
Abstract
Background:
While first metatarsophalangeal joint (MTPJ) arthrodesis is a common and effective procedure, there is a paucity of studies examining obesity’s effect on outcomes of 1st MTPJ arthrodesis. This study’s purpose was to evaluate patient-reported outcomes following 1st MTPJ arthrodesis in obese versus non-obese patients.
Methods:
A retrospective cohort study of 94 patients undergoing first MTPJ fusion over the age of 18 with a diagnosis of hallux valgus or hallux rigidus was performed. Surgical and postoperative outcomes were examined preoperatively and at 6 and 12 months follow-up via Visual Analog Pain scale (VAS), and Short Form 36 (SF-36) surveys, and data were stratified into 2 patient groups: BMI < 30 (n = 62, mean age 63.9 ± 9.1 and ≥ 30 (n = 32, mean age 61.9 ± 8.4).
Results:
Average overall VAS and SF-36 physical component scores improved significantly at 6 months (P < .001, .006) and 1 year postoperative visits (P < .001, .007) with no differences in survey scores, outcomes, or complications between weight groups.
Conclusion:
Our study showed first MTPJ fusion improves short-term pain and physical quality-of-life in arthritic obese and non-obese patients without differences in nonunion, complications, or patient-reported measures.
Level of Evidence:
Level III, Prognostic, Case-Control Study
Introduction
First metatarso-phalangeal joint (MTPJ) arthrodesis is a commonly performed procedure for patients with various disorders of the first ray including hallux rigidus, severe hallux valgus, failed 1st MTPJ replacement, and failed hallux valgus correction. 1 Outcomes are generally favorable with reported fusion rates greater than 90% with commensurate improvements in patient-reported outcomes including function, satisfaction, and pain2-5 Patients can return to being active and participate in sports such as golf and tennis with no functional consequence. 6
“First MTP fusion reliably produces short-term improvements in pain and physical quality-of-life in patients with advanced arthritis without a difference in nonunion, complications, or patientreported pain and quality-of-life measures in both obese and non-obese patients.”
The importance of various surgical factors on patient outcomes of first MTP joint arthrodesis has been previously studied, 1 and while certain patient-related factors have generally been associated with worse outcomes in elective foot and ankle surgery,3,7 -11 there is limited data on how these specifically correspond to patients undergoing 1st MTPJ arthrodesis. Factors such as pre-existing disease, higher grades of osteoarthritis, and increased dorsiflexion of the hallux postoperatively have been identified as having a negative influence on union rates following 1st MTPJ arthrodesis12 -15 while age, sex, smoking, hallux valgus angle (HVA), and American Society of Anesthesiologists (ASA) status have not been found to affect nonunion rates. 16
From 2000 to 2018 the American obesity rate (body mass index [BMI] ≥ 30) increased from 30% to approximately 42%, 17 and current estimates anticipate a greater than 50% obesity rate by 2030. 18 Obesity in particular has been broadly studied among the foot and ankle literature, 19 and has been associated with increased complications20 -23 and worse outcomes in fracture surgery,23,24 total ankle arthroplasty,25,26 hallux valgus surgery, 27 and surgical repair of Achilles ruptures. 22 However, there is some controversy as other studies have shown no difference in outcomes for obese patients undergoing forefoot surgery, 28 adult acquired flat foot deformity reconstruction, 29 and total ankle arthroplasty. 24 Despite the data suggesting that obesity as a risk factor for outcomes in the foot and ankle literature, there is a paucity of data regarding outcomes of 1st MTP joint arthrodesis among obese patients.30 -32
Given the magnitude of this epidemic and the rise of the aging population, it is important to understand how obesity affects outcomes following 1st MTPJ arthrodesis. The purpose of this study is to evaluate both clinical and patient-reported outcomes following 1st MTP joint arthrodesis in obese patients and compare these results with non-obese patients.
Methods
Study Design
A review of outcomes data of patients undergoing first MTP fusion by a single foot and ankle fellowship trained orthopaedic surgeon from August 1, 2015 to July 1, 2018 was conducted following institutional review board approval.
