus arthrodesis (MLA) is a well-established treatment option for symptomatic hallux valgus deformity (HVD). However, recurrence of the deformity remains a concern. The goal of this study was to evaluate the effect of an additional intermetatarsal fusion on the radiographic recurrence rate after first tarsometatarsal (TMT-I) arthrodesis.
Methods
This is a retrospective evaluation of 56 feet that underwent TMT-I arthrodesis for moderate to severe HVD. Twenty-three feet received an isolated arthrodesis of the TMT-I joint (TMT-I), whereas 33 feet received an additional fusion between the base of the first and the second metatarsal bone (TMT-I/II). Various radiological parameters were determined preoperatively, 6 weeks and at a mean of 2 years postoperatively.
Results
The intermetatarsal angle (IMA) and the hallux valgus angle (HVA) were significantly lowered at both follow-up evaluations in both groups. In the TMT-I/II group, the initial reduction of HVA was significantly higher (29.3° vs 21.1°). This difference disappeared by the second follow-up, leaving no significant differences between both techniques at final follow-up. Radiological recurrence rates of HVD were comparable in both groups.
Conclusions
Isolated TMT-I arthrodesis provides reliable radiological results in the correction of HVD. Whether additional fusion of the first and second metatarsal base should be routinely performed remains unclear.
Levels of Evidence:
Level 3
“The MLA has become a well-established treatment modality for moderate to severe HVD leading to a patient satisfaction between 74% and 96%.”
Introduction
With a prevalence of 23% to 38% hallux valgus deformity (HVD) represents the most common surgically corrected deformity of the foot.1 -4 Relapse of the deformity is one of the most common problems after HVD correction with rates reported up to 25%.5,6 The risk of recurrence depends on several factors, among which the choice of surgical technique with its inherent capacity for reduction plays an important role. In this context, fusion of the first tarsometatarsal (TMT-I) joint, also known as modified Lapidus arthrodesis (MLA), is a well-established treatment modality for symptomatic HVD with low recurrence rates and good clinical outcomes.7 -9 While Lapidus performed the arthrodesis of the first TMT-I joint without rigid internal fixation, the MLA is nowadays fixed with screws and/or plates. Even with a fused TMT-I, recurrence of metatarsus primus varus and/or HVD is still possible. Therefore, reports seeking additional intermetatarsal or intercuneiform stabilization have gained increasing attention in recent years.10 -14 To improve stability and to reduce recurrence of intermetatarsal instability, an intermetatarsal screw from the base of the first metatarsal to the base of the second metatarsal or the middle/lateral cuneiform has been suggested by various authors.11,15 -19 However, radiological studies concerning the outcome of intermetatarsal fusion by interposition of autogenous bone and an additional screw from the base of the first to the base of the second metatarsal are still rare and to the best of our knowledge are based only on case series.15,20
Therefore, the goal of this retrospective study was to compare various radiographic parameters after MLA with and without additional fusion of the first and second metatarsal base. We hypothesized that additional fixation of the first and second ray might lower the overall recurrence rates of HVD.
Methods
The study design received approval by the Institutional Review Board and the local Ethics Committee. We retrospectively enrolled 56 patients who had painful moderate-to-severe HVD and were treated with the MLA in 2017 at 2 orthopaedic institutions, both performing more than 400 foot and ankle procedures per year (Table 1). The indication for surgical treatment was based on both clinical and radiological examination. Concerning the latter, an intermetatarsal angle (IMA) of 16° to 20° and/or a hallux-valgus-angle (HVA) of 20° to 40° were considered a moderate and an IMA > 20° and/or a HVA > 40° were considered a severe HVD.4,21 Recurrence of deformity was defined as IMA > 10° and HVD > 20° after final follow-up. All patients suffered from pain in the affected area, and no surgery was performed for aesthetic reasons only. Exclusion criteria were previous operations for HVD, additional correction of hindfoot pathologies during the hallux valgus surgery or lack of preoperative radiographs under full weight-bearing in 2 planes. Patients were matched to 2 groups depending on the chosen procedure: isolated fusion of the TMT-I joint (TMT-I) or additional fixation and fusion of the first to the second metatarsal base (TMT-I/II). The procedure and method of fixation were chosen according to surgeons preference without evaluating objective criteria such as first-to-second ray instability, the extent of HVD/IMA or bone quality.
Patient Demographics and Characteristics.
