
Abstract
Aims. This study presents the first report of clinical and radiographic outcomes of the Infinity Total Ankle System (Wright Medical, Memphis, TN) with minimum 2-year follow-up. Patients and Methods. The first 67 consecutive patients who underwent primary total ankle arthroplasty (TAA) with the Infinity system at 2 North American sites between August 2013 and May 2015 were reviewed in a prospective, observational study. Demographic, radiographic, and functional outcome data were collected preoperatively, at 6 to 12 months postoperatively, and annually thereafter. Results. The overall implant survival rate was 97% (65 of 67 implants) at a mean follow-up of 35.4 months (27 to 47 months). Two cases underwent talar component revision for aseptic loosening. Six of the 67 cases (9%) required a nonrevision reoperation. Mean Foot Function Index and Ankle Osteoarthritis Scale scores at latest follow-up improved from preoperative by 21.6 (P < .0001) and 34.0 (P < .0001), respectively. No radiographic loosening of any talar or tibial components was identified in the 65 nonrevised cases. Conclusion. Early clinical and radiographic outcomes with the Infinity TAA are promising and compare favorably to those reported for both fixed- and mobile-bearing third-generation TAA designs, even when used in cases with deformity and increased case complexity.
Keywords
“The majority of TAA [total ankle arthroplasty] implants used in the United States incorporate a 2-component, fixed-bearing design.”
The use of total ankle arthroplasty (TAA) in the treatment of end-stage ankle arthritis (ESAA) is increasing in the United States1,2 and the United Kingdom. 3 This trend correlates with the emergence of data that demonstrate that TAA leads to significant improvements in function and pain relief 4 and, in comparison to ankle arthrodesis, is better at meeting patient expectations, 5 results in biomechanical function and gait that more closely resemble normal,6,7 and potentially may reduce the risk of adjacent hindfoot joint degeneration. 8
The majority of TAA implants used in the United States incorporate a 2-component, fixed-bearing design. 9 The use of 2-component designs outside of the United States has begun to increase, 3 with data showing equivalent or improved results as compared to 3-component mobile bearing designs.10,11 The increasing interest in 2-component designs and the increased use of TAA overall has led to the development of a new generation of 2-component TAA implants. The Infinity Total Ankle System (Wright Medical, Memphis, Tennessee) was first implanted in the United States in 2013, with general availability beginning in mid-2014. The design rationale and technique for this TAA system have been described 12 along with a radiographic analysis at minimum 3-month follow-up for a small case series. 13 However, despite now being the most commonly used TAA in the United Kingdom, 3 there have been no published clinical outcome studies for the Infinity Total Ankle System to date.
This study presents the first report on the clinical and radiographic outcomes of 67 patients who underwent TAA with the Infinity Total Ankle System with a minimum of 2-year follow-up.
Patients and Methods
Study Population
A prospective, observational study was performed to assess all consecutive patients who underwent primary TAA with the Infinity Total Ankle System at 2 large subspecialty foot and ankle training sites in North America. The first cases at both Site A and Site B were performed in August 2013. All subsequent, consecutive cases performed prior to June 2015 at both sites were included in the study. All cases had a minimum 2-year follow-up. No cases were excluded.
All study patients had a diagnosis of ESAA, were 30 years of age or older, could provide informed consent, and were deemed appropriate for a low-profile, primary TAA based on surgeon assessment. Patients undergoing primary TAA with severe deformity (talar tilt greater than 20°) or insufficient bone stock (as judged by the treating surgeon), or patients undergoing revision TAA were managed with a stemmed TAA device and were not included in this study.
This study was approved by each institution’s research ethics board.
Surgical Technique
The operative technique utilized standard instrumentation as previously described 12 until computed tomography (CT) scan-derived, patient-specific instrumentation (PSI; Prophecy, Wright Medical Technology, Memphis, TN) became available in 2014. Thereafter, PSI was used for all cases, apart from 2 cases in which insurance approval for PSI could not be obtained. The standard PSI operative technique was utilized, and this has been described elsewhere. 13 Cement fixation was used in one case due to poor-quality bone stock. Additional procedures were performed as required to achieve a stable ankle joint and plantigrade foot. All procedures were performed by orthopaedic surgeons with subspecialty foot and ankle fellowship training.
