
Abstract
Background
Hallux valgus is one of the most common orthopaedic deformities of the foot, affecting as much as 23% of the population age 18 to 65. In addition to its high prevalence, it has a complex multifactorial pathogenesis. Surgical correction options have variable rates of success and new techniques are being developed. The modified Lapidus procedure attempts to correct in 3 planes of deformity, which may create a steeper learning curve for those newly adopting the technique.
Methods
A retrospective review was performed on patients who underwent hallux valgus reconstruction with a modified Lapidus procedure between March 2018 and July 2020. Exclusion criteria included revision surgery, 6 or more concurrent procedures, or a flexor digitorum longus tendon transfer for adult acquired flatfoot correction.
Results
There were a total of 81 modified Lapidus procedures for hallux valgus within the study time frame and 68 were included in the study. Over a period of 2 years there was a significant decrease in overall surgery duration from 78.93 minutes at month 0 to 61.80 minutes at 24 months (P = .036). The average preoperative/postoperative intermetatarsal angles were 15.08° and 4.91°, respectively. There was an average decrease of 10.17°. The rate of nonunion was 4.41% (3/68), and the rate of recurrence at 6 months was 5.88% (4/68). There was not a significant difference in the rate of recurrence (P = .394) or the rate of nonunion (P = .817) as the surgeon increased in experience.
Conclusion
Although there is a significant learning curve for the modified Lapidus procedure, it is largely overcome by the 23rd case. Additionally, experience with the technique does not appear to affect the patient outcomes of nonunion or recurrence.
Levels of Evidence
Level IV: Retrospective
Hallux valgus is one of the most common orthopaedic deformities of the foot, affecting as much as 23% of the population age 18 to 65, and 35% over age 65.
Hallux valgus is one of the most common orthopaedic deformities of the foot, affecting as much as 23% of the population age 18 to 65, and 35% over age 65. 1 In addition to its high prevalence, it has a complex and multifactorial pathogenesis. Numerous surgical options for hallux valgus correction exist with each of these procedures have been shown to have varying levels of both success and complications.1-3
In the past, hallux valgus treatments have been based on focusing on 2 dimensions.4,5 With the increased popularity of using weight-bearing computed tomography, it is now understood the deformity exists in all 3 anatomical dimensions, and this has promoted surgeons to utilize techniques that address the entire triplanar deformity.
Given this new understanding, modified surgical techniques and new devices have been developed to correct this 3D deformity utilizing a modified Lapidus procedure. Given these novel interventions and technique, there may be a learning curve for surgeons associated with this modified Lapidus procedure. If a learning curve exists and is not understood, the success of a new procedure can be underestimated. This can negatively affect the dissemination of an improved procedure and patients may not receive the best surgical intervention available.6,7
The purpose of the study was to determine if there was a learning curve when performing a 3D correction utilizing a modified Lapidus procedure for correction of a hallux valgus deformity. Additionally, we sought to assess preoperative/postoperative intermetatarsal angles, rates of nonunion, and rates of recurrence at 6 months.
Methods
After institutional review board approval, a retrospective chart review was performed on patients who underwent the hallux valgus reconstruction with a modified Lapidus procedure between March 1, 2018, and July 16, 2020. Surgery was performed by a single surgeon (JBJ). Exclusion criteria included revision surgery, 6 or more concurrent procedures, or if they had a flexor digitorum longus tendon transfer for adult acquired flatfoot correction.
Surgical Procedure
A standard dorsal medial approach to the patient’s first tarsometatarsal joint was done. An oscillating saw was used to resect the plantar eminence of the joint. Then a de-rotational pin was placed. A lateral release of the first metatarsophalangeal joint was performed if needed based on the ability to correct the rotation, hallux valgus, and/or intermetatarsal angle. The de-rotational pin along with the C-clamp was used to de-rotate the first metatarsophalangeal joint. At this time, acceptable correction of the hallux valgus and intermetatarsal angle was confirmed with fluoroscopic imaging. The joint seeker was then placed, followed by the cut guide (Treace Medical Concepts), which was pinned in place. The distal portion of the medial cuneiform and proximal portion of the first metatarsal base were then resected. Next, one of the pins was removed and a compressor distractor was utilized. The joint was then distracted, the bony cuts were removed, and the joint was compressed. Initially 90-90 plates (Treace Medical Concepts) were utilized for correction. During the study period, the surgeon switches to a 90-90 staple construct (Wright Medical). Finally, acceptable correction across the first tarsometatarsal joint as well as acceptable correction of both the hallux valgus and the intermetatarsal angle was confirmed with fluoroscopic imaging. The majority of patients then had a medial approach to the first metatarsophalangeal joint and a silver bunionectomy along with medial capsulorrhaphy. Postoperatively the patients were non–weight bearing for 4 to 6 weeks and then progressed to full weight bearing over an additional 2 weeks in a postoperative shoe. Patients were allowed to return to a regular shoe between 6 and 8 weeks.
