
Abstract
Background
The aim of the study is to investigate the differences between the extensile lateral (EL) and sinus tarsi (ST) approaches for the treatment of displaced intra-articular calcaneus fractures as treated by a single surgeon.
Methods
A retrospective cohort study performed at a Level 1 trauma center. One hundred twenty-nine consecutive intra-articular calcaneus fractures from 2011 to 2018 that were surgically treated by a single surgeon. Primary outcomes were time to surgery, operative time, postoperative restoration of the critical angle of Gissane, postoperative wound complications, and need for unplanned re-operation.
Results
Patient characteristics, including demographics, mechanism of injury, and fracture patterns were similar between the EL and ST approach groups. There was a significant decrease in unplanned secondary procedures (P = .008), shorter time to definitive fixation (P = .00001), and shorter average operative time in the ST group (P = .00001). Postoperative measurement of the critical angle of Gissane between the two groups was significantly different, but minute with an average difference of approximately 3 degrees (P = .025). Measurements in both groups were within the expected range of normal.
Conclusions
For displaced intra-articular calcaneus fractures, a limited open ST approach is associated with a significant reduction in the time to definitive fixation and decreased operative time. The EL approach was associated with a small, but significant improvement in the restoration of the critical angle of Gissane compared with the ST approach. Therefore, an ST approach may allow for earlier surgical intervention and result in equivalent quality of reduction compared with an EL approach.
Level of Evidence:
Level III
“Displaced, intra-articular calcaneus fractures can be treated via a limited ST approach with satisfactory restoration of calcaneal morphology with a shorter operative time and a decrease in woundrelated complications”
Introduction
The surgical treatment for displaced, intra-articular calcaneal fractures may often be challenging and rife with complications.1-12 The extensile lateral (EL) approach is the most common approach used for open reduction and internal fixation (ORIF) of intra-articular calcaneus fractures, offering the surgeon excellent visualization of the posterior facet and lateral wall. However, studies have described a complication rate as high as 37%, which is largely attributed to the tenuous blood supply to the lateral hindfoot during this approach.2,4,5,8,13 With the EL approach, there is the risk of devitalizing the soft tissue flap in addition to the lateral wall. Performing a tension free closure and meticulous soft tissue handling are paramount when using the EL approach.
The past few decades have seen an introduction of less invasive techniques, such as percutaneous fixation that have been popularized for their reduction in soft tissue complications particularly in patients with multiple comorbidities, including diabetes, peripheral vascular disease, and a history of tobacco use.14 -20 Chief of these techniques is the sinus tarsi (ST) approach that is performed through a limited incision from the tip of the lateral malleolus, in line with the fourth ray, and ends at the level of the calcaneocuboid joint (Figure 1). The primary benefit to this approach is minimal soft dissection particularly of the lateral skin of the hindfoot and several studies have demonstrated lower wound complication rates and decreased surgical time with the ST approach.14 -23 However, few studies have compared the EL and ST approaches for comminuted, displaced, intra-articular fractures, including AO-OTA 82-C3 (Sanders type IV) fractures. These severely comminuted fracture patterns have been associated with poor outcomes even with open treatment and acute arthrodesis should be highly considered.11,24

The location of the sinus tarsi incision (between arrow heads). Fibula (solid line) and approximate location of sural nerve (dotted line) are outlined.
The purpose of this study was to review a single surgeon’s experience with the EL and ST approaches in treating displaced intra-articular calcaneal fractures over a 7-year period, including AO-OTA 82-C3 (Sanders type IV) calcaneus fractures. We hypothesized that the ST approach would result in similar postoperative radiographic outcomes, while resulting in a reduction of operative time and wound-related complications.
Patients and Methods
After institutional review board approval, all intra-articular calcaneal fractures treated by the senior author were reviewed over a 7-year period (2011-2018). Inclusion criteria included displaced, intra-articular calcaneal fractures treated with an EL or ST approach with a minimum of 3-month follow-up with complete clinical and radiographic records. A total of 129 fractures were included in the study. Patient demographics and injury characteristics obtained included age, gender, body mass index (BMI), medical, and social history (such as diabetes, vascular disease, tobacco, and drug use), mechanism of injury, presence of ipsilateral extremity injury, and presence of an open or closed fracture. Use of staged treatment, such as external fixation or acute subtalar arthrodesis, was also recorded.
