
Abstract
Introduction
This study provides the first comparison of patient-reported outcomes between isolated cheilectomy (C) and cheilectomy with Moberg (CM) osteotomy for hallux rigidus.
Methods
A single-center, retrospective registry search identified all patients with preoperative Patient-Reported Outcomes Measurement Information System (PROMIS) scores who underwent cheilectomy, with and without concomitant proximal phalangeal dorsiflexion osteotomy, for hallux rigidus between January 2016 and December 2020. Because there were far fewer isolated cheilectomies (62), all C patients were compared with a commensurate number of consecutive CM cases (67) using preoperative, 1-year, and 2-year PROMIS scores for physical function, pain interference, pain intensity, global physical health, global mental health, and depression, as well as complication and revision data from a chart review. A multivariable linear regression analysis was performed to compare adjusted postoperative PROMIS scores between the 2 cohorts.
Results
There were no differences between groups among the demographic and preoperative variables compared. The CM cohort reported worse pain interference scores preoperatively (P < .001) and at 1 year postoperatively (P = .01). However, the C cohort reported worse pain intensity scores preoperatively (P < .001) and at 1 year postoperatively (P < .001). Adjusted postoperative PROMIS score comparison demonstrated that the CM cohort had better 1-year postoperative pain intensity scores (P < .05). However, there were no differences between cohorts for additional PROMIS scores or complications data.
Conclusion
The addition of a Moberg osteotomy does not appear to significantly change short- to medium-term outcomes of cheilectomy for hallux rigidus treatment.
Levels of Evidence:
Level III: Retrospective comparative study
“This comparative cohort analysis found that the addition of a Moberg osteotomy to cheilectomy for the treatment of hallux rigidus did not significantly change shortterm outcomes. There were no differences in the majority of PROMIS subscales or complications data.”
Introduction
Hallux rigidus is a degenerative arthritis of the first metatarsophalangeal (MTP) joint characterized by the proliferation of osteophytes at the dorsal articular surface as well as progressively increasing pain and restriction of motion at the first MTP joint. 1 When conservative treatment is ineffective, surgical treatment is offered, which may include joint-sparing procedures such as cheilectomy, interposition arthroplasty, and synthetic cartilage implantation or joint-sacrificing procedures such as first MTP arthrodesis.2-8 The choice of surgical treatment is determined by the severity and nature of the patient’s symptoms, the degree of radiographic MTP joint deterioration, and most importantly, the patient’s postoperative goals. 9
Cheilectomy is a popular procedure for early- to moderate-stage hallux rigidus as it is the least invasive treatment, allows relatively easy conversion to arthrodesis if necessary, and has been shown to meaningfully reduce pain and improve function. 5 However, while cheilectomy alone demonstrates excellent results for early- to moderate-stage hallux rigidus, gait analysis studies suggest that cheilectomy does little to alter the pathologic biomechanics of hallux rigidus, thereby rendering the first MTP joint vulnerable to further degeneration and re-emergence of arthritis.10,11
A proximal phalangeal dorsal closing wedge (Moberg) osteotomy is commonly used as an adjunctive procedure to increase dorsiflexion and has been shown to offload the diseased MTP dorsal cartilage by shifting contact pressure of the first MTP plantarly. 12 Case series suggest improved results for cheilectomy with Moberg in advanced stages of hallux rigidus. 13 However, adding a Moberg osteotomy has unique disadvantages such as increased operating time, added implant cost, and the potential for additional complications including soft tissue damage and malunions or nonunions. 14 Very few studies exist that directly compare results between the 2 treatments, and these studies, while insightful, are marked by small sample sizes and a distinct lack of patient-reported outcome measurement (PROM) data.14,15 As health care in the United States gradually transitions from fee-for-service models to increasingly value-driven incentive structures, it is imperative that foot and ankle surgeons, like other providers, consider the value of the care they provide. As a result, PROMs have been increasingly adopted by foot and ankle surgeons and researchers as central indicators of health care quality. 16
This study aims to compare 1- and 2-year PROM scores between patients who underwent cheilectomy alone and chielectomy with Moberg osteotomy for moderate-stage hallux rigidus using PROMIS, a validated patient-reported outcomes measurement system, as well as to compare rates of complications and returns to the operating room between the 2 groups. We hypothesized that patients who undergo cheilectomy with the Moberg procedure would experience better clinical outcomes and fewer returns to the operating room than patients undergoing cheilectomy alone.
Materials and Methods
Patient Selection
This single-center retrospective study reviewed the institutional review board–approved Foot and Ankle Registry, and the protocol was approved by the steering committee at the investigators’ institution. Patients who underwent open cheilectomy with or without first proximal phalangeal dorsal closing wedge osteotomy between February 2016 and December 2020 by 1 of 7 fellowship-trained foot and ankle orthopaedic surgeons were reviewed. Inclusion criteria included patients aged 18 years or older who underwent cheilectomy without interposition arthroplasty or synthetic cartilage implant arthroplasty (CARTIVA, Cartiva Inc., Alpharetta, GA) for a primary diagnosis of hallux rigidus and had PROMIS scores preoperatively. Excluded were patients without preoperative radiographs and patients with histories of previous ipsilateral forefoot surgeries, rheumatoid arthritis, or gout. Operative notes were reviewed, and all procedures performed were noted. Patients were divided into 2 cohorts of cheilectomy alone (C) and cheilectomy with Moberg osteotomy (CM) based on whether they underwent concomitant proximal phalangeal dorsiflexion osteotomy with their cheilectomy. Because fewer patients underwent isolated cheilectomy in this time period, a commensurate number of CM patients were selected by reviewing patients consecutively and including eligible patients until an adequate number of CM patients were obtained. Figure 1 summarizes the patient selection and exclusion processes for this study.
