
Abstract
Background
Medial column internal rotation in hallux valgus (HV) can be measured using weight-bearing computed tomography (WBCT). Anteroposterior weight-bearing foot radiographs’ (WBXR) ability to estimate medial column internal rotation in HV was evaluated comparing these measurements with those obtained from WBCT.
Methods
Three observers evaluated WBCT and WBXR of 33 HV feet twice. Medial column internal rotation was measured with WBCT and classified into 3 levels according to WBXR findings. Intra- and interobserver reliability were obtained for WBXR and WBCT, in addition to WBXR-WBCT correlation.
Results
WBXR and WBCT intraobserver agreement was substantial and near perfect, respectively (κ 0.79 and 0.84). Their interobserver agreement was excellent (intraclass correlation 0.85 and 0.9, respectively). The WBXR-WBCT correlation was substantial (κ 0.68). WBXR diagnostic accuracy to predict the WBCT results was 85%.
Conclusions
The proposed method for medial column internal rotation measurement using WBXR is reliable and has a substantial agreement with WBCT measurements.
Levels of Evidence
Level III
Keywords
Metatarsal pronation (or more accurately called medial column internal rotation) is a parameter that is present in approximately 87% of hallux valgus patients.
Intermetatarsal and metatarsophalangeal angles measured on weight-bearing anteroposterior radiographs are the traditional hallux valgus deformity parameters described in orthopaedic textbooks. These radiographic parameters are the ones commonly corrected with surgery. Some long-term studies have shown a high deformity relapse rate after hallux valgus surgery (>50%). 1 Some recognized factors that are related to this deformity relapse include postoperative sesamoid position, medial column internal rotation, underpowered surgical technique, between others.2-5 Metatarsal pronation (or more accurately called medial column internal rotation) is a parameter that is present in approximately 87% of hallux valgus patients. 6 Approximately 10 years ago, Okuda reported the influence of pronation on postoperative results.4,5,7 A 10- to 12-fold increase in the deformity relapse rate was described when an incomplete sesamoid reduction and/or a round lateral head shape appearance on radiographs was not corrected during hallux valgus surgery. A direct relation between metatarsal pronation and a round lateral head shape appearance has been shown using digitally reconstructed radiographs from computed tomography scans. 8 In the following years, it has been shown that pronation present in hallux valgus patients is really the result of a medial column pronation not an isolated first metatarsal pronation.9-13 In addition, the term pronation is not entirely accurate, because this concept includes motion in 3 planes. Internal rotation represents more precisely what is being discussed in this research.
Since the medial column internal rotation finding, different techniques have been proposed that are able to correct this rotation (eg, PROMO, 14 Lapidus, 15 Dome osteotomy 16 ). These techniques aim to correct pronation at the metatarsal, even though the metatarsal is not the origin of pronation.
A medial column pronation (internal rotation) measurement is not easily obtained from plain radiographs given that it is a rotational deformity along the medial column axis. To date, there is no reliable method to quantify medial column internal rotation. Okuda et al 4 in 2007 identified 3 different shapes of the metatarsal head: round, intermediate, and angular, with no clear definition what these meant. Yamaguchi et al 8 in 2015 further studied the head shapes utilizing digitally reconstructive radiographs obtained from computed tomography data. They showed how rotation and inclination of the metatarsal changes the lateral head shape (round contour). Finally, Wagner et al17-19 identified how these different head shapes anatomically correlated to specific internal rotation values but lacking statistical demonstration.
Due to the relationship between medial column internal rotation and weight bearing 10 and the ability to conduct 3-dimensional foot analysis, it can be assumed that the best available method to measure medial column internal rotation is a weight-bearing computed tomography (WBCT) evaluation.6,10,13,20 Nevertheless, radiographs are cheaper and more widely available than a WBCT evaluation and are routinely the only imaging studies requested when planning hallux valgus surgery. Therefore, it would be desirable to obtain a medial column rotation estimation from standard foot weight-bearing radiographs.
The main objective of this study was to validate a proposed medial column internal rotation estimation method17-19 that utilizes weight-bearing AP foot view radiographs (WBXR). Data obtained from WBXR were compared with data from WBCT scans. The secondary objective was to investigate the interobserver and intraobserver reliability of this medial column internal rotation measurements. The evaluation was performed analyzing the metatarsal head shape.
