
Abstract
Keywords
Introduction
Türkiye's population is aging rapidly, with adults aged 65 and older increasing from 6.7% in 2000 to 9.5% in 2020. This figure is expected to reach 12.9% by 2030 and 25.6% by 2080 (Ministry of Family and Social Services, Republic of Turkey, 2021; TURKSTAT, 2024). Traditionally, older adults have been cared for by family members at home, reflecting cultural norms of intergenerational support in Türkiye (Aysan & Aysan, 2016). However, urbanization, industrialization, and shifting family dynamics have led to a growing demand for formal long-term care (LTC) services (Guduk & Ankara, 2022). Despite this need, Türkiye lacks a regulated LTC system.
Other than aging in place, two main residential care models exist in Türkiye. The less common type is elderly living homes—small group residences with light supervision and visiting professionals—of which Türkiye had only 41 in 2016 (Türkiye Ministry of Family and Social Policies, 2017). The more common type, which is the subject of our study, are Nursing Homes and Elderly Care Centers, which provide accommodation (rooms for one to four people), personal care, health and psychological services, rehabilitation, and social activities for adults aged 60 and older (Ministry of Family and Social Services, Republic of Turkey, 2021; Türkiye Ministry of Family and Social Policies, 2017).
In Türkiye, there are 441 registered nursing homes, including 267 private, 153 public, and 21 nonprofit institutions (General Directorate of Services for Persons with Disabilities and The Elderly, 2021). These facilities generally operate as congregate care settings that offer assistance with everyday tasks rather than provide intensive medical care. Additionally, some nursing homes provide adult daycare services, whereby older adults receive care and participate in social activities during the day before returning to their homes in the evening. These facilities thus function as a hybrid model, combining elements of both assisted living and congregate care settings and traditional nursing homes.
Long-term care facilities in Türkiye operate under both public and private ownership using buildings that may be adapted from previous uses or specifically constructed for care. The main regulation governing nursing homes in Türkiye, whether new builds or conversions, is issued by the Ministry of Family and Social Services (Resmi Gazete, 2009). It outlines requirements for fire safety, traffic safety, and functional spaces. While it states that general areas such as kitchens and lounges must allow for comfortable movement, it does not specify minimum dimensions in every respect. Exceptions include bedrooms, which must be at least 12 m2 for one person and 18 m2 for two, with a maximum of four residents per room. The minimum bed size (90 × 190 cm) and ceiling height (270 cm) are also clearly defined. The lack of clear design standards for every aspect makes it difficult to ensure consistent quality across settings (Ministry of Family and Social Services, Republic of Turkey, 2021).
In Türkiye, older adults choose to live in nursing homes for a variety of interrelated reasons, combining personal needs, family dynamics, cultural shifts, and availability of services in these institutions. A recurring reason is the difficulty in meeting one's own needs due to physical limitations, health problems, or the absence of nearby social support (İnce, 2024; Taş et al., 2023). While family members in Türkiye have traditionally cared for their elders within the home, this practice has been challenged by urbanization, economic pressures, changing family structures, and the increased participation of women in the workforce, which has led to a decline in the availability of informal caregivers (Altunay & Özkul, 2022). Financial hardship also plays a significant role, with some older adults seeking institutional care due to economic difficulties or insufficient housing space (Demir & İnce, 2021; Taş et al., 2023). Among nursing home residents in Türkiye, the majority are between ages 65 and 74 years old. They also include people with social security and those with insufficient income levels (Bahadır et al., 2022).
In Türkiye, nursing homes evoke positive associations. More specifically, instead of being viewed as places of last resort, they are viewed as desirable living settings that support the well-being of older adults (i.e., wellness, happiness, and quality of life associated with comfort and health; Altomonte et al., 2020). Through offering comfort, professional care, and diverse social activities, nursing homes are known to enhance well-being and break the monotony of daily life (Altunay & Özkul, 2022; Demirbaş, 2018; Uslu et al., 2025). Ease of access to urban amenities and family visits is also valued, especially in centrally located facilities (Dündar & Alptekin, 2022). Interestingly, research shows that even individuals with children or those from more traditional backgrounds may opt for institutional care, suggesting a shift in cultural expectations and caregiving norms in Türkiye's aging society (İnce, 2024).
Despite this shift in attitudes toward LTCs, older adults in Türkiye still generally prefer to age in place while maintaining health, peace, and independence (Bahadır et al., 2022; Güdük, 2022). The concept of “home” is closely tied to privacy, safety, comfort, family connection, and personal control, making it a central element in older adults’ sense of well-being (Altındiş & Üner, 2023). The key preferences for older adults who do enter residential care are to have personal space, the ability to customize their environment, and opportunities for social interaction, as these factors contribute to a sense of belonging and satisfaction (Kaplan & Kaya, 2020).
The design of LTC environments is increasingly recognized as vital to older adults’ well-being (Roos et al., 2022). Supportive environments can reduce stress, improve sleep, promote movement, and foster social connection (Carlson et al., 2012; Engineer et al., 2021; Gripko & Joseph, 2024). In Türkiye, however, current regulations primarily focus on safety and infrastructure compliance rather than user-centered care or the creation of home-like settings, while research on the built environment of nursing homes in Türkiye remains limited. Accordingly, the present study aims to evaluate the physical and architectural features (PAF) of the existing environments of selected nursing homes in Türkiye identify their strengths and weaknesses and provide insights to inform the development of future care settings designed to enhance the quality of life and cultural preferences of older adults. This study aims to fill a gap in knowledge as the first comprehensive effort to evaluate the existing environments of both public and private care facilities across three major cities in Türkiye.
This study aims to fill a gap in knowledge as the first comprehensive effort to evaluate the existing environments of both public and private care facilities across three major cities in Türkiye.
Assessing the Physical Environment
Various tools are available for evaluating the quality of physical healthcare environments, each designed to focus on specific dimensions. Elf et al. (2017) reviewed 23 tools, based on several methodological quality criteria, such as reliability and structural validity. Except for the Multiphasic Environmental Assessment Procedure (MEAP), TESS-NH, and PEAP, most of the tools had low validity, limited application following their development, or were not widely adopted by other researchers (Rom et al., 2022). While TESS-NH and PEAP focus on settings for people with dementia, the MEAP evaluates a broader range of care settings. More recent instruments include EASE (Wrublowsky et al., 2024), LTCU-EAT (Chen et al., 2024), and EAT-HC (Fahsold et al., 2023). EAT-HC shows strong reliability and validity, while EASE shows strong reliability, with a validation process currently underway. Both tools target settings for older adults with cognitive impairments and high care needs. The LTCU-EAT is designed for broader LTC settings, showing promising validity during its application in the early phase of its development.