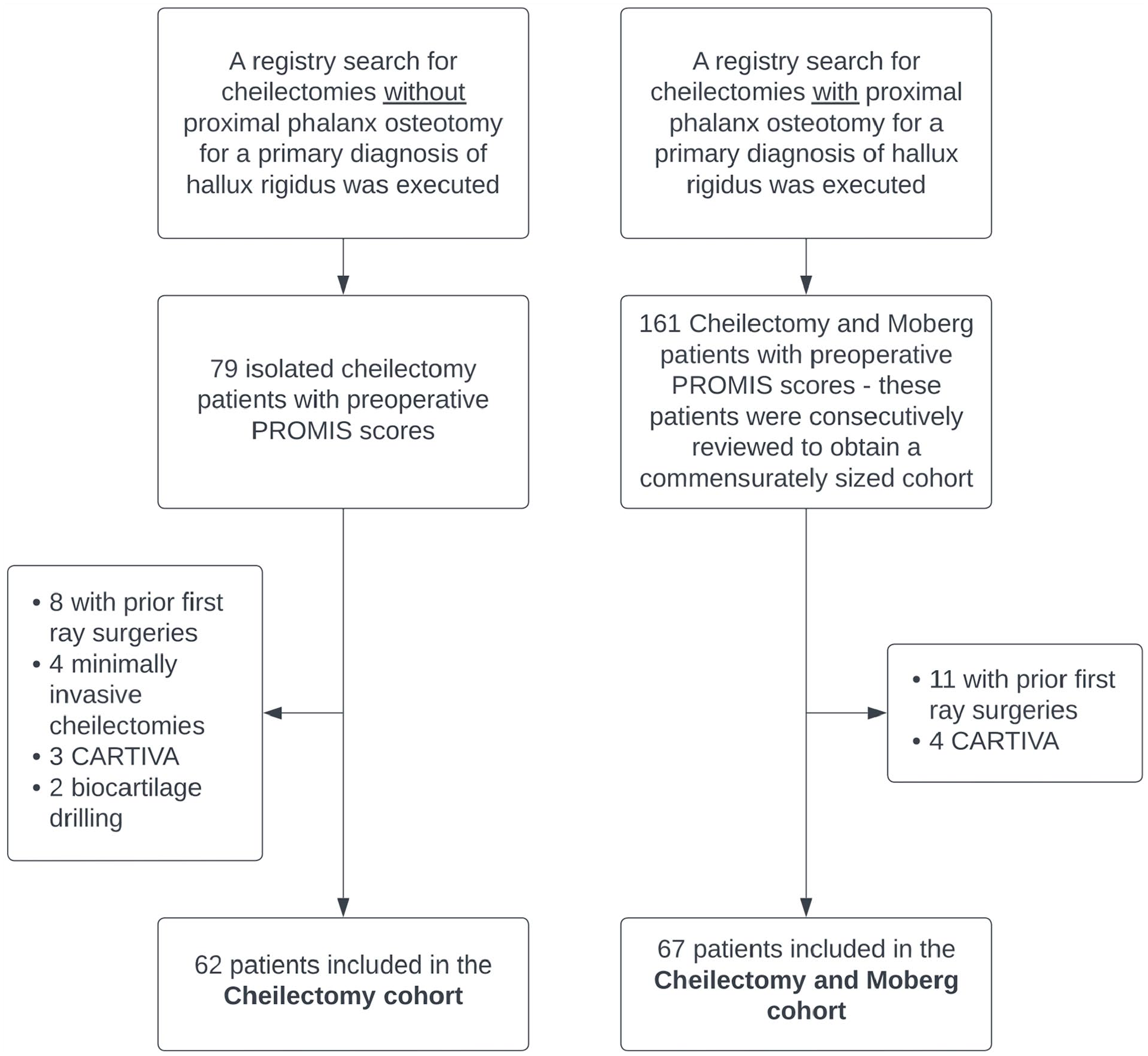
All 62 isolated cheilectomy patients with preoperative PROMIS scores were included. Of the 161 cheilectomy and Moberg osteotomy patients identified with baseline PROMIS scores, the first 67 were included for comparison to the isolated cheilectomy cohort.
Operative Algorithm
The decision algorithm on whether to pursue concomitant Moberg osteotomy alongside dorsal cheilectomy differed according to the preferences of both patients and surgeons in this study. While some surgeons opted to perform a Moberg osteotomy nearly always alongside the cheilectomy, others seldom did so. Still, other surgeons primarily based their protocol on patients’ expressed desires or a perceived likelihood of failure to comply with the longer recovery protocol necessary for a Moberg osteotomy. Therefore, although a substantial majority of patients in the registry underwent CM for early-stage hallux rigidus, there did not appear to be any systematic pattern of differences between the 2 groups.
Operative Techniques and Postoperative Protocol
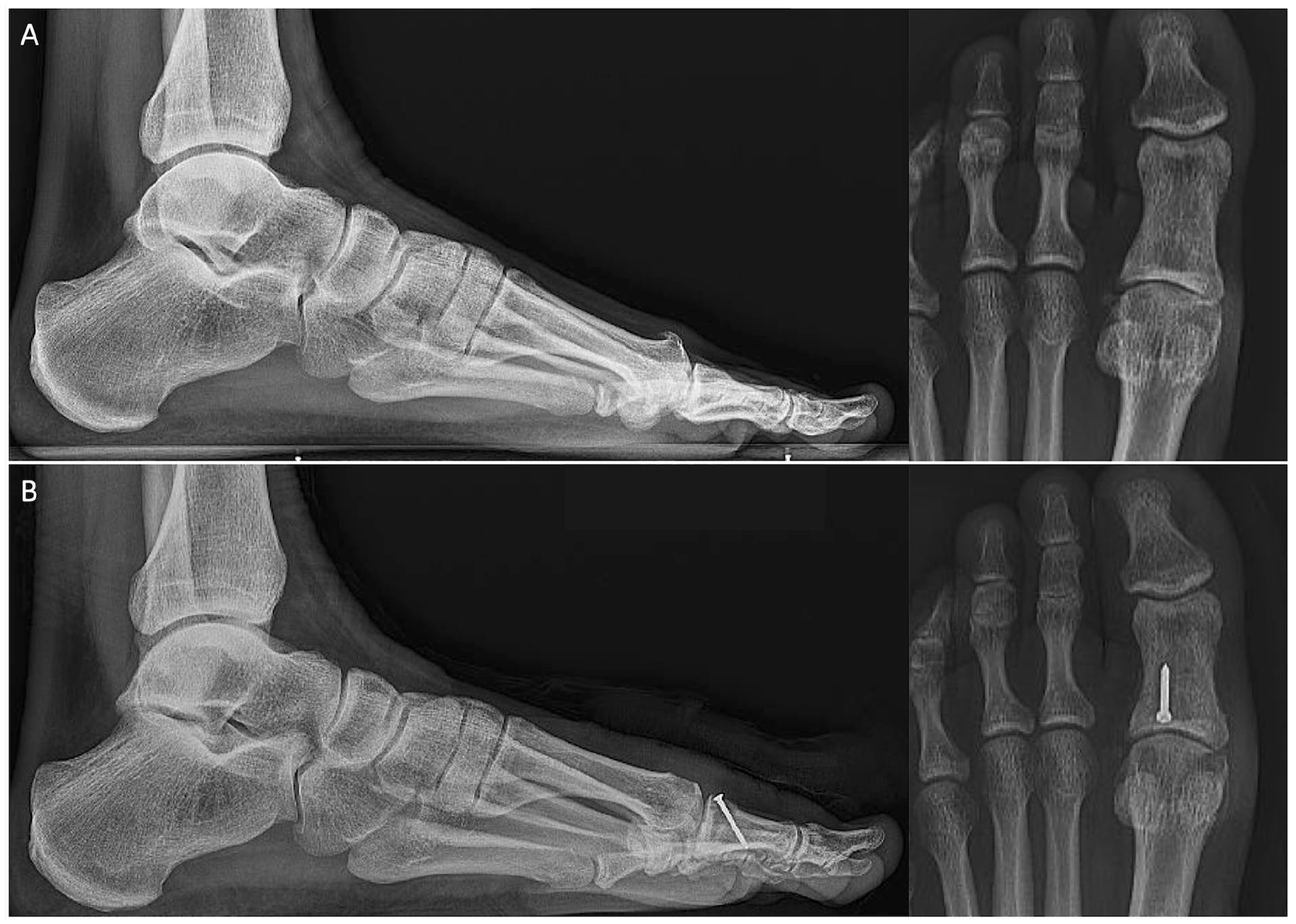
The surgical techniques used in this study were consistent with previous literature on cheilectomy with and without Moberg osteotomy.3,13 Sedation and an ankle block were used along with an ankle tourniquet. Patients were positioned supine on the operating table. A dorsomedial incision was made at the first MTP joint and carried down through the skin and subcutaneous tissue to access the first MTP joint. Dorsal osteophytes were then removed with a rongeur or saw blade, and up to 30% of the dorsal metatarsal head was excised with the saw. In patients who underwent concomitant Moberg osteotomy, a 2- to 3-mm wedge was then removed from the dorsal aspect of the proximal phalanx, preserving the plantar cortex. The wedge site was then closed and secured with a 2-mm screw or an 8-mm surgical staple. Intraoperative fluoroscopy was used to confirm correct hardware positioning (Figure 2). Some surgeons then opted to use an oscillating rasp to resurface the metatarsal head and proximal phalanx to remove any possible sharp edges. The joint capsule, subcutaneous layer, and skin were sequentially closed with suture. A soft dressing was applied to be worn with a postoperative shoe or split. Patients were either allowed to immediately bear weight or were limited for the first 2 weeks postoperatively to allow wound healing. Sutures were removed after 2 to 3 weeks, and patients were transitioned into regular shoe wear.