Data Collection
All data were collected and recorded prospectively. Patient demographics, comorbidities, ESAA etiology, and Canadian Orthopaedic Foot and Ankle Society (COFAS) preoperative arthritis type 14 were collected preoperatively. Operative details including implant size and additional procedures performed were collected at the time of surgery. Clinical outcome was assessed with patient-reported outcome (PRO) measures, including the Ankle Osteoarthritis Scale (AOS), 15 the Foot Function Index (FFI), 16 and the Short Form (SF)-36 Standard Version 2.0 Health Survey Physical Component Summary (PCS). 17 At Site A, the AOS, FFI, and SF-36 PCS were collected preoperatively and at 6 to 12 months postoperatively, and then annually thereafter. At Site B, clinical outcomes were collected postoperatively, at 6 to 12 months, and then annually utilizing only the FFI. Reoperation and revision data were collected prospectively using the COFAS Reoperations Coding System. 18 Standing ankle radiographs were obtained preoperatively and at 2 postoperative time points: early (less than 12 months) and late (greater than 24 months). Radiographs were reviewed by 2 independent observers utilizing previously published measurement techniques.19-22 Radiographic loosening was identified using the criteria of Hintermann et al. 23
Statistical Analysis
The changes in AOS, FFI, and radiographic parameters between preoperative and latest follow-up were evaluated with an unpaired Student’s t test. A P value <.05 was considered statistically significant.
Results
Study Population Demographics and Characteristics
Between August 2013 and May 2015, 67 ankles in 67 patients underwent TAA with the Infinity Total Ankle System. The study population characteristics are shown in Table 1. One patient died at 20 months postoperatively due to causes unrelated to the TAA and is included only in early postoperative outcomes.
Patient Preoperative Demographics and Characteristics.
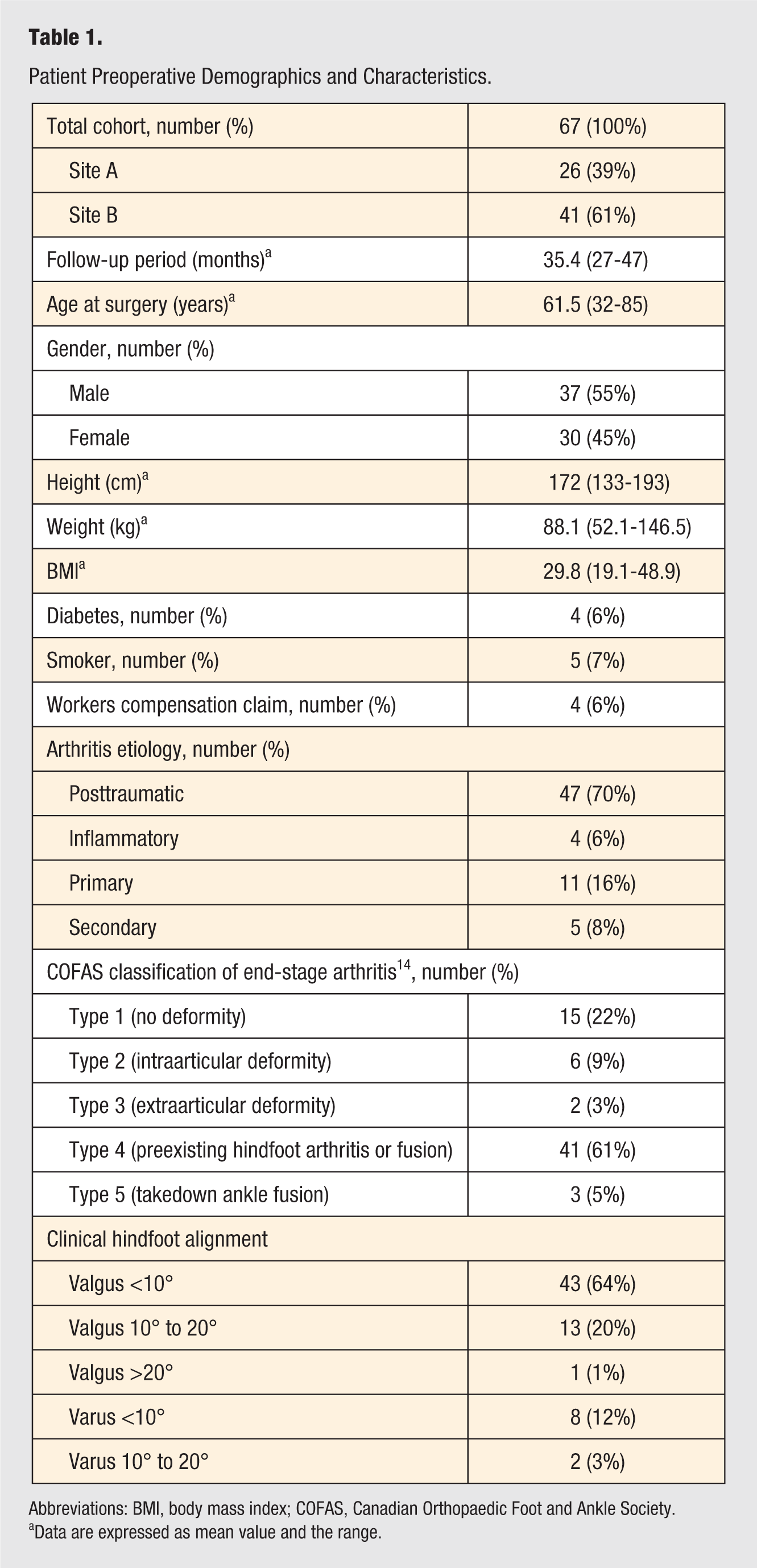
Abbreviations: BMI, body mass index; COFAS, Canadian Orthopaedic Foot and Ankle Society.