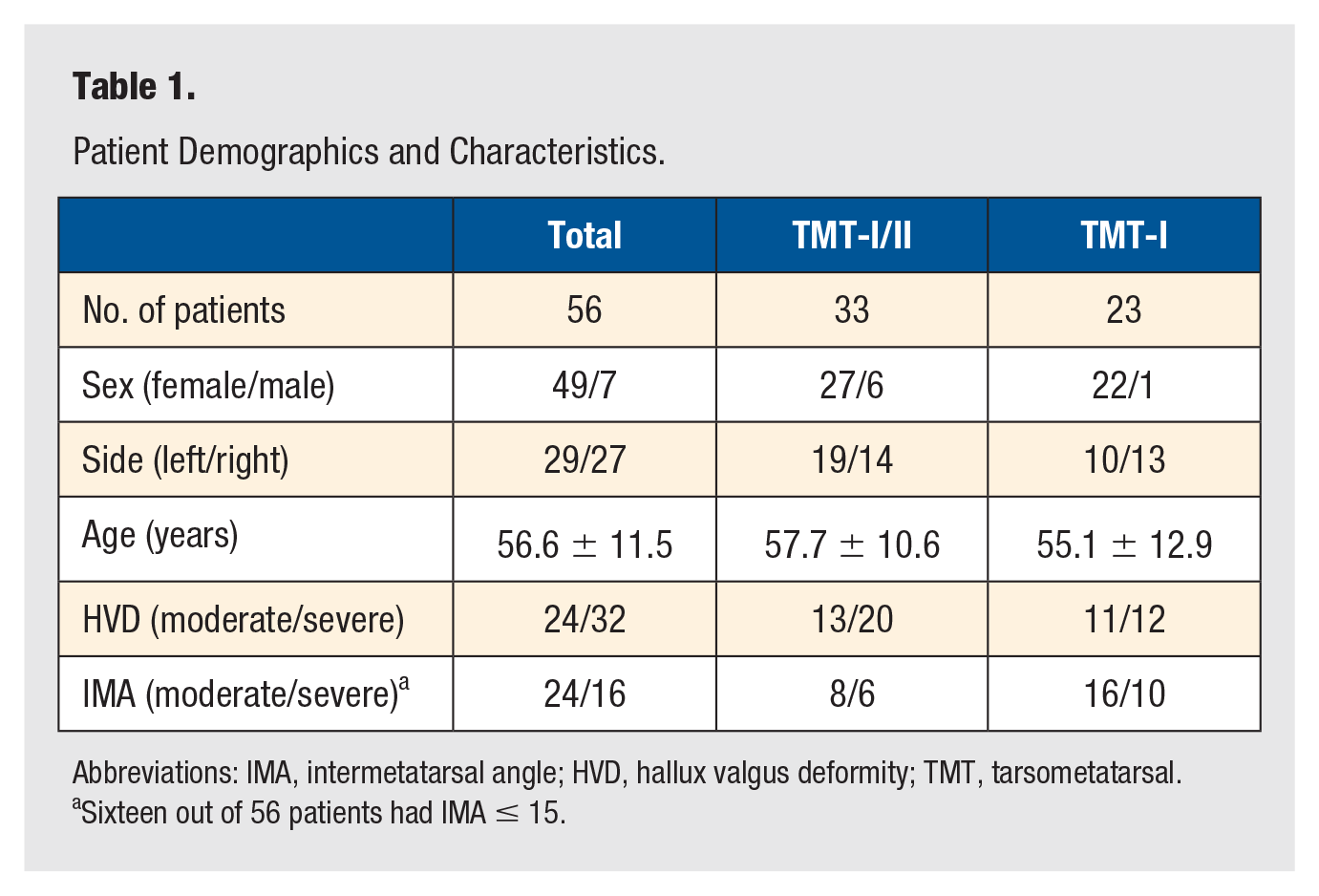
Abbreviations: IMA, intermetatarsal angle; HVD, hallux valgus deformity; TMT, tarsometatarsal.
Sixteen out of 56 patients had IMA ≤ 15.
All surgeries were performed under general anesthesia (with additional foot block for postoperative analgesia) by 2 fellowship-trained foot and ankle surgeons.
Postoperatively, all patients were kept in a below-knee boot for 6 weeks, with partial weight-bearing for the first 3 weeks and transitioning to full weight-bearing for the subsequent 3 weeks.
The radiological assessment consisted of standard radiographs of the foot in 2 planes under full weight-bearing using a fully digital device (DRX-1 System, Carestream Health Deutschland GmbH, Germany). For the dorsoplantar radiographs, the central beam was oriented 20° obliquely anteriorly from vertical. For the mediolateral radiograph, the central beam was aligned horizontally in the middle of the foot (55 kV; 2 mAs). Examinations were performed before surgery, at 6 and 12 weeks, and at final follow-up (mean 25 months, range 18-36 months).
Analysis of standard radiographs was performed using DICOM PACS System (IDS7 PACS, Sectra AB, Linköping, Sweden). All measurements were done manually by 2 independent authors of the study on 2 separate occasions, randomizing the order of the images. Each observer made the measurements independently and was blinded to both patient identification and the other’s results.
The following measurements were taken on dorsoplantar radiographs (Figure 1–3):
Intermetatarsal angle (IMA): Angle between the anatomical axis of the first and second metatarsal bones.
Hallux valgus angle (HVA): Angle between the anatomical axis of the first metatarsal bone and the proximal phalanx.
Distance between first and second metatarsal head (MI/II): Distance between the most lateral aspect of the head of the first metatarsal bone and the anatomical axis of the second metatarsal bone.
Tibial sesamoid position (TSP): Distance of the lateral edge of the lateral sesamoid bone to the anatomical axis of the second metatarsal bone.

Intermetatarsal angle (IMA): Angle between the anatomical axis of the first and second metatarsal bones on a dorsoplantar radiograph in a standing position with full weight-bearing.

