
Abstract
Background
Correction of hammertoe deformities at the proximal interphalangeal (PIP) joint results in an inherent loss of motion that can be a concern for active patients who want to maintain toe function and grip strength. Diaphyseal proximal phalangeal shortening osteotomy (DPPSO) is a joint-sparing procedure resecting a cylindrical portion of the proximal phalanx on the middiaphysis.
Patients/Methods
This was a retrospective review including patients treated using DPPSO with at least a 1-year follow-up. Demographic, comorbidity, and Visual Analogue Scale (VAS) scores and complication data were obtained. Radiological assessment included union status and alignment. Medial frontal anatomical (mFAA), frontal proximal interphalangeal (mFIA), plantar lateral anatomical (pLAA), and medial and plantar lateral interphalangeal angles (pLIA) were measured.
Results
A total of 31 patients (45 toes) were included, with a mean age of 59 years (range: 24-72) and follow-up of 35 months (range: 12-60; mean preoperative VAS score was 4.9 ± 1.72 improving to 1.62 ± 2.28; P < .01). Union occurred in all patients at an average of 11.2 weeks. Complications were present on 4 toes (8.8%), with no recurrences. The pLIA significantly changed from 44.9° to 17.9°. There were no significant differences in the preoperative and postoperative values of the mFAA, pLAA, and mFIA.
Conclusions
DPPSO provides adequate pain relief and corrects the PIP joint in the lateral plane without significantly affecting the coronal plane or the anatomical axis of the phalanx in the frontal and lateral views, nor producing secondary deformities. DPPSO is a safe, effective, and reproducible technique with a low complication rate.
Levels of Evidence:
Level IV: Retrospective case series
“Malalignment and recurrent deformity are rare complications, but the inherent loss of PIP motion can be a concern for active patients who want to maintain normal toe grip strength.”
Introduction
Hammertoe and claw toe deformities develop from an imbalance between the static and dynamic stabilizers of the lesser toes, usually producing nonphysiological proximal interphalangeal (PIP) joint flexion and variable metatarsophalangeal (MTP) hyperextension.1,2 Patients commonly complain of pain or discomfort over the dorsal aspect of the PIP joint, resulting in shoe wear restrictions. The surgical management of these deformities is one of the most common procedures performed on forefoot surgery, and it has been reported to improve function and diminish pain.3-10
Multiple techniques have been described to address nonphysiological PIP joint flexion. Currently, flexor-to-extensor tendon transfer, PIP joint arthrodesis or arthroplasty, MTP capsulotomy, and tendon releases are treatment options described in the literature.11-13 Flexor-to-extensor tendon transfer is a procedure usually indicated for flexible hammertoes and involves transferring the FDL tendon to the dorsum of the toe into the extensor mechanism.14-17 Although this technique addresses the imbalance of the stabilizers while maintaining the PIP joint motion, stiffness and recurrent deformity can be significant potential complications.17-19 PIP joint arthrodesis/arthroplasty is indicated for the correction of fixed hammertoe deformities that persist despite aggressive soft-tissue release.4,6,13 Malalignment and recurrent deformity are rare complications, but the inherent loss of PIP motion can be a concern for active patients who want to maintain normal toe grip strength. 20