Preoperative imaging included plain radiographs and computed tomography (CT). Fractures were classified by the senior author according to the AO-OTA classification. Intra-articular fracture patterns were selected, namely, AO-OTA 82-B3, C1, C2, and C3. Postoperative radiographic measurement of the critical angle of Gissane was performed by the lead and senior authors.
Outcome variables included time to definitive fixation, total surgical time, return to the operating room for unplanned procedure(s), such as hardware removal or irrigation and debridement (I&D), and measurement of the critical angle.
Data analysis was performed using Excel (Microsoft, Seattle, WA). Student’s t-test and chi-square analysis were used to evaluate for statistical significance with significance set at a P-value of less than .05. Separate data analysis was performed for unmatched and matched patient cohorts based on patient age, gender, and BMI.
Results
Unmatched Cohorts EL Versus ST
One hundred twenty-nine intra-articular calcaneal fractures were included for the unmatched cohort analysis. Fifty-six of the 129 (43%) fractures were AO-OTA 82-C3 (Sanders type IV) patterns. The EL approach was used in 55 patients and ST approach in 74 patients (Table 1). There were no significant differences between the cohorts with regards to age, BMI, and medical or social history. No significant differences were noted with regards to fracture pattern, status of open or closed fracture, ipsilateral extremity/foot injury, or use of staged treatment with provisional fixation or acute subtalar fusions.
Data for Unmatched Cohorts.
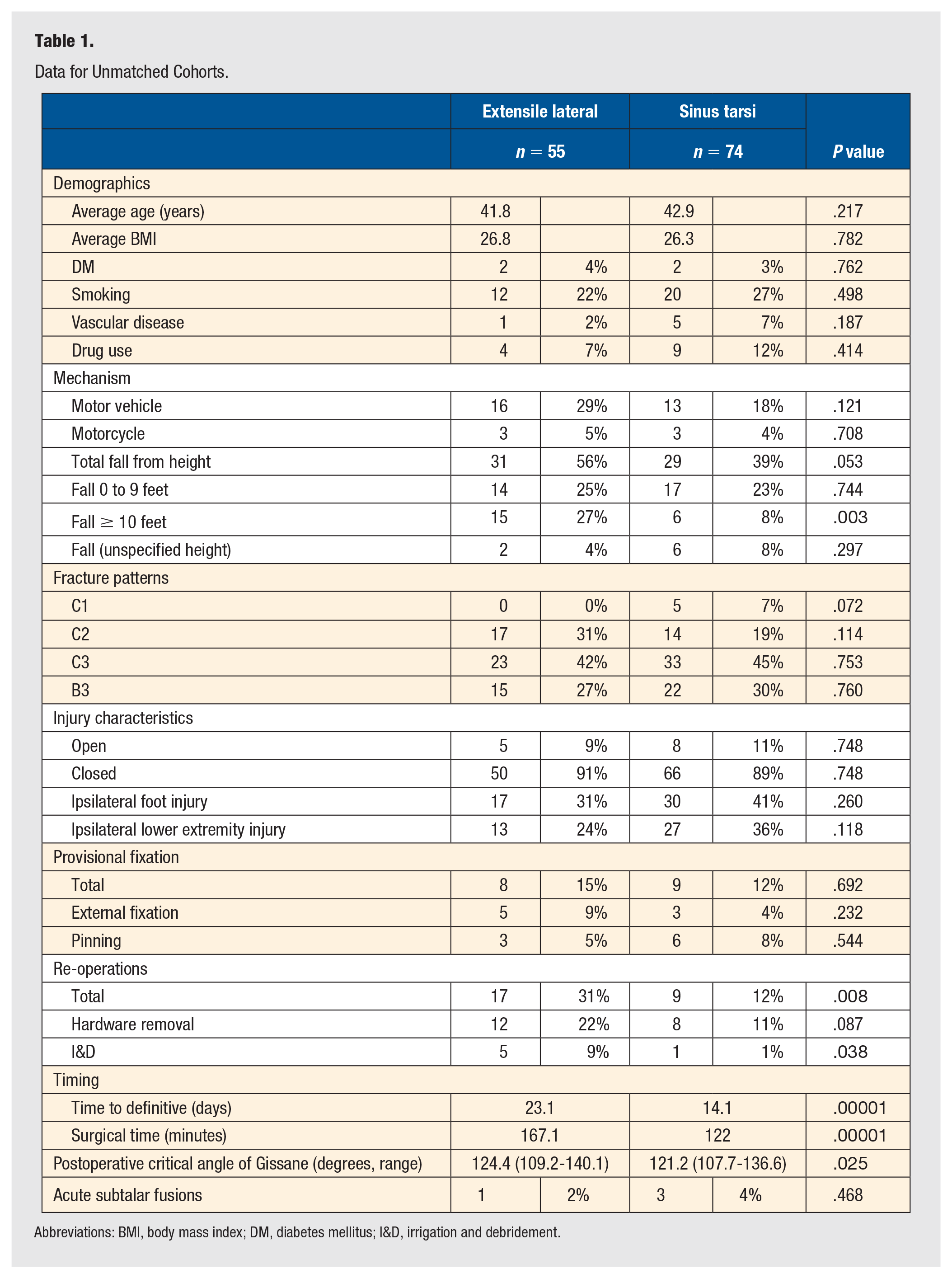
Abbreviations: BMI, body mass index; DM, diabetes mellitus; I&D, irrigation and debridement.