Hallux valgus angle (HVA): Angle between the anatomical axis of the first metatarsal bone and the proximal phalanx on a dorsoplantar radiograph in a standing position with full weight-bearing.

Assessment of the distance between the most lateral aspect of the head of first metatarsal and the axis of the second metatarsal (Distance MT1-MT2) and the distance of the lateral edge of the lateral sesamoid to the axis of the second metatarsal (tibial sesamoid position [TSP]) on a dorsoplantar radiograph in a standing position with full weight-bearing.
On the mediolateral radiograph, the elevation angle (ELEA) of the anatomical axis of the first metatarsal bone in relation to a line parallel to the ground was assessed (Figure 4).
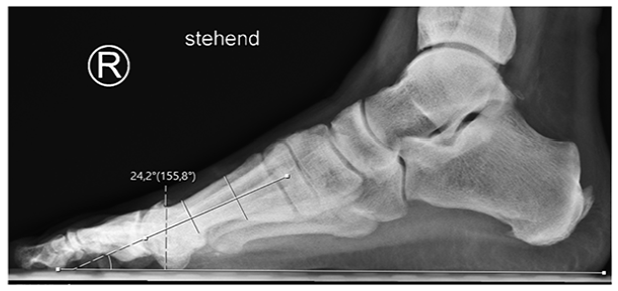
Elevation angle (ELEA) of the anatomical axis of the first metatarsal bone in relation to a line parallel to the ground assessed on a mediolateral radiograph in a standing position with full weight-bearing.
Surgical Technique
A medial longitudinal incision from the first cuneiform to the proximal phalanx was used as the preferred approach. The first metatarsophalangeal joint was opened, the pseudoexostosis resected, and a transarticular release of the lateral joint capsule, the metatarsosesamoidal ligaments, and the adductor hallucis tendon were performed. In both methods, the TMT-I joint was prepared for fusion in a routine manner (chisel, saw), with the difference that in TMT-I/II patients, the TMT-I joint was opened with a K-wire distractor and the lateral part of the second metatarsal base was slightly decorticated with a chisel. Then autogenous cancellous bone of the previously resected pseudoexostosis was impacted between these bones. The following steps were the same for both methods. The first metatarsal was reduced to be as parallel as possible to the second metatarsal and temporarily fixed with K-wires. After fluoroscopic control, a lag screw was inserted to compress the former TMT-I joint. Depending on surgeon preference, a mediodorsal or plantar plate was used to further stabilize the TMT-I joint. In TMT-I/II patients, a screw to the second ray was passed into the base of the second metatarsal and sometimes in the second cuneiform as well (Figure 5). Finally, a medial capsuloraphy of the first metatarsophalangeal joint was carried out, and an Akin Osteotomy was added in all cases. Wound closure in a layered fashion was performed.

Overview of the 2 groups: Isolated fusion of the TMT-I joint (TMT-I, left) and an additional fixation and fusion of the first to the second metatarsal base (TMT-I/II, right). In this case, an additional screw in the second cuneiform was used as well.
Statistics
Results are presented as absolute numbers, means, and standard deviations. Prior to analysis, Gaussian distribution was verified using Kolmogorov-Smirnoff testing. Differences between the means and all other parameters in both groups were determined using analysis of variance (ANOVA). A Bonferroni correction was used as a post-hoc test (P < .05: significant). The gender distribution and severity of HVD was analyzed using the chi-square test. The interobserver reliability was determined using Pearson correlation analysis, the intraobserver reliability was assessed with ICC (Intraclass Correlation Coefficient). Interobserver and intraobserver reliability was classified as minimal (correlation coefficient (CC) ≤ 0.25), low (0.26 < CC < 0.5), moderate (0.5 ≤ CC < 0.7), high (0.7 ≤ CC < 0.9), and excellent (CC ≥ 0.9). 22 All analyses were performed with GraphPad Prism 5 (GraphPad Software, Inc., La Jolla, USA).
Results
Both groups were comparable with respect to age, sex and, except for MI/II, severity of deformity (Table 1).
All TMT-I and TMT-I/II procedures had fused radiographically at final follow-up, complete hardware removal was observed in 4 patients. Recurrence of deformity was observed in 5 patients in the TMT-I/II group and 4 in the TMT-I group. Compared with the preoperative situation, both HVA and IMA were P=0,090 reduced in both groups and at both follow-up examinations (Table 2 to 4). At first follow-up, the HVA was significantly lower in the TMT-I/II group than in the TMT-I group (12.0° vs 20.0°). However, as the HVA increased significantly between the 2 follow-up examinations in the TMT-I/II group (12.0° vs 15.5°), there was no significant difference in HVA between the 2 groups at final follow-up (15.5° vs 18.0°). In contrast, the correction of the IMA was maintained in both groups.
Perioperative Changes in TMT-I/II Group.