Diaphyseal proximal phalangeal shortening osteotomy (DPPSO) is a joint-sparing procedure that corrects hammertoes without losing motion or grip strength of the toe. A cylindrical portion of the phalanx on the middiaphysis is resected, the PIP joint is manipulated into a straight position, and a K-wire is placed for stability, thus improving bone contact and alignment without resection or fusion (Figures 1A-1B). This results in improved proximal phalangeal anatomical alignment and preservation of joint motion.
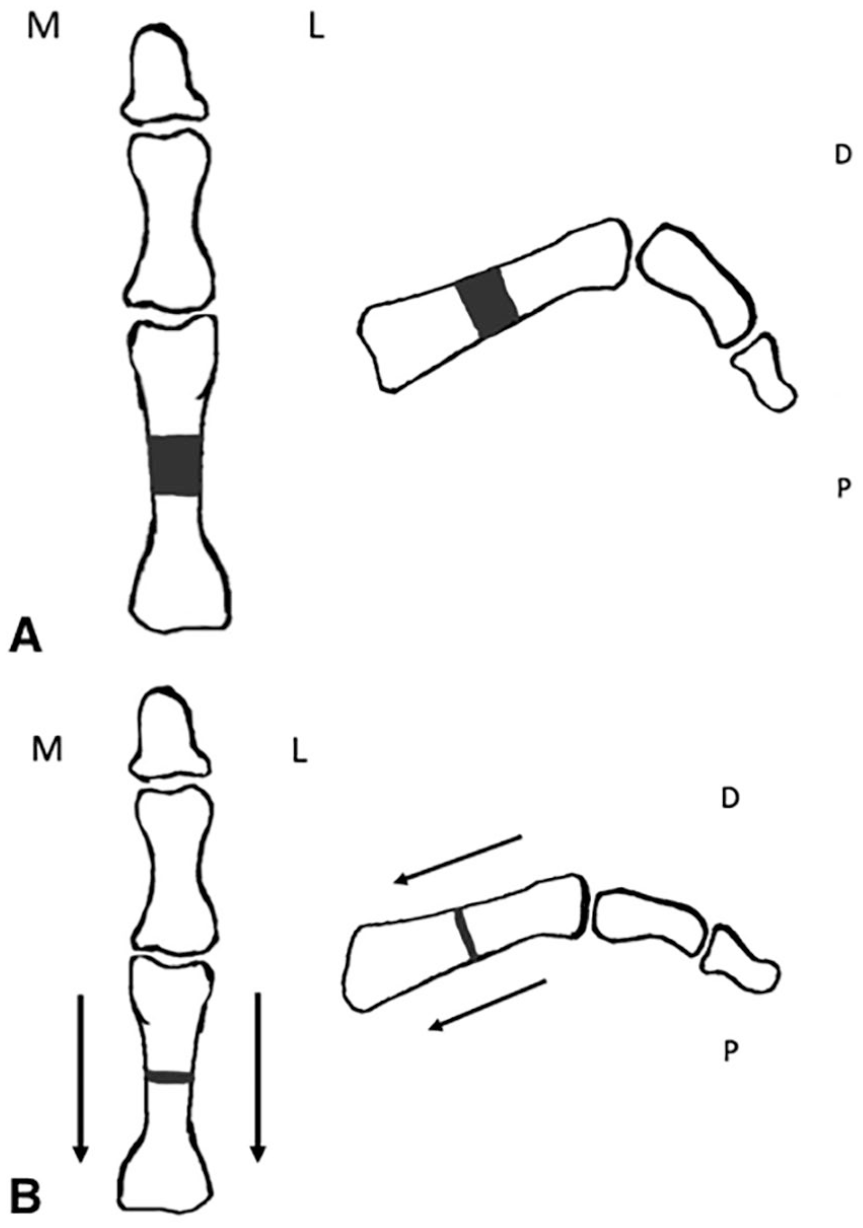
Diaphyseal proximal phalangeal shortening osteotomy: A. A cylindrical portion of the diaphysis is resected. B. Axial shortening of the proximal phalanx reduces the hammertoe deformity.
This retrospective study evaluates the radiological efficacy of this joint-sparing technique for correcting the PIP joint flexion deformity without producing secondary malalignment. It also assesses potential complications of the procedure and its effectiveness in reducing pain.
Methods
Patients who underwent DPPSO for hammertoe deformity between February 2013 and March 2018 with at least a 1-year follow-up were included in this institutional review board–approved retrospective review. All procedures were performed by the senior author in a single academic institution. Indications for DPPSO included all flexible deformities and rigid deformities with flexion contractures of the PIP joint less than 90° and without coronal malalignment. Patients with more severe rigid deformities or degenerative bone loss were treated with a PIP fusion or arthroplasty.
Exclusion criteria included previous surgery on the toe, incomplete radiological follow-up, and the use of other fixation devices different to K-wires. Patients treated with DPPSO for excessive toe length conditions without hammertoe deformity were also excluded from the study.
Surgical Technique
The procedures were done using an ankle block and sedation unless general anesthesia was required for concomitant procedures. A dorsal longitudinal approach to the proximal phalanx was performed followed by blunt dissection to expose the middiaphysis (Figure 2A). The PIP joint was avoided because this may be a factor contributing to secondary toe stiffness postoperatively. The extensor tendon was identified and protected throughout the procedure. A 3-mm cylindrical portion of the middiaphysis was resected using a 5-mm microsagittal saw blade. The osteotomy was made perpendicular to the base of the phalanx in order to avoid secondary dorsiflexion or plantarflexion of the distal segment of the toe (Figures 2B and 2C). Irrigation was dripped on the blade to minimize the generated heat. Caution was taken to use Hohmann retractors around the bone to avoid penetrating the bone and cutting the flexor tendon. Once the segment of bone was removed, we checked that there were no bony spikes that would prevent the osteotomy from closing. At this point, if the PIP could not be manipulated into a straight position, a scalpel was used to release the plantar capsulotomy of the PIP joint and flexor tendon through the dorsal incision. This was performed as follows: After dissecting superficial to the PIP capsule and collateral ligament and while the PIP was maintained in a flexed position to keep the neurovascular bundle plantar to the bone, the blade was introduced alongside the plantar condyle of the proximal phalanx. By following the bone plantarly and distally, the blade transects the capsule and flexor off the middle phalanx. An axial K-wire was used for fixation and maintained for a period of 6 weeks (Figures 2D-2F). The K-wire was positioned into the subchondral plate of the proximal phalanx unless bone quality was poor; in that case, the K-wire was advanced into the metatarsal head.