Data Collection and Statistical Analysis
The surgical start and stop times were recorded. The relationship between the increasing number of surgical procedures in series and increasing months of experience was compared with surgical duration using a linear regression model. The surgeries were also divided into 3 groups based on length of experience in the case series: low, medium, and high experience. Each group underwent a linear regression and the average time for each group was compared to one another using an adjusted Wald test. Individual case-specific information was also recorded, including fixation method comparing staples versus screws, number and type of concurrent procedures, incidence of nonunion, incidence of recurrence after 6 months, and preoperative/postoperative intermetatarsal angles. The software package STATA was used for all statistical analyses.
Results
There were a total of 81 modified Lapidus procedures for hallux valgus within the study time frame. Of the 81 subjects, 68 were included in the study. The 13 patients who were excluded from the study had the following procedures: 10, revision surgery; 1, 6+ concurrent procedures; and 2, concurrently underwent a flexor digitorum longus tendon transfer and flatfoot reconstruction.
The linear regression assessing the relationship between increase in experience with number of surgical procedures and surgery duration demonstrated a significant relationship (Figure 1; P = .040, an adjusted R2 = .32). For each 1-month increase in experience there is an average decrease of 43 seconds, 95% confidence interval 2.4 seconds to 83.4 seconds (P = .036, adjusted R2 = .29). The increase in months of experience was associated with a decrease in surgery duration. With 0 months of experience, the average duration was 78.93 minutes. At 12 months, the average duration was down to 70.36 minutes. At 24 months, the end of the series, the average duration was 61.80 minutes (Figure 2). For fixation methods, there was no significant difference between the use of plates and screws or staples (P = .117). The rate of nonunion was 4.41% (3/68) and was not significantly decreased (P = .817) as the surgeon increased in experience. The rate of recurrence at 6-month follow-up was 5.88% (4/68) and was not significantly decreased (P = .394) as the surgeon increased in experience (Table 1).
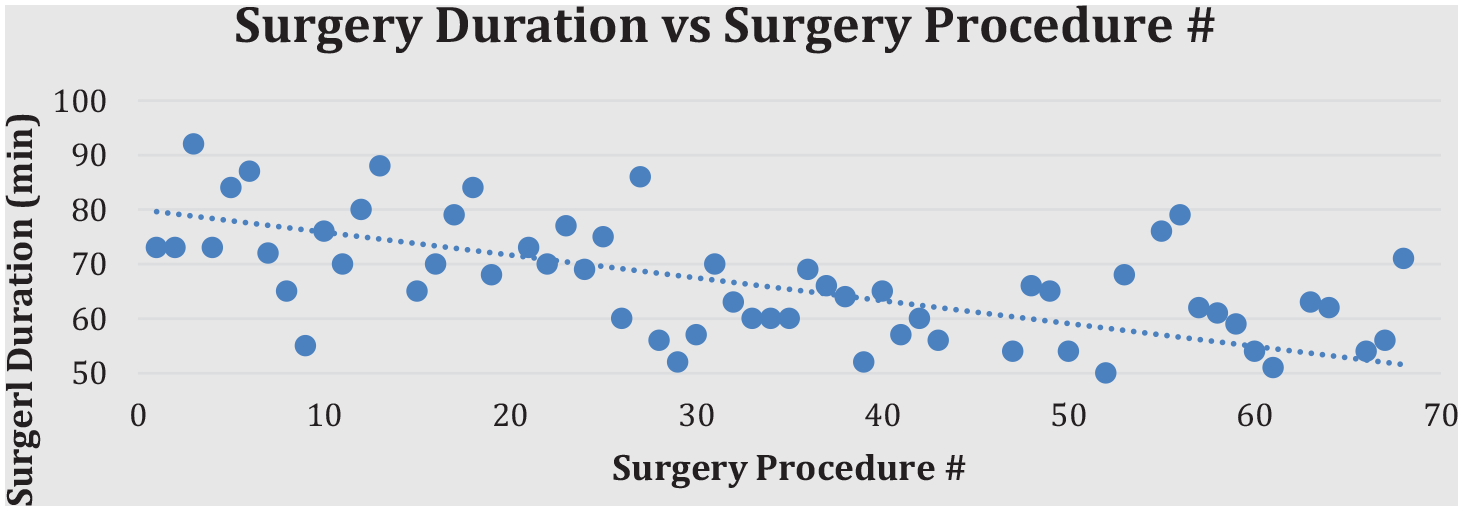
Linear regression demonstrating relationship between surgical duration and surgical procedure number in series.