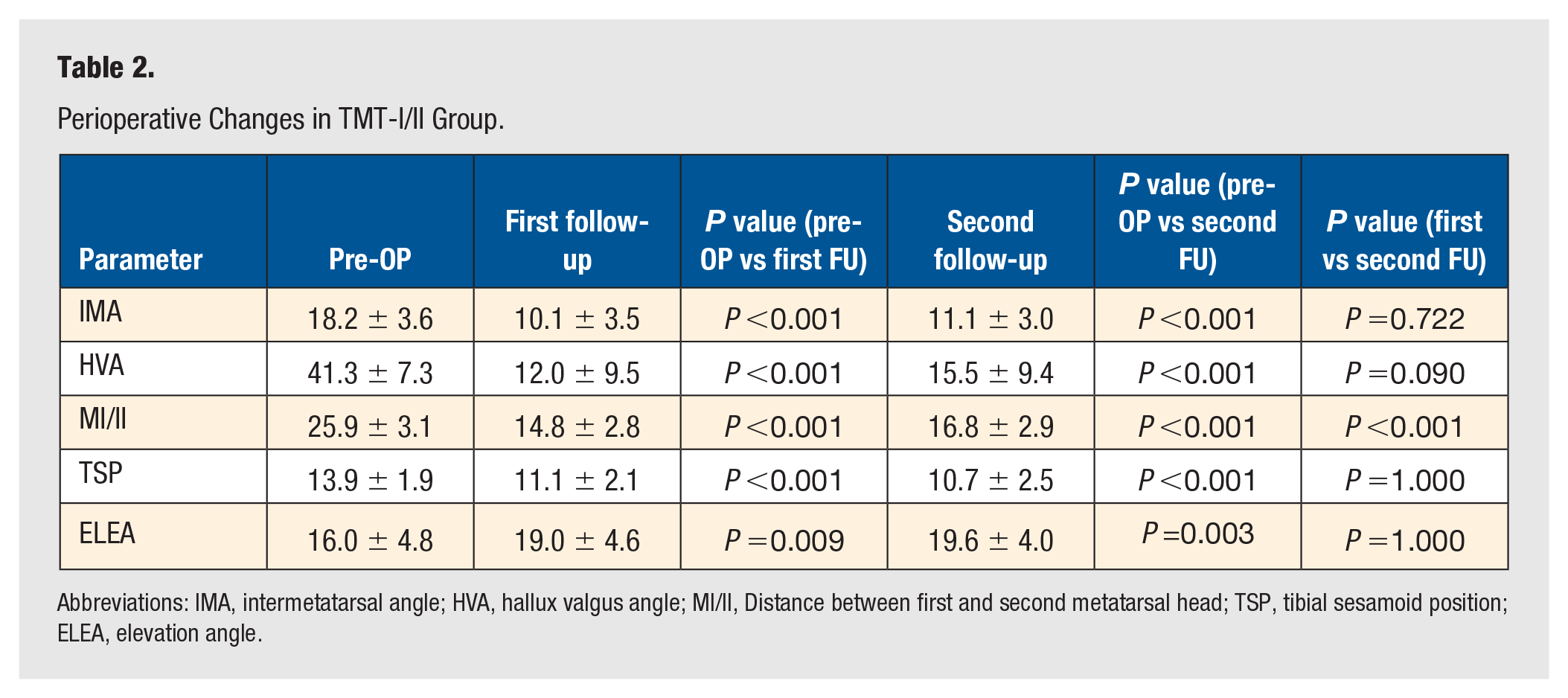
Abbreviations: IMA, intermetatarsal angle; HVA, hallux valgus angle; MI/II, Distance between first and second metatarsal head; TSP, tibial sesamoid position; ELEA, elevation angle.
Perioperative Changes in TMT-I Group.
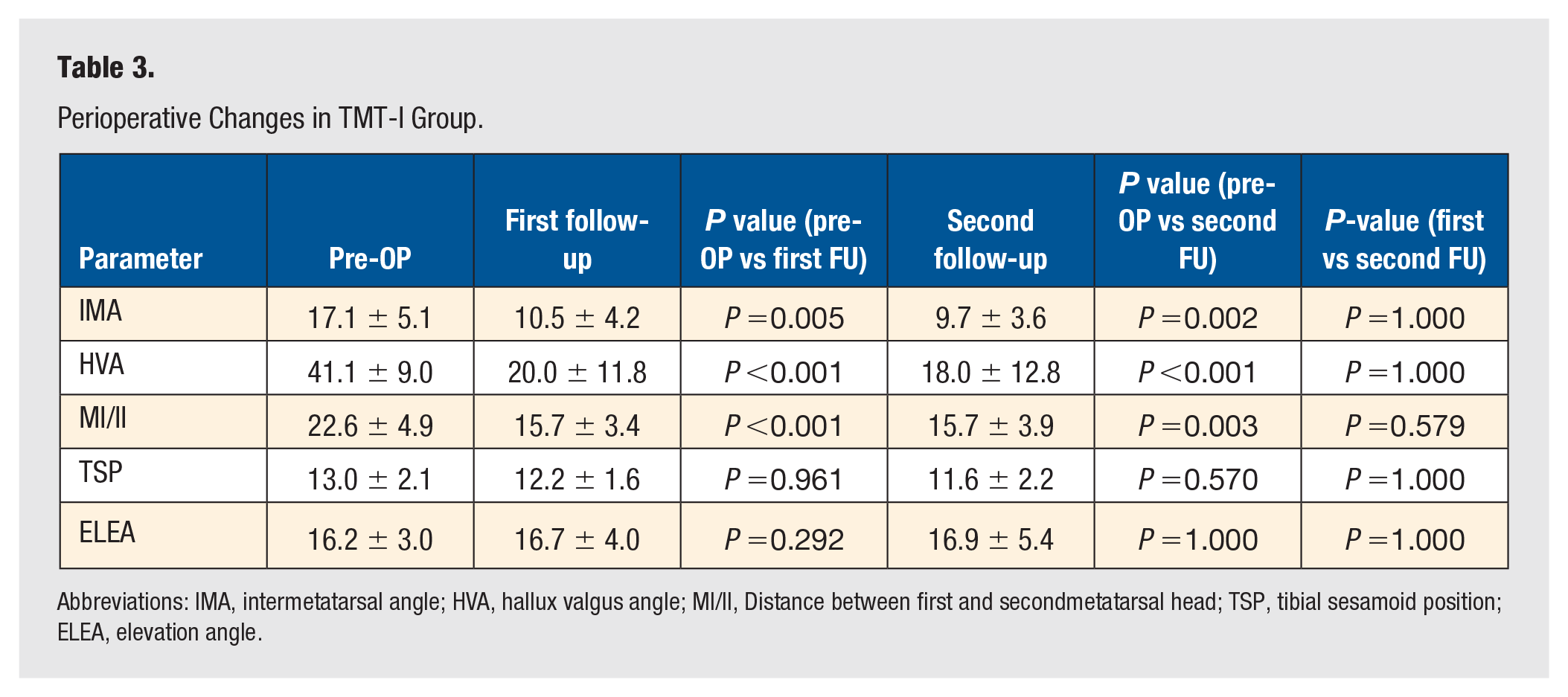
Abbreviations: IMA, intermetatarsal angle; HVA, hallux valgus angle; MI/II, Distance