Data are expressed as mean value and the range.
Operative Details
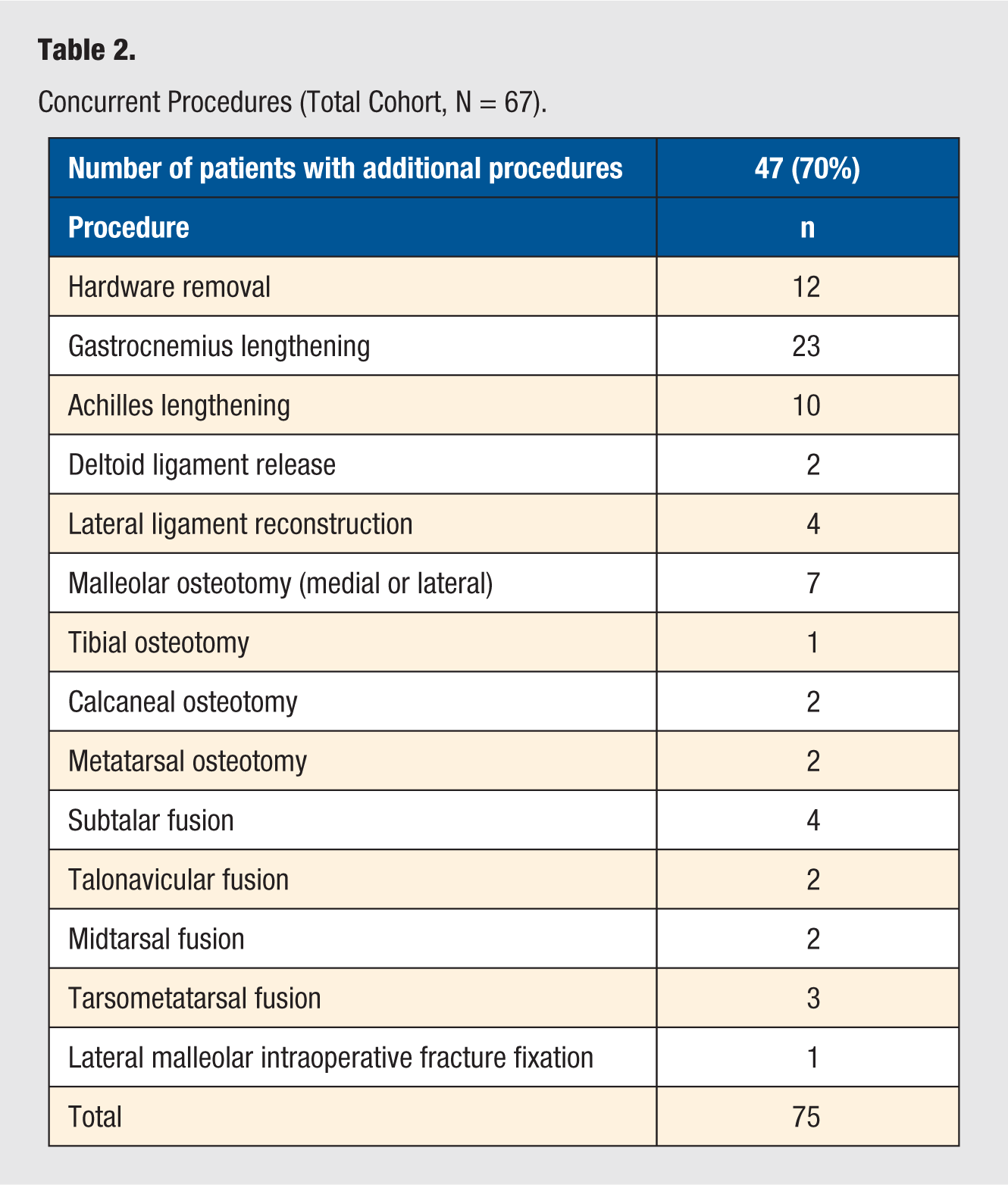
The first 6 cases and 2 later cases at Site A and the first 8 cases at Site B were performed with the standard instrumentation. The remaining 51 (76%) cases were performed with PSI. Twenty cases (30%) had no additional procedures. In the remaining 47 cases (70%), 75 additional procedures were performed. Of the 47 cases with additional procedures, 24 cases had only isolated Achilles lengthening (gastrocnemius in 18 cases; tendon in 6 cases) although 7 of these 24 cases also underwent removal of hardware. The 23 (34%) remaining cases underwent a total of 44 more extensive additional procedures, as outlined in Table 2. The COFAS Postoperative Ankle Arthritis Classification was used to categorize the total procedure complexity. 24 There were 22 Type 1 cases (no concurrent procedures other than hardware removal), 27 Type 2 cases (concurrent soft-tissue procedure(s) requiring a second incision, such as Achilles lengthening, lateral ligament reconstruction), 8 Type 3 cases (concurrent or staged midfoot arthrodesis or osteotomies of fibular, calcaneus, tibia, or midfoot), 7 Type 4 cases (concurrent or staged hindfoot arthrodesis, such as subtalar, talonavicular, triple, or calcaneocuboid), and 3 Type 5 takedowns of ankle fusion.