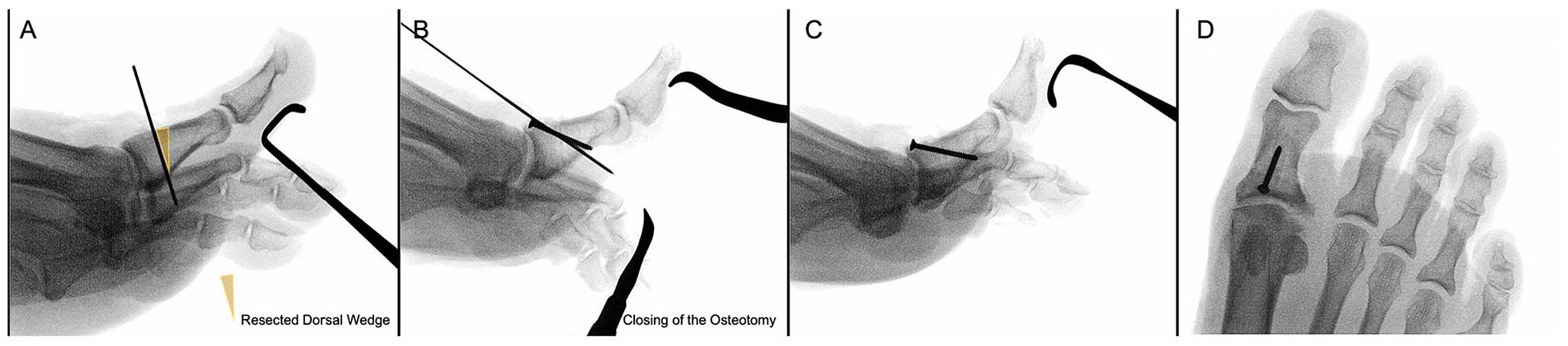
Intraoperative fluoroscopic images of Moberg osteotomy. (A) A guidewire was placed at the site of the provisional osteotomy. (B) Following osteotomy along the inserted guidewire, another Kirschner wire was inserted for temporary fixation, and a 2.0 screw was inserted. Lateral (C) and anteroposterior (D) views of the proximal phalanx following Moberg osteotomy.
Clinical Data
Preoperative clinical notes were reviewed for all included patients, and preoperative ranges of motion were noted. As surgeons differed in their notation and clinical examination styles, not all patients had preoperative range of motion data (28 in the C cohort, 25 in CM). Operative notes were reviewed to verify that each patient was classified to the correct cohort based on their procedures. Postoperative clinical notes were reviewed to identify all subsequent ipsilateral first-ray surgeries, infections, progression of arthritis, persistent pain, and other complications until the conclusion of the study.
Radiographic Data
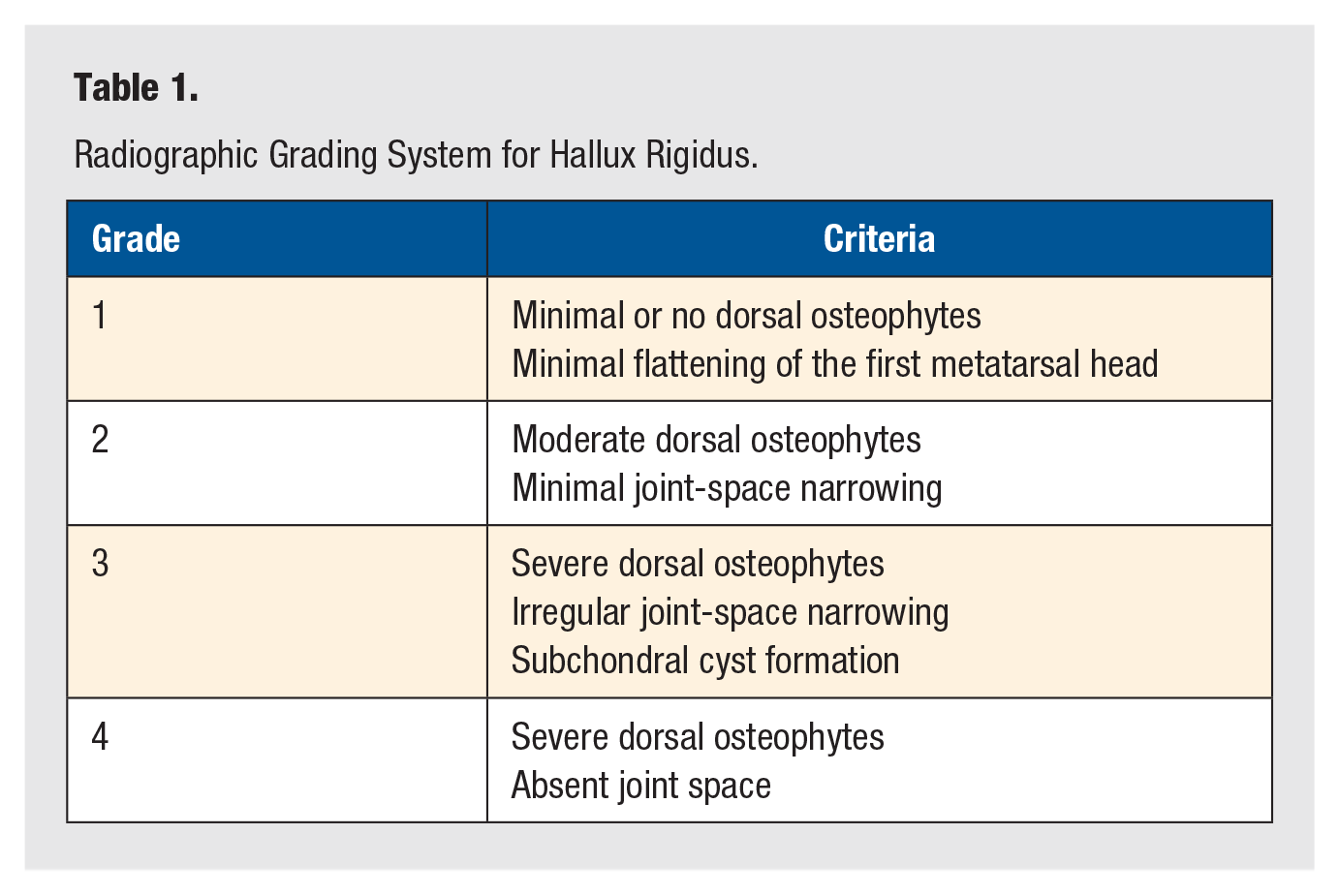
A fellowship-trained foot and ankle orthopaedic surgeon reviewed preoperative AP and lateral foot radiographs using the Sectra IDS-7 PACS system (Sectra, Linköping, Sweden) to determine the severity of each patient’s hallux rigidus using the method of Coughlin and Shurnas (Table 1).10,17
Radiographic Grading System for Hallux Rigidus.