between first and secondmetatarsal head; TSP, tibial sesamoid position; ELEA, elevation angle.
Comparison Between Both Groups at First and Second Follow-Up Examination.
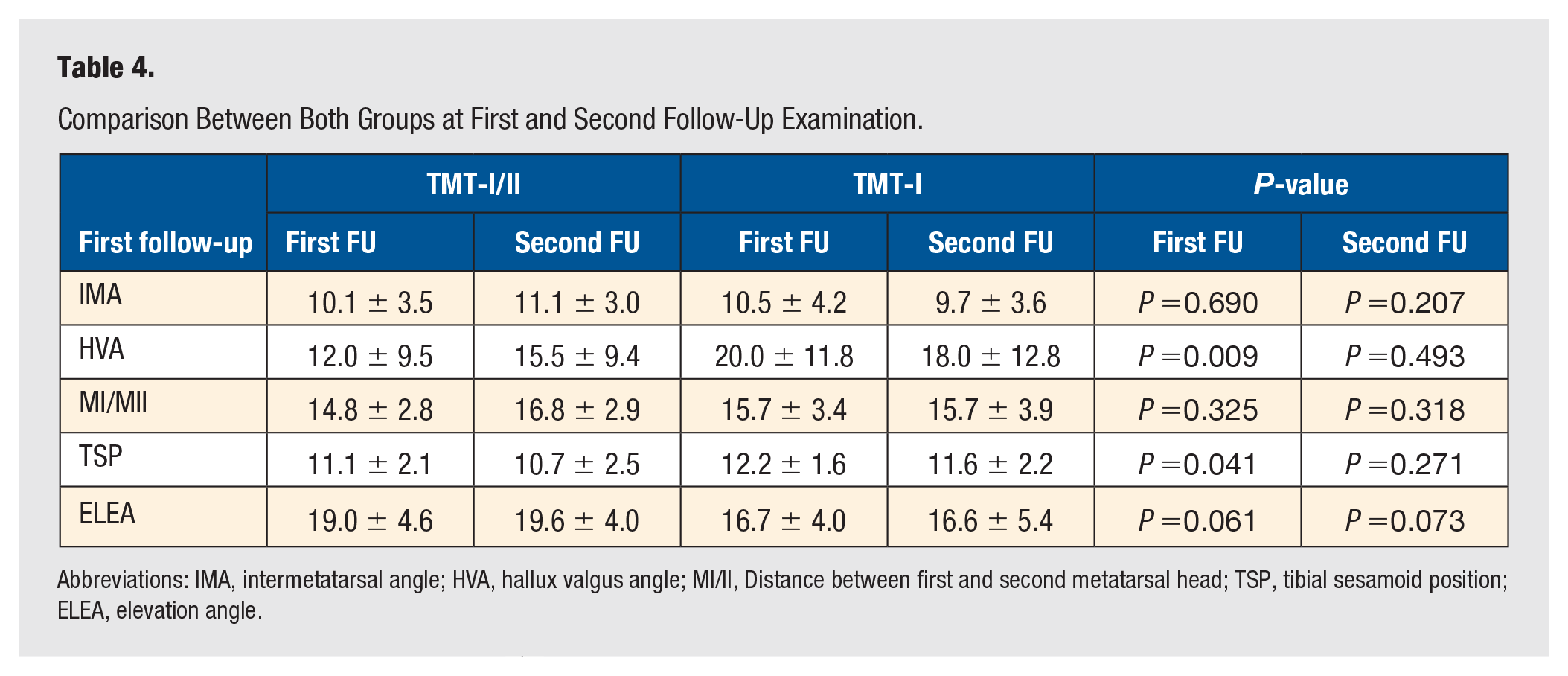
Abbreviations: IMA, intermetatarsal angle; HVA, hallux valgus angle; MI/II, Distance between first and second metatarsal head; TSP, tibial sesamoid position; ELEA, elevation angle.