Participants
Those over 18 years of age with a preoperative diagnosis of hallux valgus or hallux rigidus with radiographic evidence of disease and failure of conservative management were included in the study. The International Classification of Diseases 10th Revision (ICD-10) codes included were M20.21, M20.11, M20.22, and M20.12. After meeting study inclusion criteria, patients were consented via written agreement for participation at the time of their preoperative clinic visit. Exclusion criteria were age under 18, prisoners, other at risk populations, and patients with active cancer diagnoses. Subsequently, general demographic, surgical, and postoperative outcomes data were collected via a review of the electronic medical record.
Surgical Technique
A single surgeon performed all first MTP arthrodeses and associated procedures with a similar technique for all cases. A dorsal incision was made along the first MTP joint. The arthritic metatarsal head and phalanx are debrided using rongeurs, curettes, and osteotomes until sufficient subchondral bone was visualized. The surgeon’s preference was to not use reamers due to ease of access to the joint, and a 2.0-mm drill bit was used to perforate multiple holes in both the metatarsal head and phalanx to stimulate bleeding. The toe was then pinned in the corrected position. An MTP fusion plate (Stryker Anchorage without CP technology) was secured over the joint with 3.5-mm non-locking screw fixation and 1 compression screw through the plate across the fusion site. A 4.0-mm partially cannulated compression screw was placed across the joint as well to assist with stability and compression of the arthrodesis. All patients were instructed to begin weightbearing through the heel postoperatively in a postoperative shoe or boot, and all patients included in the study were placed on aspirin 81 mg twice daily for 4 weeks postoperatively for deep vein thrombosis prophylaxis (DVT) prophylaxis. Sutures were removed at 2 to 3 weeks, and patients were instructed to bear weight as tolerated.
Outcomes Evaluation
Visual analog pain scale (VAS) and Short Form 36 (SF-36) patient-reported outcome surveys were administered and collected, prospectively, at preoperative, 6-month and 12-month postoperative clinic visits. At each visit, the surgeon assessed the patients for post-operative complications, including wound infections requiring antibiotics, wound infections requiring incision and drainage, deep vein thrombosis, recurrence of the deformity, and revision surgery. At final post op visit, radiographs were taken to confirm correction and surgical success.
These self-assessment tools were provided to the patients by clinical staff and reviewed by the attending physician and included in his note. This data was then retrospectively reviewed for this study. VAS is an extensively validated survey introduced in 1921 that is still commonly used in orthopedics used to evaluate subjective pain perception among subjects. 33 It consists of a 10 cm scale on which patients can rate their current pain level and can also be used to track pain over time or between groups of patients. 33 SF-36 is one of the most widely used surveys around the world measuring health-related quality of life outcomes and provides 2 uncorrelated summary scores, the Physical Component Summary (PCS) and Mental Component Summary (MCS) scores. 34
Data Evaluation
Following data compilation, patients were stratified into 2 groups based on a body mass index (BMI) less than 30, and 30 or above, based on the WHO Obesity threshold. 35 No patients in the present study met criteria for WHO Obesity class III (above 40). After stratification, a total of 94 patients were included in the final analysis, 62 with a BMI less than 30 and 32 with a BMI of 30 or more (26 met Obesity class I, 6 met Obesity class II) (Table 1).
Baseline Characteristics.