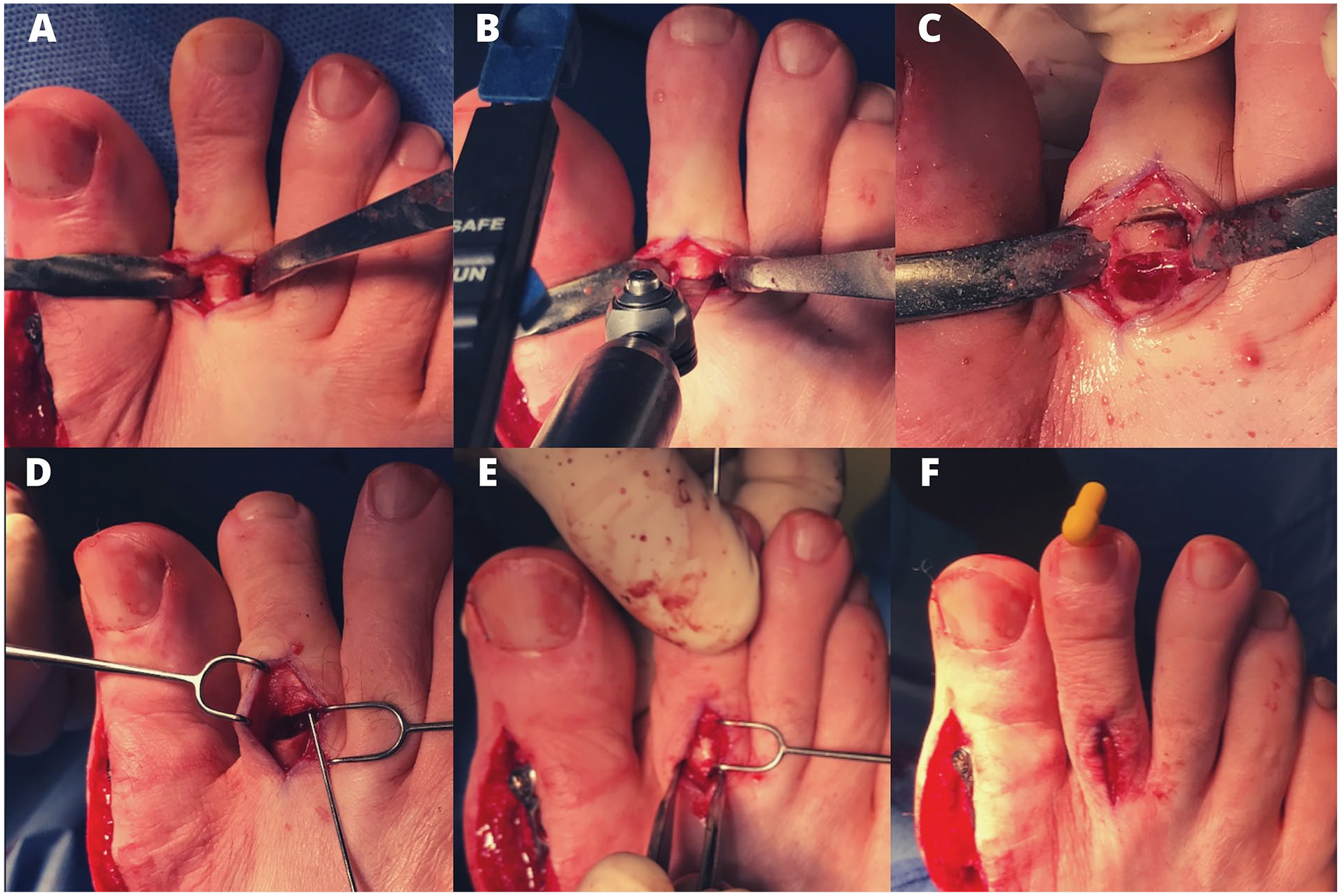
Intraoperative photographs depicting diaphyseal proximal phalangeal shortening osteotomy for hammertoe deformity of the second toe. A. Longitudinal approach and protection of the extensor complex, neurovascular bundle, and flexor tendons using Hohmann retractors. B. Both osteotomies are made perpendicular to the base of the phalanx. C. A 3-mm cylindrical portion of the middiaphysis is resected. D and E. An axial K-wire was used for reduction and fixation. F. Second toe appearance after completion of the procedure.
Radiological assessment was performed preoperatively, at 2 and 6 weeks postoperatively, and at 3 and 6 months postoperatively. Union of the osteotomy site was determined by bridging of at least 3 cortices on the anteroposterior and lateral view. This was determined by radiological review by 2 fellowship-trained foot and ankle surgeons. The preoperative and 6-month postoperative X-rays were analyzed by obtaining 4 different angle measurements following the anatomical and articular axis on the anteroposterior and lateral views (Figures 3A-3D):
Medial frontal anatomical angle (mFAA)
Medial frontal proximal interphalangeal angle (mFIA)
Plantar lateral anatomical angle (pLAA)
Plantar lateral proximal interphalangeal angle (pLIA)
All patients were evaluated preoperatively and at 1 year postoperatively using the Visual Analogue Scale (VAS). Data on demographics, comorbidities, postoperative complications, and secondary procedures were also collected.