Overall, there was no significant difference between the two groups with regards to the mechanism of injury. However, further subgroup analysis of falls from height demonstrated significantly more fractures from a fall from 10 feet or higher in the EL group (15 vs 6, EL vs ST, respectively, P = .003) (Table 1).
With regards to surgical intervention, no difference was found with the use of provisional fixation or acute subtalar arthrodesis. However, there was a significant difference in the time from injury to definitive fixation with EL taking approximately 23 days versus 14 days for ST (P = .0001). In addition, procedures utilizing EL had significantly longer operative times (167 minutes) than ST (122 minutes, P = .0001).
There were a total of 26 cases (20%, 26/129) with unplanned secondary procedures regardless of surgical approach used. A significantly higher percentage of patients in the EL group (31%, 17/55) had secondary procedures compared with ST (12%, 9/74; P = .008). More patients in the EL group (9%, 5/55) had an I&D performed than the ST group (1%, 1/74, P = .038). There was no difference in the percentage of hardware removals (Table 1).
Postoperative radiographic measurement of the critical angle of Gissane demonstrated a significant difference between the two approaches (EL average 124.4 degrees vs ST average 121.2 degrees, P = .025).
Matched Cohorts EL Versus ST
In addition, matched cohort analysis was performed matching patients based on age, gender, and BMI between the EL and ST groups. A total of 102 calcaneal fractures were included for analysis with 51 cases each for EL and ST groups. Forty-three percent of these fractures were classified as AO-OTA 82-C3 (44 of 102). There were no statistical differences between the cohorts with regards to medical/social history, fracture patterns, open or closed fractures, ipsilateral extremity/foot injury, or use of staged treatment with provisional fixation or acute subtalar fusions (Table 2).
Data for Matched Cohorts (Patients Matched for Age, BMI, and Diabetes).