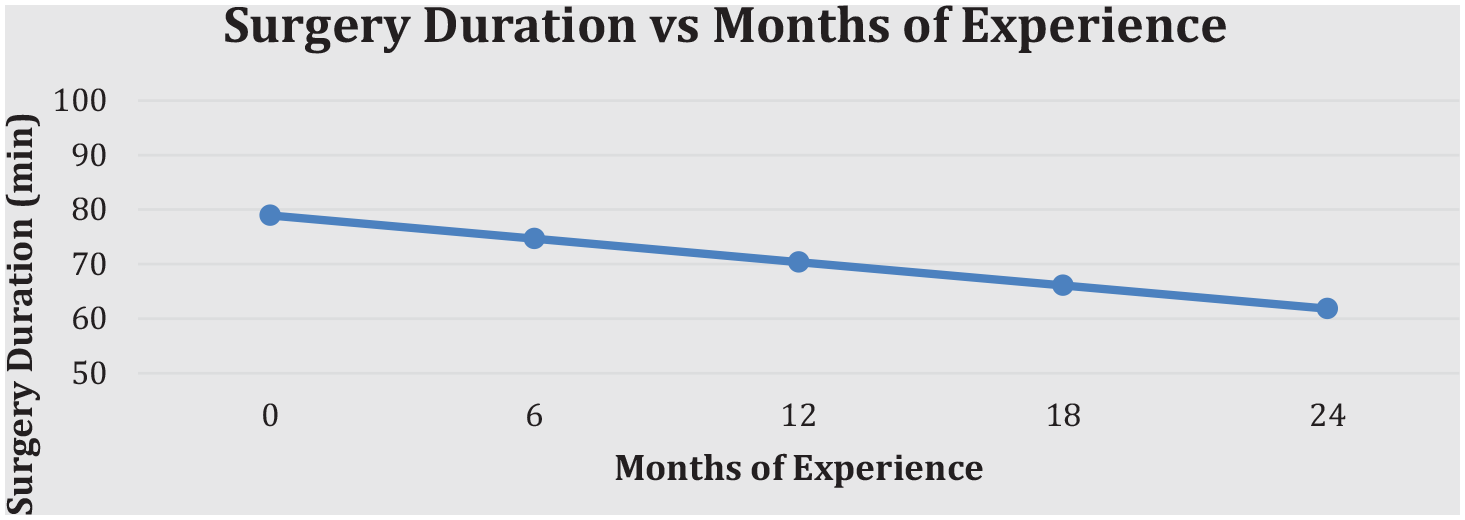
Average surgical duration as surgeon progresses through the case series.
Average duration of surgery, IMA decrease, and rates of nonunion and recurrence based on level of experience.
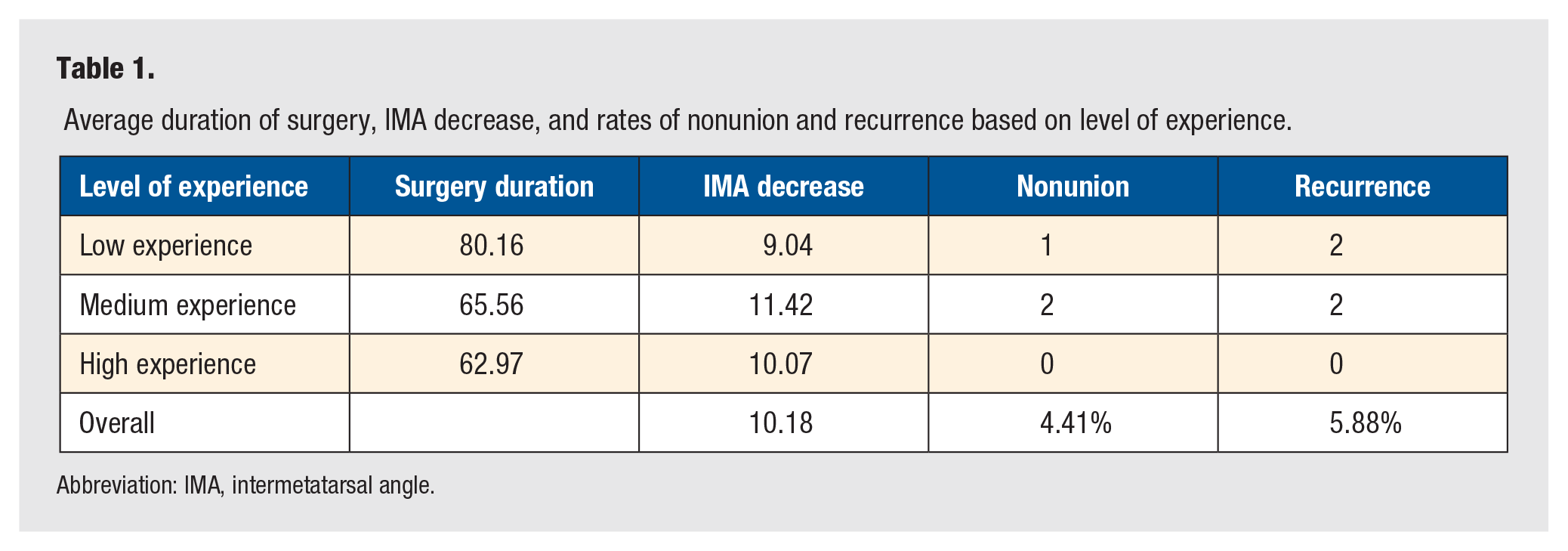
Abbreviation: IMA, intermetatarsal angle.