Concurrent Procedures (Total Cohort, N = 67).
An Infinity tibial component was used in all cases, while an Infinity talar component was used in 59 cases (Figure 1). An InBone II (Wright Medical, Memphis, Tennessee) talar component, a stemmed flat-cut design that is an optional component in the Infinity Total Ankle System, was used in 8 cases to manage a flat top talus (Figure 2).
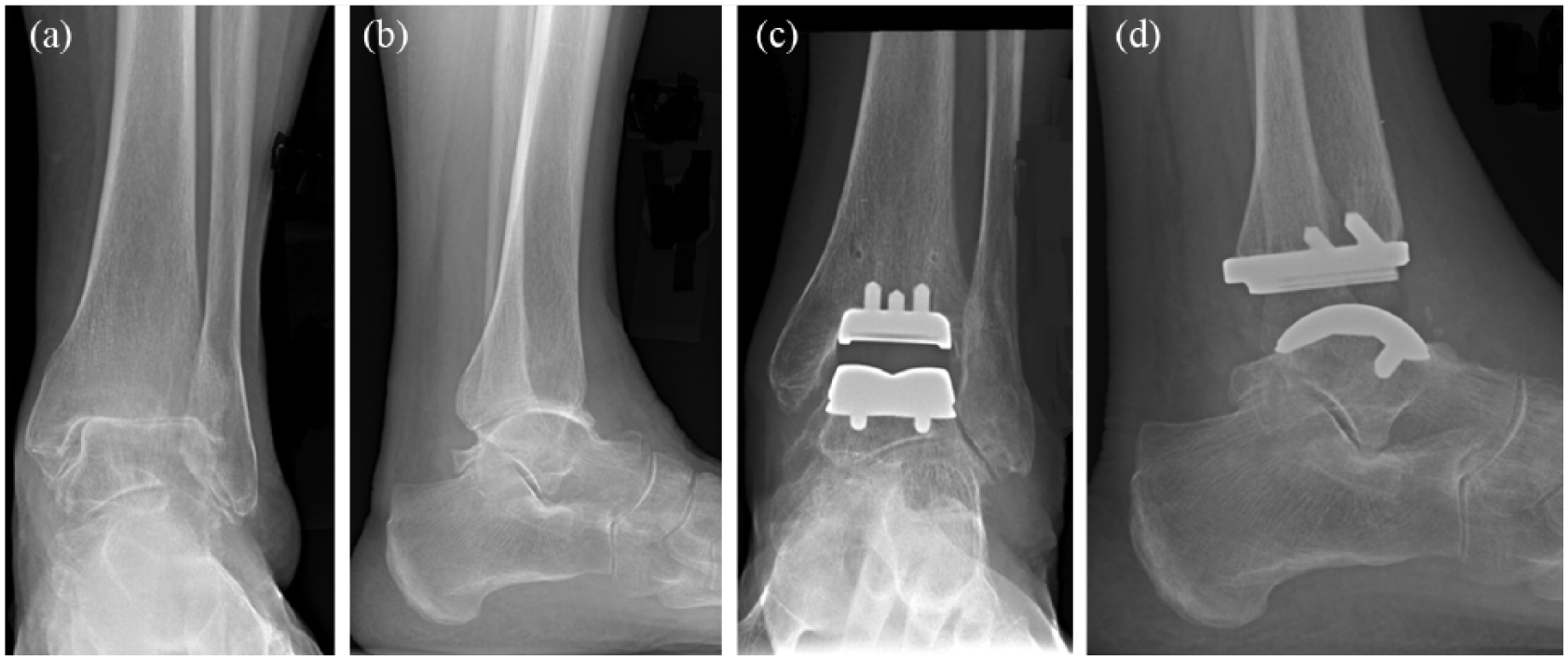
Preoperative AP (a) and lateral (b) radiographs demonstrate a well-aligned ankle with end-stage arthritis. AP (c) and lateral (d) radiographs at 2 years postoperative demonstrating Infinity tibial and talar components with no complications.