Methods
After approval by the local ethics committee and institutional review board, 33 consecutive patients with hallux valgus who presented to a foot and ankle clinic were prospectively selected, from March 2018 to October 2018: 30 female and 3 male patients with a mean age of 51 years. Exclusion criteria were evident first metatarsophalangeal radiographic osteoarthritis, metatarsal dysplasia, and previous trauma that affected the distal first metatarsal joint. Patients were included if they had a WBXR and a corresponding WBCT scan, independently of their surgical status (ie, preoperative or postoperative). The senior author taught 3 fellowship-trained foot and ankle surgeons how to measure medial column internal rotation looking at the metatarsal head shape on WBXR and WBCT scans. After training, the 3 trained surgeons measured medial column rotation on 33 WBXR and their corresponding WBCTs that were presented in a random order. Five days after the initial measurement session, the surgeons repeated the rotation measurements on the same WBXRs and WBCTs in a different order.
Obtaining Medial Column Rotation Measurements on WBCT Scans
First, an adequate weight-bearing coronal CT (Curvebeam) image of the first metatarsal head was selected (WBCT settings: 360° rotation; 360 projection images; matrix: LFOV 950 × 950, MFOV 666 × 666; kVp: LFOV 100-120, MFOV 100-120; 5 mA [all protocols]; mAs: LFOV 43.2, MFOV 21.6; slice thickness: LFOV 0.37 mm, MFOV 0.3 mm). To do this, the CT cut in which the sesamoid facets of the first metatarsal head is more clearly visible is chosen, with an evident sharp lateral and medial border. Second, a line is drawn following the weight-bearing surface. Third, a second line is drawn from the lateral border of the lateral sesamoid facet to the medial border of the medial sesamoid facet. Finally, the angle between the 2 previously drawn lines is measured (Figure 1). This is the alpha angle previously published by Kim et al.6,21
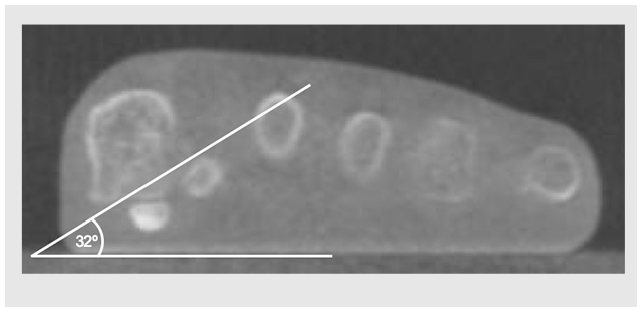
Weight-bearing computed tomography of a left foot. Coronal cut at the level of the sesamoid facets. Angle measured between a floor line and a line that starts at the lateral corner of the lateral sesamoid facet and ends at the medial border of the medial sesamoid facet. Angle measured 32°.
Obtaining Medial Column Internal Rotation Measurements on Weight-Bearing Radiographs
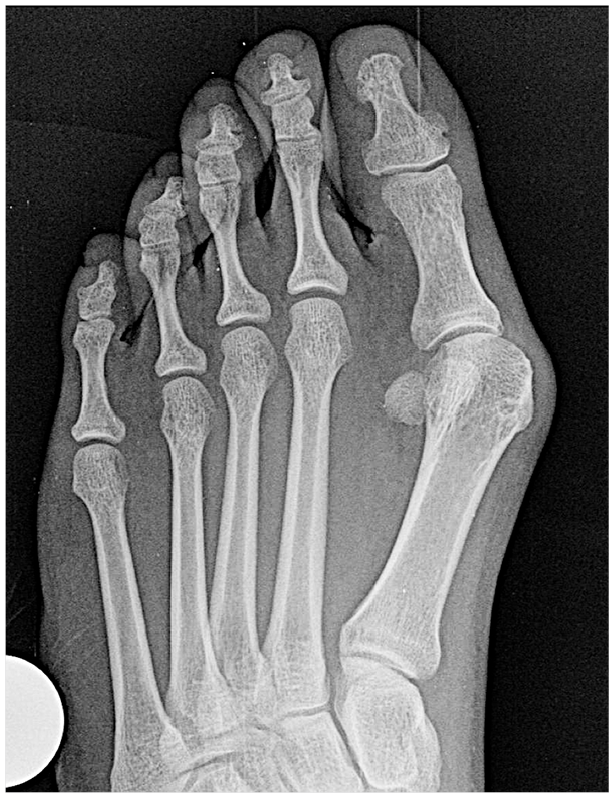
Medial column internal rotation8,22 was analyzed on a bilateral AP foot WBXR. The AP foot WBXR is taken with the patient standing with both feet together on the radiograph cassette. The X-ray beam is angled in 15° from anterior to posterior, centered at the midfoot. Medial column internal rotation was divided into 3 levels depending on the roundness of the lateral aspect of the metatarsal head on an AP foot WBXR. Digital radiographic software (PACS; General Electronic) was used to identify medial column internal rotation levels into 0, 1, 2, and 3 based on the descriptions below. Level 0 represent 0° to 10° of medial column rotation. The first metatarsal lateral head contour is flat (Figure 2). Level 1 (Figure 3) represents 10° to 19° of medial column internal rotation. The metatarsal head lateral condyle is visible on the radiograph as a round image. A clear mismatch appears where the condyle contour (round lateral image) meets the distal metatarsophalangeal joint line, like a right-angle step. This corner extends normally for 0.5 to 3 mm (Figure 4, magnified).