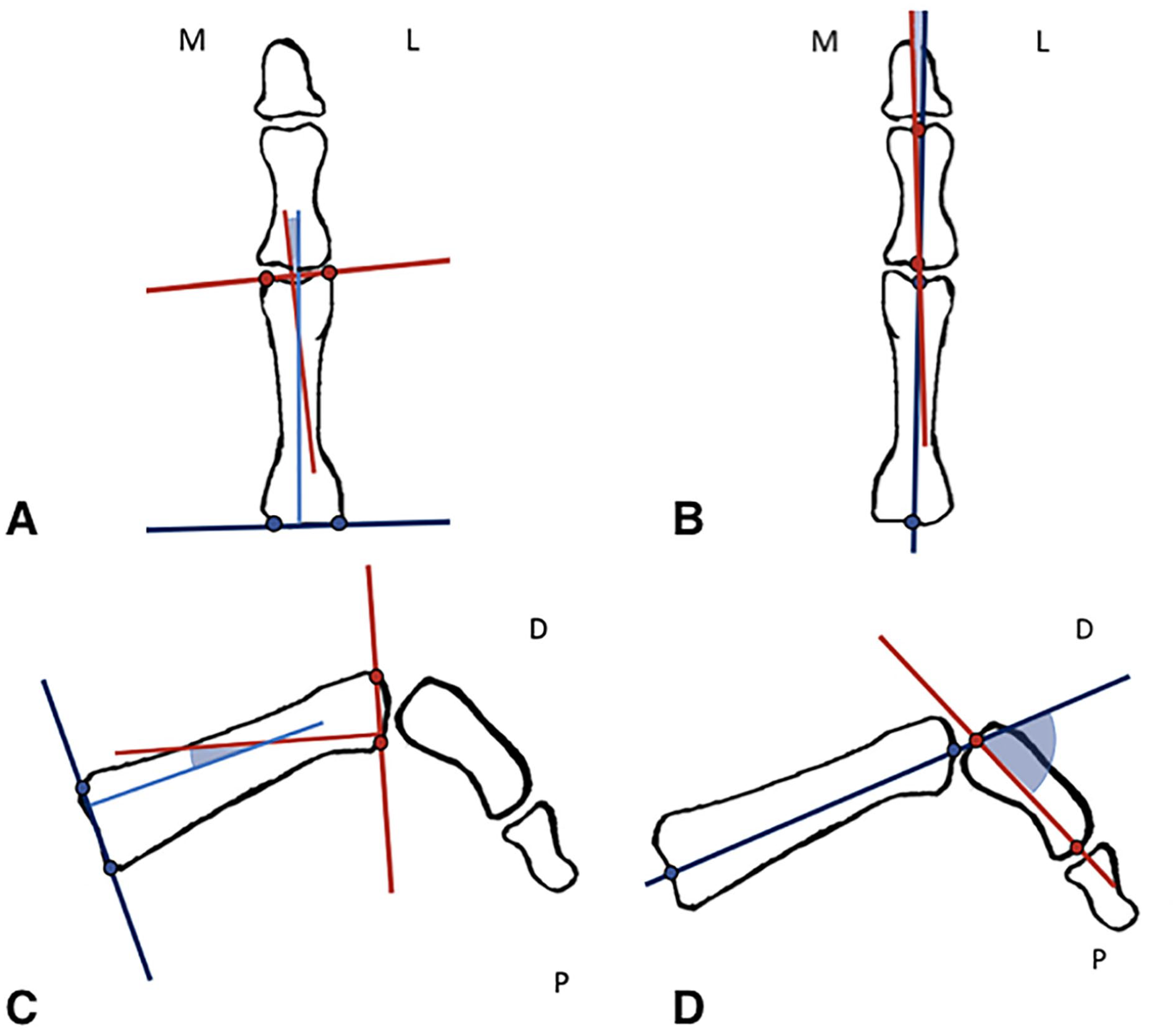
Radiological articular and anatomical angle measurements on anteroposterior (A, B) and lateral views (C, D). A. Medial frontal anatomical angle. B. Medial frontal interphalangeal angle. C. Plantar lateral anatomical angle. D. Plantar lateral proximal interphalangeal angle.
Statistical Analysis
The statistical analysis was performed using the SPSS program (version 23.0; IBM Corp, Armonk, NY). Comparison between preoperative and postoperative radiographic angles and VAS scores was made using the t-test for paired samples. Comparison of fusion times between subpopulations was made using the t-test for independent samples. A P value <.05 was considered for statistical significance.
Results
Demographic Data
A total of 31 patients (28 female and 4 male) were included in the study (Table 1), corresponding to 18 right and 13 left feet. A total of 45 toes met the inclusion criteria, with 31 second toes, 10 third toes, and 4 fourth toes. The mean age was 59 years (range 24-72), and follow-up was 35 months (range 12-60). In all, 29 patients received adjunct procedures, with hallux valgus correction being the most common in 22 patients, followed by Weil osteotomy in 17 patients. Other concomitant procedures included the following: Kramer osteotomy for bunionette (2 patients) and PIP fusion of the fifth toe (1 patient). Systemic comorbidities found in this cohort were as follows: diabetes (2 patients), gout (1 patient), and rheumatoid arthritis (1 patient). In all, 12 patients (39%) were smokers.
Demographic Data.