Patient-Reported Outcome Measures
Patient-Reported Outcomes Measurement Information System (PROMIS) scores were collected preoperatively and at 1 and 2 years postoperatively. PROMIS is a patient-administered questionnaire assessing various dimensions of patient outcomes. PROMIS physical function, pain interference, pain intensity, global physical health, global mental health, and depression scores were evaluated. PROMIS has been specifically validated for several foot and ankle conditions and has been shown to perform as well or better than the Foot and Ankle Outcome Score (FAOS), a reliable and well-performing patient-reported outcome survey, in all aspects of psychometric validity.18,19 For each PROMIS domain, a higher score indicated a greater degree of the dimension measured; therefore, higher scores in the physical function domain indicate better physical function, whereas higher scores in the pain interference, pain intensity, and depression domains indicate worse outcomes with more pain and depression.
Statistical Analysis
Descriptive statistics were reported as means and standard deviations for continuous variables and counts and percentages for categorical variables. Normality was tested using Shapiro-Wilk tests, and all continuous values were distributed normally. An a priori power analysis found that 24 patients were needed for each cohort to achieve 80% power, given a minimum detectable difference of 5.8 points on the PROMIS physical function scale and a standard deviation of 8 points. These values were taken from previous literature on minimal clinically important differences for PROMIS scores in foot and ankle patients. 20 Paired t tests were used to test changes between scores taken preoperatively and at both 1 and 2 years postoperatively, as well as between 1 and 2 years postoperatively. Differences between groups were tested using independent samples t tests for continuous variables and Pearson’s chi-square or Fisher’s exact test for categorical variables. Group differences in 1-year PROMIS scores were analyzed with multivariable linear regression, adjusting for preoperative score, age, sex, body mass index, radiographic hallux rigidus grade, and by cohort. Statistical significance was established at alpha 0.05. The analysis was conducted on R: A Language and Environment for Statistical Computing (R Core Team 2021, Vienna, Austria).
Results
Demographics and Preoperative Hallux Rigidus Severity
Demographic results are given in Table 2. There were 62 isolated cheilectomy patients and 67 cheilectomy-Moberg patients identified. Among the cheilectomy patients, 43 had 1-year PROMIS scores (69%) and 36 had 2-year PROMIS scores (59%). In the CM group, 62 patients had 1-year PROMIS scores (93%) and 40 had 2-year scores (60%). There were no significant differences in age, BMI, or sex distribution between the 2 cohorts. Additionally, there were no significant differences in the distribution of preoperative hallux rigidus grades or preoperative range of motion.
Demographic and Preoperative Cohort Comparison.
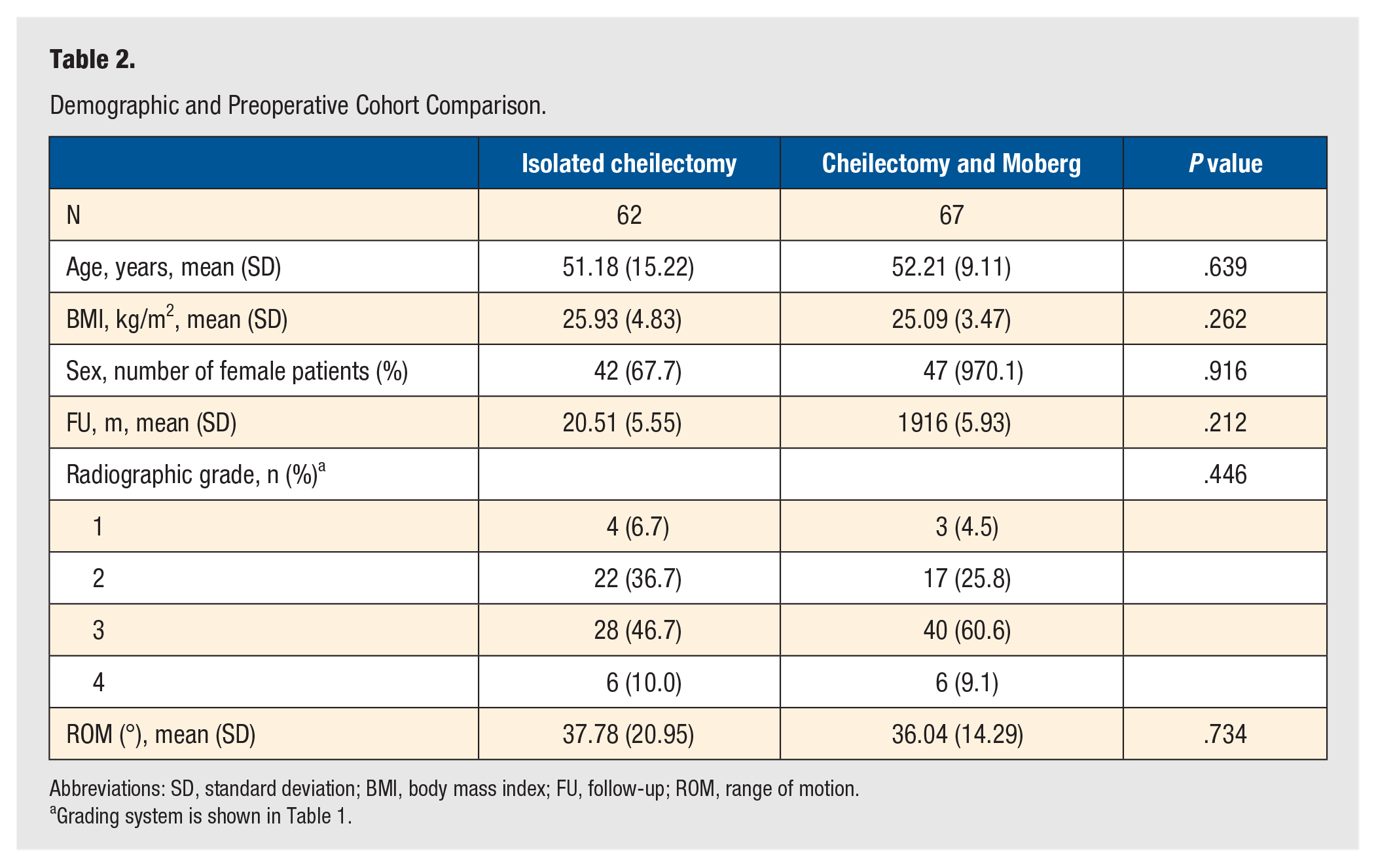
Abbreviations: SD, standard deviation; BMI, body mass index; FU, follow-up; ROM, range of motion.