AP weight-bearing foot view of a right foot without first medial column internal rotation. Please note the sharp edge at the lateral corner of the first metatarsophalangeal joint. A flat or straight line follows this corner into the metatarsal shaft.
AP weight-bearing foot view of a right foot with hallux valgus and with mild (level 1) medial column internal rotation. Please note the sharp edge at the lateral corner of the first metatarsophalangeal joint. Immediately proximal to this edge, a round contour appears, representing the lateral metatarsal condyle.

Magnified view of Figure 3, focusing on the metatarsal head. Please note the sharp edge and step at the lateral corner of the first metatarsophalangeal joint that is continuous proximally with a round contour. This round contour represents the metatarsal head condyle that starts to appear on an AP view given the metatarsal rotation. The black line follows the contour for easier identification.
Level 2 (Figure 5) represents 20° to 29° of medial column internal rotation. The metatarsal head lateral condyle (round lateral head contour) when followed distally is in continuity with the metatarsophalangeal joint line (no straight line or corner exists between the condyles and the distal joint surface as in level 1 pronation). However, they do not form a continuous and congruent round line with the articular surface as in level 3. The joint line changes its curvature radius from the head to the condyles and does not form a perfectly round, continuous circle.

AP weight-bearing foot view of a right foot with hallux valgus and with moderate (level 2) medial column internal rotation. Please note that there is no sharp edge at the lateral corner of the first metatarsophalangeal joint. The distal metatarsophalangeal joint laterally is continuous with a round contour laterally at the head, which represents the condyles. The line follows the joint contour for easier identification. This line has no step or angle at the joint junction (as in level 1) but does present a curvature radius change compared with the distal joint line.
Level 3 (Figure 6) represents more than 30° of medial column internal rotation. The metatarsal head condyle contour (lateral head round image), if followed distally, is in absolute continuity with the distal metatarsophalangeal joint line. The condyle contour forms a continuous round line with the articular surface joint line with no interruption or change in the curvature radius. A circle could be superimposed over the metatarsal head and would match the joint line and the metatarsal condyle contour. Figure 7 shows the 3 levels side to side to help with differentiation. This classification was already proposed using anatomical references.17-19