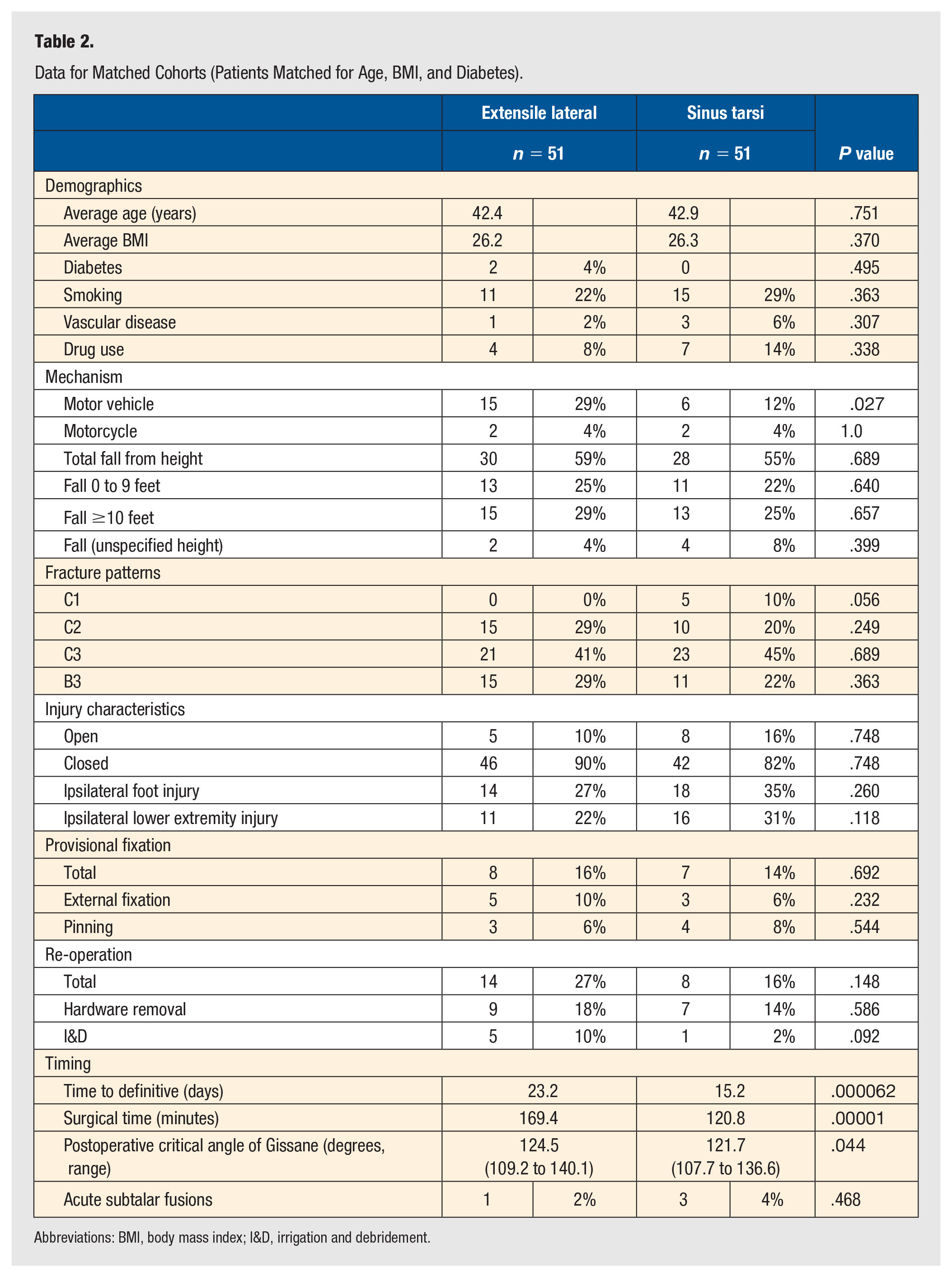
Abbreviations: BMI, body mass index; I&D, irrigation and debridement.
With regard to mechanism of injury, the EL group had more patients involved in motor vehicle collisions (29%, 15/51) compared with ST (12%, 6/51, P = .027). There was no significant difference the total number patients who fell from a height independent of the height (Table 2).
The time from injury to definitive surgical fixation was increased in the EL group at approximately 23 versus 15 days for the ST group (P = .0001). In addition, procedures utilizing EL had significantly longer operative times (169 minutes) than ST (121 minutes, P = .0001).
A total of 22 of 102 (22%) cases underwent re-operations in the matched group for either hardware removal or I&D. Although not statistically significant, there was a trend toward more secondary procedures in the EL group with 27% (14/51) needing an unplanned secondary procedure versus 16% (8/51) of the ST group (P = .148). Hardware removal rate was 18% (9/51) versus 14% (7/51) and I&D rate was 10% (5/51) versus 2% (1/51) for EL versus ST, respectively (Table 2).
Postoperative radiographic measurement of the critical angle of Gissane demonstrated a significant difference between the two approaches (EL average 124.5 degrees vs ST average 121.7 degrees, P = .044).
Discussion
We have demonstrated that displaced, intra-articular calcaneus fractures can be treated via a limited ST approach with satisfactory restoration of calcaneal morphology with a shorter operative time and a decrease in wound-related complications (Figure 2). We hypothesized a similar postoperative radiographic outcome, however, our results showed that the EL approach had a small, but significant improvement in the restoration of the angle of Gissane (approximately 3 degrees, P = .025). In review of the current orthopaedic literature, a normal critical angle range is reported between 120 and 140 degrees, and both approaches had postoperative measurements within this range.25 -27 Therefore, the small difference seen in our study may not be clinically significant. Regarding wound related complications, our results showed a significantly higher re-operation rate for wound complications after the EL approach (9%, 5 of 55) compared with the ST approach (1%, 1 of 74, P = .038).