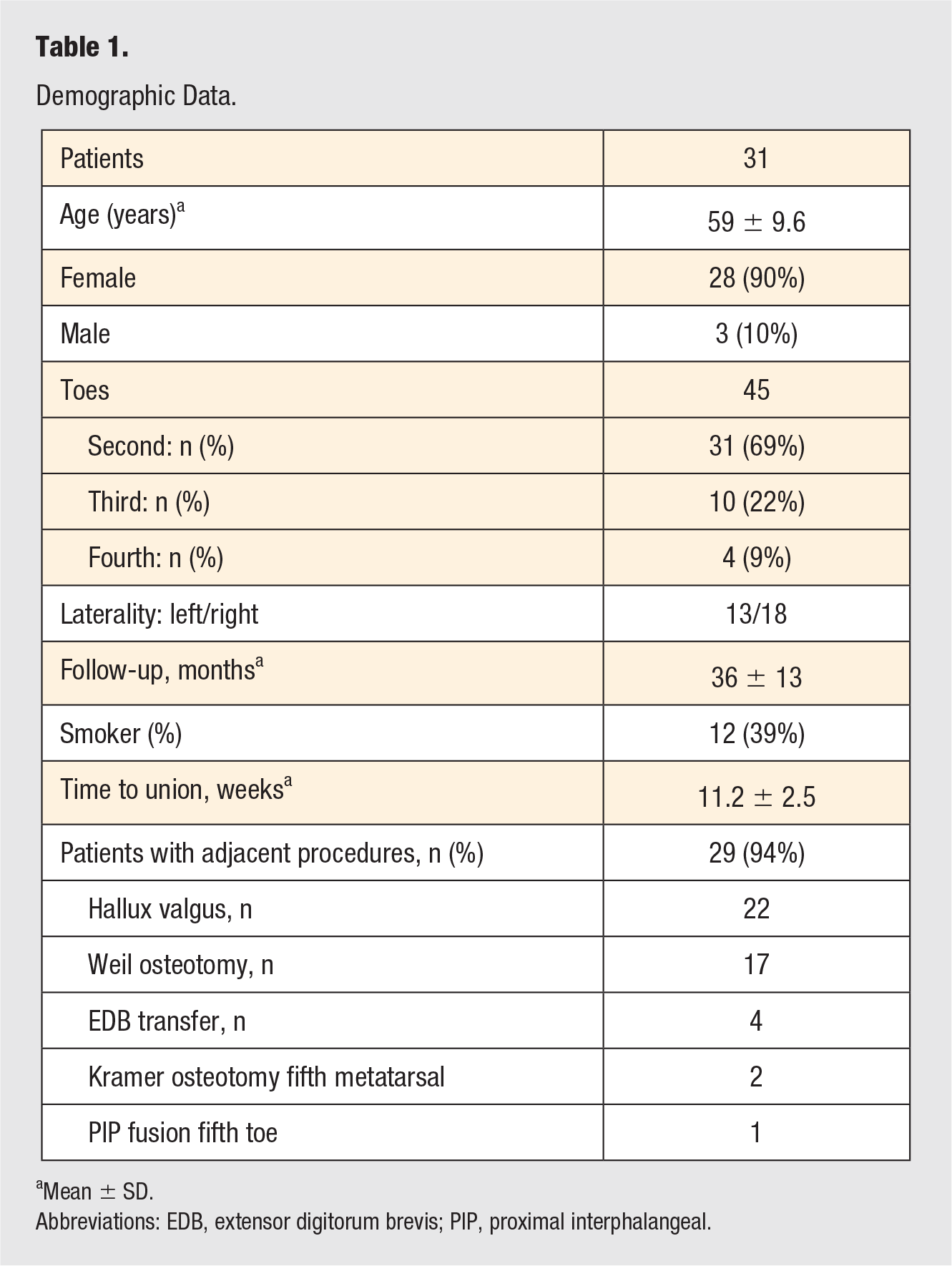
Mean ± SD.
Abbreviations: EDB, extensor digitorum brevis; PIP, proximal interphalangeal.
Union Rates
There were no nonunions, with healing occurring at an average of 11.2 weeks (range 8-19 weeks), determined by healing of 3 cortices on radiographs. Second toes healed on average at 11.3 weeks (range 8-18 weeks), third toes at 11.6 weeks (range 9-19 weeks) and fourth toes at 9.75 weeks (range 7-12 weeks). Two patients presented with delayed healing, with final union at 18 and 19 weeks. Both these patients were smokers. However, there was no statistically significant difference between union times of smokers and those of nonsmokers (P = .85).
Visual Analogue Scale
All patients had decreased pain at the 1-year follow-up. The mean preoperative VAS score was 4.9 ± 1.72, improving significantly to 1.62 ± 2.28 (P < .01).
Complications
Complications were present on 4 toes. Three patients (3 toes) developed superficial infections that were treated with K-wire removal and oral antibiotics, with full resolution of the infection. One patient presented with a floating toe but was sufficiently satisfied and declined revision surgery. There were no recurrences of the hammertoe deformity on this series, based on radiographic follow-up at 1 year.
Radiological Assessment
Radiographic results are summarized in Table 2. The pLIA, representing the hammertoe deformity, was corrected significantly from 44.9° ± 18.9° to 17.9° ± 9.7° (P = .01). There were no significant differences in the preoperative and postoperative values of the mFAA (P = .43), pLAA (P = .24), and mFIA (P = .65).
Overall Preoperative and Postoperative Angle Measurements.