The mean distance between the first and second metatarsal (MI/II) after surgery was significantly lowered in both groups at both follow-up examinations; significant differences between the groups were not detectable (Table 2 to 4). In contrast to the TMT-I group, the distance increased significantly between both follow-ups in the TMT-I/II group (14.8 vs 16.8).
The elevation angle (ELEA) was significantly increased from 16.0° to 19.0° at first follow-up in the TMT-I/II group. This alteration was maintained at the second follow-up. No significant changes were detectable in the TMT-I group throughout the observation period (Table 2 to 4).
The reliability testing (Table 5) for all parameters revealed high to excellent reproducibility of the measurements.
Intra-/Interobserver Reliability Testing (Pearson Correlation Coefficient).
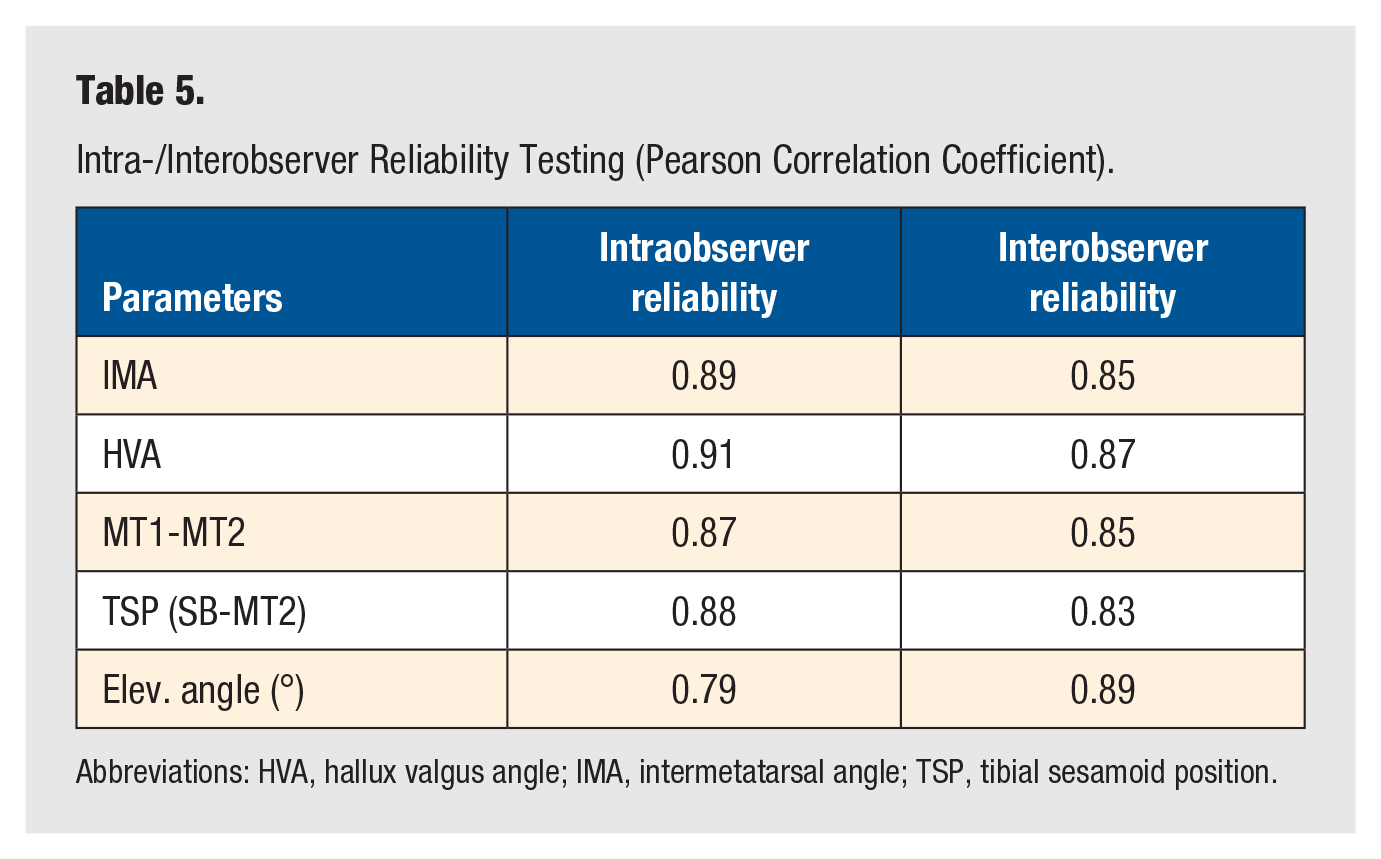
Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle; TSP, tibial sesamoid position.