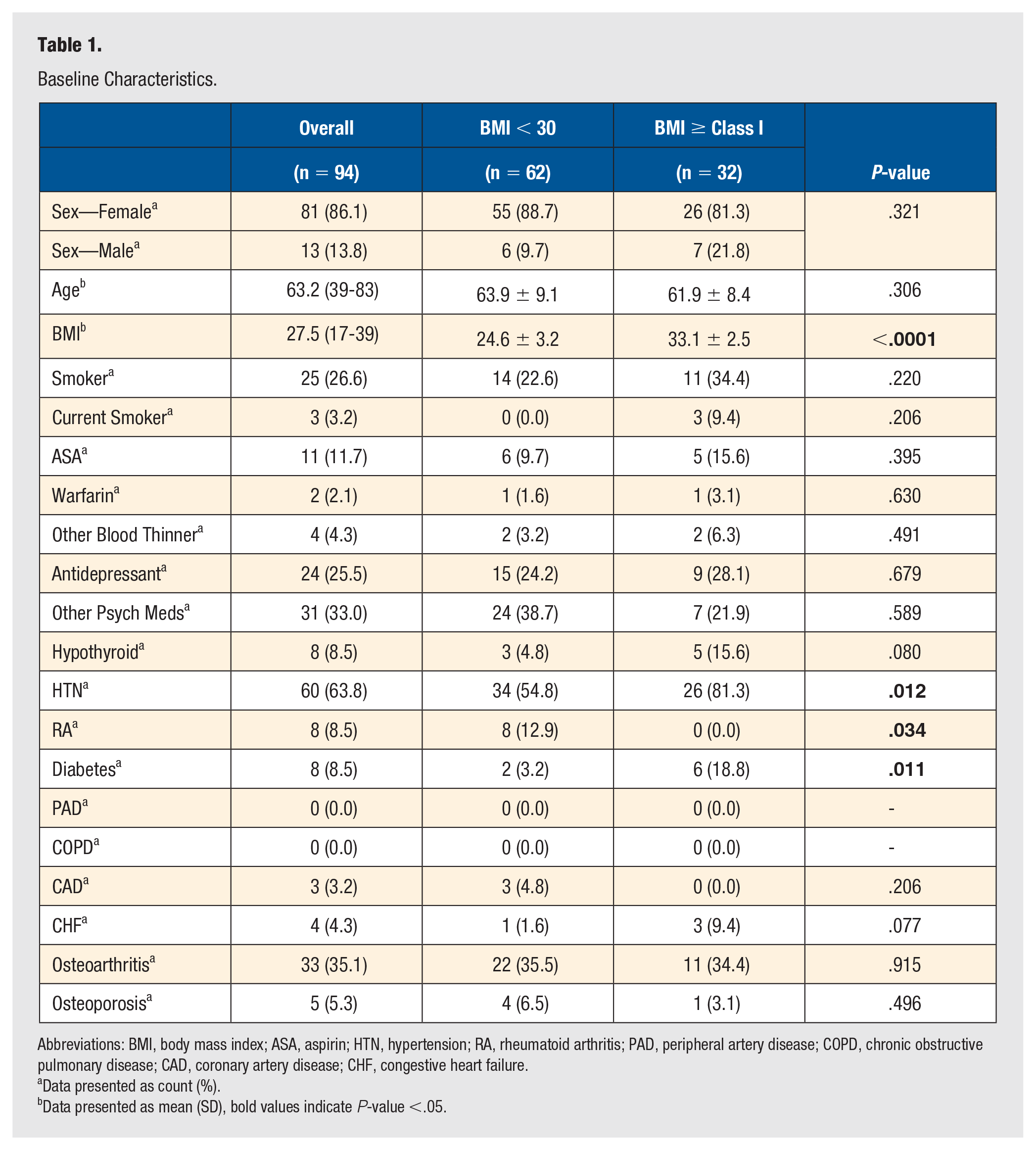
Abbreviations: BMI, body mass index; ASA, aspirin; HTN, hypertension; RA, rheumatoid arthritis; PAD, peripheral artery disease; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; CHF, congestive heart failure.
Data presented as count (%).
Data presented as mean (SD), bold values indicate P-value <.05.
Statistical Analysis
Patient demographic data were analyzed with general descriptive statistics. Fisher’s exact and chi-squared tests were used to assess categorical data, including operative procedures and postoperative complications. All continuous data were tested for normality. Mean VAS and SF-36 component scores were compared between BMI cohorts using independent sample t-test for parametric data, while a Mann-Whitney U test was used for comparison of nonparametric data. For all statistical tests, assumptions of α < .05 and β = .8 were made. All other analyses were conducted with SPSS software version 27.0 (IBM Corporation, Armonk, NY).
Funding
This study did not receive any source of external funding.
Results
General Demographics and Operative Procedures
The mean age of all patients included in the study was 63.2 (range: 39-83) years, and no significant difference in age was observed between BMI cohorts (P = .31) (Table 1). Patients in the BMI ≥ 30 cohort had significantly greater mean BMI (P < .001), and increased prevalence of hypertension (HTN) and diabetes (DM) (P = .01, P = .01, respectively) relative to the BMI < 30 cohort. Additionally, those with BMI < 30 had a significantly greater prevalence of rheumatoid arthritis (RA) (P = .03). No other differences in rates of medical comorbidities were observed between groups. Similarly, no differences in tourniquet time (P = .82) nor operative time (P = .07) were observed between cohorts (Table 2). A significantly greater proportion of patients with BMI < 30 had a calcaneal bone graft (P = .02), but no other differences in operative procedures were noted (Table 2).