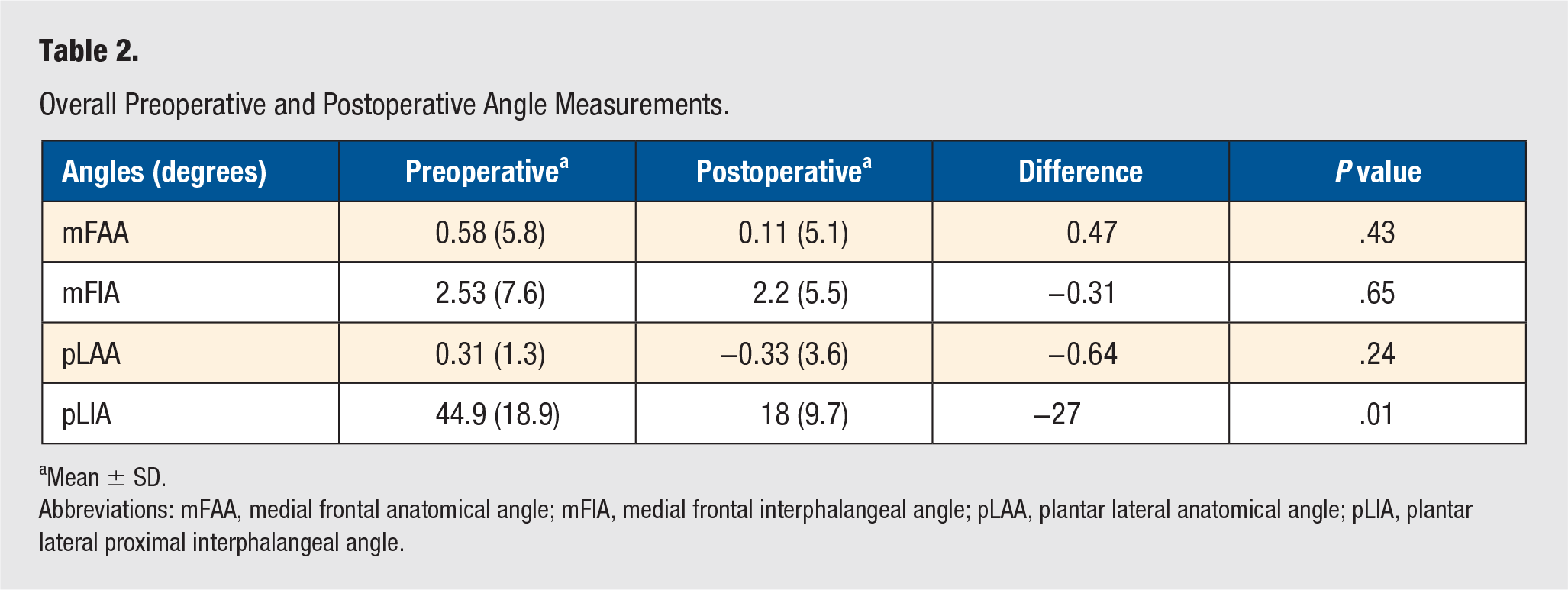
Mean ± SD.
Abbreviations: mFAA, medial frontal anatomical angle; mFIA, medial frontal interphalangeal angle; pLAA, plantar lateral anatomical angle; pLIA, plantar lateral proximal interphalangeal angle.
The same results are found when the analysis is made differentiating by type of toe, except for the fourth toe (Table 3). The pLIA was corrected postoperatively at a mean of 28° but did not change significantly probably because of the limited number of patients undergoing correction of a fourth-toe hammertoe (4 toes).
Preoperative and Postoperative Angle Measurements Individualized by Toe.
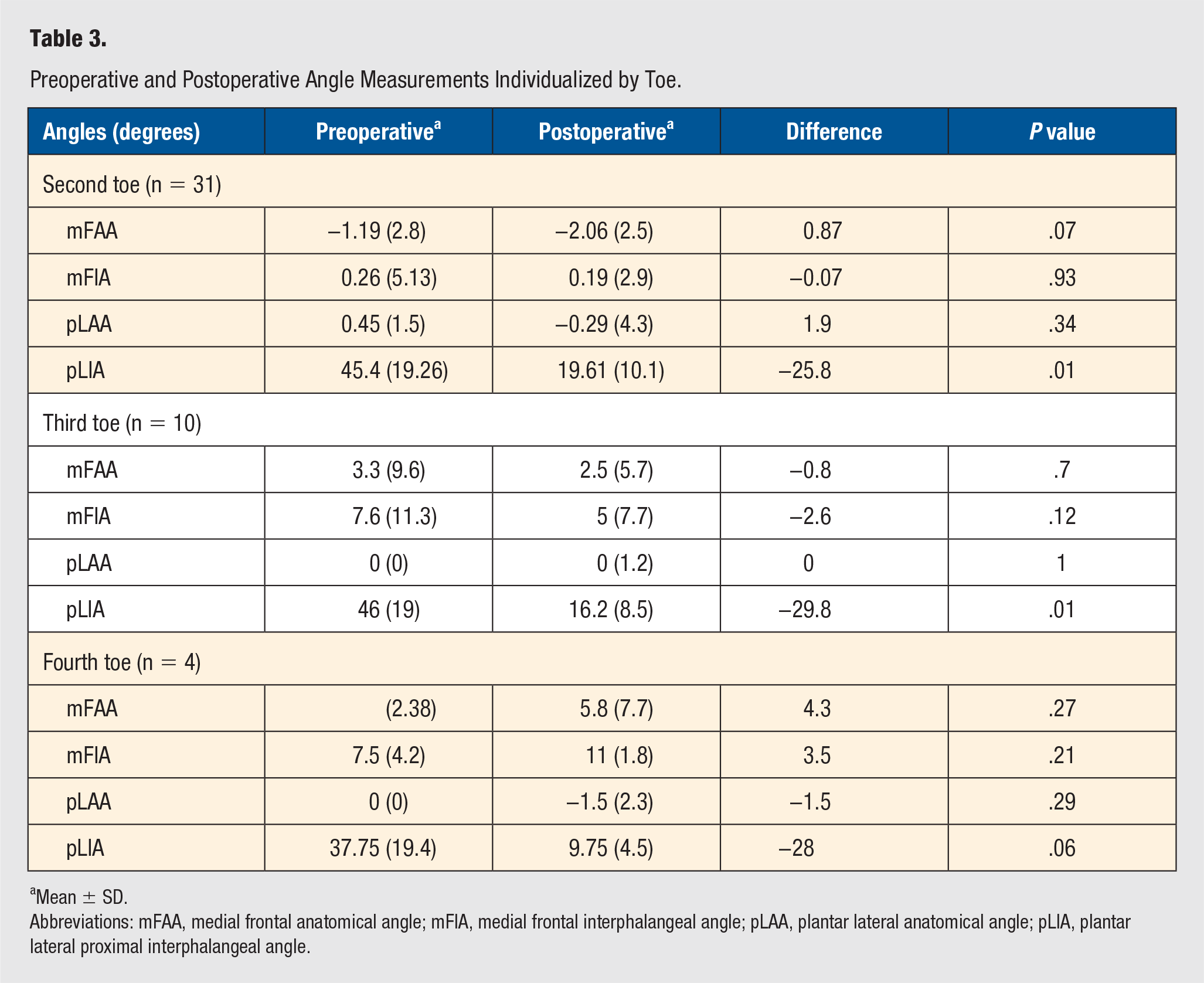
Mean ± SD.
Abbreviations: mFAA, medial frontal anatomical angle; mFIA, medial frontal interphalangeal angle; pLAA, plantar lateral anatomical angle; pLIA, plantar lateral proximal interphalangeal angle.
Discussion
The optimal technique for correcting hammertoe deformities has been a matter of debate and surgeon preference. Many of these procedures are based on the concept of rebalancing the deformation forces, either by tendon transfers or by producing a relative shortening of the toe to relax the extensor and flexor mechanisms, thus correcting the deformity.3,15
PIP fusion or arthroplasty produces shortening of the toe by resecting the distal portion of the proximal phalanx with or without resection of the articular surface of the middle phalanx’s base. 4 This allows the reduction of the flexion contracture directly at the joint level. Multiple reports endorse the use of this strategy for obtaining good and excellent results concerning pain reduction and deformity correction.5,8,12,13,21
Independently of the solid body of evidence concerning hammertoe deformity management and functional results, correction at the PIP joint is not exempt from complications such as hyperextension deformity, floating toe, and malalignment which are strongly related to patient dissatisfaction because of the relation to cosmetic appearance.4,22,23
The contribution of the PIP and distal interphalangeal (DIP) joint hyperextension deformity to floating toe, after PIP joint procedures, has not been well studied. PIP fusion or arthroplasty in the context of a Weil osteotomy has been related to a higher incidence of floating toe. 24 One of the rationales for the advent of joint-sparing procedures for correcting hammertoe deformities is that it can lead to reducing the number of toes that do not contact the ground, even in the setting of a floating toe entirely secondary to a metatarsal osteotomy, the latter by allowing an overall normal appearance through a flexion adaptation of both PIP and DIP joints.