Grading system is shown in Table 1.
Patient-Reported Outcomes
Preoperative, 1- and 2-year postoperative, and changes in PROMIS score data are shown in Table 3 and Figures 3 and 4. Both groups demonstrated statistically significant improvements in physical function, pain interference, pain intensity, and global physical health scores from the preoperative to 1-year timepoint and the preoperative to 2-year timepoint, but not from 1 year to 2 years postoperatively (P < .001 for baseline to 1-year changes and baseline to 2-year changes for all 4 domains in both cohorts). There were no statistically significant changes in PROMIS global mental health or depression domains. There were no statistically significant differences in physical function, global physical health, global mental health, or depression scores between the C and CM cohorts at any of the timepoints evaluated, nor were there statistically significant differences between cohorts in the changes in these scores. However, the CM cohort demonstrated significantly worse pain interference scores than the C group both preoperatively (58.11 vs 52.43, P < .001) and at 1 year postoperatively (50.02 vs 45.12, P = .01). Conversely, the C cohort demonstrated significantly worse pain intensity scores both preoperatively (55.57 vs 49.64, P < .001) and at 1-year postoperatively (45.87 vs 39.85, P < .001). There were no significant differences between the 2 cohorts for either pain interference or pain intensity at 2 years, and there were no significant differences in the changes in either cohort for these domains.
Comparison of Preoperative, 1-Year, and 2-Year Postoperative PROMIS Score Changes Between the 2 Groups.
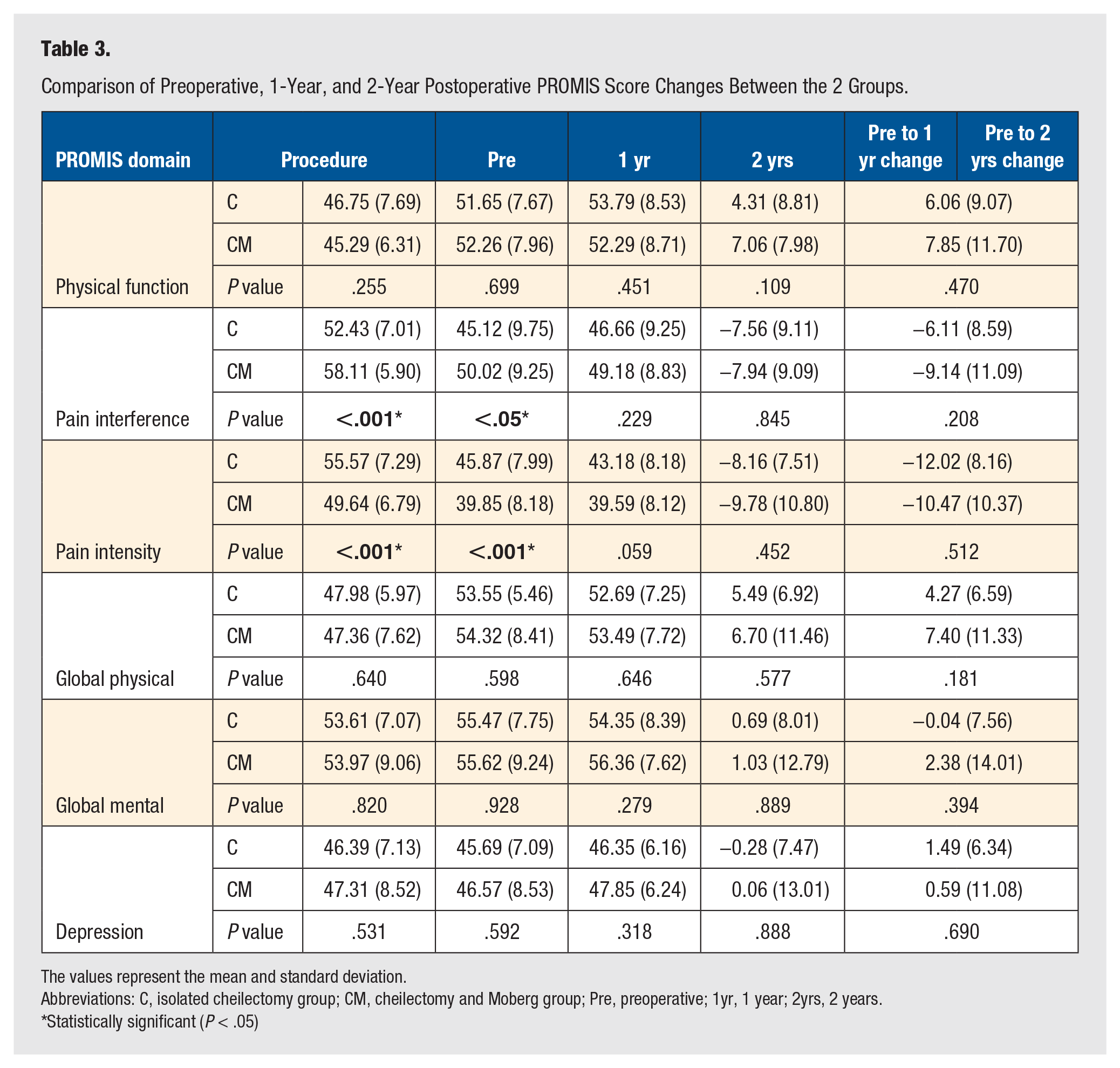
The values represent the mean and standard deviation.
Abbreviations: C, isolated cheilectomy group; CM, cheilectomy and Moberg group; Pre, preoperative; 1yr, 1 year; 2yrs, 2 years.