Although these newer built environment assessment tools are available, MEAP was selected for the present study for a number of reasons. First, it has strong validity and aligns with the study's target population. It is considered the most comprehensive instrument for evaluating the environments of care facilities (Cutler et al., 2006) and explicitly targets residential environments for older adults. Additionally, its validity and reliability have been tested and confirmed in multiple studies (Elf et al., 2017; Linney et al., 1995), making it a foundational reference for developing subsequent instruments (Elf et al., 2017; Cho & Kim, 2014; Cutler, 2000) and appropriate for assessing environments for older adults (Niezabitowski, 2019). Second, it has a strong theoretical foundation, emphasizing the need for congruence between an older person's capabilities and the demands of their environment (Elf et al., 2017). Third, researchers still rely on MEAP for its rigorous, multiphasic view of environments, while selectively refining it (or developing spin-off tools) to better capture what today's older adults expect from the places they call home (Mahmood et al., 2022; Niezabitowski, 2019). In short, MEAP offers a valuable tool for evaluating the built environment, providing a useful framework for gaining a general understanding of current conditions in nursing homes and identifying areas for improvement.
MEAP is composed of four subinstruments, namely the Resident and Staff Information Form, the Physical and Architectural Features (PAF) Checklist, the Policy and Program Information Form, and the Sheltered Care Environment Scale. Given the present study's focus on evaluating the physical environment, and considering feasibility constraints within institutional settings, only the PAF checklist was used. In this study, the terms “physical features” and “architectural features” are used in alignment with the PAF. Physical features refer to the tangible, observable elements within the built environment, such as furniture and safety features. Architectural features describe the structural and spatial characteristics of the building, including room sizes, corridor widths, layout, and the placement of key areas such as nurse stations or exits. PAF Checklist has 153 items across eight dimensions: Community Accessibility, Physical Amenities, Social–Recreational Aids, Prosthetic Aids, Orientational Aids, Safety Features, Staff Facilities, and Space Availability. Table 1 briefly describes each subscale with example items.
The Physical and Architectural Features (PAF) Checklist Subscale Description (Adapted from Moos, 2012).
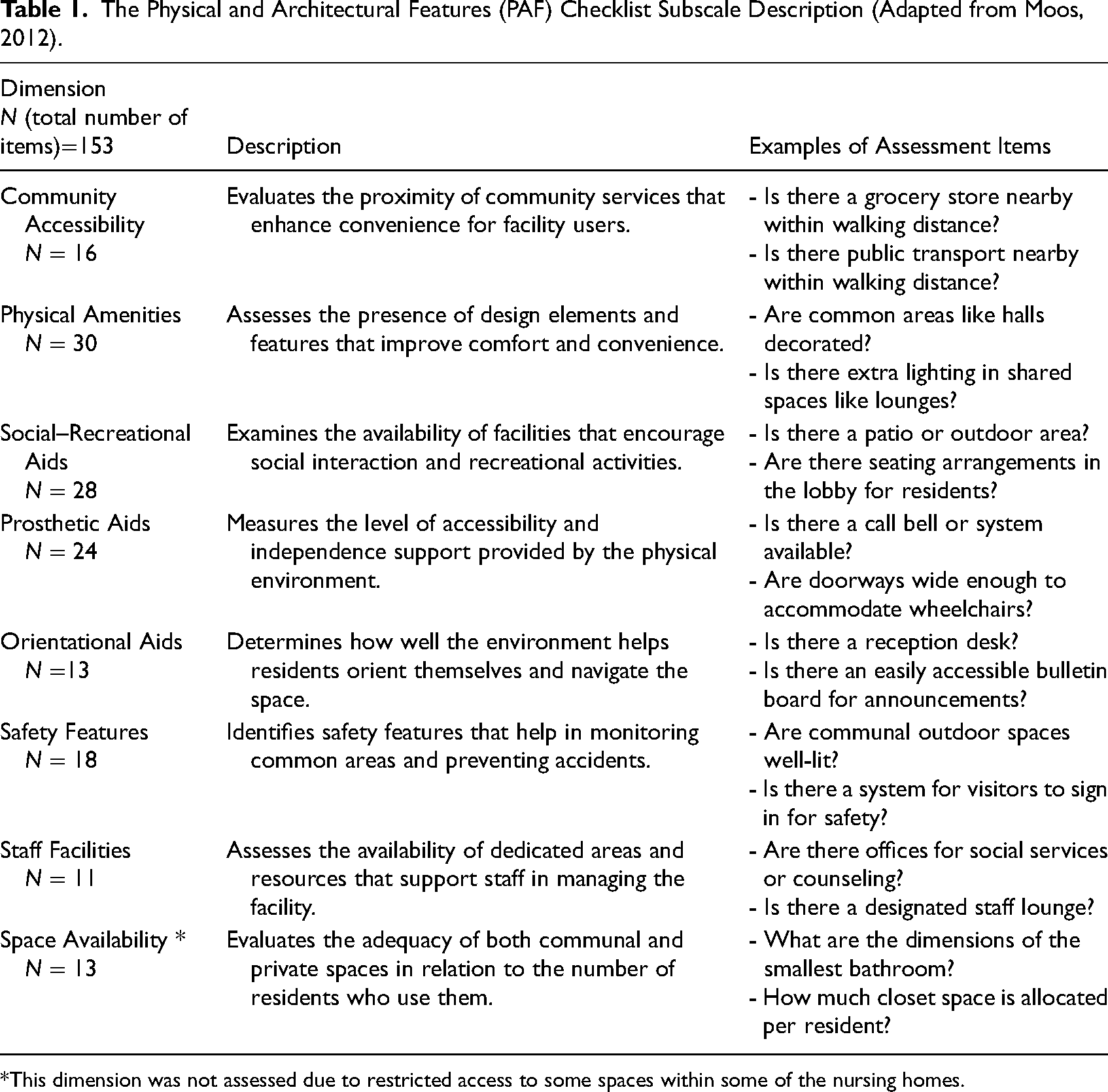
This dimension was not assessed due to restricted access to some spaces within some of the nursing homes.
Background
The PAF dimensions have been the subject of numerous case studies and validated in the literature.
Community Accessibility
The surrounding context for nursing homes has been found to directly impact their residents. For example, Moos and Lemke (1996) assessed City Haven, finding that its urban location contributed positively to community accessibility by enabling residents to access public transportation and essential services more easily. Similarly, Mahmood et al. (2022) evaluated four multiunit buildings in Vancouver, Canada, as part of a case study of a temporary housing program for older adults at risk of homelessness. They found that public transportation facilitated the residents’ social activities and engagement with the community, although improvements were needed to exterior amenities such as seating and storage. Prime Ministry General Directorate of Social Assistance and Solidarity Social Services Child Protection Agency of Republic of Türkiye (T.C. Başbakanlık Sosyal Yardımlaşma ve Dayanışma Genel Müdürlüğü Sosyal Hizmetler Çocuk Esirgeme Kurumu [SYDGM], 2006) reported that residents were dissatisfied with the distance of nursing homes from city centers, which hindered their ability to engage with community services and participate in social activities outside the facility. In a cross-sectional study, Aydın et al. (2020) evaluated the spiritual well-being of older adults in care facilities. Based on their findings, they recommended high proximity to natural landscapes and incorporating nature-based activities within nursing homes to support residents’ quality of life. Overall, these studies underscore the importance of balancing the integration of nursing homes within community settings and nature.