Procedural Characteristics.
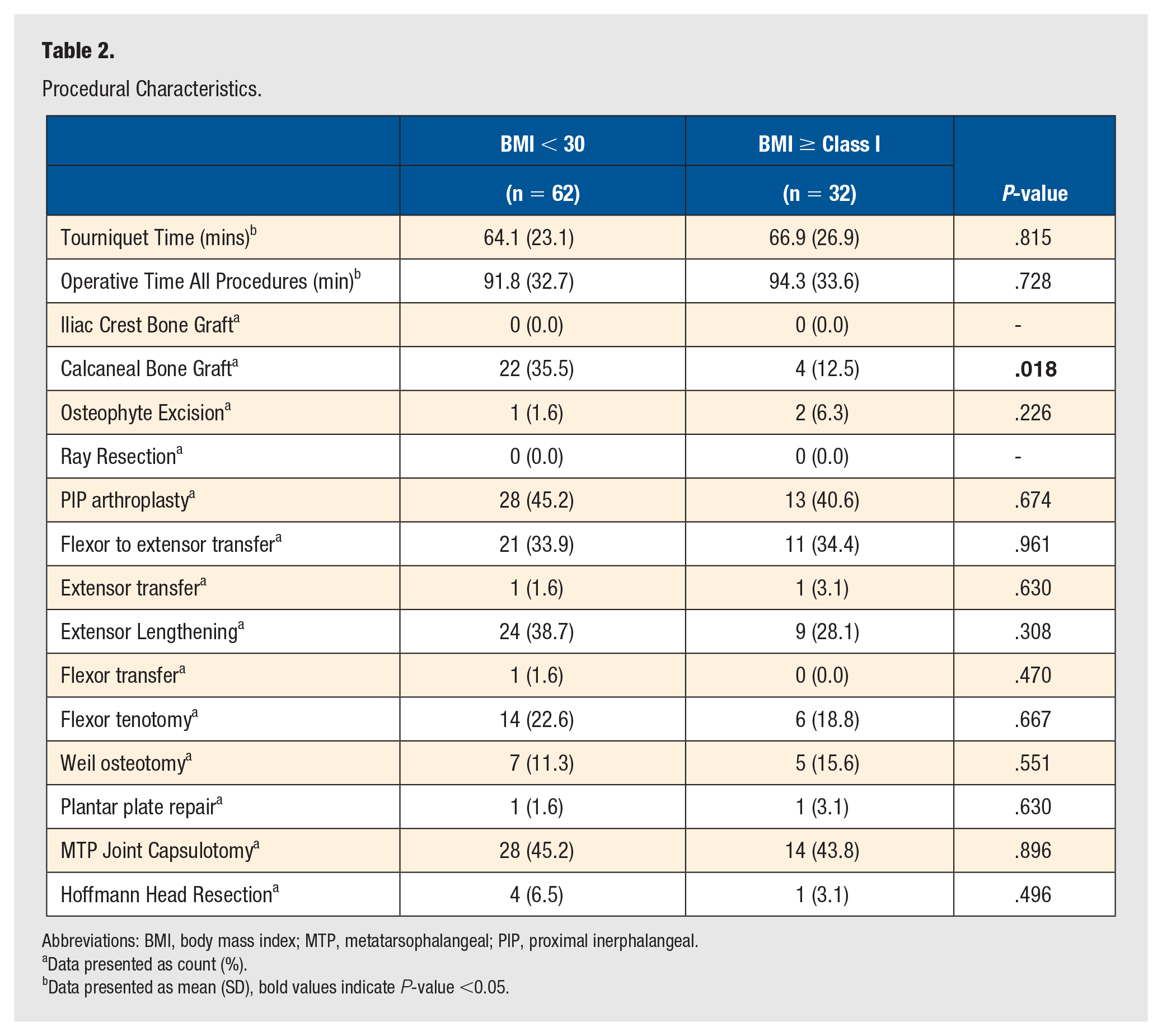
Abbreviations: BMI, body mass index; MTP, metatarsophalangeal; PIP, proximal inerphalangeal.
Data presented as count (%).
Data presented as mean (SD), bold values indicate P-value <0.05.