The subjects were then divided into 3 groups based on experience. Low experience contained the first 23 patients, medium experience contained the middle 23 patients, and high experience contained the last 22 patients that underwent the modified Lapidus procedure. The groups had an average surgery duration of 80.16 minutes for low experience, 65.56 minutes for medium experience, and 62.97 minutes for high experience. Compared to low experience, medium experience had a significantly shorter surgery duration time on average with a decrease on average of 14.60 minutes (P = .002). Compared to low experience, high experience had a significantly shorter surgery duration time on average with a decrease on average of 17.18 minutes (P < .001; Figure 3). With subjects grouped, the rate of nonunion continued to be not significant (P = .431). The preoperative/postoperative intermetatarsal angles (IMA) were also measured. The average preoperative IMA was 15.08°, and the average postoperative IMA was 4.91°. There was an average decrease of 10.17°. The low experience group had a mean decrease in IMA of 9.04°, medium experience had a mean decrease of 11.42°, and high experience had a mean decrease of 10.06° (Table 1). The decrease in IMA of the medium experience group was significantly higher than the low experience group (P = .048). The decrease in IMA of the high experience group was not significantly higher than the low experience group (P = .261).
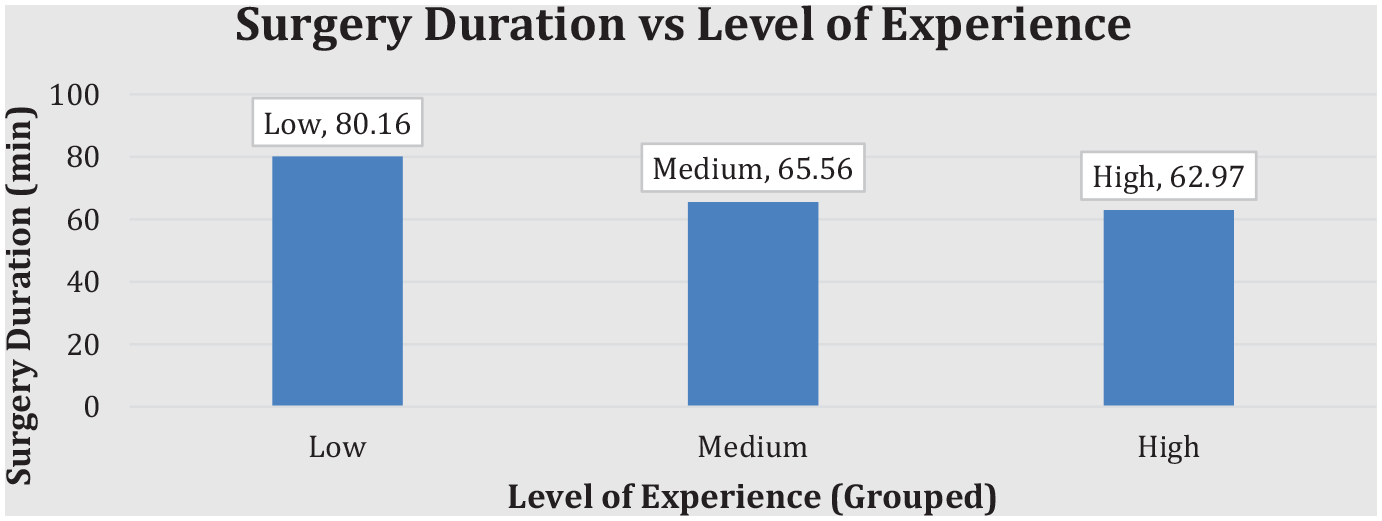
With the series of patients grouped into thirds, surgical duration versus level of experience.