Physical Amenities
Research shows that certain physical features play a vital role in supporting residents’ well-being and quality of life. For example, from their comprehensive observational study of 40 U.S. nursing homes, Cutler et al. (2006) identified significant gaps in resident accommodations, including limited private bathrooms, restricted opportunities for personalization, and workspaces, and a lack of life-enhancing amenities like refrigerators. In addition, cluttered corridors and minimal noise control measures reduced the overall comfort and convenience of the environment for residents. In a cross-cultural study comparing Finnish and Swedish LTC environments, Wahlroos et al. (2021) found that Swedish environments generally offered higher-quality physical amenities, including private apartments with attached bathrooms and kitchenettes, whereas Finnish facilities typically provided single bedrooms with only attached bathrooms (Nordin et al., 2017). Their findings also revealed that the physical environments of Swedish LTCs vary significantly between units, raising concerns that not all older adults in LTC facilities have equal access to quality environments. Research assessing physical amenities in other LTC environments has reported that sheltered outdoor seating, communal televisions, and room mirrors (Moos & Lemke, 1996) and interior amenities such as sufficient and functioning light fixtures (Mahmood et al., 2022), are needed to improve comfort and functionality for older adults. Residents in Turkish nursing homes identified several key features for creating an ideal nursing home environment, including the provision of kitchens on each floor, the availability of libraries, and having personal amenities such as televisions and refrigerators in each room (SYDGM, 2006). Overall, these studies demonstrate that well-designed physical amenities are critical for enhancing the quality of life for residents in care environments.
Social–Recreational Aids
Research shows that environments that encourage social interaction and meaningful activities are among the most crucial factors determining older adults’ well-being. For example, Cutler et al. (2006) found that U.S. nursing homes frequently lack essential social and recreational spaces, with insufficient dining and lounge areas that limited opportunities for meaningful interaction. From their study of temporary housing units in Vancouver, Mahmood et al. (2022) concluded that more thoughtfully designed common areas and seating arrangements can foster greater social interaction and engagement among residents. Similarly, the SYDGM (2006) report revealed that residents in Turkish nursing homes are dissatisfied by the lack of adequate sports and recreational amenities, and private and specialized spaces for family visits. Arıkan Dönmez and Aslan (2024) examined physical activity in Turkish nursing homes from the staff's perspective. Commonly reported issues included the absence of dedicated spaces for physical activity. Moreover, they found that structural limitations such as narrow, short hallways, and spiral staircases hindered access to outdoor gardens, particularly for residents with mobility challenges. Overall, these studies identify that a lack of adequate social and recreational aids is a barrier to promoting social connectivity and overall well-being among older adults.
Prosthetic Aids
Designing the environment thoughtfully can enhance residents’ ability to move freely and maintain autonomy. Cutler et al. (2006) reported that while U.S. nursing homes included various necessary features, such as handrails and grab bars, many areas lacked essential modifications to promote mobility and independence for residents. Similarly, Mahmood et al. (2022) found that while Vancouver's temporary housing program performed well in providing exterior mobility features such as ramps and seating, there were notable gaps in interior accessibility measures, particularly handrails and safety surfaces. Gökler et al. (2022) conducted a risk assessment of Istanbul's nursing homes and identified critical hazards related to prosthetic aids. Key features such as grab bars were absent, while narrow corridors and narrow door openings compromised mobility for residents. Overall, these findings emphasize the importance of incorporating adequate prosthetic aids to support residents’ independence and ensure their safety within care environments.
Orientational Aids
Research shows that the ability to locate oneself and navigate the space is a key aspect of the built environment that supports residents’ quality of life. Engineer et al. (2018), for example, identified orientation aids as a critical component of supporting older adults’ well-being, demonstrating the need for clear wayfinding elements and signage to reduce disorientation and confusion. Several studies have reported that nursing homes often lack sufficient orientational aids, which makes it harder for residents to navigate their surroundings (Cutler et al., 2006; Moos & Lemke, 1996). In Türkiye, Gökler et al. (2022) found various deficiencies in Istanbul nursing homes, such as a lack of clear signage, color-coded corridors, and accessible wayfinding, which hindered the residents’ ability to navigate their environments safely and independently. Collectively, these studies highlight the importance of incorporating effective orientational aids to enhance spatial awareness and autonomy for older adults in residential care settings.
Safety Features
Design features that enhance resident safety are a crucial aspect of care facility planning. Wahlroos et al. (2021) found that Swedish LTC environments scored higher in safety features than their Finnish counterparts, while Mahmood et al. (2022) identified problems in Vancouver's temporary housing program, such as the absence of nonslip surfaces and a lack of handrails in residents’ units, increasing the potential for falls and injuries. Similarly, in Türkiye, Gökler et al. (2022) reported a lack of nonslip flooring and emergency call buttons, as well as unsecured entrances and nonergonomic furniture in Istanbul's nursing homes. These critical safety hazards presented major risks to resident safety. Overall, these findings emphasize the need for robust safety features in residential care environments to ensure the well-being and security of older adults.
Staff Facilities
The PAF of environments in residential care facilities also affect staff satisfaction and performance (Parker et al., 2004). Well-designed environments promote staff focus and safety, thereby improving both staff and resident care quality. Joseph et al. (2016) found that smaller, resident-centered units enhance job satisfaction and reduce stress. Research in various healthcare environments, including residential healthcare centers and hospitals, has demonstrated that adequate infrastructure (such as ergonomic spaces and lifts) minimizes physical strain for staff, whereas large, dispersed layouts, and ambient stressors (high temperature, high noise levels, and low lighting levels) increase their workloads (Joseph et al., 2016; Shetty et al., 2024). Moos and Lemke (1996) reported that City Haven scored high in the staff facility dimension due to the presence of multiple staff offices, meeting rooms, and lounges that supported effective staff management and coordination. Overall, research highlights the critical role of the built environment in shaping the quality of life and well-being of older adults in care settings,
Method
The present study applied the PAF checklist from MEAP to compare seven nursing homes in Türkiye.