MTPJ Fusion Outcomes & Complications
Average grouped VAS and SF-36 physical component (PCS) scores for the entire cohort of patients improved significantly from preoperative to 1-year postoperative (P < .001, .007) (Table 4). A significant decrease in grouped VAS pain score and significant increase in grouped SF-36 PCS score were also observed at the 6-month postoperative visit (P < .001, .006). No differences in grouped SF-36 MCS scores were noted at the 6-month or 1-year postoperative visits. Cohort comparison examining any differences between BMI<30 group versus the BMI Class I or greater (>30) revealed no statistical differences in mean VAS (P = .36, .69) or change in VAS (P = .68, .60) at 6 months or 1 year respectively. Similarly, no statistical differences in mean SF-36 PCS (P = .44, .78), mean SF-36 MCS (P = .54, .56), change in SF-36 PCS (P = .27, .48), or change in SF-36 MCS (P = .56, .96) were detected between groups at 6 months or 1 year. Rates of wound washout (P = .21), recurrence of hallux rigidus or valgus treated nonoperatively (P = .47), revision surgery for reason other than infection (P = .52), and overall nonunion rates (P = .79) were not statistically different between cohorts, nor was the time to full weight bearing (P = .10) (Table 3).
Surgical Outcomes.
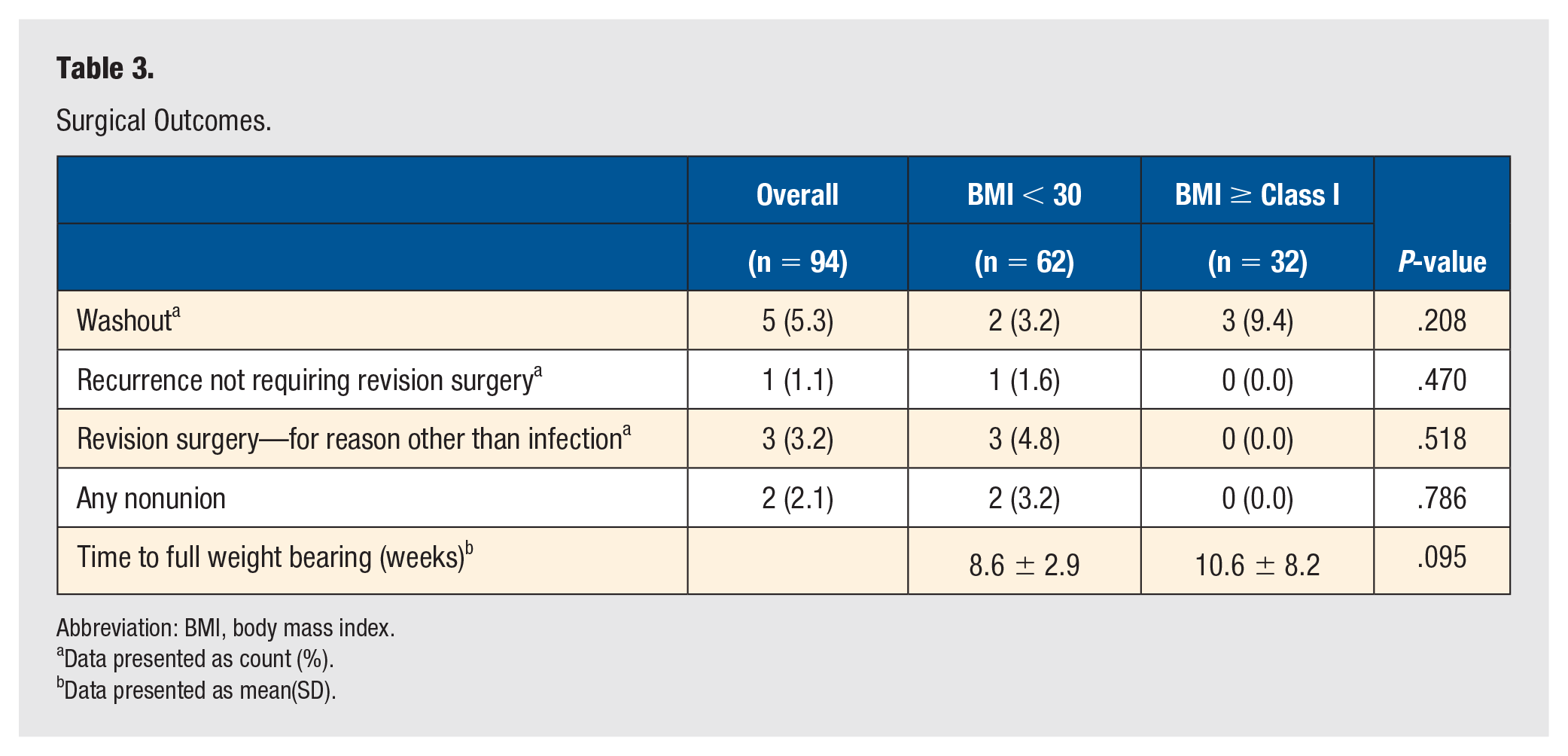
Abbreviation: BMI, body mass index.