Statistically significant (P < .05)
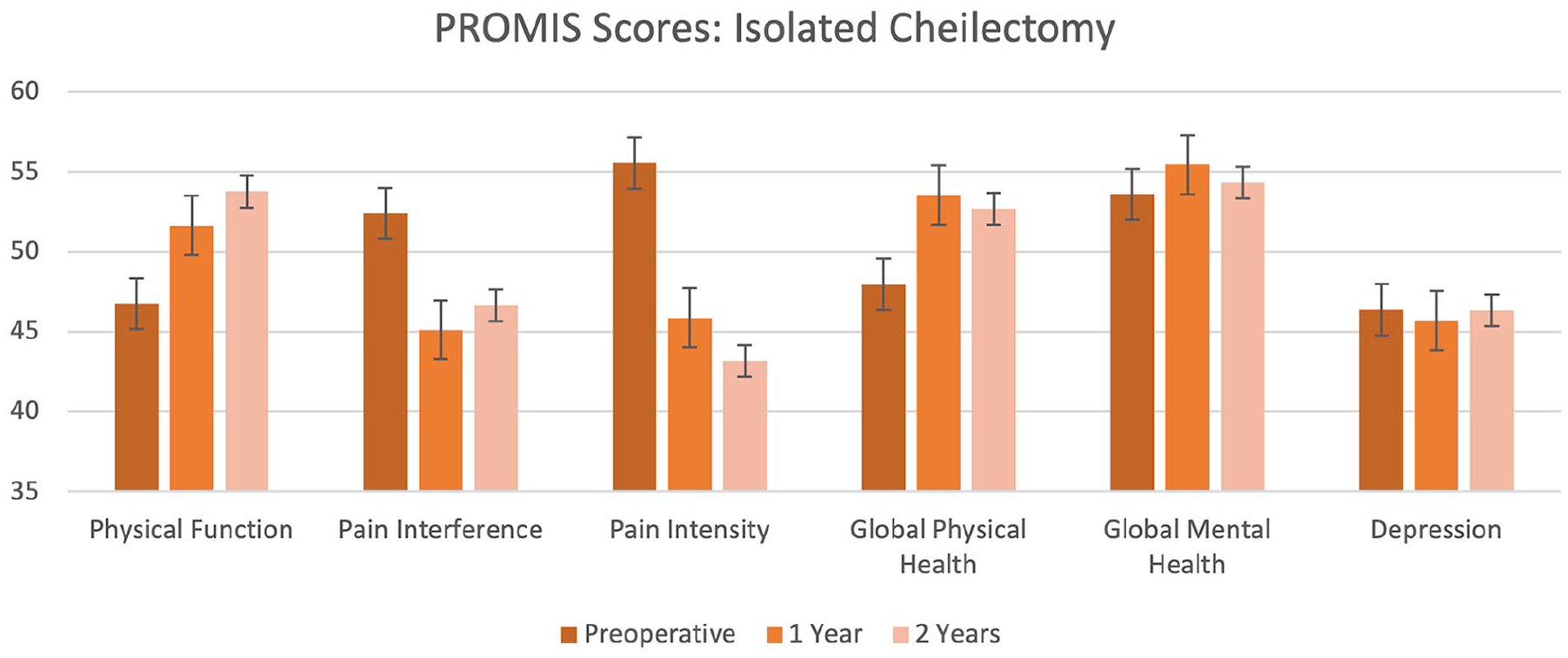
Isolated cheilectomy patients reported statistically significant improvements in the PROMIS domains of physical function, pain interference, pain intensity, and global physical health.
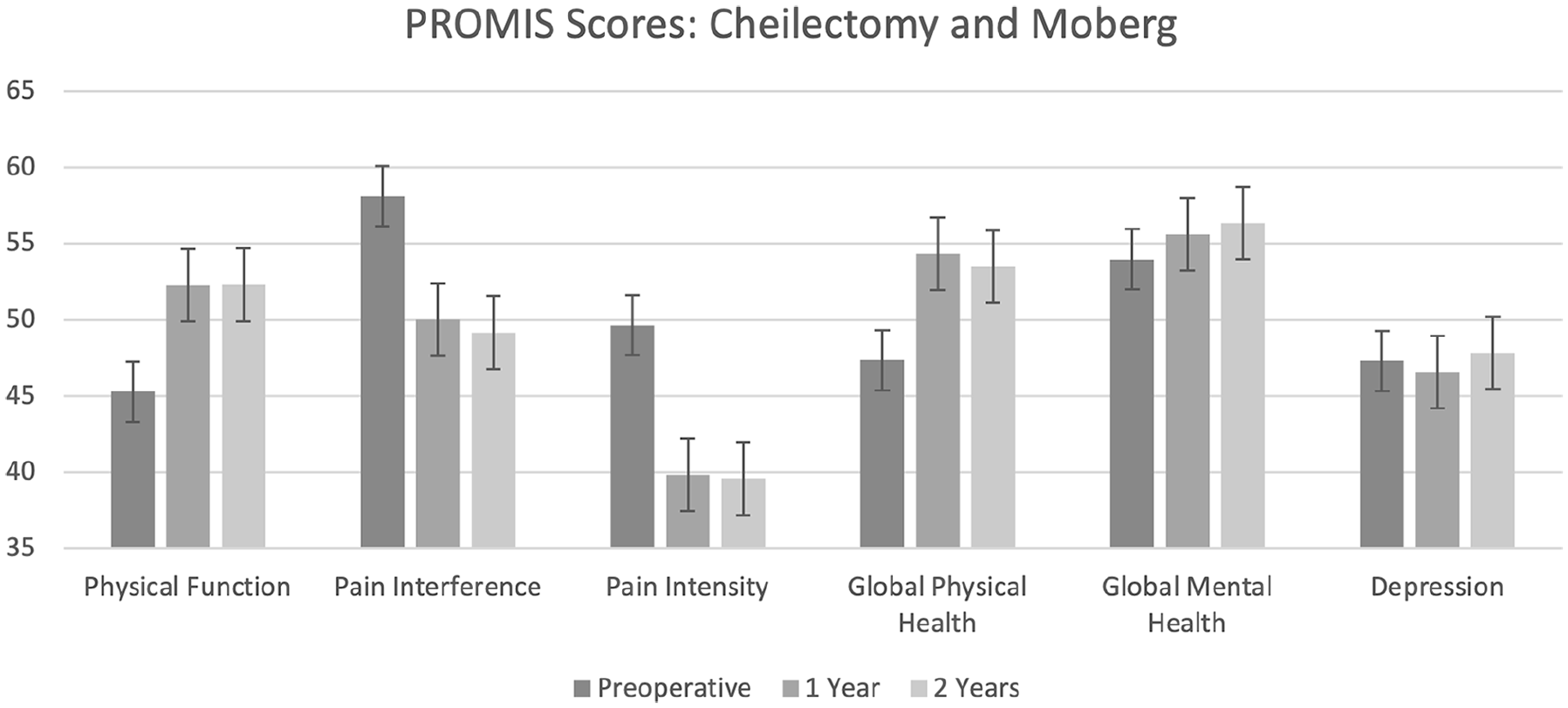
Cheilectomy and Moberg osteotomy patients reported statistically significant improvements in the PROMIS domains of physical function, pain interference, pain intensity, and global physical health.
When adjusted for preoperative score, age, sex, body mass index, radiographic hallux rigidus grade, and by cohort, multivariate regression revealed that the C cohort had worse 1-year postoperative pain intensity scores than the CM group (44.85 vs 39.93, P < .05, Table 4), but there was no difference in 1-year postoperative pain interference scores across groups (44.56 vs 44.75, P = .381).