Settings
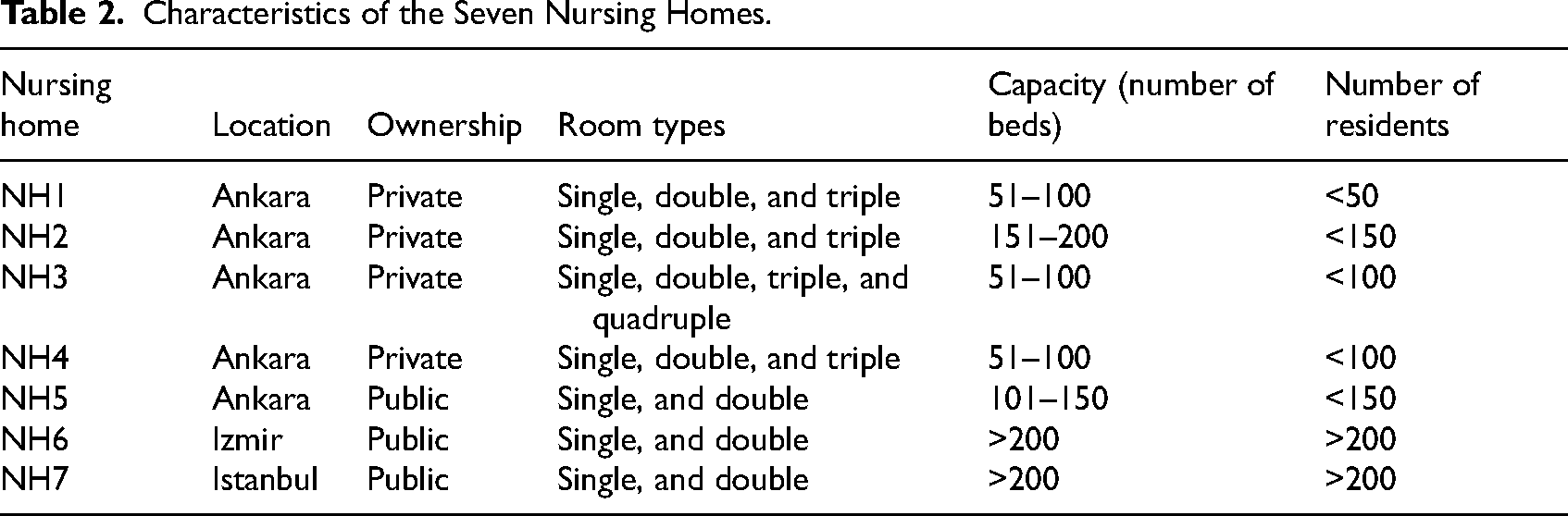
A list of nursing homes was obtained from the official website of the Ministry of Family and Social Services. An initial outreach was conducted with 47 facilities, resulting in agreements with eight nursing homes to participate in the study and allow assessment of their PAF of environments. Efforts were made to include a diverse sample by contacting facilities varying in size, type (public and private), and resident profiles. Private nursing homes tend to be smaller and typically serve residents with more advanced cognitive and physical impairments. These residents are often individuals whose families can afford private care but are unable to provide 24-h support themselves. In contrast, public nursing homes are significantly more affordable, often leading to long waiting lists and specific eligibility criteria for admission. The selection of nursing homes was finalized not only to capture diversity (public/private and size) but also by the willingness of the facilities to participate in the study. After conducting a pilot study in one of the nursing homes, seven further nursing homes were assessed in the study, five in Ankara, one in Izmir, and one in Istanbul (Table 2). The nursing homes’ capacities (number of beds) ranged between 50 and more than 200 residents.
Characteristics of the Seven Nursing Homes.
Only two facilities are purpose-built as nursing homes with multiple buildings (NH6 and NH7). The main shared amenities, such as libraries, stores, and multipurpose activity rooms, are located in the central building, although each accommodation building has its own dining room and lounge. Some buildings are designated for residents requiring special care. In contrast, the other facilities consist of single buildings ranging from two to eight stories (Figure 1). NH5 was originally constructed as a hotel, while the remaining nursing homes began as residential apartment buildings that were later renovated and adapted for use as nursing homes.

Overview of the nursing homes, highlighting differences in building size.
All the selected facilities accommodate residents with diverse care needs. In private nursing homes, the majority of residents are highly dependent on their caregivers, whereas public nursing homes accommodate both independent and dependent residents. The public nursing homes also provide separate floors and blocks for residents with special care needs, such as dementia or significant mobility impairments. In contrast, all the private nursing homes except one accommodate all residents in the same area, regardless of their care requirements.
Instrument
As outlined earlier, this study used the PAF subscale of MEAP (Moos & Lemke, 1996) as the primary measurement tool, supplemented by direct observations. Physical and Architectural Features Checklist uses dichotomous scales to record the presence or absence of specific features, compare the actual situation with standards, and identify areas for improvement. The checklist is accompanied by an administration guide that provides a structured framework for observing relatively objective environmental features and completing the assessment. This includes detailed instructions on how to determine whether each item should be marked as “yes” or “no.” For example, in facilities with multiple main hallways, the guide advises assessors to base their judgment on the narrowest hallway.
In the present study, all dimensions were assessed except for Space Availability due to restricted access to specific areas within certain nursing homes, which limited the evaluation of all intended spaces (140 items out of 153 included in this study). Of the 140 items on the checklist, 135 were straightforward and could be assessed objectively by the researcher. However, five items involved more subjective judgment—three related to lighting conditions and two to the condition of furniture. These were evaluated based on the researcher's observations without the use of light measurement tools. For the furniture-related items, assessments were based on whether the furniture appeared well-maintained, safe, and stable, with no signs of splintering, rough edges, or similar hazards.
Procedure
A pilot study was conducted in one of the facilities to test the feasibility of the checklist and refine the data collection process. Prior to data collection, the checklist was examined multiple times to gain familiarity with its content and structure, allowing the researcher to develop proficiency and ensure consistent application throughout the study. The pilot study also ensured that the checklist was appropriate for the study's cultural context. Ultimately, no alterations were made to the checklist following the pilot study, except for one specific item under Community Accessibility. The item considers whether a church or a synagogue is within walking distance of the facility. In this case, to account for cultural differences, the item was modified to measure the proximity of a “mosque.” After the pilot study, the first author administered the PAF checklist to the remaining seven nursing homes through direct observation, supplemented by photographic documentation where permitted. All site visits were conducted during working hours and took 2–4 hours depending upon the size of setting.
Data Analysis
The data were first transferred to hand-scoring worksheets, as in accordance with the MEAP guidelines (Moos & Lemke, 1996). For each of the seven PAF dimensions, raw scores were calculated as the percentage of features that were present in that dimension. The analysis was primarily descriptive and comparative. Standard scores allowed cross-facility comparisons to identify strengths and weaknesses across PAF dimensions. This comparison refers to standardized MEAP scoring from Moos and Lemke (1996), acknowledging its age but using it as a comparative reference rather than a prescriptive standard. The MEAP Guidelines provide conversion tables for the standardized scores categorized into three types of residential settings: nursing homes, residential care facilities, and apartment settings. For this study, standard scores were calculated using the “nursing home” category from the conversion tables, as it most closely aligns with both the official classification of facilities in Türkiye and the level of care provided. This typically includes 24-h supervision, assistance with daily living activities, and medical support. Despite the hybrid nature of LTC models in Türkiye, the overall structure of care and resident profiles across the sampled facilities reflected higher levels of dependency. Moreover, in the absence of a localized or hybrid benchmark within the MEAP framework, the nursing home standard scores offer the most appropriate and consistent basis for making comparisons. These standardized scores, with a mean of 50 and a standard deviation (SD) of 10, enabled comparative analysis across dimensions and facilities, taking into account differences in ownership type (public vs. private) and building origin (purpose-built vs. converted). Supplementary qualitative field notes and photographs contextualized and illustrated the key findings.
Results
As noted earlier, the raw scores for each facility are percentage based, representing the portion of features present out of the total possible features (Moos & Lemke, 1996). For instance, a facility with 15 out of the 30 physical features would receive a raw score of 50% for physical amenities. Table 3 presents the seven facilities’ standard scores in the seven domains, while the following subsections comparatively assess facilities in terms of the seven dimensions.
Standard Scores of Seven Nursing Homes in Seven Dimensions of the Physical and Architectural Features (PAF; Moos & Lemke, 1996).