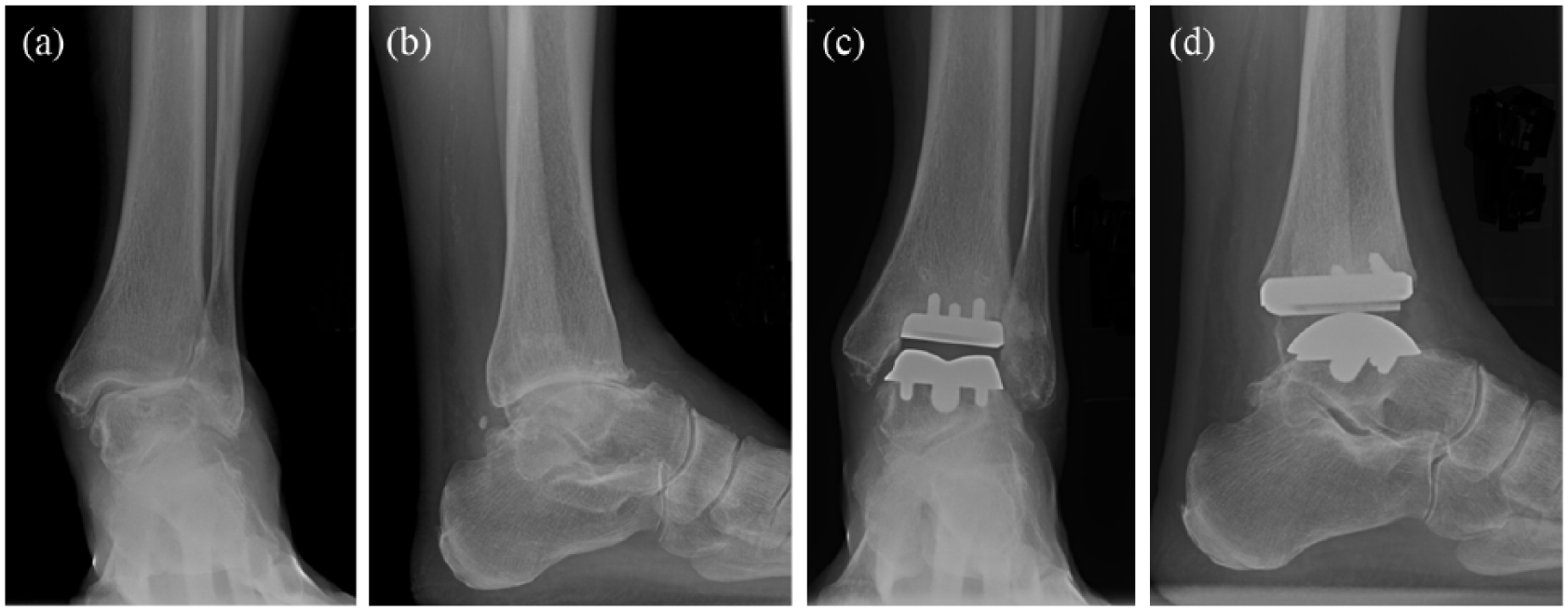
Preoperative AP (a) and lateral (b) radiographs demonstrate end-stage ankle arthritis with 14° valgus talar tilt and a flat top talus. Postoperative AP (c) and lateral (d) radiographs demonstrate insertion of an Infinity tibial component and InBone II talar component with correction to neutral talar tilt.
Reoperations and Revision
Reoperations are summarized in Table 3. Revision of metal components was performed for aseptic loosening and persistent pain in 2 cases (3%). The first case showed subtle lucency at the posterior aspect of the talar component only on CT scan, but no change in component position. Talar component loosening was identified intraoperatively, though the tibial component remained well fixed. Isolated talar component revision with an InBone II talar component was performed at 24 months postoperatively.
COFAS Reoperation and Revision Coding 18 .