Discussion
This study evaluated the learning curve when a single surgeon starting to perform a modified Lapidus procedure performed for hallux valgus correction. From 68 cases over a period of 2 years the data demonstrate that overall surgery duration time decreased from 78.93 minutes at month 0 to 61.80 minutes at 24 months, indicating the presence of a learning curve. In addition, grouping by low (meaning first one third), medium, and high (meaning last one third) experience demonstrated that the peak learning curve is present in the first 1/3 of patients, or in this study the first 23 cases. One possible reason that the learning curve was represented best in the first one third of patients is the switch from screws to staples early in the study period. However, in addition to the improvement between low and medium groups, there was a statically significant improvement between medium and high experience groups as well. Further reinforcing that it may take roughly 23 cases to show a decreased procedure time is that the 3 experience groups contained 23, 23, and 22 patients, respectively. Palmanovich and colleagues evaluated the learning curve for the minimally invasive Chevron akin operation for hallux valgus, and their results were similar to this study. They showed a significant decrease in operating room time over the 3-year time period, with the learning curve plateauing by the 21st patient. 8
This study also evaluated the rates of nonunion as the surgeon increased in experience on a monthly basis and across the low, medium, and high experience groupings. The results showed that the risk of nonunion was not different at any point in the learning curve or among any of the groups, indicating that the surgeon was equally proficient in the initial procedure but became increasingly more efficient with progression through the case steps as going through the learning curve of the procedure. This suggests that there is no greater risk of nonunion if treated at the beginning or the end of the learning curve with an appropriately experienced surgeon.
The preoperative/postoperative IMAs were measured as well to assess the prevalence of the learning curve. The average preoperative IMA was 15.1°, and the average postoperative IMA was 4.9°, yielding an average IMA decrease of 10.2°. These averages were on par with the recent literature, including another modified Lapidus study published by Greeff et al, which reported average pre-/postoperative IMAs of 15° and 5°, respectively. 9 With further analysis of the IMA angles into low, medium, and high experience groups there showed a significant difference in decrease of IMA angles between the low to medium experience groups (P = .048), but not between low to high experience groups (P = .26). The significant results between the low to medium experience groups further reinforces the existence of a learning curve that is overcome by the 23rd patient. However, even though there is a difference between the low to high groups it was not statistically significant. This may also be due to the small sample size and therefore lack of statistical power.
While the learning curve did not have a significant impact on the rate of nonunion, the study did allow us to look at the overall rate of complications and assess the quality of the modified Lapidus procedure. The rate of nonunion in this study (4.41%; 3/68) was higher than two of the reported modified Lapidus procedure studies at 2.2% and 0%.3,10 However, it was still lower than the average nonunion rate of 6.35% as reported by Crowell et al, which assessed 898 hallux valgus correction surgeries. 11 Additionally, this study demonstrated a recurrence rate of 5.88% (4/68; P = .39), which is lower than the reported rates of recurrence of hallux valgus with some other surgical procedures. However, one of the limitations of this study is the short follow-up time of 6 months, and as such, the long-term rate of recurrence is not evaluated.
Our study has several limitations including a relatively small sample size. While the data showed a statistically significant learning curve, a larger sample size would increase the strength of the results including significance of rates of recurrence and decrease in preoperative/postoperative intermetatarsal angles between the levels of varying experience. Additionally, this study focused on the procedures of a single surgeon and, as such, are only analyzing the results of a single surgeon. A multi-surgeon study would make for a more generalizable prediction of the learning curve. As mentioned above, the variation in sample size between screws and staples made any comparison impractical. Additionally, to better assess the rate of recurrence, all patients should have at least a 1-year follow-up. While this study focused primarily on surgery duration as a measure of progress through the learning curve, there are certainly other ways to evaluate a surgeon’s level of improvement with a technique. Further research can evaluate long-term outcomes and patient satisfaction, set-up time, C-arm use, and a more thorough examination of the rate of recurrence. Additionally, a more robust comparison of staples versus screws and the impact on the above variables. A future study using multiple surgeons’ results would also provide a more generalized representation of the learning curve for 3-dimensional hallux valgus correction.
Conclusion
This study supports the existence of a learning curve in a single surgeon using a modified Lapidus procedure for hallux valgus correction. Findings suggest that surgery duration decreases as the surgeon advances through the learning curve, with the initial 23 patients showing the highest rate of decrease in time. Notably, the rate of complications was not significantly changed as the experience of the surgeon increased.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Trial Registration
Not applicable.