AP weight-bearing foot view of a right foot with hallux valgus and with severe (level 3) medial column internal rotation. Please note that there is no sharp edge at the lateral corner of the first metatarsophalangeal joint, and on the contrary, there is a congruent round contour, on which a circumference could be superimposed. The line follows the contour for easier identification. This foot had previously some kind of metatarsal shaft osteotomy.
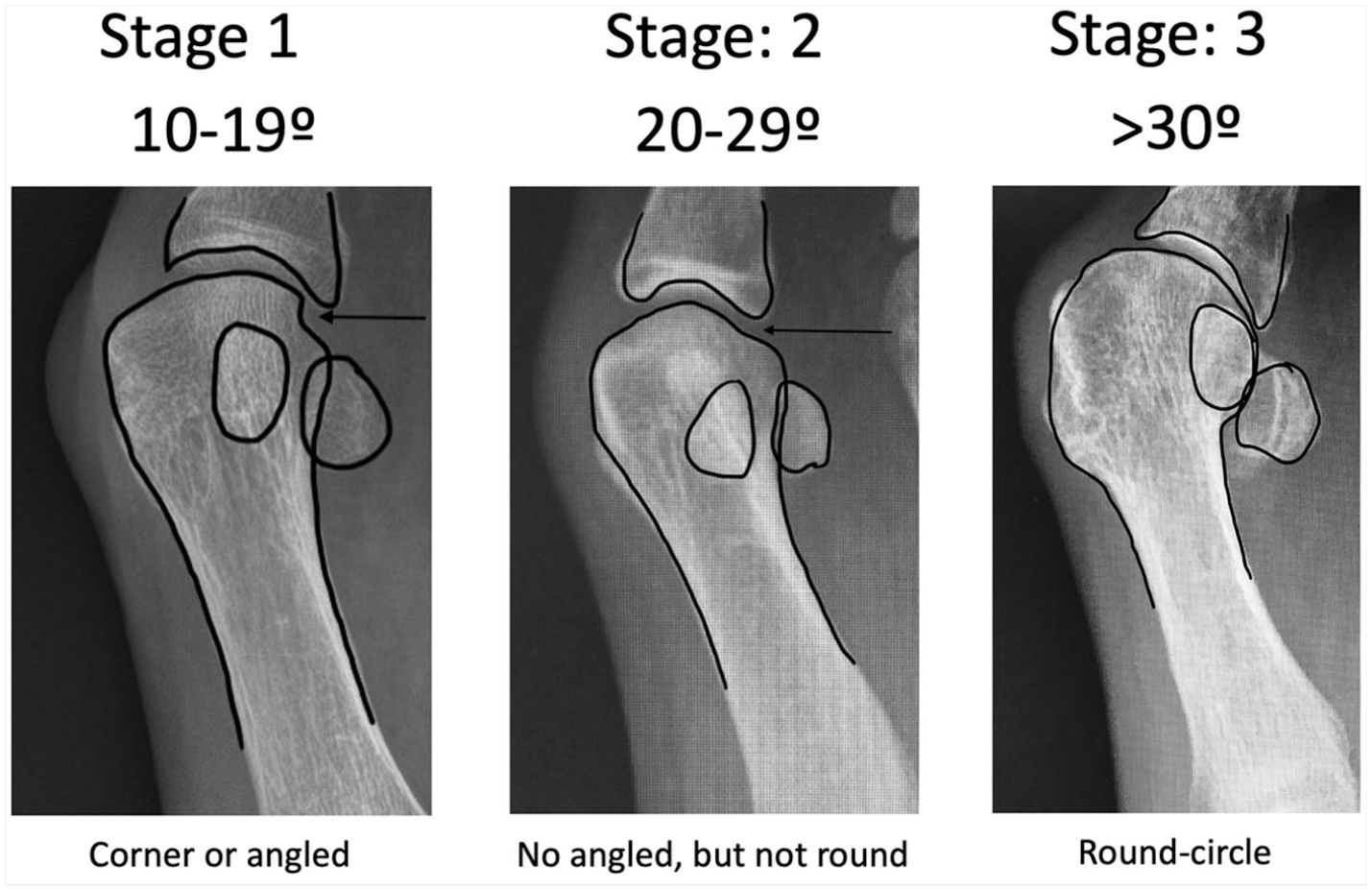
Internal rotation stages. Comparison image showing the 3 levels of medial column internal rotation. Note that in the first internal rotation level, the lateral head contour presents an edge or corner (arrow). At the second level the corner disappears and a round contour follows the joint line. At the third level, when following the joint line, the lateral head contour resembles a circle, without any change in curvature radius from the distal joint line.
Medial column internal rotation in WBXR was classified into 3 levels as shown before, yielding a categoric variable. In WBCT (gold standard), pronation was measured in degrees and subsequently separated into 3 levels (categories): level 1: 10° to 19°; level 2: 20° to 29°; level 3: >30°. For each WBCT level, a contingency table was created, adding the corresponding radiographic information for each patient (gold standard-WBCT vs diagnostic test-WBXR).
Cadaveric Example
To reproduce this study findings of how a medial column internal rotation changes the metatarsal head shape on X-rays, a cadaveric trial was performed. A lower limb cadaver specimen without hallux valgus and without medial ray internal rotation was analyzed. A simulated (10 kg) weight-bearing AP view foot radiograph was obtained (ie, image with zero degrees of rotation; Figure 8). As the reader can see, the metatarsal head does not have a lateral round contour, similar to Figure 2. To simulate medial column internal rotation, a first metatarsal proximal transverse osteotomy was performed, through which internal rotation was applied to the distal segment. A 1.6 K-wire was driven 1 cm distal to the osteotomy (mobile metatarsal segment) and another 1.6 K-wire was driven 1 cm proximal to the osteotomy. By progressive internal rotation of the distal K-wire, 25° of metatarsal internal rotation was achieved. Internal rotation was measured with the help of a goniometer measuring both K-wires divergence. A WBXR was obtained (Figure 9). Please note how this image shares with Figure 5 the level 2 internal rotation criteria (no corner or step is present at the lateral head contour, but it does not form a uniform round image).

AP weight-bearing foot view of a right cadaver foot without hallux valgus and without medial column internal rotation. Note the metatarsal head squared shape. A sharp edge at the lateral metatarsophalangeal corner can be seen. A straight line can be drawn from the lateral metatarsophalangeal corner to the diaphysis. The black line follows the contour for easier identification.