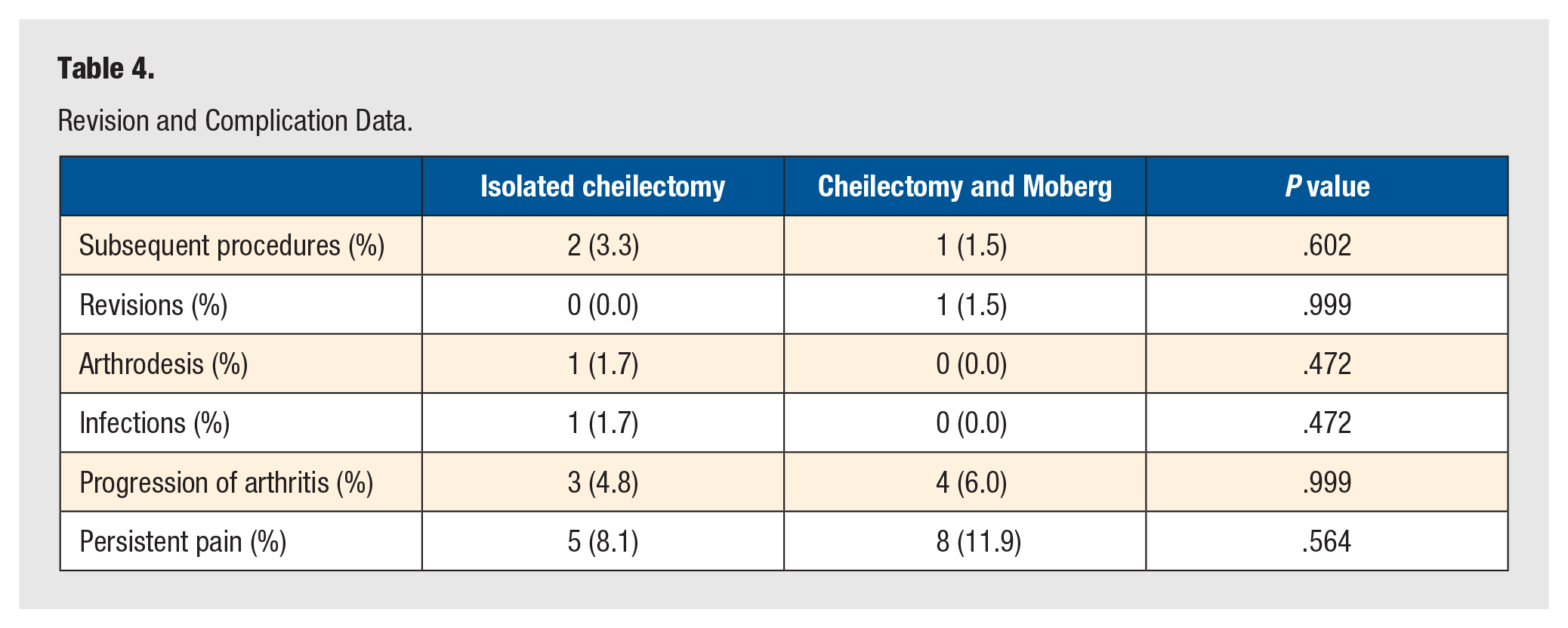
Revision and Complication Data.
Complications and Subsequent Surgeries
Complication and revision data are presented in Table 5. There were no significant differences in the incidence of revisions, postoperative conversions to first MTP arthrodesis, or overall subsequent procedures on the ipsilateral first ray. Moreover, there were no significant differences in infection, progression of arthritis, or persistent pain between the 2 groups.
Adjusted 1-year PROMIS Scores, Adjusted by Preoperative PROMIS Score, Age, Sex, Body Mass Index, and Radiographic Hallux Rigidus Grade.
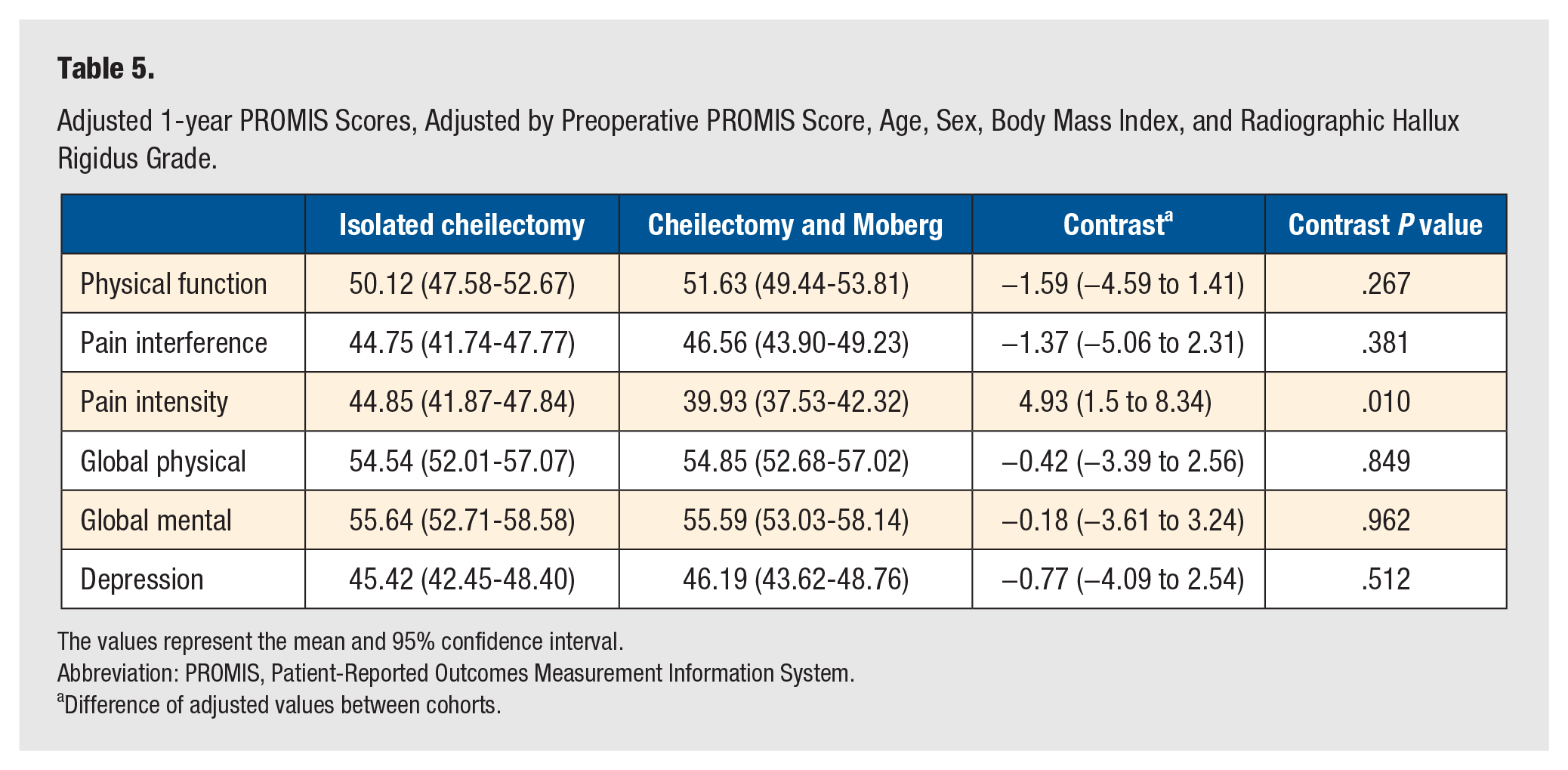
The values represent the mean and 95% confidence interval.
Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
Difference of adjusted values between cohorts.