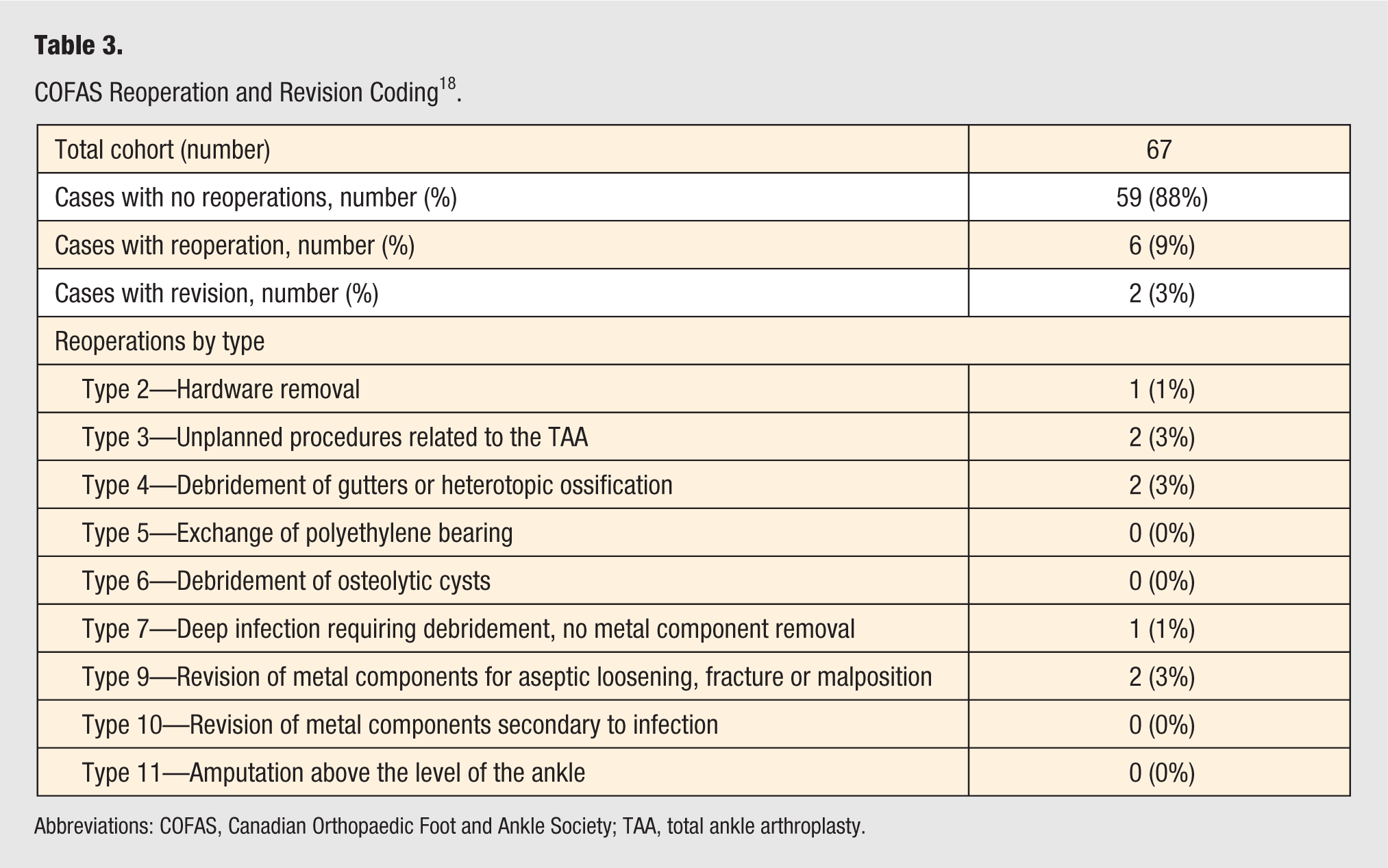
Abbreviations: COFAS, Canadian Orthopaedic Foot and Ankle Society; TAA, total ankle arthroplasty.
In the second case, the tibial component was seen to subside into dorsiflexion by 7° on radiographs, and CT scan demonstrated subtle osteolysis adjacent to both the talar and tibial components. Intraoperatively both the talar and tibial components were found to be loose and were revised with InBone II tibial and talar components at 22 months postoperatively.
Reoperation for gutter debridement was performed in 2 cases at 17 and 19 months postoperatively for persistent pain and radiographic evidence of mild bony hypertrophy in the medial gutter.
Clinical Outcome Measures
The AOS, FFI, and SF-36 PCS early and late postoperative scores all showed significant improvement compared to the preoperative scores (Table 4). The FFI score improved from early- to late-postoperative follow-up by 8.7 (P = .027).
Clinical Outcome Data.