AP foot fluoroscopy. A proximal transverse osteotomy can be seen. This image was taken with 25° (level 2) of medial column internal rotation. The line follows the contour for easier identification.
Statistical Analysis
Data were analyzed using Stata software (StataCorp, 1996-2019) and the help of our university statistician. Intraobserver reliability and WBXR to WBCT correlation were evaluated using the κ coefficient. The interobserver reliability was measured using the intraclass correlation estimates (ICC) (95% confidence interval) for WBXR and WBCT observations.
Contingency tables were built for each rotation level (WBCT as gold standard). Sensitivity (Sens), specificity (Spec), positive predictive value (PPV), negative predictive value (NPV), diagnostic accuracy (dga), positive likelihood ratio (LR+), and negative likelihood ratio (LR−) were determined.
Results
Of a total of 198 radiographic observations (33 X-rays analyzed by 3 observers at 2 different occasions), 170 were in keeping with WBCT measurements, which gives an overall diagnostic accuracy of 85% ((true positive + true negative)/total tests). The intraobserver agreement for the WBXR observations yielded a κ value of 0.79 (substantial agreement). The intraobserver agreement for the WBCT observations yielded a κ value of 0.84 (almost perfect agreement). The interobserver agreement for the WBXR and WBCT observations was 0.85 (range = 0.78-0.91; excellent agreement) and 0.90 (range = 0.86-0.94; excellent agreement), respectively. The WBXR-WBCT correlation yielded a κ value of 0.68 (substantial agreement). In Tables 1, 2, and 3, contingency data are shown for each category. The diagnostic accuracy ((true positive + true negative)/total tests) for stages 1, 2, and 3 is 83%, 81%, and 95%, respectively.
Contingency Table and Data for Level 1 Medial Column Internal Rotation a .
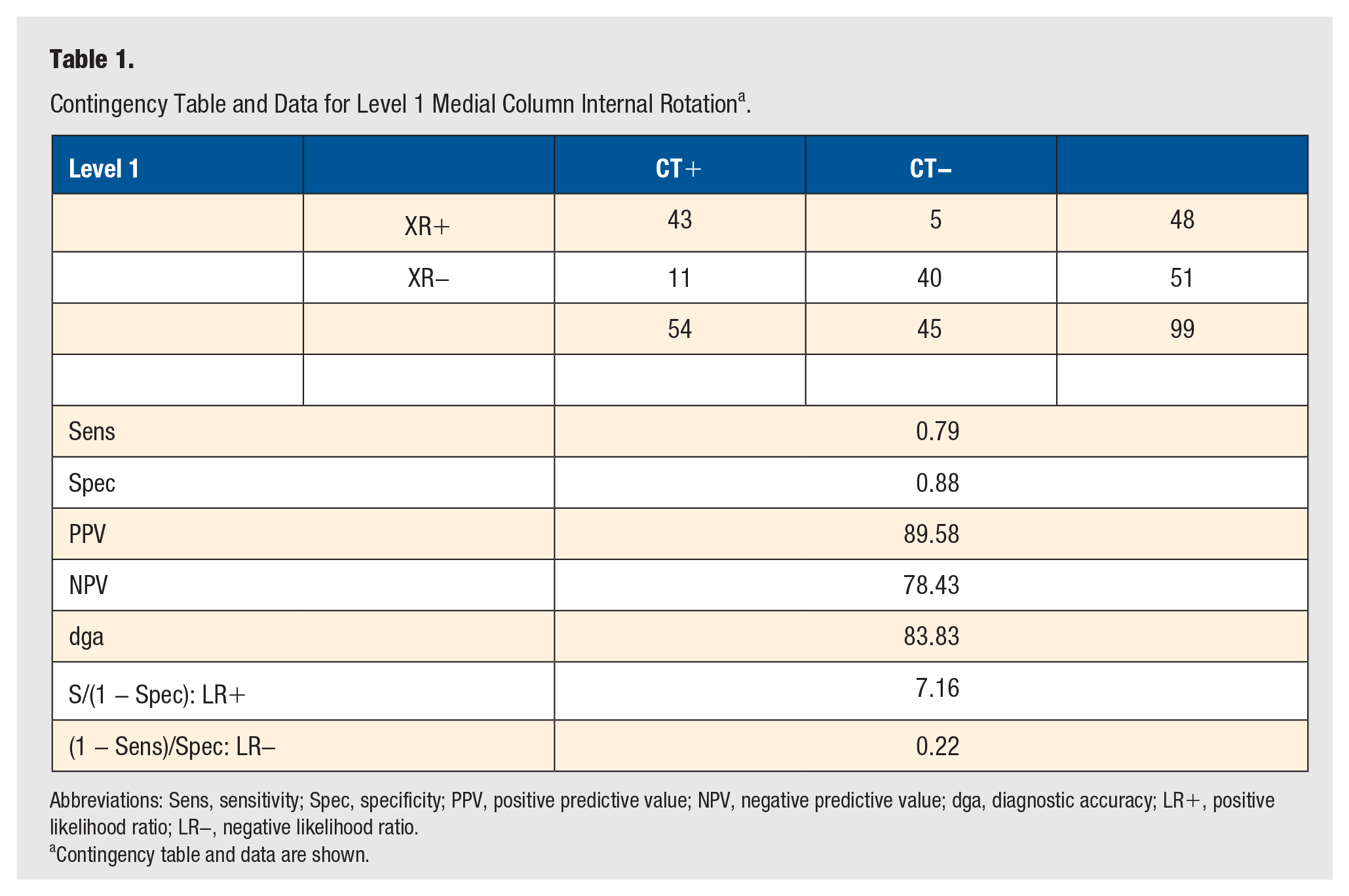
Abbreviations: Sens, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value; dga, diagnostic accuracy; LR+, positive likelihood ratio; LR−, negative likelihood ratio.