Preoperative and postoperative images of a comminuted, depressed intra-articular calcaneus fracture treated with a sinus tarsi approach.
Several studies have demonstrated the utility and efficacy of minimally invasive approach for the treatment of displaced intra-articular calcaneal fractures.15,16,21 -23 One of the earliest comparative studies by Weber et al 23 described 50 patients with Sanders type II and type III calcaneus fractures. Twenty-four were treated with an ST approach, while 26 were treated with an EL approach. There were no significant differences in clinical outcome. However, they found significantly shorter operative times and increased rate of hardware removal in the limited open group. The authors reported that the less invasive technique became their standard technique for all operative calcaneus fractures.
Xia et al 24 compared the two approaches for 117 calcaneal fractures in a randomized control trial and found decreased surgical times and equivalent postoperative radiographic measurements. More recently, a study of 125 calcaneus fractures by Schepers et al 21 utilized postoperative CT scans to evaluate the quality of reduction. They found comparable restoration of anatomy in both groups with two cases of minimal step off in the EL group and none in the ST group. Other anatomical characteristics, such as varus/valgus, calcaneal width, and restoration of Bohler’s angle were similar between the two groups. A subsequent retrospective comparative study by Kline et al 16 reviewed 112 Sanders type II and type III calcaneal fractures, 79 of which were treated with EL approach and 33 via ST approach. They reported a 29% versus 6% wound complication rate in the EL versus ST approach, respectively. In addition, no significant differences were noted in their postoperative measurements of Bohler’s angle and critical angle of Gissane. A recent meta-analysis by Yao et al 28 in 2017 identified a significant difference in wound complication rates with 15% incidence after the EL approach versus 0% for ST (P = .01).
To our knowledge, there has been a paucity of a large case series comparing EL and ST approaches particularly those that include AO-OTA type C3 fractures. Many of the comparative studies in the literature exclude type C3 or Sanders type IV fractures often citing a high level of intra-articular comminution that may portend a poor functional outcome and the need for acute primary arthrodesis.10,11 However, in our study, type C3 fractures accounted for more than 40% of the total number of fractures (43%, 56 of 129). In addition, for Sanders type IV or other severely comminuted patterns, an acute primary arthrodesis can also be performed through an ST approach (Figure 3).

Preoperative and postoperative radiographs of a severely comminuted intra-articular calcaneus fracture treated with an acute subtalar arthrodesis through a sinus tarsi approach.
The strengths of this study are multiple. We report on the largest single surgeon cohort of patients with intra-articular calcaneus fractures who underwent ORIF with either EL or ST approaches. All patients were treated by the senior author, using the same preoperative, perioperative, and postoperative protocols, so that, variability in treatment and decision-making were minimized. Given that this is a single surgeon study, the external validity of these results may be limited or difficult to replicate. Other weaknesses of the study include retrospective study design and potential selection bias for the approach performed by the single surgeon. Furthermore, independent evaluation of radiographs by a musculoskeletal trained radiologist would have limited bias in the measurement of postoperative radiographic parameters as this was done by the lead and senior authors. Another significant limitation is that no functional outcome scores were obtained at follow-up visits. However, none of the patients in this study underwent secondary procedures for subtalar arthrodesis at the conclusion of the data collection period for this study. A minimum follow-up period of 3 months may likely underrepresent the number of patients which may have subsequently required hardware removal at a later time point.
Overall, our results support the use of the ST approach for the acute definitive treatment of displaced intra-articular calcaneus fractures. Utilizing a minimally invasive approach may allow for earlier definitive fixation, decreased overall procedure times, and decreased wound complication rates. With careful preoperative planning, a more limited approach may result in nearly equivalent intra-articular fracture reduction, including that of AO-OTA type C3 fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Consent was not applicable to this study as this study utilized an HIPAA compliant deidentified patient database
Trial Registration
Not applicable, because this article does not contain any clinical trials.