Discussion
In this study, the radiological results of 2 different fixation methods of the MLA (with and without additional fusion of the first to second metatarsal base) were evaluated after a 2-year follow-up period. Despite satisfactory correction rates and no significant revalgization angles of the hallux in both groups, no relevant effect on the recurrence rate of HVD or metatarsus primus varus was found for an additional fusion of the metatarsal bases 1 and 2.
The MLA has become a well-established treatment modality for moderate to severe HVD leading to a patient satisfaction between 74% and 96%.7 -9,23 Various techniques for screw placement have been described, with a TMT-I joint crossing compression screw in conjunction with a plate usually being the preferred method.20,24 -26 Despite adequate fusion of the TMT-I joint, HVD recurrence after MLA is described in 6% to 16% of cases at long-term follow-up. 27 In this context, recurrence of an adducted first metatarsal might play a crucial role. Here, relevant intercuneiform or intermetatarsal instability has been pointed out as the major etiologic factor causing metatarsal adduction and consequently relapse of HVD. 11 To prevent this secondary loss of correction, some surgeons perform an additional fixation between the first and second ray to achieve further stability.10,11,13,28 Several techniques have been described in this regard: Screw placement between first and second cuneiform, a “Lisfranc screw” from the first cuneiform to the second metatarsal base or between the base of the first and second metatarsal bones (Table 6).10,13,29
Published Studies With Additional Screw Fixation of MLA to Intermediate (C2)/Lateral (C3) Cuneiforms or Base of Second Metatarsal (M2); M1: First Metatarsal.
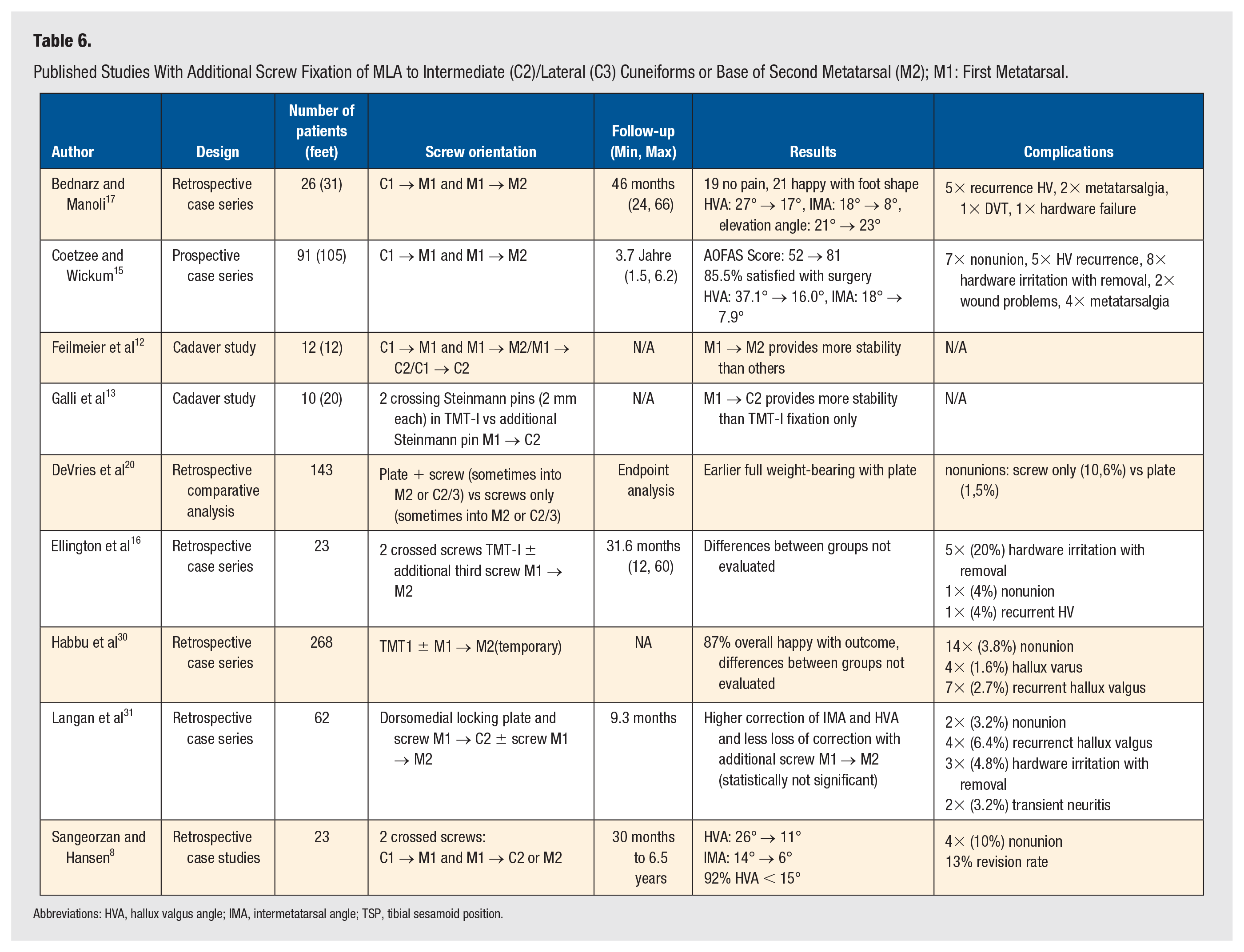
Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle; TSP, tibial sesamoid position.