Discussion
This study represents the largest comparison of outcomes to date between the 2 major forms of joint-preserving hallux rigidus surgery, as well as the only investigation on this topic using a validated patient-reported outcome measure. Although our results do not clearly favor the use of either isolated cheilectomy or cheilectomy with a dorsal opening closing wedge osteotomy, the additional precision and insights conferred by the PROMIS data reported here contribute to a greater understanding of hallux rigidus treatment and pose important questions for future research. Specifically, the additional sample size and more precise PROMIS metrics here add a greater degree of confidence in the short-term similarity of outcomes between the 2 treatment methods.14,15
In general, outcomes between the cheilectomy cohort and the cheilectomy and Moberg osteotomy cohort were similar (Figures 5 and 6). Contrary to our hypotheses, which predicted that patients who underwent just cheilectomy would experience significantly worse clinical outcomes and more returns to the operating room, there were few differences between the cohorts in either category. Isolated cheilectomy patients reported greater pain intensity preoperatively and at 1 year, while cheilectomy and Moberg patients reported greater pain interference at these same timepoints. Additionally, although the magnitude of the differences between groups did not reach the level of statistical significance, patients who underwent cheilectomy with Moberg osteotomy tended to achieve a clinically significant improvement from their preoperative state at 1 year, whereas patients who just underwent cheilectomy did not. Specifically, the degree of physical function score improvement in the CM cohort (7.06) exceeded the cited MCID at 1 year (5.8), while the C group failed to clear this threshold (4.31). 20 Both the CM group (+7.85) and the C group (+6.06) exceeded this value at 2 years. Although the cited threshold of 5.8 points is rather subjective due to substantial variations in methods for calculating a minimal clinically important difference, this finding suggests that cheilectomy patients may find greater early relief when surgeons also incorporate Moberg osteotomy. 21 An adjusted 1-year PROMIS comparison indicating that the CM cohort had better pain intensity scores by 5 points further supports this notion; nonetheless, we cannot favor one technique over the other based on this single-scale difference out of 6.

Preoperative (A) and postoperative (B) weightbearing foot radiographs of a patient with isolated cheilectomy for hallux rigidus.
Preoperative (A) and postoperative (B) weightbearing foot radiographs of a patient with cheilectomy and Moberg osteotomy for hallux rigidus.
Our findings help to clarify the basic findings of previous studies. Waizy et al 15 followed up 60 cheilectomy patients, 27 of whom underwent a concomitant Moberg osteotomy, and compared 1- and 2-year outcomes between the 2 groups. For the 46 patients who reached 2-year follow-up, the authors reported outcomes with short surveys assessing pain (classified into none, occasional, daily, and continual) and satisfaction (not satisfied, satisfied, completely satisfied). Additionally, surgeon-reported Kitaoka scores and radiographic classifications were performed. They found generally good outcomes overall, with 54% of patients having no or only occasional pain. As in the current study, they found statistically equivalent outcomes between the 2 groups but slightly better outcomes in their cheilectomy and Moberg cohort that did not reach the level of statistical significance. However, their lack of a standardized, validated assessment of functionality or pain prevents both an unequivocal comparison between cohorts as well as an ability to situate patients’ outcomes within a wider context of pain or disability.
Similarly, Warganich et al 14 compared cheilectomy patients with (32) and without Moberg (31) at a minimum of 1-year follow-up and found slightly more favorable outcomes in the cheilectomy and Moberg group that did not reach the level of statistical significance. The authors used surveys to gather data on time to full weightbearing, time to a subjective “100% recovery,” as well as satisfaction and pain as graded on a 1 to 10 scale. Patients in both groups reported satisfaction and decreases in pain. Again, cheilectomy and Moberg patients experienced greater pain reductions (8.1 preoperatively to 2.3 postoperatively) than cheilectomy patients alone (7.5 preoperatively to 2.0 postoperatively), although these differences did not reach significance. The larger sample size of our study provides greater statistical power, and thus greater certainty, for similar outcomes which both prior comparison studies found.
Our findings have direct implications, both for clinical care and for future research. The overall good results found for both procedures, as well as the general similarity between outcomes between them, suggest that external considerations may be of greater importance than short-term clinical outcomes when deciding on the appropriate course of treatment for a given patient. For example, patient-specific concerns like recovery time, comfort level with a more invasive osteotomy, and overall goals with surgery might need to be discussed and considered in the course of care. 14 Our data, however, contradict the notion that addition of a Moberg osteotomy increases the likelihood of postoperative complications and suggest that it is a great treatment option for early-to-moderate hallux rigidus, particularly if the surgeon determines a need for greater dorsiflexion.
Future research will be necessary to further explore outcome differences between the 2 procedures. Most notably, although our sample size is more than double the size of the 2 previous studies comparing isolated cheilectomy with cheilectomy and Moberg, our results imply that perhaps greater sample sizes are still needed. Although MCID values for PROMIS scores have been demonstrated to vary considerably depending on the methods used to calculate them, smaller, more sensitive MCID estimates exist, for which our study would be underpowered. 21 Multicenter studies will likely be necessary to amass enough patients to detect the smallest differences between groups with statistical certitude. Additionally, data are lacking on long-term outcomes between groups. Studies with 5- to 10-year follow-ups would be helpful to offer a more holistic comparison of the relative merit of the 2 approaches, particularly given the palliative, rather than curative, nature of cheilectomy alone.10,22
Finally, this study is not without limitations. First, it is a retrospective comparison study, and although patients did not significantly differ in any demographic or clinical respects between the 2 cohorts, it nevertheless lacks the experimental rigor of a prospective randomized control trial. Second, the incomplete follow-up, especially in the cheilectomy-only group, leaves a possibility of response bias, wherein the typical outcomes for the subset of patients who responded to the study may be different from the typical outcomes for the cheilectomy-only group as a whole. Third, this study comprised patients from multiple surgeons; hence, the selection of patients who will be candidates for which procedure and the amount of resection during cheilectomy may have varied, necessitating future prospective research using a well-designed methodology. Lastly, other possible factors that can affect the development of hallux rigidus or the surgical outcome, such as radiographic arch parameters, foot shape (hallux valgus), or instability or hypermobility at the first ray,23,24 were not included in the analysis, limiting the generalizability of our study’s results.
Conclusions
In conclusion, this study compares short- to medium-term patient-reported clinical outcomes and complications of isolated cheilectomy against cheilectomy and Moberg osteotomy for hallux rigidus. The addition of Moberg osteotomy did not increase the incidence of postoperative complications nor appreciably lower the reoperation rate when compared to isolated cheilectomy, while producing better scores on one of the PROMIS pain scales at 1 year of follow-up. This study and previous works suggest that any potential differences in outcomes between groups are not large enough to be clinically meaningful in the short term and that other, patient-specific factors may be more relevant in determining the best course of treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SJE discloses consulting fees from Wright Medical, Vilex, and Paragon 28, as well as paid presentations for Stryker and Paragon 28. JTD discloses IP royalties from Zimmer and Arthrex, as well as stock in Wright Medical. The other authors declare no potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This was a single-center retrospective study, with a protocol approved by the Foot and Ankle Registry Steering Committee at the investigators’ institution (IRB #2013-038).
Informed Consent
Researchers were approved by a Steering Committee for an IRB-approved registry to retrospectively view patient-reported outcomes measurement data collected from all patients under the registry IRB.
Trial Registration
Not applicable, because this article does not contain any clinical trials.