Data presented as count (%).
Data presented as mean(SD).
Discussion
The main findings of this study were that improvements in pain and physical quality of life at 6- and 12-month postoperative visits were observed in all patients without any significant differences detected between obese and non-obese patients undergoing 1st MTP joint arthrodesis. Similarly, there were no differences in surgical outcomes or complication rates between those 2 groups.
First MTP fusion reliably produces satisfactory patient outcomes including improved function and decreased pain,2,4,5,36 and remains the gold standard in the treatment of advanced first MTP arthritis. 37 A 2021 systematic review of 570 patients undergoing first MTP arthrodesis conducted by França et al 38 showed greater than 90% patient satisfaction rate with revision rates ranging from 0% to 20.5%. In a 2019 review by Da Cunha et al 6 of a prospective registry of young patients undergoing first MTP fusion focusing on return to sport, 96% of patients (48/50) reported being satisfied with their return to sport and physical activities at a mean of 5.1 years postoperatively. These patients demonstrated improvements across all Foot and Ankle Outcome Score (FAOS) subscores. 6 Similarly, DeSandis et al 36 reported excellent outcomes in a series of 53 patients (56 feet) undergoing first MTP fusion with improvements in all subscores using both the FAOS and SF-36/12 surveys with a 14.3% (8/56) complication rate (symptomatic hardware, 2nd metatarsal stress fracture, persistent pain, and pressure). Overall results from the present study demonstrate outcomes in line with these standards, with significant improvements in pain and SF-36 PCS (Table 4) and a 6.4% revision rate. A notable difference includes our lack of significant improvement in our cohort’s MCS score which is likely due to a relatively high preoperative MCS baseline (78.2, Table 4).
Patient-Reported Outcomes BMI Class I or Greater.
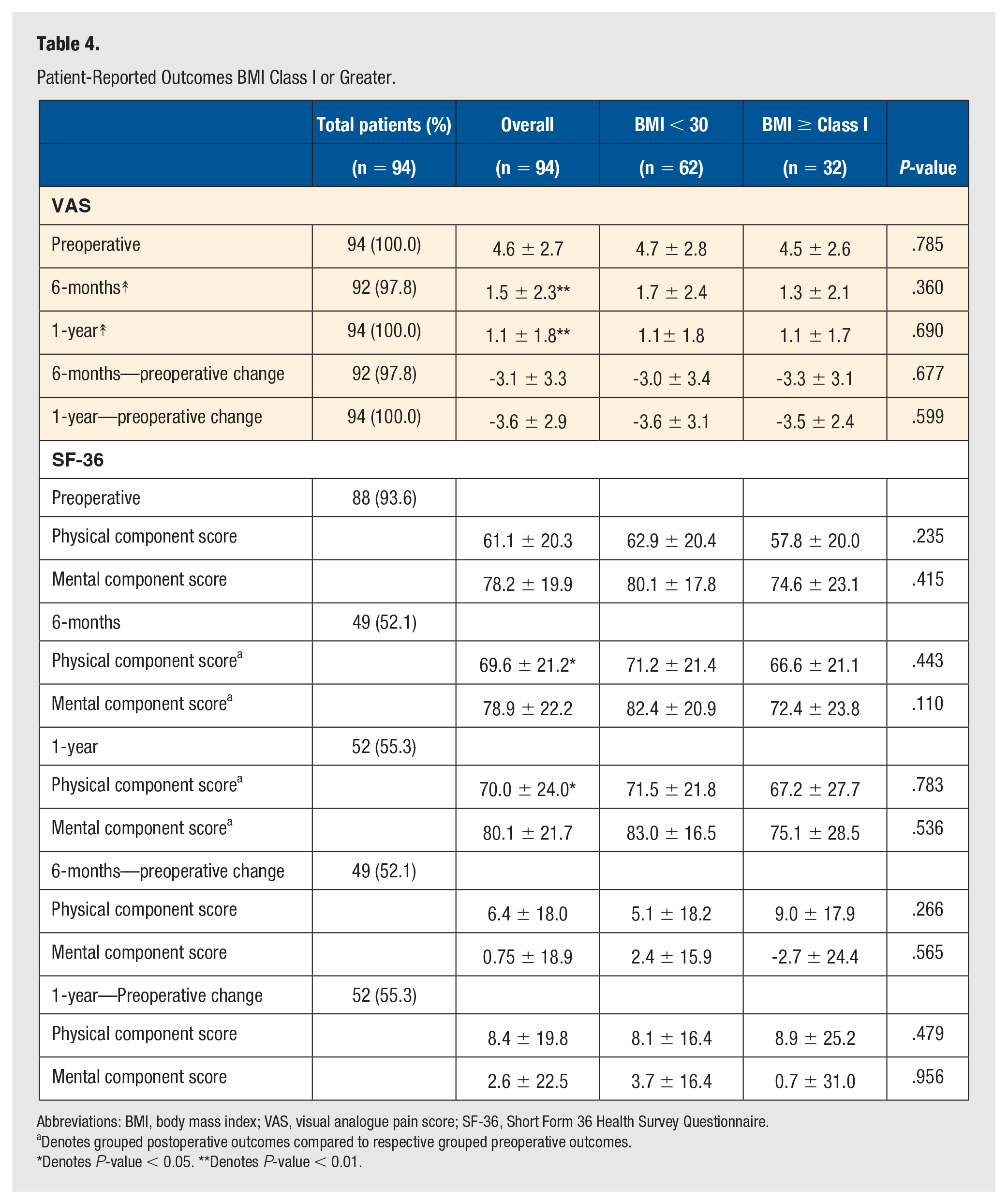
Abbreviations: BMI, body mass index; VAS, visual analogue pain score; SF-36, Short Form 36 Health Survey Questionnaire.
Denotes grouped postoperative outcomes compared to respective grouped preoperative outcomes.