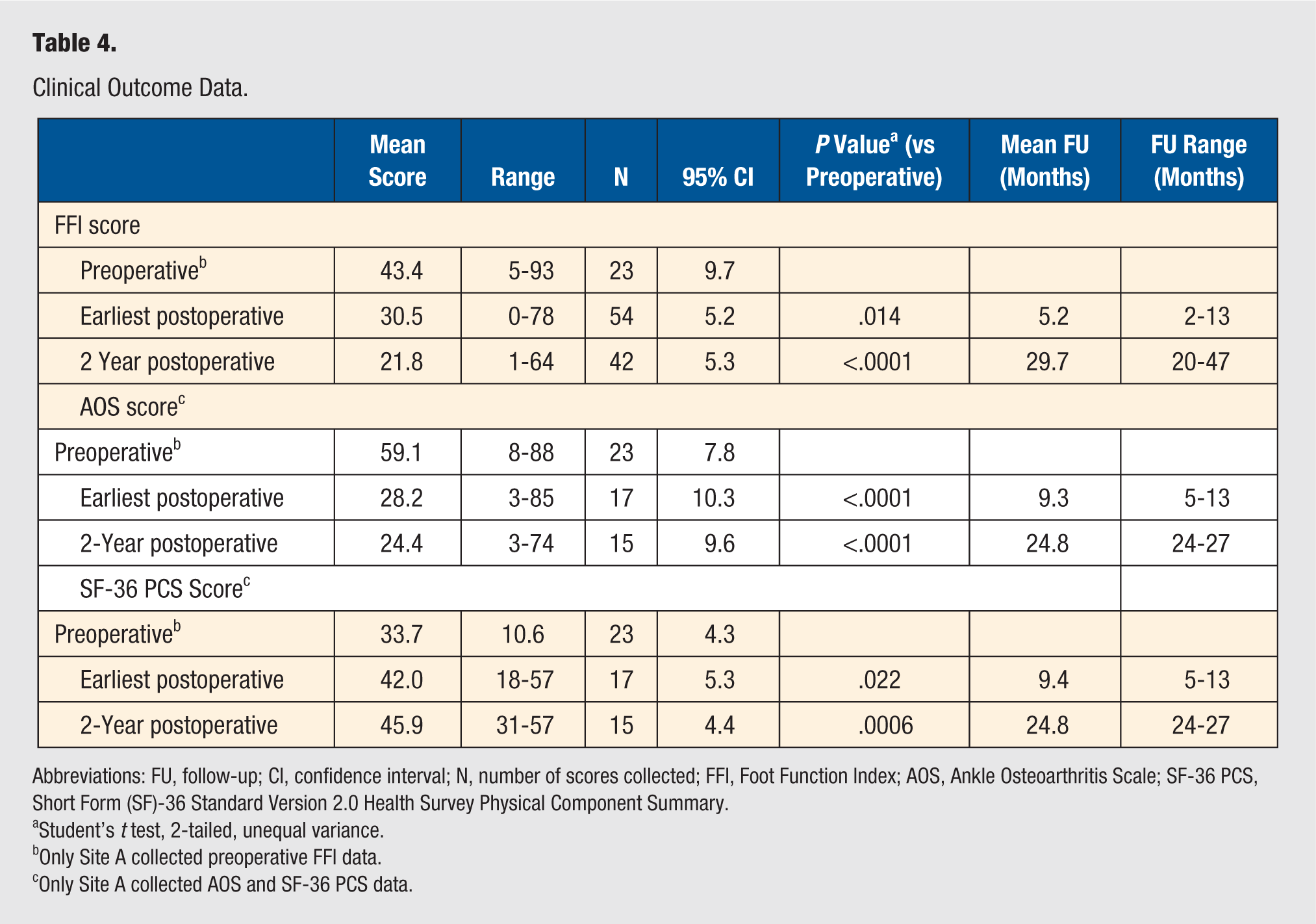
Abbreviations: FU, follow-up; CI, confidence interval; N, number of scores collected; FFI, Foot Function Index; AOS, Ankle Osteoarthritis Scale; SF-36 PCS, Short Form (SF)-36 Standard Version 2.0 Health Survey Physical Component Summary.
Student’s t test, 2-tailed, unequal variance.
Only Site A collected preoperative FFI data.
Only Site A collected AOS and SF-36 PCS data.
Radiographic Outcomes
Preoperative radiographs and early postoperative radiographs (mean 6 months postoperative, SD = 5.8, range 2-11) were available for all 67 cases, while subsequent late postoperative radiographs (mean 29.4 months, SD = 8.2, range 13-47) were available for 46 cases. Preoperative radiographs showed talar tilt of 20° varus to 14° valgus and tibial plafond angles ranging from 13° varus to 17° valgus. Utilizing the radiograph-based criteria of Hintermann et al (tibial component loosening: greater than 2° or 2-mm change in position; talar component loosening: greater than 5° or 5-mm change in position), 23 no radiographic loosening of any talar or tibial components was identified, apart from the case that underwent revision of both metal components.