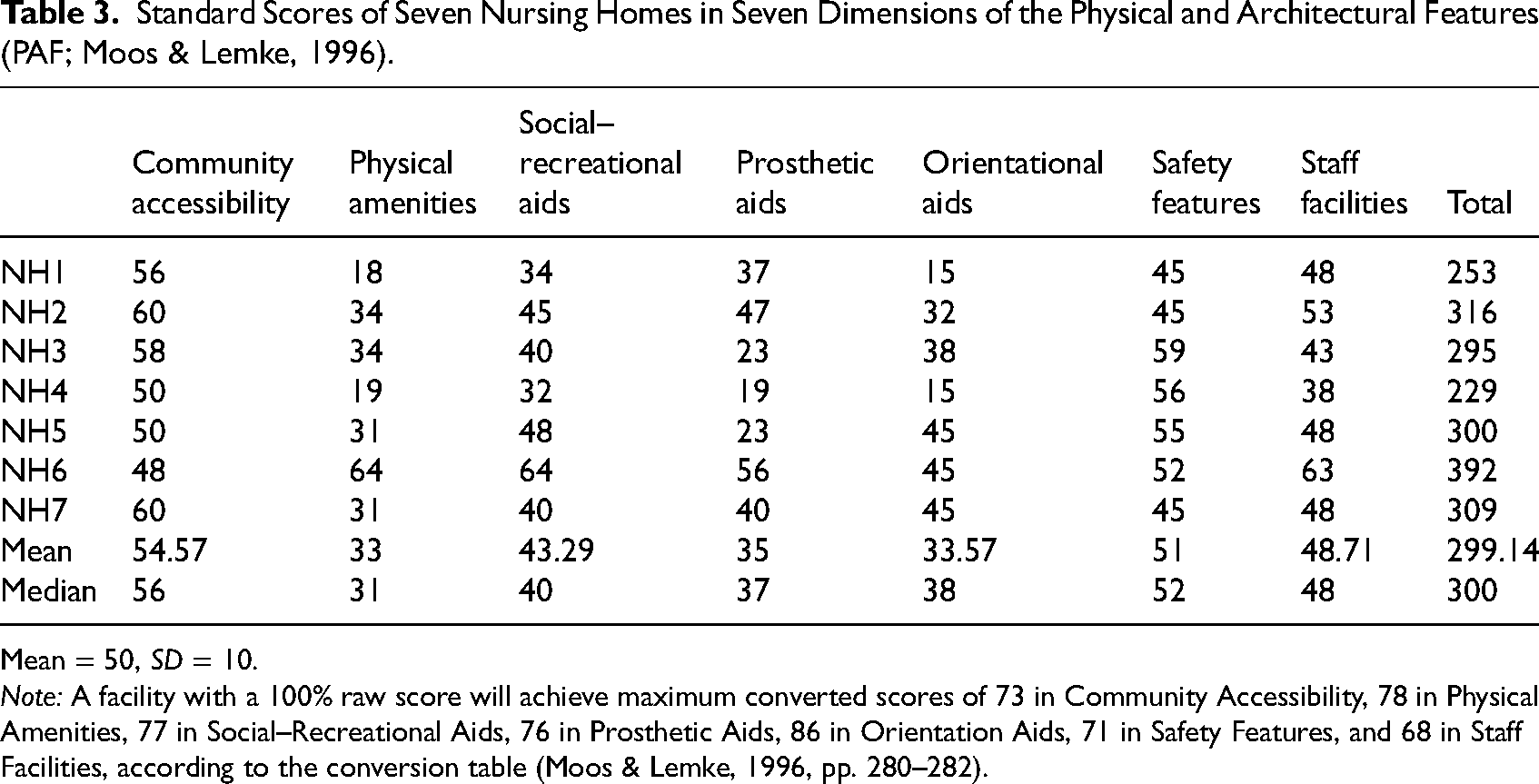
Mean = 50, SD = 10.
Note: A facility with a 100% raw score will achieve maximum converted scores of 73 in Community Accessibility, 78 in Physical Amenities, 77 in Social–Recreational Aids, 76 in Prosthetic Aids, 86 in Orientation Aids, 71 in Safety Features, and 68 in Staff Facilities, according to the conversion table (Moos & Lemke, 1996, pp. 280–282).
Community Accessibility
This dimension evaluates the proximity to the nursing homes of various community resources, such as banks, post offices, and pharmacies, with “easy walking distance” defined in the guidelines as ¼ mile (approximately 402 meters). It is important to note that these facilities serve a diverse population, not only frail older adults. Thus, some residents can walk this distance independently. This dimension also assesses the availability and ease of access to public transportation. In cases where facilities included multiple buildings, walking distances were measured from the main resident entrance to the nearest relevant community feature, while Google Maps was used to identify the nearest community resources for each nursing home. The walking distances to specific nearby amenities ranged from 81 to 1,100 meters for the mosque; 400 to 1,300 meters for the bank; and 130 to 350 meters for the park.
The seven nursing homes’ average score was 0.46 SDs above the standard mean in community accessibility, indicating higher access to nearby community services than the PAF benchmark. Figure 2 presents examples of nursing homes with their immediate surroundings in locations with higher scores of community accessibility, including well-lit streets with bus stops equipped with benches.

High community accessibility: Sheltered bus stops with benches and lighting in the street.
Physical Amenities
This dimension evaluates nursing homes based on the availability of specific exterior physical features, such as outdoor furniture and sheltered entrances, and interior features, such as shops, kitchen facilities, and wall spaces for hanging pictures. The mean score for physical amenities was 1.7 SD below the standard mean, showing a lack of physical amenities compared to the standard scores.
Regarding exterior spaces, all facilities had sheltered entrances to protect residents from the weather. Their outdoor furniture was in good condition, with three public nursing homes providing outdoor seating areas protected from the weather (Figure 3). However, all the nursing homes except NH6 had limited amenities, particularly in the interiors. Only two provided commissary stores or shops, while only three had air conditioning. It is important for nursing homes to include at least a small shop offering basic daily necessities and emergency items, such as shampoo and pens, regardless of the facility's size or urban location. Not all residents can leave the premises independently at any time, while even short trips can pose challenges, whether due to mobility limitations or the physical effort of carrying items back. Therefore, the presence of an on-site convenience shop is a practical necessity, not merely a luxury that supports the residents’ quality of life. Four of the facilities’ hallways were partially decorated with artwork regardless of the nursing home's size, but most of the other walls were left undecorated. Moreover, in the community areas, only one facility had a drinking fountain, while there were no writing surfaces or table lamps for individual use. Regarding cooking facilities, two nursing homes had no kitchenette at all, three had a communal kitchen on each floor, and two had kitchenettes in the rooms (Figure 4). The observations indicated that the shared kitchens were rarely used, whereas residents with in-room kitchenettes regularly prepared tea/coffee and small snacks, regardless of whether the facility offered communal dining rooms or in-room meal service. Regarding other positive interior features, some of the nursing homes’ rooms had windowsills wide enough to accommodate flower arrangements (Figure 4), wall spaces for hanging pictures, and mirrors in the bathrooms.

Exterior physical amenities: Seating with umbrella shading.

Interior physical amenities: Rooms with available spaces for plants and a kitchenette.
Social–Recreational Aids
This dimension assesses how well the PAF promote socialization and activity engagement by examining the availability of amenities such as seating areas at the building's entrance, gardening spaces, game tables, designated activity areas, library resources, and reading materials. The average social–recreational aid score was 0.67 SD below the standard mean, suggesting limited space for social and recreational activities.