Denotes P-value < 0.05. **Denotes P-value < 0.01.
Obesity’s effect on these reliable outcomes of first MTP fusion is debated. Specifically, data on the relative risk of nonunion during first MTP arthrodesis for obese patients is mixed. A recently published current concepts review regarding risk factors for nonunion in the foot and ankle concluded that there was insufficient evidence to label obesity as an independent risk factor largely because of significant conflicting evidence. 39 Weigelt et al 15 retrospectively reviewed 165 consecutive patients with an average BMI of 28 undergoing 178 primary first MTP arthrodeses to identify risk factors for nonunion. The overall nonunion rate in their cohort was 6.2% (11/178), and the researchers concluded that BMI was not associated with decreased fusion rates. 15 Contrary to these findings, however, Thevendran et al 40 conducted a retrospective case-control validation study in 2015 of a nonunion risk assessment tool in foot and ankle surgery and found that obesity was significantly predictive of nonunion. Although the tools proposed purpose was for evaluation of nonunion risk in any foot and ankle surgery, the validation study only examined ankle arthrodesis, so its direct applicability to first MTP fusion is limited. Supporting that study’s conclusion, however, are the findings by Anderson et al, 30 who in 2013 retrospectively examined 165 patients undergoing first MTP fusion. This study found an overall nonunion rate of 6.7% (11/165) and reported significantly higher rates of nonunion in obese patients (2/5, 40%) compared to non-obese patients. These findings are limited by a small sample size of obese patients (n = 5), as well as the confounding finding that rheumatoid arthritis (RA) was significantly associated with risk for nonunion and at least 1 patient was diagnosed with both RA and obesity. Results from the present study show an overall relatively low nonunion rate of 2.1% (2/94) without any significant difference between obese and non-obese patients. Our study also demonstrates no difference in complications and postoperative outcomes.