Contingency table and data are shown.
Contingency Table and Data for Level 2 Medial Column Internal Rotation a .
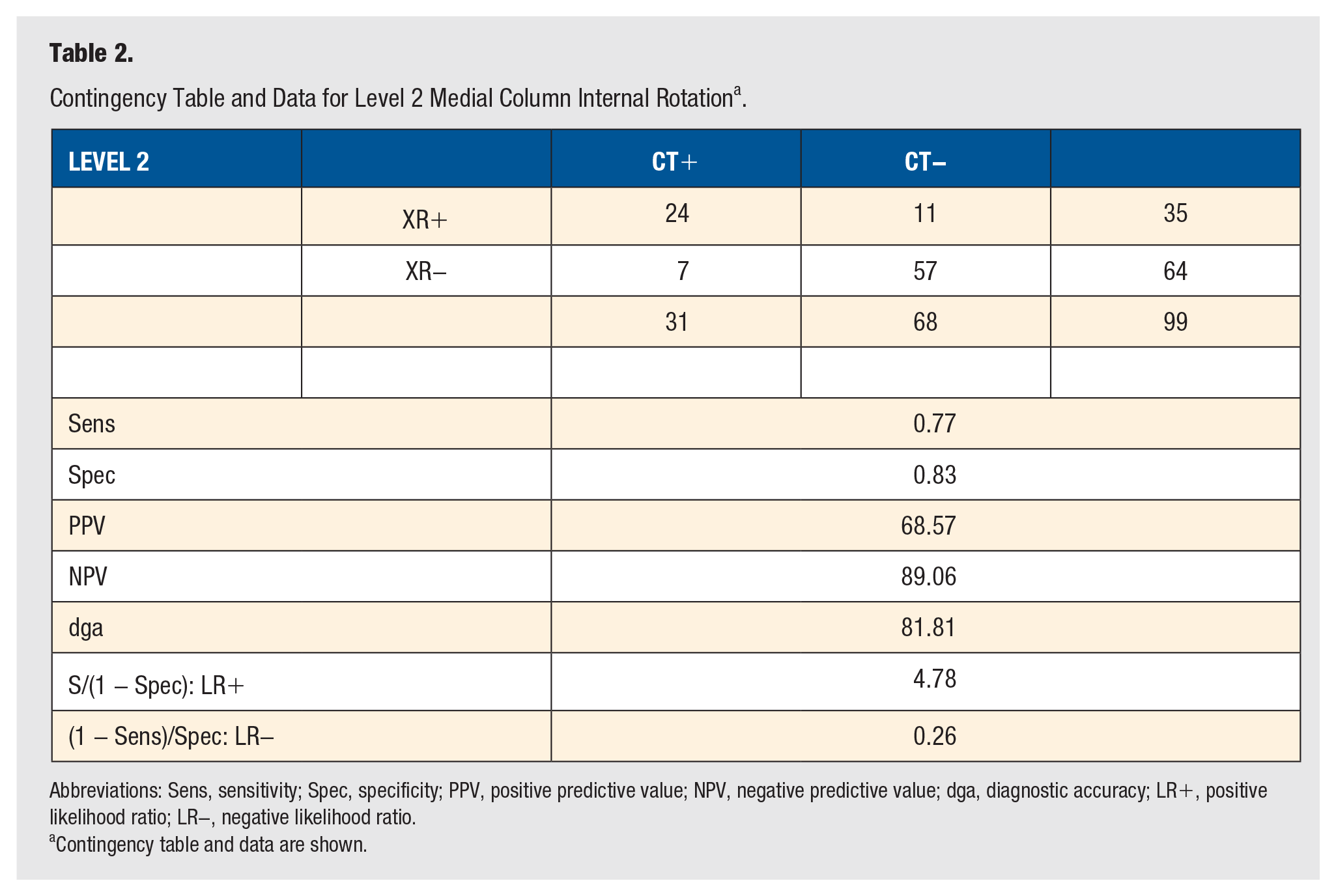
Abbreviations: Sens, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value; dga, diagnostic accuracy; LR+, positive likelihood ratio; LR−, negative likelihood ratio.