Opportunities for social interaction were limited in the majority of the nursing homes. However, NH6, which received the highest score by a significant margin, provided numerous socialization opportunities for its 200-plus residents. These included a dedicated space for a choir, two hobby rooms, a library, a music room, multiple lounges, and small lobbies serving every four rooms (Figure 5). Additionally, NH6 offered multiple dining options, which is expected in such a large facility. These included a coffee shop and restaurant, where residents could choose from alternative meal options. While these spaces were not open to the general public, they served as welcoming areas where residents could spend time with their visitors. The two other public nursing homes also offered common areas with indoor and outdoor seating, along with gardening spaces and courtyards (Figure 6) and multipurpose hobby rooms that served as a library and a space for activities such as painting, arts and crafts, pottery, and knitting. Although these smaller facilities did not offer the same variety of amenities as NH6, they provided more distinct spaces for activities than the private nursing homes.

Social–recreational indoor spaces: Small lobbies for every four room.

Social–recreational outdoor spaces: A plantation garden and courtyard.
All the facilities provide regular meal services three times a day; however, in contrast to the public nursing homes, the private nursing homes lacked dedicated dining rooms, with meals being served to residents in their rooms. Furthermore, no specific spaces were allocated for exercise or activities such as arts and crafts; instead, these were conducted in the lobby or in common areas within the wards.
Physical and Architectural Features Checklist also recommends that certain basic amenities, such as a reading or activity room, should be available in all nursing homes, regardless of their size. These features support residents’ access to everyday needs and opportunities for socialization. The provision of shared spaces for informal gathering, reading, or light activity is important for residents’ quality of life, even for those who spend most of their time inside their rooms. Therefore, noncompliance—indicated by a low score on this dimension—represents an important shortcoming.
Prosthetic Aids
This dimension assesses the aspects of the environment that support resident mobility and promotes ease of use within the facility, including the presence of safety bars and handrails in hallways, bathrooms, and inside rooms; hallway widths; sufficient spacing between furniture to allow wheelchair access; automatic doors; the absence of raised thresholds; and the elimination of stairs. The average score for prosthetic aids was 1.5 SD below the standard mean, indicating that these nursing homes are significantly underequipped in these respects.
The hallway widths varied across the nursing homes. In the public nursing homes, they met the minimum width requirement of 2.4 meters (Moos & Lemke, 1996; Figure 7); however, in one private nursing home that had been repurposed from a different building type, some hallways were as narrow as 90 cm. On the other hand, all the nursing homes were equipped with automatic doors (Figure 7).

Prosthetic aids: Wide hallways with handrails and automatic doors.
In all the nursing homes, safety bars and handrails were available in most bathrooms and hallways. Some nursing homes received lower scores because they had bathroom doors that did not open outward, lacked lift bars beside the toilets, and had bathroom spaces that were not wide enough to accommodate a turning wheelchair.
Orientational Aid
This dimension assesses the nursing home environment's ability to support residents in navigating the facility and the surrounding neighborhood. The elements used to assess this dimension include the reception area, signage, bulletin boards, and other features that support residents’ orientation. The score for orientational aids was 1.65 SD below the standard mean, indicating limited provision of features that support wayfinding, although scores varied noticeably across facilities.
Each nursing home had a reception area. Three facilities provided visible signs indicating the floor number, whereas others lacked such signage. Bulletin boards were present in all the public nursing homes but in only one private facility. However, none of the nursing homes provided a list or pictures of staff members. Only two of the public nursing homes had a sound system for making announcements. None of the nursing homes had maps displaying nearby community resources or directions for accessing them. All nursing homes in the study displayed the residents’ names on their room doors, although only one facility also had photographs. In certain homes, the residents had personalized their doors with flowers, knitted decorations, or posters of their favorite sports teams or historical figures (Figure 8). Such personalization is not only a wayfinding aid but also an important sociocultural expression of personal identity. The ability to personalize spaces, depending on managerial policies, was a noteworthy aspect of these homes.

Orientational aids: Personalized door of a resident's room.
Safety Features
This dimension assesses how well the environment ensures the safety of its residents in terms of attributes such as the visibility of entrances and seating areas from employees’ stations, adequate interior and exterior lighting, nonslip surfaces, call buttons, and smoke detection devices in rooms and hallways. The average score for safety features was 0.1 SD above the standard mean, demonstrating a satisfactory focus on safety issues.
The nursing homes’ outdoor areas were well-lit, and the entrances and outdoor seating areas were visible from employees’ offices or stations. Each nursing home had a single main entrance monitored for security purposes. In all facilities, the bathrooms had call buttons while the hallways had smoke detectors. However, not all the nursing homes featured nonskid surfaces on stairs or ramps. In two facilities, the lighting levels in stairways or hallways were noticeably lower than in other areas. In six of the nursing homes, areas prone to wetness, such as bathrooms, lacked nonslip materials, posing potential safety risks (Figure 9).

Low safety features: Lack of nonslip materials and grab bars.
The slip resistance of flooring materials was assessed through direct observation by the researcher, based on professional experience and the type of material present (e.g., ceramic vs. rubber flooring). An unusual observation in one facility was the placement of a microwave and what appeared to be a mini-refrigerator within a toilet room situated between the toilet and shower area (Figure 9). While this may have been an improvised attempt to provide residents with access to food preparation tools, it posed significant safety and hygiene concerns. This type of ad hoc adaptation highlights the need for clearer design regulations to ensure that efforts to promote independence do not risk compromising the residents’ well-being.
Staff Facilities
This dimension evaluates how the built environment of the nursing home supports staff in performing their duties. Staff facilities scored 0.13 SD below the standard mean, suggesting room for improvement in providing spaces that support staff well-being and job performance—factors that can influence the overall quality of resident care.
In all the nursing homes, the offices were generally free from distractions caused by nearby activities. Most of the public nursing homes had sufficient space for performing managerial functions, with offices allocated for managers, social services staff, psychologists, registrars, and accountants. In three cases, a single office was shared by different staff members on different days; for example, it was used by the psychologist on Mondays and Wednesdays and by social workers on other days. Only two nursing homes had conference rooms, while in most facilities, meetings were held in individual offices, usually that of the nursing home manager. In addition, only two nursing homes had designated staff lounges. In the other facilities, staff took breaks in their offices or common areas within the nursing home.
Figure 10 compares the scores in each nursing home for each dimension and between nursing homes. As the figure shows, purpose-built facilities (NH6 and NH7) consistently scored higher across nearly all domains, particularly in social–recreational aids, prosthetic aids, orientation aids, and staff facilities in comparison to converted facilities. These facilities demonstrated greater spatial efficiency, dedicated communal areas, and better planning, indicating that architectural intent at the design stage is associated with better environmental support for residents and staff. The converted facilities generally scored lower in categories requiring structural modifications. Thus, they frequently lacked appropriate hallway widths, customized bathrooms, and personalized activity spaces, highlighting the limitations inherent in retrofitting existing structures for elder care.