Procedures addressing the proximal phalanx for the treatment of hammertoes were first described by Thretowan 25 in 1925 and followed by Glassman et al 26 in 1945, describing a complete proximal phalangectomy with good functional results in 21 patients (54 toes). Newman and Fitton 27 compared the results of PIP arthrodesis, flexor to extensor transfer, and proximal phalangectomy in 63 patients (136 toes). The phalangectomy group (22 patients) presented 77% of excellent results in comparison to the 46% of the PIP arthrodesis group (58 patients) and 34% in the flexor-to-extensor transfer group (19 patients). The authors concluded that phalangectomy was the most successful procedure and should be considered the procedure of choice.
McConnell 28 in 1975 published one of the earliest reports on proximal phalangeal midshaft resection for the treatment of hammertoes. The author described a “subperiosteal resection of the narrow waist of the phalanx” on 95 patients (466 toes), producing shortening of the toe and relaxation of the soft tissues. All cases but one required K-wire fixation, and the importance of the preservation of the periosteum tube is highlighted to allow the migration of the resected ends of the bone on to each other.
Ceccarini et al 29 proposed a subtraction proximal phalangeal osteotomy at the level of the neck of the phalanx for correcting hammertoe deformity at the level of the PIP joint, reporting excellent clinical and radiological results on 40 patients, with a mean follow-up of 24 months. Functional results were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) score increasing from 28 to 91 points. Radiologically, the procedure corrected the deformity on the sagittal plane reflected on a diminution of the lateral IP angle from 65° to 11° without changes in the coronal plane. Nevertheless, some corrections may have been the result of malunion at the osteotomy site creating a secondary phalangeal deformity and diminishing the effect on the PIP joint. This secondary phalangeal deformity may create a significant malalignment of the toe, resulting in a risk of iatrogenic deformities. These issues were not addressed by the authors, and to our knowledge, there are no other reports in the literature on the subject. In our study, bone resection was performed on the middiaphysis because we believe that performing the osteotomy near the PIP joint can contribute to postoperative rigidity.