Contingency table and data are shown.
Contingency Table and Data for Level 3 Medial Column Internal Rotation a .
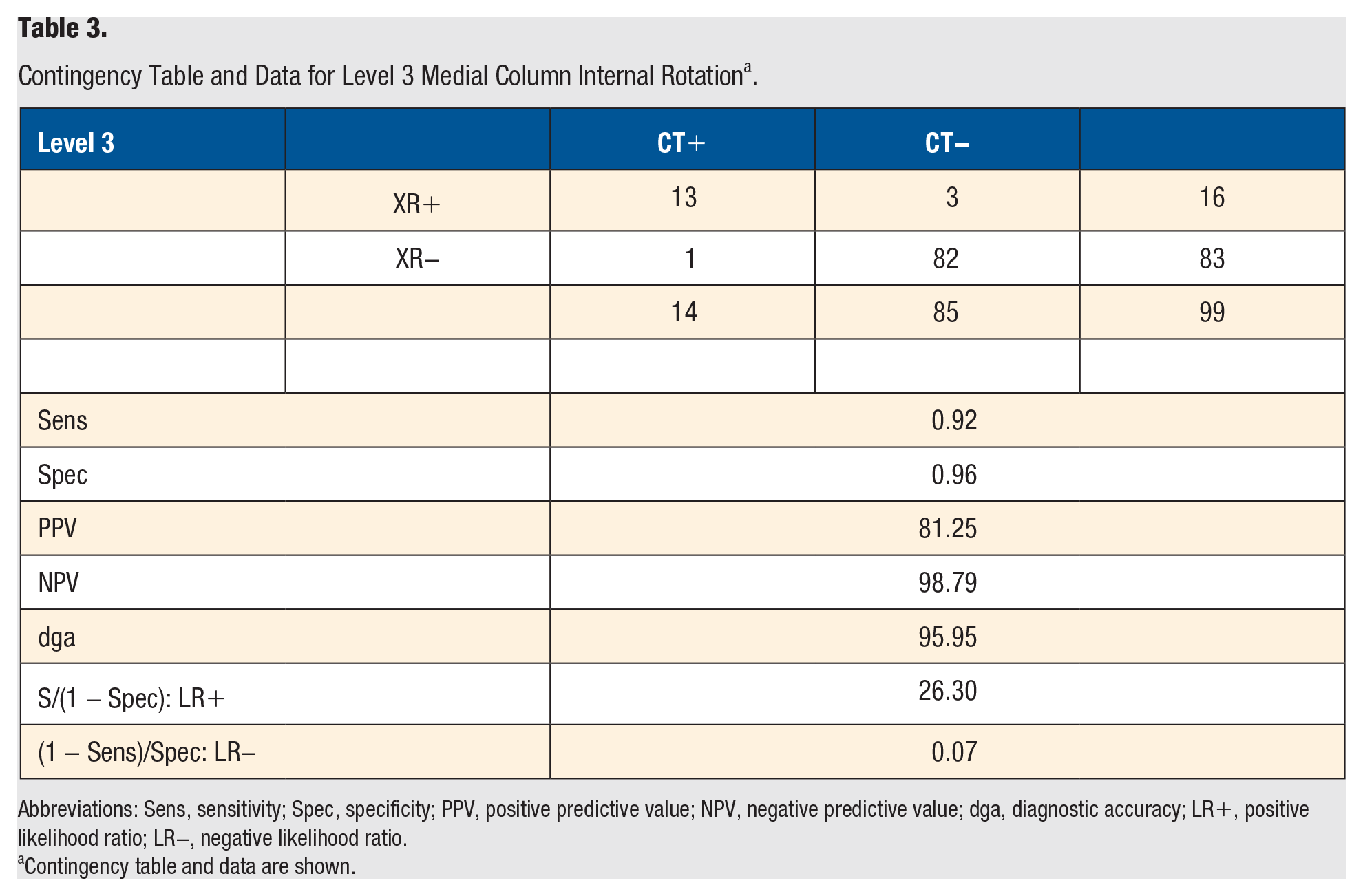
Abbreviations: Sens, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value; dga, diagnostic accuracy; LR+, positive likelihood ratio; LR−, negative likelihood ratio.