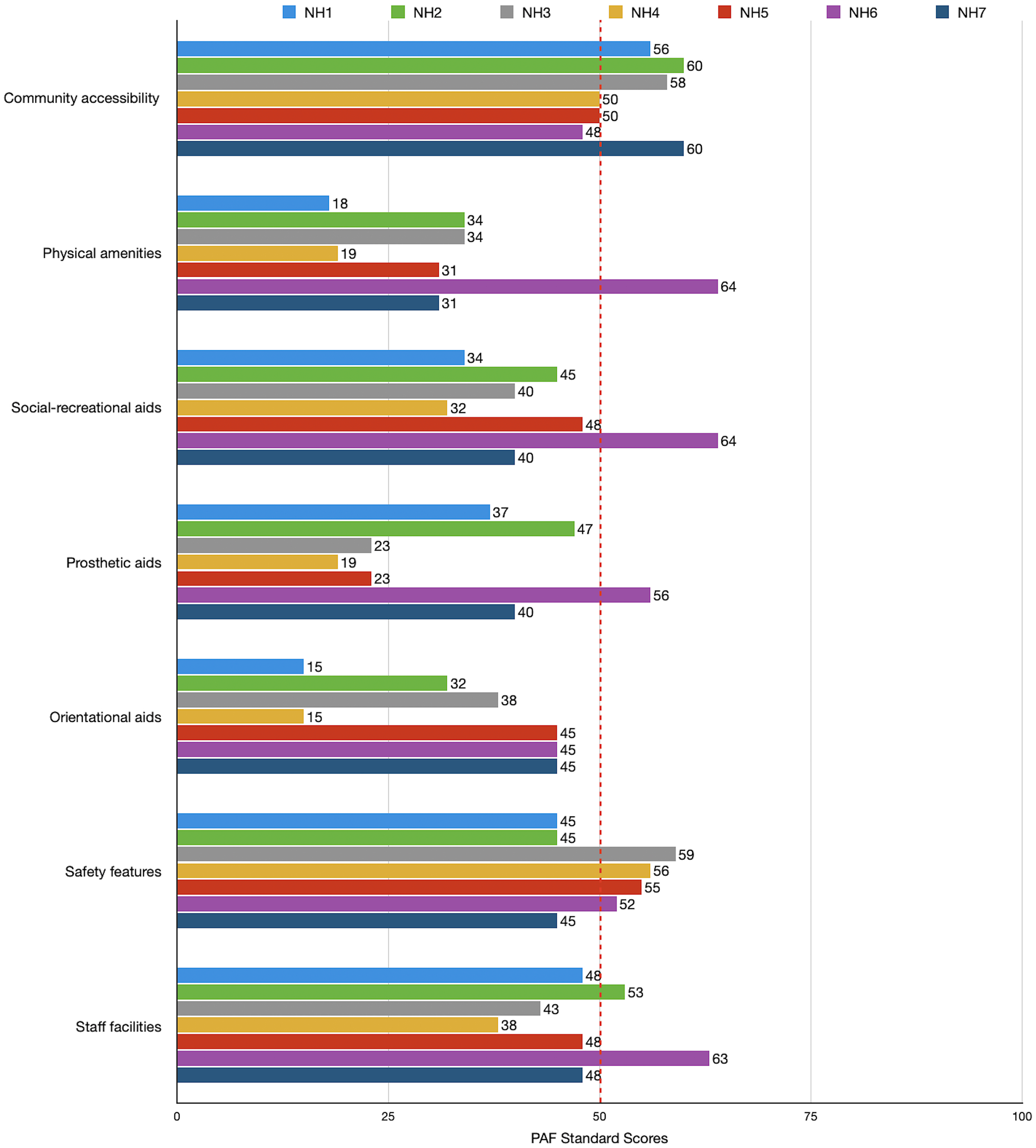
Bar chart of seven nursing homes’ performance in seven dimensions of Physical and Architectural Features Checklist (PAF).
All seven facilities are located in urban areas, which contributed to strong scores in community accessibility. Proximity to services such as mosques, banks, and public transit helped maintain residents’ connection with the broader community. However, despite their urban location, the homes varied in their access to public transportation and the proximity of community services. For example, residents at two of the public nursing homes faced challenges accessing the nearest bus stop.
The larger facilities, particularly NH6 and NH7, tended to perform better in providing diverse social spaces, staff offices, and safety features. However, larger size alone was not sufficient; rather, the benefits were more pronounced when paired with purpose-built design and public ownership. Conversely, some smaller private homes (e.g., NH4) scored poorly on essential features such as hallway width, orientation aids, and staff infrastructure, reflecting challenges in adapting to a limited space.
Overall, the nursing homes received the lowest scores for physical amenities and orientational aids, indicating systemic design limitations across the sample. Safety features showed the most consistency across all facilities, suggesting that regulatory standards may contribute to uniformity in this area. The greatest variability was observed in social–recreational aids and staff facilities, which seem to depend more on institutional priorities and available space than regulatory requirements.
Discussion
This study explored the built environments of seven nursing homes in Türkiye, highlighting both shared strengths and noticeable disparities across the facilities. These findings must be interpreted within the broader cultural context of elder care in Türkiye, where changing family dynamics, economic pressures, and limited informal caregiving have increasingly made institutional care a viable and sometimes necessary option for older adults. While many older adults in Türkiye still express a preference for aging in place, those who move into nursing homes often do so due to physical limitations, health problems, or the absence of family support.
One of the most consistent strengths across the facilities was their urban location, which provided residents with high community accessibility to amenities such as mosques, shops, and parks. This accessibility may reflect Turkish cultural values of connection, familiarity, and proximity to daily life outside the institution, which can help maintain social ties and ease the emotional transition into institutional living. While the higher scores in this dimension suggest that location might play an important role in infrastructure and the supporting social and emotional continuity valued by older adults in Türkiye, these findings are based on the current sample, which did not include rural or suburban settings. Therefore, further research on more diverse geographical contexts is needed to confirm this relationship.
The safety features scores showed minimal deviation (ranging from 45 to 59), likely reflecting the effect of national regulations. All seven nursing homes had safety features near the mean of 51 (rangeing from 42 to 59), although they urgently need bathroom safety upgrades. These include installing grab bars beside toilets, ensuring outward-opening doors for ease of access, and using nonslip materials in wet areas—all of which were present inconsistently across the facilities.
Another area of relative strength was the availability of dedicated staff facilities in public nursing homes. Particularly in purpose-built facilities like NH6, staff were provided with designated break rooms, offices, and meeting spaces. This is especially important as families become less available for informal caregiving due to urban migration and shifting gender roles in the workforce in Türkiye.
However, the findings also revealed critical environmental shortcomings, including the lack of social–recreational aids. Except in two nursing homes, these spaces were limited, reducing opportunities for community building. This is noteworthy in the Turkish context, where elders report valuing activities such as socializing, engaging in hobbies, or participating in religious or family gatherings. Environmental elements for orientation aids and mobility through prosthetic aids, such as clear signage, color-coded corridors, and handrails were also inconsistently present, with the lowest scores found in converted private homes.
A final area of concern is physical amenities, which had the lowest score (ranging from 18 to 64). This was particularly apparent in the private nursing homes converted from residential buildings. For example, the NH1 and NH4 lacked key physical features that support autonomy and dignity in aging, such as in-room kitchenettes, accessible bathrooms, and personalized storage.