In a recent follow-up study, the same group compared a series of 78 patients treated with shortening osteotomy (40 patients) versus PIP arthrodesis (38 patients), with a mean follow-up of 56 months. 20 Functional results were comparable among both techniques using the Foot and Ankle Outcome Score (FAOS) and AOFAS scores, but a shorter recovery was reported on the osteotomy group reflected in a quicker time for bone healing (4.3 vs 5.4 weeks) and K-wire removal (4 vs 5.3 weeks).
In the present study, bone healing times were longer (11.2 weeks), probably because the midshaft of the phalanx is not as well perfused as the metaphyseal bone. However, this did not have an influence on the final results because all our patients healed, with only 2 cases presenting with delayed union. The K-wire was removed in all cases at 6 weeks regardless of union status.
Radiological results of this study were consistent with other series with regard to the efficacy of DPPSO for correction of flexion deformity at the level of the PIP joint without altering coronal joint alignment.6,21,30,31 In our patients, the anatomical axis of the phalanx on both sagittal and coronal planes was maintained significantly after shortening in all patients (Figures 4A-4C). To our knowledge, this is the first study that assesses the anatomical axis component in the correction of hammertoes using phalangeal osteotomies. Furthermore, clinical results were consistent with regard to a diminution of pain, with significant improvement of VAS scores in all patients.

A 36-year-old patient underwent diaphyseal proximal phalangeal shortening osteotomy (DPPSO) for second hammertoe deformity associated with severe hallux valgus. A. Preoperative anteroposterior and lateral weight-bearing X-rays compatible with severe PIP joint deformity of the second toe. B. Immediate postoperative anteroposterior and lateral X-rays after DPPSO and Weil and Ludloff osteotomies. The lateral X-rays show adequate correction of the hammertoe deformity. C. One-year follow-up weight-bearing X-rays compatible with complete healing of the osteotomy site on the proximal phalanx without recurrence of the deformity of the second toe on the lateral X-rays.
The complication rate with this technique was 8% (4/45 toes), which is similar to other reports involving hammertoe correction.8,9,18,22 No revision surgery was performed in this group of patients. Our complications can be classified as minor because 3 of the patients presented with simple superficial infections that were resolved with oral antibiotics, and 1 patient presented with a floating toe that was asymptomatic.
Limitations of this study are its retrospective nature and the lack of objective functional outcomes. However, in most patients, DPPSO was performed in conjunction with hallux valgus correction (22 patients) or Weil osteotomies (17 patients), thus making it difficult to avoid the adjunct procedure influence in the functional outcome and evaluate the hammertoe correction by itself. Other limitations can be identified in the accuracy of radiological measurements of the sagittal alignment, especially concerning the overlapping from the other rays. This complexity has been recognized and acknowledged in other similar studies.6,7,21
Future studies should focus on comparing joint-sparing techniques such as DPPSO with PIP fusion or arthroplasty procedures, especially in terms of range of motion and toe grip strength in order to optimize patient satisfaction.
Conclusions
DPPSO is a joint-sparing procedure that diminishes pain and has a corrective effect on the PIP joint on the sagittal plane, significantly reducing the pLIA and, therefore, the hammertoe deformity. DPPSO has no significant effect on the PIP joint in the coronal plane and on the anatomical axis of the proximal phalanx in the frontal and lateral views, thus neither producing secondary bone deformities, nor malalignment of the toe in this group of patients.
The results support our contention that DPPSO is a safe, effective, and reproducible procedure, with a low rate of complications at a minimum of 1 year of follow-up. Future studies should delve into comparing functional outcomes of DPPSO and PIP arthroplasty or arthrodesis, especially concerning the effect on toe grip strength and floor contact of the toe.
Footnotes
Acknowledgements
The authors would like to acknowledge Javiera Jofre MD for the illustrations contained on this investigation.
Authors’ Note
This study was presented at the 2018 AOFAS Annual Meeting at Boston, MA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GFB, KS, and JO have nothing to disclose. LS reports other support from Zimmer Biomet, grants and other from Arthrex, grants and other from Wright Medical, grants from Bioventus, grants from Omega, grants from Smith Nephew, other from Carestream, other from Elsevier, other from MiRus, other from Tetrix, other from Gerson Lehrman Group, other from Guidepoint Global, and other from Additive Orthopaedics, outside the submitted work; In addition, LS has a patent TM ankle replacement by Zimmer with royalties paid, a patent ProStop implant by Arthrex with royalties paid, a patent Toe guard, night splint Darco with royalties paid, a patent Airlift Ankle Brace DJO with royalties paid, a patent Wave plate by Wright Medical with royalties paid, and a patent Prosthetic Hindfoot Replacement issued.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study has IRB aproval.
Informed Consent
All patients signed informed consent.
Trial Registration
Not applicable, because this article does not contain any clinical trials.