Contingency table and data are shown.
Discussion
Medial column internal rotation was recently described as an important variable to consider when performing hallux valgus surgery.4-7 If not corrected, medial column internal rotation could be responsible for an increase in the relapse rate. However, there is no reliable nor validated method to quantify medial column rotation using plain weight-bearing radiographs.
The authors first attempted evaluating medial column rotation with weight-bearing axial sesamoid views but decided to abandon this approach due to inconsistency in obtaining reproducible radiographic images. The method is difficult for the radiology technician to obtain and uncomfortable for the patient (standing on a radiographic cassette with 30° of ankle equinus and toes dorsiflexed). In addition, hallux dorsiflexion reduces the sesamoids onto their facets, thus hindering first metatarsal pronation measurement. 23 Finally, this axial view did not show good correlation with WBCT. 20 The metatarsal rotation measurement method for WBCT was already published,6,18 nevertheless, there is no strong evidence on which are the best cuts or the best measurement method for estimating medial column internal rotation. It is important to emphasize that for accurate measurement, a weight-bearing image must be used. Some surgeons do not measure rotation preoperatively and just estimate pronation intraoperatively using fluoroscopy. Given that weight-bearing changes pronation10,24 and only a simulated weight-bearing view can be obtained intraoperatively, pronation should be analyzed in preoperative weight-bearing images rather than in the intraoperative setting.
Weight-bearing AP foot view radiographs are the most common method to evaluate and measure a hallux valgus deformity. It is cheaper and widely available compared to a WBCT scan. WBCT scans are not available throughout the world. Estimating medial column rotation from the sesamoid position is not a reliable parameter, given that they can be dislocated from their facets in presence and in absence of medial column rotation.6,21 Okuda reported that the sesamoid position and lateral head shape indirectly represented a pronated medial column.4,5,7 Thus, we analyzed the lateral head shape to estimate the medial column rotation. The more pronated a medial column is, the more lateral metatarsal condyle you will be able to see on an AP radiographic foot image forming a rounded appearance.
With the radiographic classification described here, internal rotation was divided into 3 levels: Level 1 (mild, 10° to 20°), Level 2 (moderate, 20° to 30°), and Level 3 (severe, >30°). This classification showed a good inter- and intraobserver reliability and good correlation with CT scans. Having 3 levels of deformity gives a decent approximation to the medial column pronation, avoids complicated calculations, and provides a good approximation of the real measured rotation on WBCT with a tolerable error. When analyzing the results obtained, there is substantial agreement regarding intraobserver and interobserver observations, for WBXR and WBCT. When analyzing the correlation between WBXR and WBCT observations, a substantial agreement was obtained as well, with an agreement percentage over 80%. There were 28 errors (out of 198 measurements) in correlating radiographs and CT scans. Most of those errors occurred in cases where WBCT showed a value close to the limit between 2 rotation levels. As in all classifications, the gray area between one level and the following level is always difficult to define.
The authors’ practical recommendation is to learn how to use WBXR to identify Level 1 internal rotation (“is there a corner or straight segment between the metatarsophalangeal joint line and the lateral aspect of the head contour?”) and Level 3 internal rotation (congruent and continuous round contour starting from the metatarsophalangeal joint line ending on the lateral aspect of the head contour; “could you fit a circle in that image?”). Level 2 is the most difficult to identify, but it can be obtained just by ruling out Levels 1 and 3 rotation.
The main limitation of this study is that a digital radiograph is needed. There are places around the world where traditional film radiography is still prevalent, which possesses less definition than a digital radiograph. With traditional film radiographs, it could be more difficult to clearly differentiate the head joint line, the sesamoids, and the metatarsal condyle contour. The authors found that to accurately measure and clearly identify the medial column rotation stage, every metatarsal head needs to be magnified using the digital radiographic software. In addition, the authors found that this method is not accurate in cases with metatarsophalangeal osteoarthritis. Finally, it is important to note that there are hallux valgus cases with sesamoid dislocation and mild to no medial column internal rotation. This could happen in posttraumatic cases or in long-standing hallux valgus deformities, between others. This finding will be better visualized with a WBCT than radiographs.
Conclusions
The medial column internal rotation estimation method presented in this study is easy to perform, uses simple radiographic imaging routinely obtained, and is a reliable method with a good performance as a diagnostic test.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval was provided by the local ethics committee and the institutional review board.
Informed Consent
Not applicable.
Trial Registration
Not applicable.