Discussion
Historically, the primary concerns with TAA were high early rates of revision and reoperation. As a result, gaining an early understanding of these outcomes is paramount in the assessment of any new TAA design. Short-term (less than 4 years of follow-up) revision rates of 4% to 15% for current third-generation implants23,25-28 set the minimal goal for any new fourth-generation TAA system. In view of this, the revision rate of 3% (2 cases) at 27 to 47 months in this study is encouraging. In the first revision case, malposition of the talar component in excessive plantarflexion may have contributed to early loosening. To address this, we began taking an intraoperative fluoroscopic image just prior to making the initial talar resection to confirm good positioning of the resection guide. In the second case where revision of both the talar and tibial components was performed, no initial malalignment was present. Both cases were revised with good outcomes.
This study identified a 9% rate of nonrevision reoperation. In comparison to the rates of 12% to 20% seen in the early experience with some other systems25,29 and for TAA in general, 18 these results are encouraging.
Some of the high rates of failure seen with early TAA designs were attributed to a steep learning curve. 30 In view of this, a goal for any new TAA design should be to incorporate techniques and instruments that aim to reduce the learning curve and enhance ease of use, as third-generation designs may have done over prior designs. 31 The low revision and reoperation rates seen in this study suggest this may be a possibility, potentially due to the use of CT scan–derived PSI in 76% of these cases, since such instrumentation has been shown to have high rates of accuracy and time efficiency.13,32,33 Indeed, only 1 revision case and 4 cases with nonrevision reoperations occurred in the 51 cases with PSI. Nevertheless, even in the 16 cases with standard instrumentation, which represent the earliest part of the learning curve as well as the cases with the longest follow-up, only 1 case went on to revision and 2 to nonrevision reoperations. This suggests PSI is not the only factor contributing to the low failure rate and minimization of learning curve effects seen in this study.
Determining the efficacy of a new TAA design in achieving a patient’s desired outcomes of reduced pain and increased function is equally important as implant durability. In this study, the mean PRO scores (AOS, FFI, SF-36 PCS) improved postoperatively, and the mean AOS score at latest follow-up of 25.1 compares favorably to the mean score of 26.4 published in a large prospective, multicenter study of 281 TAA cases utilizing a variety of TAA systems. 4 These findings offer some early reassurance that the Infinity Total Ankle System may offer not only reasonable durability but also reasonable efficacy in the treatment of ESAA.
The etiology of ESAA in this study was seen to be comparable to that commonly reported, with 70% posttraumatic arthritis in origin. 34 However, the 61% rate of COFAS Type 4 and 4% rate of COFAS Type 5 cases are relatively high 14 and, coupled with a wide range of preoperative coronal plane deformities, suggest the study cohort was composed of a moderately complex case mix. This degree of deformity and complexity likely contributed to the somewhat high rate (51 of 67 cases; 76%) of concomitant procedures seen in this series.5,35 The ability to utilize the Infinity prosthesis in cases of this complexity during our initial experience with the system while achieving the low rate of revision and reoperation identified is encouraging.
One of the strengths of this study stems from the relatively long follow-up period (mean 35.4 months) for the initial presentation of results of a new design as compared to the minimum follow-up periods of 6 or 12 months reported in other initial series.29,36 Overall, however, the results are short term, thereby limiting the strength of the study. An additional strength is the relatively large study cohort of 67 cases in comparison to many other initial device reports.29,37-40
The study is limited by the availability of preoperative PRO scores in only 39% of the cases. In addition, objective range-of-motion data were not available, nor objective physical ability measures (eg, gait analysis). Future studies will need to include these parameters. This study also has a limited range of radiographic outcomes, although this will be addressed in future work that is already underway to couple CT scan and radiographic findings for this cohort. Last, 3 of the authors are co-inventors of the Infinity Total Ankle System (Wright Medical, Memphis, Tennessee), potentially contributing to bias and reduced generalizability of the results due to a greater familiarity with the system than standard users may have during their early experience with the system.
In conclusion, early clinical and radiographic outcomes for the Infinity Total Ankle System appear promising and compare favorably to early outcomes reported for both fixed-bearing and mobile-bearing third-generation TAA designs, even when used in cases with deformity and increased case complexity. Further future study with larger cohorts, longer-term outcomes, and more detailed radiographic and functional data are needed.
Footnotes
Acknowledgements
The authors wish to thank the following for their contributions of data collection: Biraj Bora, Research Coordinator, and the Foot and Ankle Research Staff, St. Paul’s Hospital, Vancouver, Canada; and Amy Roznowski, Research Coordinator, OrthoCarolina, Charlotte, North Carolina.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The following are co-inventors of the Infinity TAA system and additionally report consulting fees from Wright Medical: Murray Penner; W. Hodges Davis; and Robert B. Anderson. Kevin Wing is a consultant for Wright Medical.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by Wright Medical, the manufacturer of the total ankle arthroplasty system that is the subject of this report.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Trial Registration
Not applicable.