Overall, the findings show that public nursing homes, especially those designed specifically for elder care, consistently outperformed private ones in areas such as staff facilities, social–recreational aids, and orientation aids. This suggests that ownership type and original building function are strong predictors of environmental adequacy, thereby underscoring the need for robust national design guidelines. None of the seven care settings received near-perfect scores in any dimension largely due to systemic and structural limitations observed across the sample. Several contributing factors may explain why the majority of the facilities fell below standardized care means. First, many of the homes, especially the private and converted ones, were not originally designed with the specific spatial and functional needs of older adults in mind, resulting in compromised design quality in key areas such as orientation and mobility. Second, there appears to be a gap between policy-level design standards and their consistent implementation or enforcement on the ground. Finally, limited financial resources, prioritization of basic safety over quality-of-life features, and institutional constraints (e.g., space or staffing) may further contribute to suboptimal performance in several dimensions. To conclude, these findings highlight the need for more comprehensive, context-sensitive planning and evaluation mechanisms for LTC environments in Türkiye.
In light of these findings, several key modifications are recommended. First, enhancing social–recreational areas and providing communal dining spaces can reduce isolation, promote everyday interaction within the nursing home, and ensure adequate space for family visits—a significant need for elderly residents (Kaplan & Kaya, 2020; SDGYM, 2006). Second, it is necessary to upgrade orientation features, including signage, color-coded paths, and visual cues, to support the residents’ navigation and cognitive comfort. Third, it is critical to improve overall safety, including bathroom safety through grab bars, nonslip surfaces, and accessible layouts, for maintaining dignity and preventing injury. This is in line with previous findings in Türkiye concerning health and safety (Gökler et al., 2022). Finally, personal amenities such as kitchenettes and private storage should be integrated so that residents can express their identity and maintain autonomy. This is particularly significant given that Turkish older adults associate the concept of “home” with privacy, comfort, and a sense of control (Altındiş & Üner, 2023).
Overall, while the study identified promising practices in some public facilities, the disparities in physical environments reflect broader issues of inequity in Türkiye's growing LTC sector. As cultural expectations around aging continue to evolve, the physical environment of care settings must evolve with them, supporting not only the health and safety of residents but also their preferences, dignity, and sense of home. Regulations should also be established to ensure that health and safety standards are consistently upheld in all aspects of managing these facilities. Over time, original design features may become outdated and replaced with less effective elements. Design guidelines should not only be assessed for adherence but also periodically evaluated for their effectiveness in supporting resident well-being and autonomy. These changes can be monitored using other components of the MEAP checklist or similar assessment tools that extend beyond the scope of this study.
Limitations and Future Directions
There are certain limitations to this study. The first is the small sample size of seven facilities across three cities. Further research could include nursing homes from smaller towns across other regions of Türkiye to expand the database and enhance generalizability. The second limitation is the restricted access and detailed examination of certain areas, particularly regarding space availability. Future studies could establish protocols that balance privacy concerns with the need for thorough facility access to ensure a comprehensive assessment. Due to the hybrid structure of the sampled facilities, the generalizability of the findings to countries or contexts with more standardized care models may be limited.
While PAF's strengths lie in its comprehensive and action-oriented approach, it has certain limitations that mean the findings should be interpreted cautiously. For example, cultural variability should be considered to ensure a holistic understanding of institutional effectiveness, such as by adapting items like access to religious facilities. Moreover, although the PAF administration guide offers helpful instructions for completing the checklist, some criteria remain subjective and require more standardized measurement tools such as light meters. Nevertheless, as this study shows, working with international scholars to update the assessment tools to reflect cultural, technological, and lifestyle changes among older adults can make them more relevant in future studies for a wider community.
The PAF checklist should be integrated with policy considerations and other MEAP scales to account for the actual use of features, not merely their presence or absence. The PAF should also be revised to adopt a more user-centered approach and to better assess home-like features within the environment. Future research could focus on refining the tool to incorporate these dimensions more effectively, ensuring it aligns with residents’ lived experiences and perceptions of home. Further research can incorporate qualitative feedback from residents and staff to enrich our understanding of the physical environment's impact on their daily experiences. Finally, longitudinal research can provide insights into how facility changes affect resident well-being over time, thereby supporting evidence-based policy improvements.
Conclusion
This study revealed considerable variability in the PAF of the environments of nursing homes to support residents’ comfort, safety, autonomy, and social engagement. As Türkiye develops an LTC continuum for older adults, additional guidance is required. This study contributed to knowledge by determining the conditions of nursing homes, identifying the aspects that require improvement, and offering suggestions to consider for designers and managers for new construction. Addressing these features requires focused efforts from policymakers, architects, and administrators to create environments that support residents’ health, dignity, and quality of life. These findings emphasize the need for targeted improvements in the design of nursing home environments. Facilities should prioritize the integration of social–recreational spaces, orientation cues, and safety-enhancing features, particularly in bathrooms and circulation areas. Design strategies should also support residents’ independence through personalized spaces and in-room amenities. Addressing these deficiencies through thoughtful environmental modifications will help create more supportive, inclusive, and culturally responsive care environments in Türkiye.
This study revealed considerable variability in the PAF of the environments of nursing homes to support residents’ comfort, safety, autonomy, and social engagement. As Türkiye develops an LTC continuum for older adults, additional guidance is required.
Design strategies should also support residents’ independence through personalized spaces and in-room amenities.
Implications for Practice
While establishing basic design guidelines is important to reduce disparities between facilities, flexibility should also be built into these standards to reflect the diverse cultural, socioeconomic, and care needs of residents and staff. By incorporating adaptable features that reduce the need for relocations, all residents should have access to spaces that support autonomy, dignity, and well-being throughout their care journey.
Nursing homes should be located near community services such as grocery stores, public transport, and parks to foster social inclusion and engagement beyond the facility. Internally, providing amenities like in-room kitchenettes, TV, etc., and access to natural elements like gardens and plants can support residents' independence and comfort.
Facilities should incorporate features that promote both safety and orientation. This includes non-slip flooring, grab bars in residents' bathrooms, and appropriate lighting in high-risk areas like bathrooms and staircases, clear signage, color-coded corridors, and visual orientation cues. Specialized activity spaces that accommodate varying levels of socialization and mobility levels are recommended.
Creating positive work environments with dedicated lounges, ergonomic office setups, and flexible meeting areas contributes to staff satisfaction and morale. These improvements not only benefit caregivers but also enhance the overall quality of care and reduce staff turnover.
Assessments and design alterations should be culturally responsive, reflecting the values, traditions, and daily preferences of older adults, and should accommodate the technological and contemporary life-style changes and expectations.
Footnotes
Acknowledgments
The authors would like to extend their sincere gratitude to the staff and authorities of the nursing homes in Ankara, Izmir, and Istanbul for their invaluable support and cooperation throughout this study.
Author Contributions
Negin Froughisaeid: Conceptualization, data curation, formal analysis, methodology, visualization, and writing – original draft, review and editing. Burçak Altay: Conceptualization, methodology, visualization, and writing – original draft, review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open access funding provided by Bilkent University.