Comparing biomechanical stability of different screw orientations in a cadaver study, Feilmeier et al demonstrated that the stability of the first ray after TMT-I arthrodesis can be consistently improved by an additional screw between the first and second metatarsal. 12 Intermediate gain of stability is possible if the screw is placed from the first metatarsal into the second cuneiform (confirmed by the study of Galli et al 13 ), and no relevant stability is obtained if the screw is placed from the first to the second cuneiform. However, these biomechanical findings seem reasonable, but so far clinical studies are rare. Sangeorzan et al and Coetzee et al were one of the first to use an intermetatarsal screw to enhance the rigidity of the Lapidus arthrodesis and to treat intercuneiform instability.8,32 Fleming et al 11 reported intercuneiform instability in more than 70% of their Lapidus procedures treated with intermetatarsal screw fixation. These authors found few complications with their concept of targeting instability between the first 2 rays. Nevertheless, it seems worth mentioning that the placement of an intermetatarsal screw is not without risk, as the deep peroneal nerve and the dorsalis pedis artery are located close to the TMT-I.33,34 So et al 35 identified that the intermetatarsal screw traversed the neurovascular bundle in 1 out of 10 specimens. In the remaining 9 specimens, the neurovascular bundle was located 7.1 ± 3.3 mm dorsal to the screw. Although this complication appears to be of little clinical relevance, the risk of injury to the neurovascular bundle should be considered in clinical decision-making.
In our study, we tried to substantiate the concept of intermetatarsal fusion in conjunction with the MLA by including a control group without additional fixation of the first to the second metatarsal (TMT-I group). Radiological success of the surgical procedure was demonstrated using established radiological indicators for both groups: IMA and HVA were reduced at final follow-up. These findings are in accordance with previous studies evaluating the success of the modified Lapidus procedure.7,8,16,36,37 Interestingly, our results indicate that the additional intermetatarsal screw fixation with fusion of the first and second metatarsal base results in a higher initial reduction of HVA compared to the TMT-I group (29.3° vs 21.1°). This could be at least partly explained by the compression effect of the intermetatarsal screw alone because all patients in both groups received an additional Akin osteotomy and a medial capsuloraphy of the first metatarsophalangeal joint. However, due to a higher loss of correction in the TMT-I/II group in terms of the distance between the first and second metatarsal (MTI/II) and HVA, this difference was not maintained until the second follow-up. Hence, no significant differences between the 2 surgical techniques were detectable at the end. Therefore, these radiological results would not confirm any benefit of an additional intermetatarsal fusion. In this context, loss of correction after MLA has been described by several authors, and risk factors have also been identified.5,6 Even though some authors found constant long-lasting reduction rates of HVD after intermetatarsal fusion, our findings did not support this benefit. 15
To evaluate stability in the sagittal plane, the ELEA of the first metatarsal was measured. We found no significant changes of the ELEA from the first to second follow-up in both groups, except for a minimal increase in the TMT-I/II group after the operation. This indicates a slight plantarization of the first metatarsal in this group. However, it can be stated that both methods in this study provided stable fixation of the most distal aspect of the medial longitudinal arch, independent of intermetatarsal fusion.
The main limitations of our study include the retrospective design and small number of patients. However, most relevant studies with similar questions do have comparable patient numbers (Table 5); nevertheless, studies with higher numbers are needed to confirm our findings. Another weakness of our investigation is the lack of clinical data regarding the outcome of our patients. Even though it is generally accepted that the reduction of HVD correlates with clinical outcome in most cases, we did not collect clinical outcome data in our cohort. Nevertheless, this has to do with form and function. If correction of HVD is incomplete, limitations in hallux function are likely to persist. Another drawback of our study is the mean follow-up of 2 years, which allows only medium-term conclusions. However, previous studies have demonstrated that the greatest loss of correction occurs within the first year and remains rather constant thereafter.27,38
In conclusion, this study does not support the theory that an additional screw and concomitant fusion between the first and second metatarsal base can generally reduce the loss of correction or improve midterm radiographic success after MLA. In the clinical setting, some authors take an individual decision whether to place the additional intermetatarsal screw or not after an intraoperative clinical assessment of hypermobility between the MT-I and MT-II. Nevertheless, the study cannot provide the statement that an additional screw is entirely unnecessary, as recurrence of metatarsus primus varus or HVD can still occur. Further high-quality studies are needed to provide more information on this topic.
Footnotes
Authors’ Note
Christian Kinast is now affiliated to ATOS Klinik München, Munich, Germany.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approval of local ethics committee (TU Munich) was obtained (approval no. 2015/143/16).
Informed Consent
All patients signed an informed consent form.
Consent for Publication
All authors agreed to publish. Written consent has been obtained from all patients.
Availability of Data and Material
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.