Obesity has also been thought to affect patient-reported outcome measures (PROMs) of pain, satisfaction, and quality-of-life, although the data are also mixed. Kuick et al 32 examined patient-reported satisfaction after first MTP fusion at a minimum of 6 months follow-up. Their study reported that 15.9% (7/44) were dissatisfied and 4.5% (2/44) were very dissatisfied, but there was no association with BMI and patient-reported satisfaction. Likewise, a 2003 study 31 examining 38 joints with hallux rigidus undergoing first MTP fusion found no association between body weight or BMI and patient-reported pain reduction postoperatively; however, this study did not report the total number of obese patients included. Somewhat contradicting these studies was a 2011 study by Nemec et al 41 reporting on 95 patients (45 obese) undergoing various midfoot fusions, which found that obese patients were likely to experience a significantly smaller improvement in their postoperative American Orthopaedic Foot and Ankle Society (AOFAS) scores (mean increase of 42) compared to non-obese patients (mean increase of 52; minimum clinically important difference of 5 for midfoot fusion). 42 They also found significantly higher BMI (33.2) among those patients with operative complications than those without (BMI = 29.3). Additionally, that study found that 20% of patients with BMI over 30 reported not being satisfied with their surgical outcome as compared to less than 3% of patients with BMI under 30, although the study was not powered to achieve significance in this outcome measure. However, this study was not isolated to 1st MTPJ arthrodesis, involving multiple midfoot joints and surgical techniques, thus the results may be skewed based on the arthrodesis procedure performed. The current study shows that obesity did not impact the PROMs postoperatively. Overall, there was no significant difference in patient-reported measures of pain (VAS) or quality-of-life (SF-36) between our obese and non-obese cohorts (Table 4). This work is important as many patients with end stage hallux rigidus are limited functionally, and weight loss may be difficult for these patients. As surgeons, we must optimize the patient’s overall health status, and lowering BMI has always been considered an integral part of this. The results of this study suggest that 1st MTPJ arthrodesis outcomes, both clinical and patient-reported, may not be impacted by BMI overall. However, additional studies with larger numbers of patients with class II and III obesity (BMI of 35 or greater) are needed to evaluate whether there is a true difference in outcomes for those patients.
There are limitations to consider when interpreting the results of this study. These conclusions are based on retrospective review of prospectively collected data, and as such no priori power analysis was conducted to adequately power the study to confidently evaluate for significance in our outcome measures. Therefore, it is possible that significant trends exist that we were not able to detect, and a larger sample size would help clarify this. However, evaluation of the mean values for nonobese versus obese patients, suggests that even with a larger patient cohort, clinically meaningful differences likely would not be detected even in a larger sample size. There were also a few significant differences in the baseline characteristics and procedures of our 2 study groups. The non-obese cohort had significantly higher number of rheumatoid patients while the obese cohort had significantly more hypertensives and diabetics. It is unclear how this may have affected our outcomes; however, further research should adequately control for these demographic differences. Additionally, the obese cohort was significantly less likely to receive calcaneal bone grafting at the time of fusion; however, this does not appear to have affected their union rate as there were no nonunions in this cohort. Finally, follow-up of the patients in this study concluded at 12 months postoperatively; therefore, conclusions regarding the effect of obesity on medium and long-term outcomes cannot be drawn from this study and should be examined further.
This retrospective study of 94 patients showed first MTP fusion reliably produces short-term improvements in pain and physical quality-of-life in patients with advanced arthritis without a difference in nonunion, complications, or patient-reported pain and quality-of-life measures in both obese and non-obese patients. This information can be helpful to orthopaedic foot and ankle surgeons as they counsel patients with elevated BMI during the operative management of hallux rigidus.
Footnotes
Acknowledgements
There are no additional acknowledgements for this paper.
Disclosures/Contact Info
Jason T. Bariteau, MD—no disclosures
Michelle Coleman, MD, PhD—no disclosures
Rishin Kadakia, MD—no disclosures; 404-778-2250
Alex Webb, MD, Wesley J. Manz, MD—no disclosures; 984-232-1585
Andrew Fuqua, BS—no disclosures; 615-767-6174
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study has been carried out in accordance with the Declaration of Helsinki and ICMJE recommendations. Prior IRB approval was obtained by Emory IRB. Written consent was obtained preoperatively before collecting the data used for this paper.
Informed Consent
Informed consent was not sought for the present study.
Trial Registration
Not applicable, because this article does not contain any clinical trials.